endodontic surgery · to endodontic surgery involve: 1-the nasal floor. 2-the maxillary sinus....
TRANSCRIPT

ENDODONTIC SURGERY
Presented by Reham Hassan
Associate Professor, Endodontic Department
Minia University

• Endodontic surgery involve all surgical
procedures performed to remove
causative agents of periradicular pathosis
and to restore the periodontium to a state
of biologic and functional health.
▪ Definition:

The aim of surgical endodontics is to
restore the integrity of the supporting tissues of
a tooth or teeth, when non-surgical endodontics
has failed and re-treatment cannot be
undertaken or is contraindicated.
I.R. Matthew. 2007.

Changing Concept!!!
The term CONSERVATIVETREATMENT has beenused as an equivalent fornon-surgical endodontictreatment but it appliedalso to surgicalendodontics as thesurgical procedurebecomes theconservative effort toavoid radical sequela-theextraction of the tooth.
• The current concept is treat a tooth non-surgically and to follow the progress oftherapy by periodic clinical and radiographicexaminations.

➢ Many of the previously accepted indications are no longer valid in light of current concept of the biological basis for endodontic treatment.
➢ Therefore, it must be recognized that periradicularsurgery has become very selective in modern endodontics.
➢ Also, the retreatment possibilities offered by modern endodontics has reduced the number of cases requiring surgery.
False Indications

1.Extreme Apical Curvature .
The introduction of Ni Tiinstruments allows abetter ability to axiallyprepare curved canalsthat were otherwisecandidates for root endresection.


2. Internal resorption.
Heavy irrigation with hypochlorite and subsequentcanal enlargement followed by thermoplasticizedobturation technique.
Conventional Endodontics Surgical Endodontics

3.Presence of immature apex:
❑Hermetic sealing of the apeximpossible.
❑The final result produced a tooth with extremely thin dentin walls
❑Complicated by a decreased crown-root ratio if an apicectomy was done.



35 monthes after intialtreatment

4. Persistent pain
Missed canalThe presence of an additional unexpected canal such as mesiobuccal root of maxillary molars and first bicuspids.
Cause

4. Persistent pain.
Incomplete cleaningand shaping
Periapical tissue inflammation due to
retained irritants within the root canal foramina that
could not be removed with instrumentation.

4. Persistent pain .
• Operator's inability tolocate the elusive apicalconstriction.

Indications for endodontic surgery:
1) Need for surgical drainage.
2) Failed non-surgical endodontic treatment.
a. Irretrievable root canal filling material.
b. Irretrievable intraradicular post.
3) Calcific metamorphosis of pulp space “Solid
tooth”.

4) Procedural errors:
a. Instrument separation.
b. Non-negotiable ledging.
c. Root perforation.
d. Symptomatic overfilling.
5) Anatomic variations:
a. Root dilacerations.
b. Apical root fenestration.
6) Biopsy.

7) Corrective surgery:
a. Root resorptive defects.
b. Root caries.
c. Root resection (Amputation).
d. Hemisection.
e. Bisection (Bicuspidization).
8. Replacement surgery. (Intentional replantation).
9. Implant surgery:
a. Endodontic implant.
b. Osseointegrated.

1-Faliure of root canal therapy.
a-Irretrievable root canal filling material.
b-Irretrievable intraradicular post.


2-Calcific metamorphosis of the pulp space.
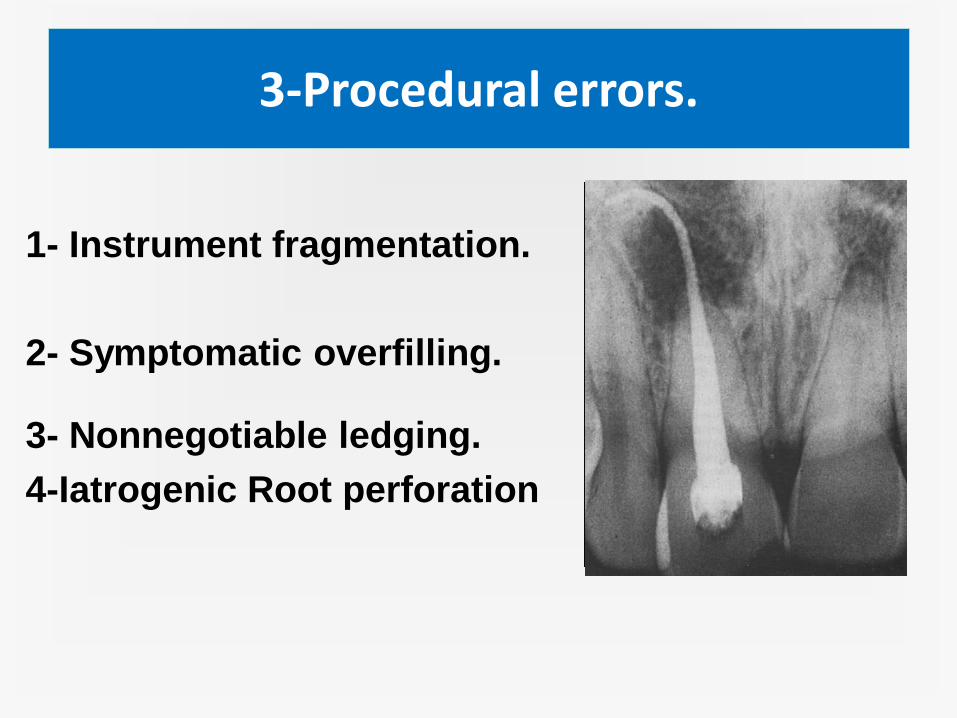
3-Procedural errors.
1- Instrument fragmentation.
2- Symptomatic overfilling.
3- Nonnegotiable ledging.
4-Iatrogenic Root perforation

Root dilacerations or Bayonet shape canal.
4-Anatomic variations.

(5) Surgery to gain information from a biopsy.

6-Corrective surgery.
• a-Root resorptive defects.
• b-Root caries.
• c-Root resection.
• d-Hemisection.
• e-Bicuspidization.

A-Root Resorptive Defects.

B-Root Caries.

C-Root Resection.
Removal of one or more roots of multi-rooted teeth , which separated at the junction of roots & into the crowns.

D-Hemisection.
Surgical division of multi-rooted teeth & the removal of the defective half

E-Bicuspidization.
Surgical division of a tooth
with the root that leaves the two halves of the crown and their respective roots retained in its place .


7- A Horizontal fracture of root apex with pulpal necrosis.
10-Replacement surgery
1-Replant surgery
1- Intentional
2- Posttraumatic
2- Implant surgery
• 1- Endodontic
2- Endosseous


CONTRA-INDICATIONS FOR
ENDODONTIC SURGERY

A-THE PATIENT MEDICAL STATUS.
Patient must be physically, mentally,
and systemically healthy enough to
permit uneventful healing.
1-Clotting Deficiencies.
2-Diabetes.
3-Dialysis Patients.
4-Immunocompromised patients.

B-ANATOMIC CONSIDERATIONS.
The major anatomic considerations of important
to endodontic surgery involve:
1-the nasal floor.
2-the maxillary sinus.
3-the mandibular canal and its neurovascular
bundle.
4-the mental foramen and its neurovascular bundle.
5-anatomic limitations to adequate visual and
mechanical access to surgical site,too thick
cortical plate of bone.

C- PERIODONTAL CONDITION.

D-VERTICAL ROOT FRACTURE.

E-UNSKILLED SURGEON.
➢ A skilled surgeon with the
needed armamentarium is
usually able to circumvent these
anatomic limitations and
accomplish successful
endodontic surgery.
➢ The majority of endodontic
surgical procedures should be
done by trained endodontic
specialists.


CLASSIFICATION OF
ENDODONTIC SURGICAL
PROCEDURES

1-Surgical drainage
a-Incision & drainage . (I&D)
b-Cortical trephination (fistulative surgery) & Marsupulization
2-Periradicular surgery:
a-Curretage. b-Biopsy c-Root-end resection.
d-Root-end preparation and filling.
c- Corrective surgery:
i-Perforation repair:
-Mechanical. -Resorptive (internal& external)
ii-Root resection. iii-Hemisection.
3-Replacement surgery (extraction/ replantation).
4-Implant surgery:
a-Endodontic implant.
b-Root –form osseo integrated implants.

1-SURGICAL DRAINAGE
A-Incision & Drainage (I&D).
B-Cortical Trephination.

a-Incision & drainage . (I&D)
Definition:
Release of purulent or hemorrhagic exudates from a tissue swelling.
Aim:
• Decrease of pain.
• Elimination of toxins to:-
- Accelerate healing.
- Allows rapid penetration of antibiotic to the affected area.
Indications of (I&D)
➢Treatment of acute apical abscess.
➢Treatment of fluctuant , localized soft tissue swelling.
Generalized ,defuse, & indurated swellingSystemic antibiotic.Hot saline mouth wash.
The problems accompanying of ( I & D)
1) Optimal time to drain.
2) Obtaining adequate local anesthesia.
3) Maintain the drainage site.
Ideal time for drainage
When:-❑ The immediate area to be incised, should
feel soft under the finger tip.
❑ If pressure is exerted on one side &
transmitted through the fluid & felt as awave on the opposite side of the swelling.
❑ The apex of the swelling may appearwhitish or yellowish .

Problem???
I. Anesthesia
➢The presence of inflammation & swelling.
➢Injection into the region is painful due to pressure.
➢Fear of spreading of the infection.
Block anesthesia with topical anesthesia in the region.

1) topical disinfectant.

2) Administration of L.A

3) Perform a horizontal incision with a No. 11 scalpel which placed at base of
fluctuant area.

4) probing with hemostat into incisional wound to facilitate a more effective results.
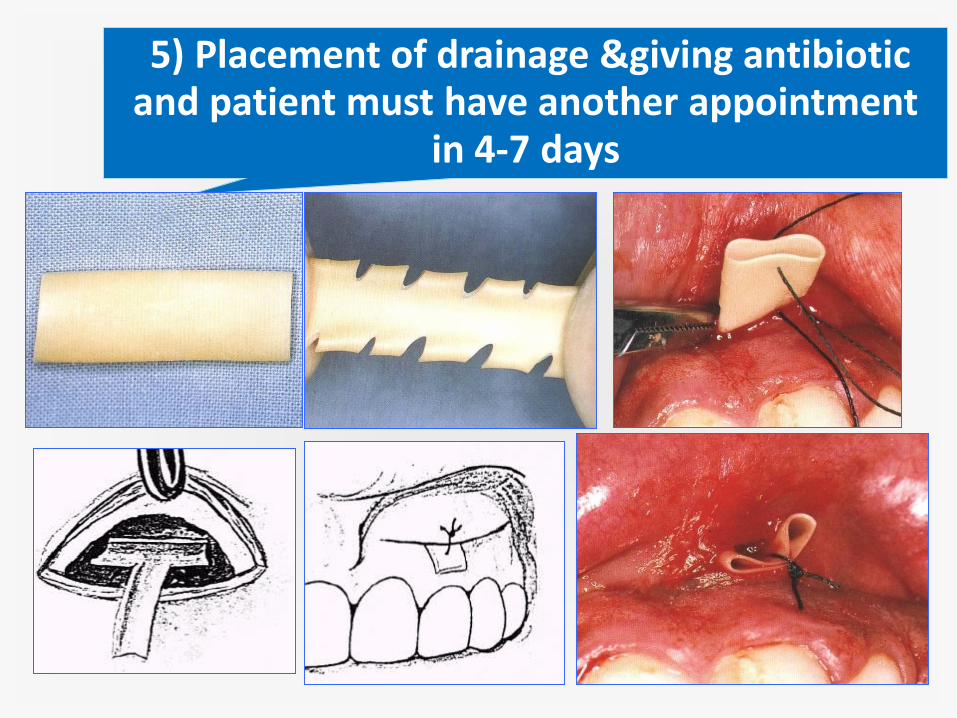
5) Placement of drainage &giving antibiotic and patient must have another appointment
in 4-7 days

6) Removing the rubber drain after 4-7 days.

Complete healing

2-TREPHINATION.
1-Apical Trephination
2-Cortical Trephination

1) APICAL TREPHINATION
➢ It is drainage through the root canal system.
➢ Penetration of the apical foramen with smallendodontic file and enlarging the apicalopening to #20 or #25 to allow drainagefrom the Periradicular lesion into canalspace.

2) CORTICAL TREPHINATION.
Definition:It is a procedure involving the perforation of the cortical plate
to release the pressure from the accumulation of exudates within alveolar bone

INDICATION OF TREPHINATION.
1) If the Apical fistulation fails to give sufficientdrainage & pressure remains within theperiapical bone.
2) Patients who present with sever pain butwith no intra oral or extra oral swelling.
3) When pain cannot be controlled byIntracanal procedures.

1)Giving local anesthesia.

2) The site of trephination should be as close as possible to the
apex of then offending tooth.
3) Semilunar flap is made through mucoperiosteal tissue opposite
to the apex of then offending tooth.
4) Reflect the flap & expose the area opposite to the root apex.

7) The trephination is initiated from buccal approach never from
lingual or palatal.
8) No.6 or No.8 a rose head surgical bur or fissure bur in high- speed
hand piece to penetrate or perforate the cortical plate as holes on
the periphery of the circle of 1 cm in diameter.
9) Use a fissure bur to connect between these holes & remove disc of
bone of 1 cm in diameter.

10) H or T is placed & sutured.
11) Giving antibiotic and patient return in 4-7days.
12) At the subsequent appointment the drain is removed and
apicoectomy with retrograde filling is performed.

Thank You