endocrine control of growth. endocrine glands pituitary anterior pituitary - oral ectoderm....
TRANSCRIPT
Endocrine Control of Growth

Endocrine glands
Pituitary
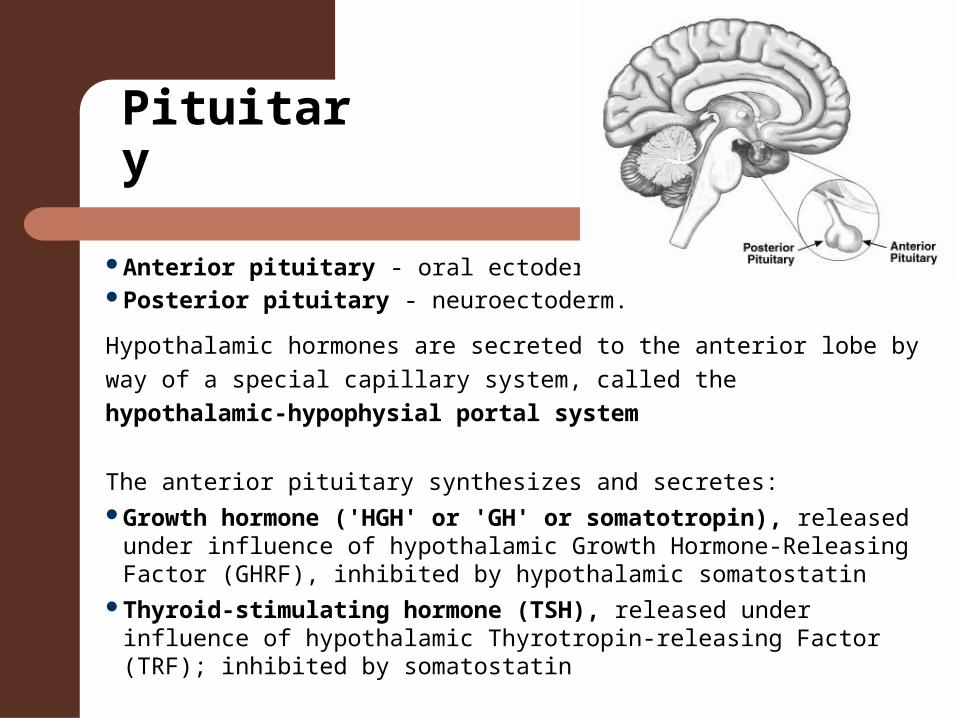
Anterior pituitary - oral ectoderm. Posterior pituitary - neuroectoderm.
Hypothalamic hormones are secreted to the anterior lobe by way of a
special capillary system, called the hypothalamic-hypophysial portal
system
The anterior pituitary synthesizes and secretes: Growth hormone ('HGH' or 'GH' or somatotropin), released under
influence of hypothalamic Growth Hormone-Releasing Factor (GHRF), inhibited by hypothalamic somatostatin
Thyroid-stimulating hormone (TSH), released under influence of hypothalamic Thyrotropin-releasing Factor (TRF); inhibited by somatostatin
Pituitary
Adrenocorticotropic hormone (ACTH), released under influence of hypothalamic Corticotropin-Releasing Factor (CRF)
Gonadotropins– Luteinizing hormone (also referred to as 'Lutropin'
or 'LH').– Follicle-stimulating hormone (FSH), both
released under influence of Gonadotropin-Releasing Hormone (GnRH)
Original Somatomedin Hypothesis
Insulin-like Growth Factor System
3 ligands– IGF-1 = Somatomedin-C– IGF-2– Insulin
6 binding proteins– IGFBP-1 to -6
Cell surface receptors that mediate the ligand action
Growth Hormone
Pulsatile secretion from anterior pituitary; maximum during early stages of deep sleep
Increases DNA synthesis and cell multiplication
Adequate levels of thyroid hormone required:"permissive"
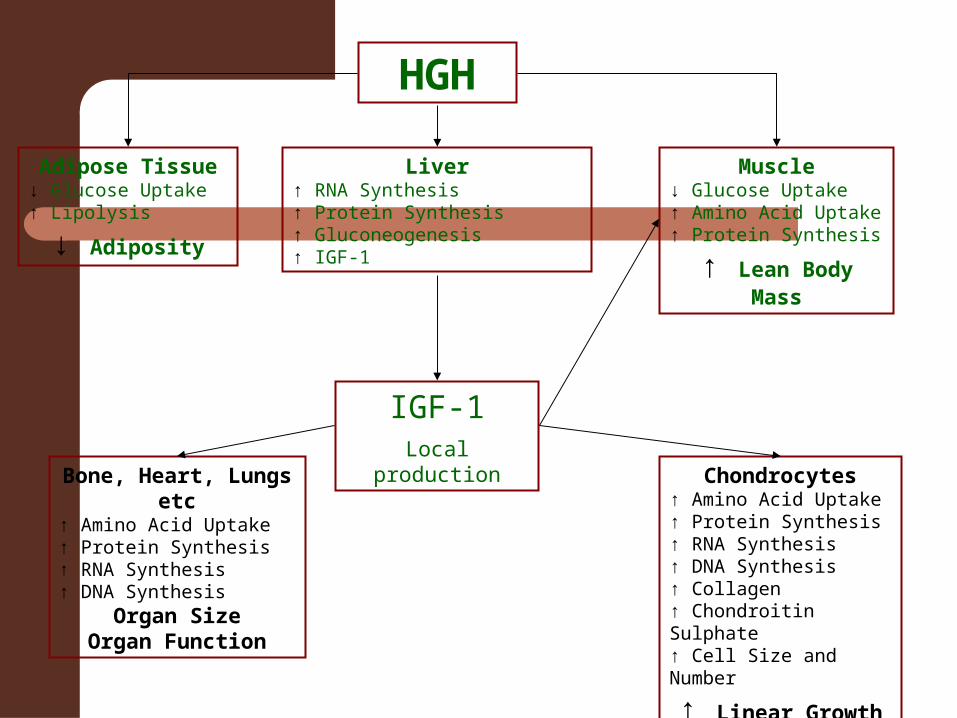
Adipose Tissue↓ Glucose Uptake↑ Lipolysis
↓ Adiposity
Chondrocytes↑ Amino Acid Uptake↑ Protein Synthesis↑ RNA Synthesis↑ DNA Synthesis↑ Collagen↑ Chondroitin Sulphate↑ Cell Size and Number
↑ Linear Growth
Bone, Heart, Lungs etc↑ Amino Acid Uptake↑ Protein Synthesis↑ RNA Synthesis↑ DNA Synthesis
Organ SizeOrgan Function
IGF-1Local production
Muscle↓ Glucose Uptake↑ Amino Acid Uptake↑ Protein Synthesis
↑ Lean Body Mass
Liver↑ RNA Synthesis↑ Protein Synthesis↑ Gluconeogenesis↑ IGF-1
HGH
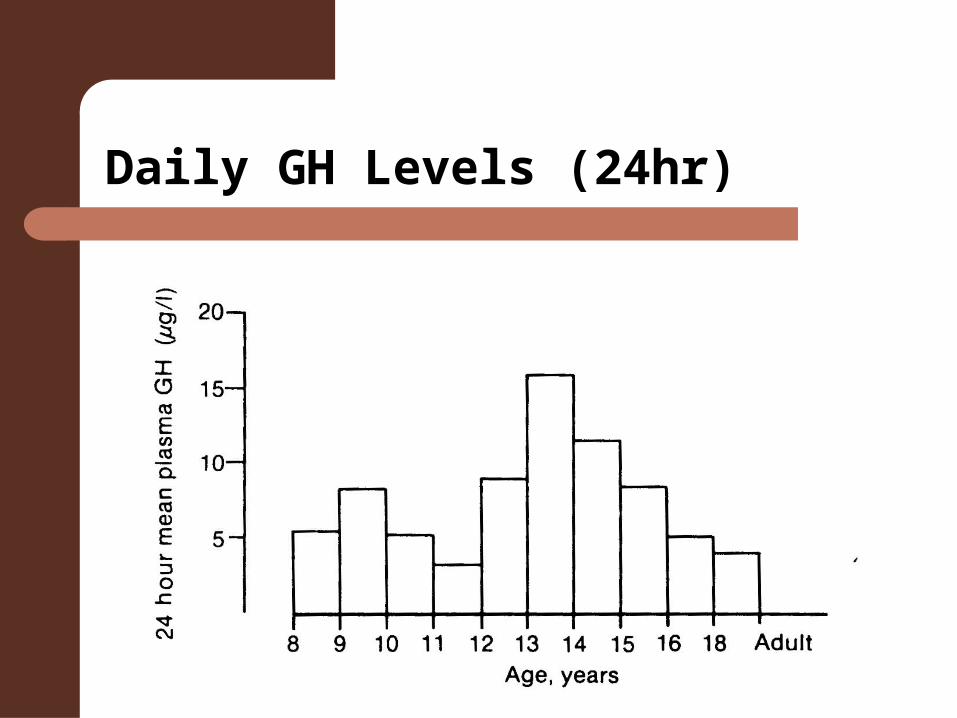
Daily GH Levels (24hr)
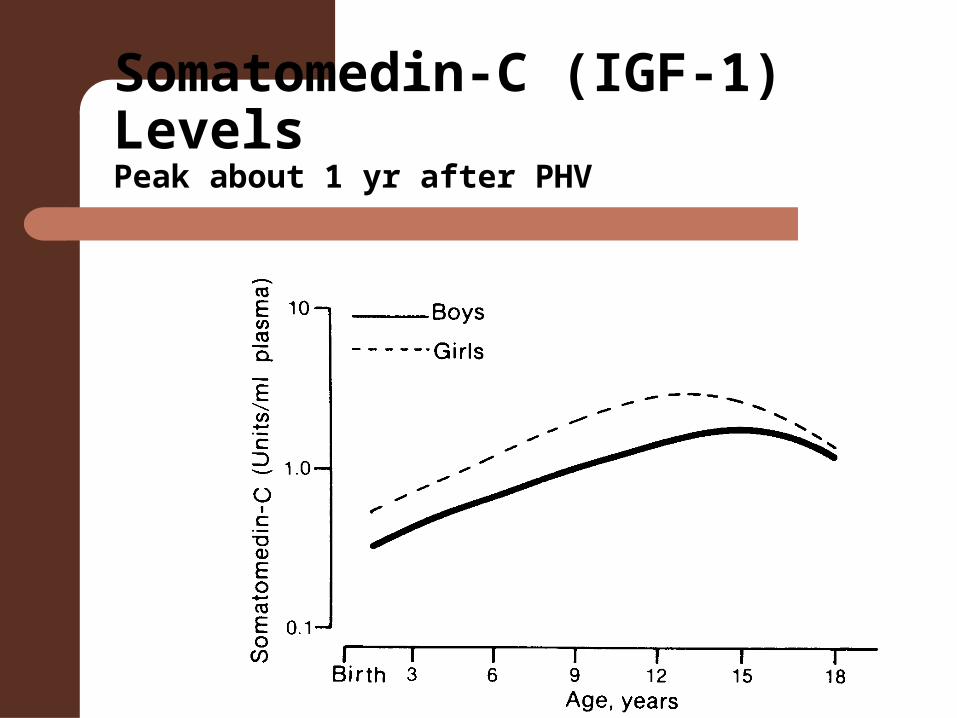
Somatomedin-C (IGF-1) LevelsPeak about 1 yr after PHV
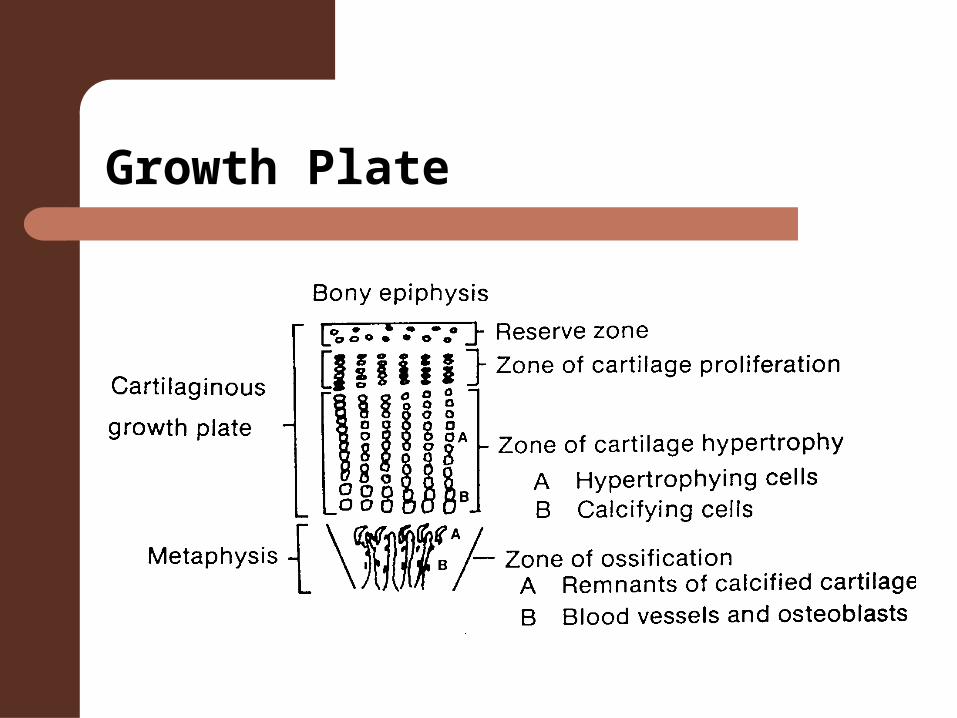
Growth Plate
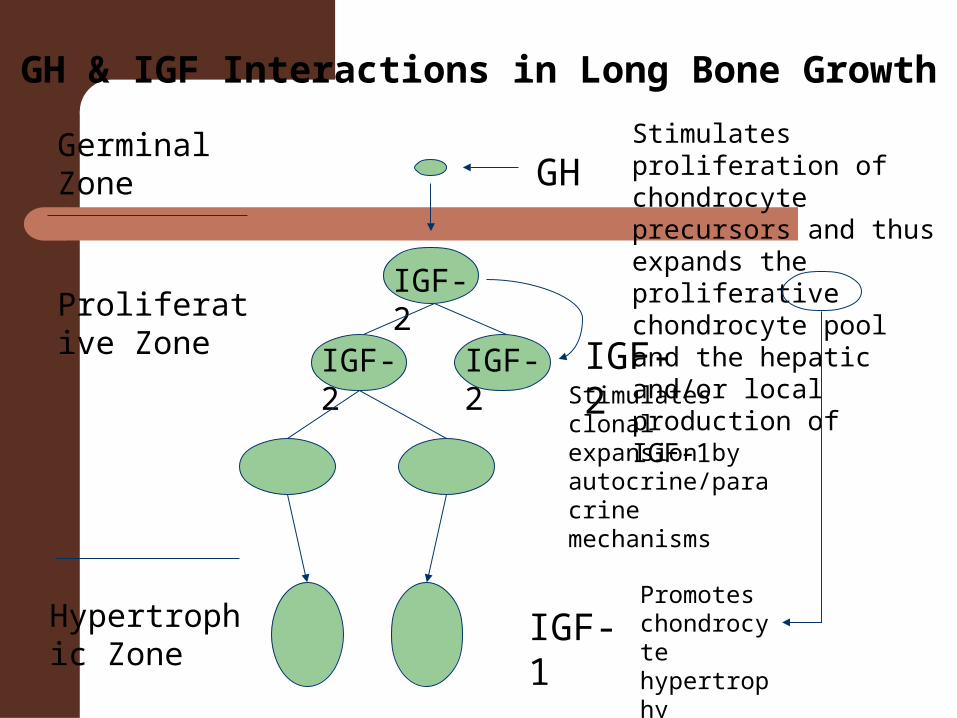
GH & IGF Interactions in Long Bone Growth
Germinal Zone
Proliferative Zone
IGF-2
IGF-2IGF-2
Hypertrophic Zone
Stimulates proliferation of chondrocyte precursors and thus expands the proliferative chondrocyte pool and the hepatic and/or local production of IGF-1
GH
Promotes chondrocyte hypertrophy
Stimulates clonal expansion by autocrine/paracrine mechanisms
IGF-2
IGF-1
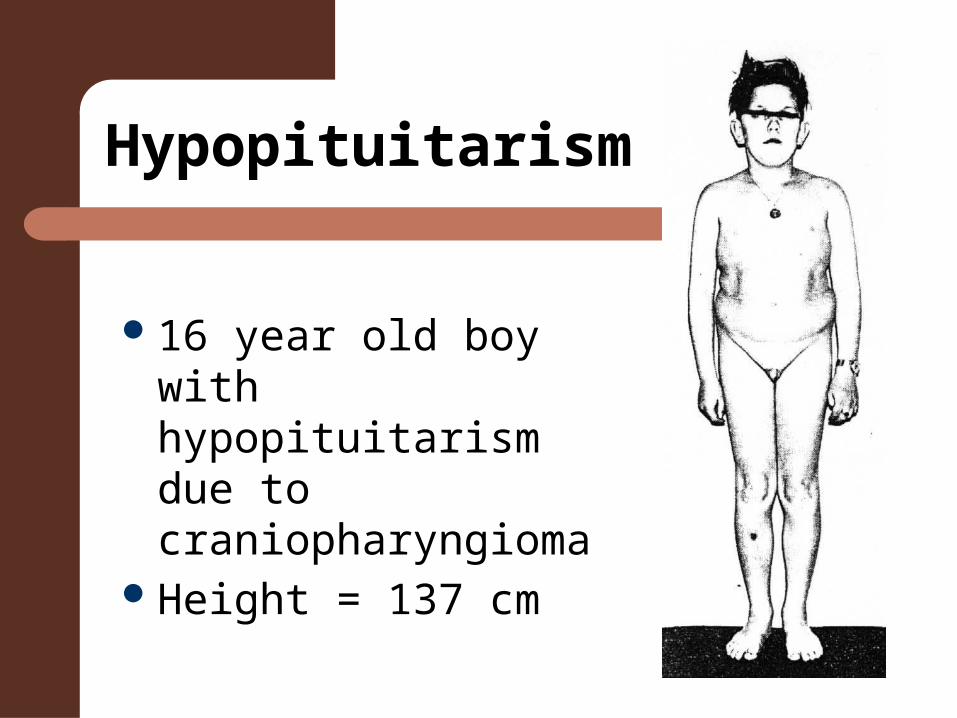
Hypopituitarism
16 year old boy with hypopituitarism due to craniopharyngioma
Height = 137 cm
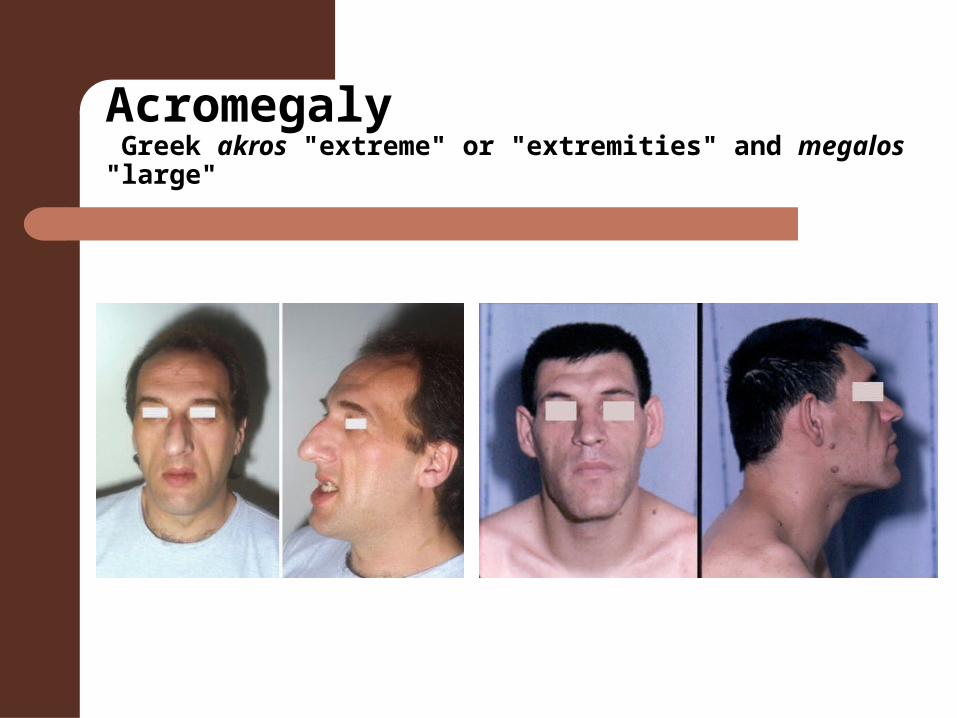
Acromegaly Greek akros "extreme" or "extremities" and megalos "large"
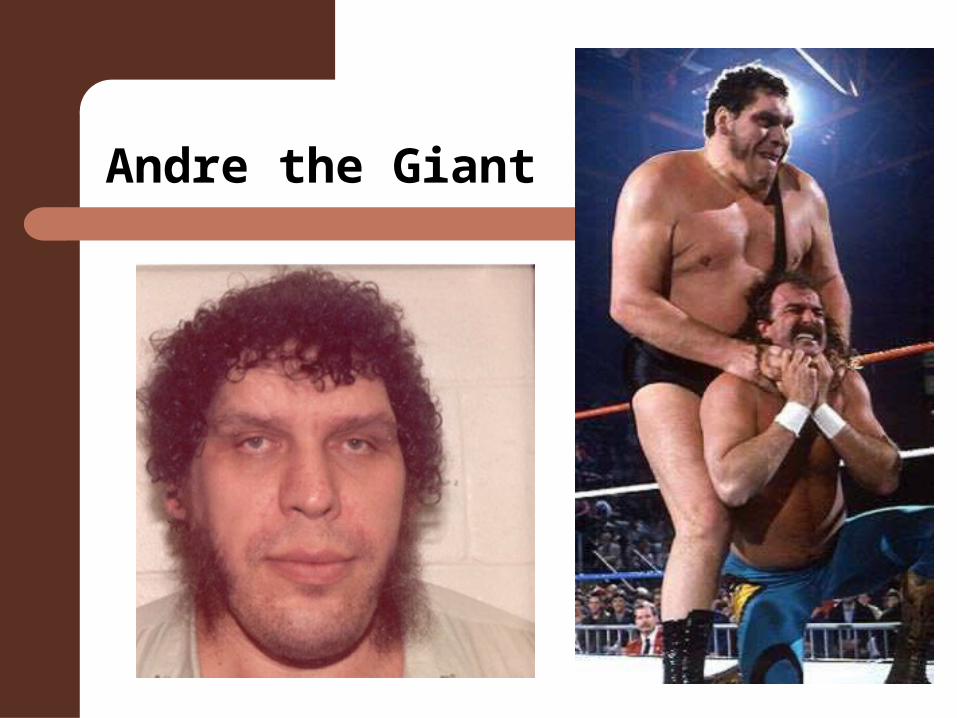
Andre the Giant
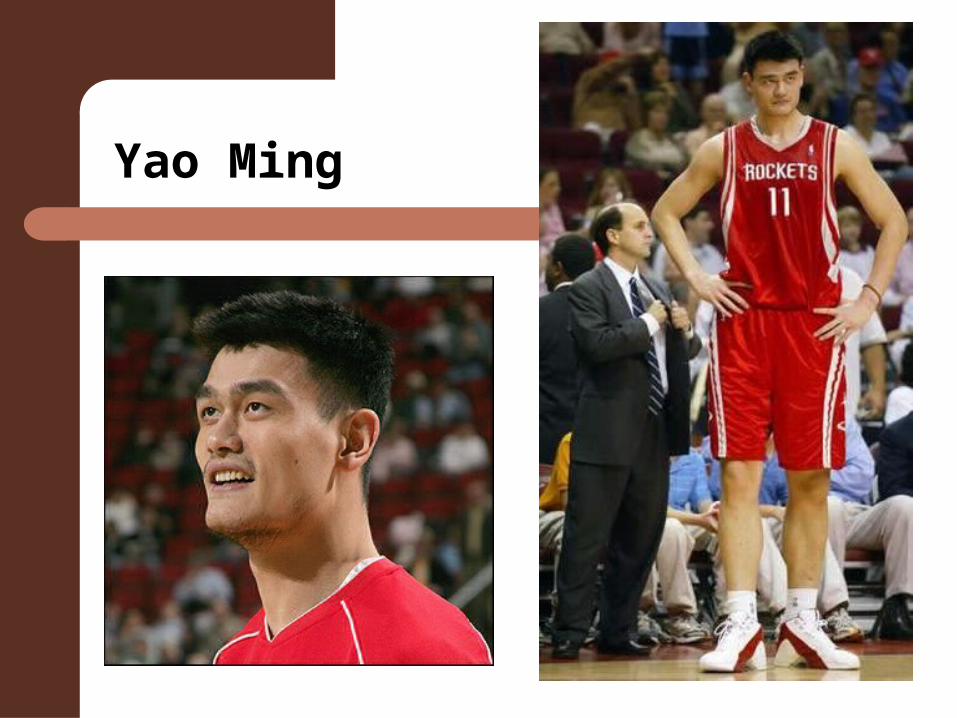
Yao Ming
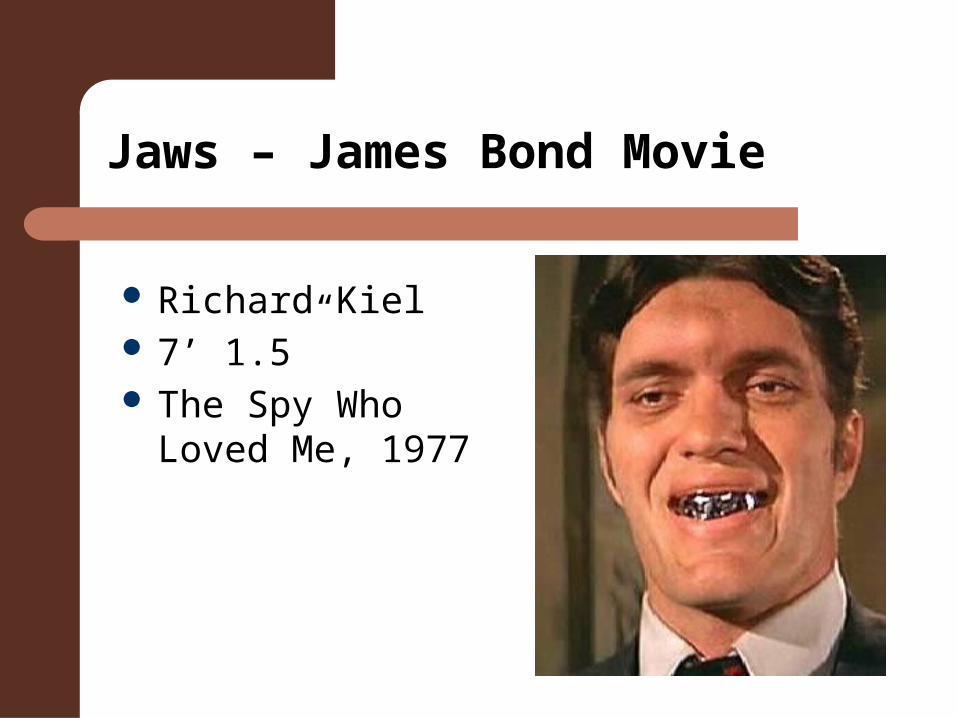
Jaws – James Bond Movie
Richard Kiel 7’ 1.5” The Spy Who
Loved Me, 1977
Thyroid
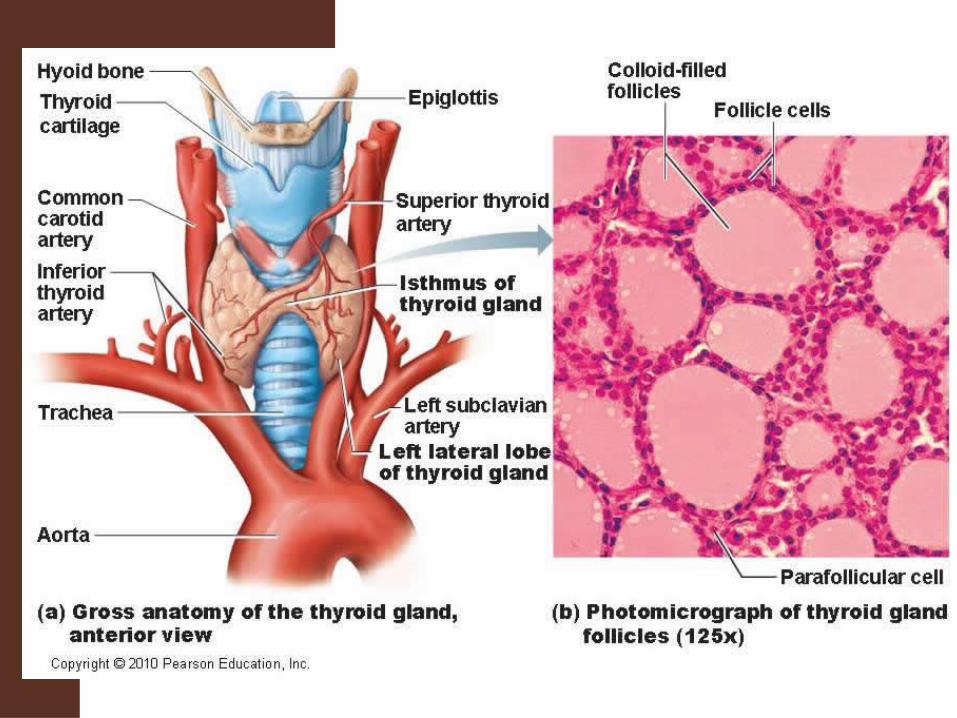
3–4 weeks of gestation, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue
Over the next few weeks, it migrates to the base of the neck, passing anterior to the hyoid bone.
Thyroid
Thyrotropin-releasing factor (TRF) and thyroid-stimulating hormone (TSH) start being secreted from the fetal hypothalamus and pituitary at 18-20 weeks of gestation
Fetal production of thyroxine (T4) reach a clinically significant level at 18–20 weeks.
Fetal triiodothyronine (T3) remains low until 30 weeks of gestation
Fetal thyroid hormones tend to protect the fetus against brain development abnormalities caused by maternal hypothyroidism.
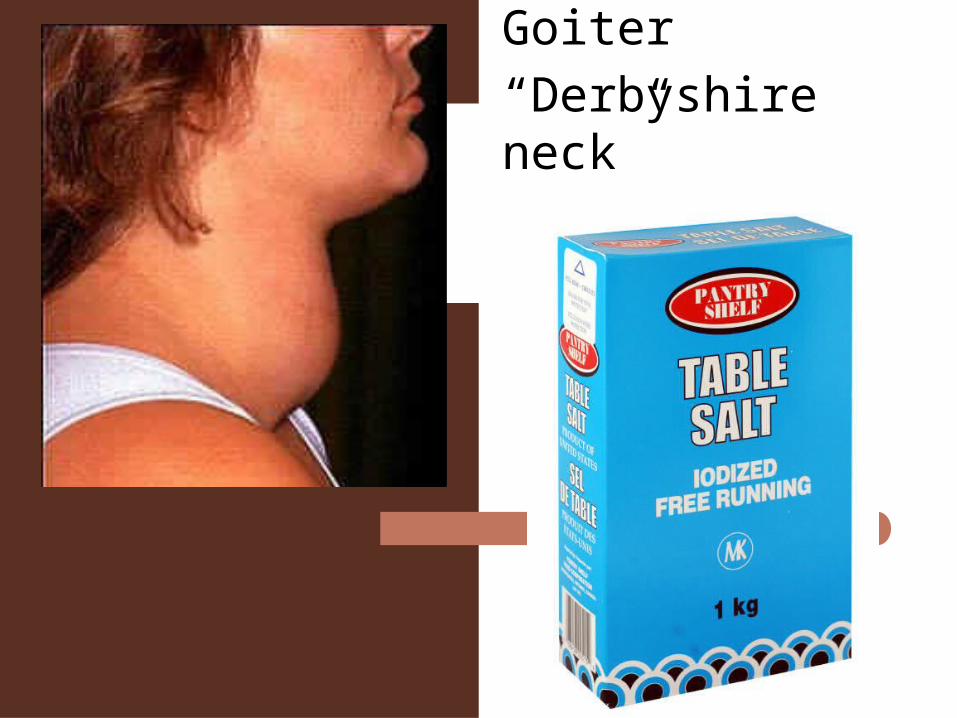
Goiter
“Derbyshire neck”
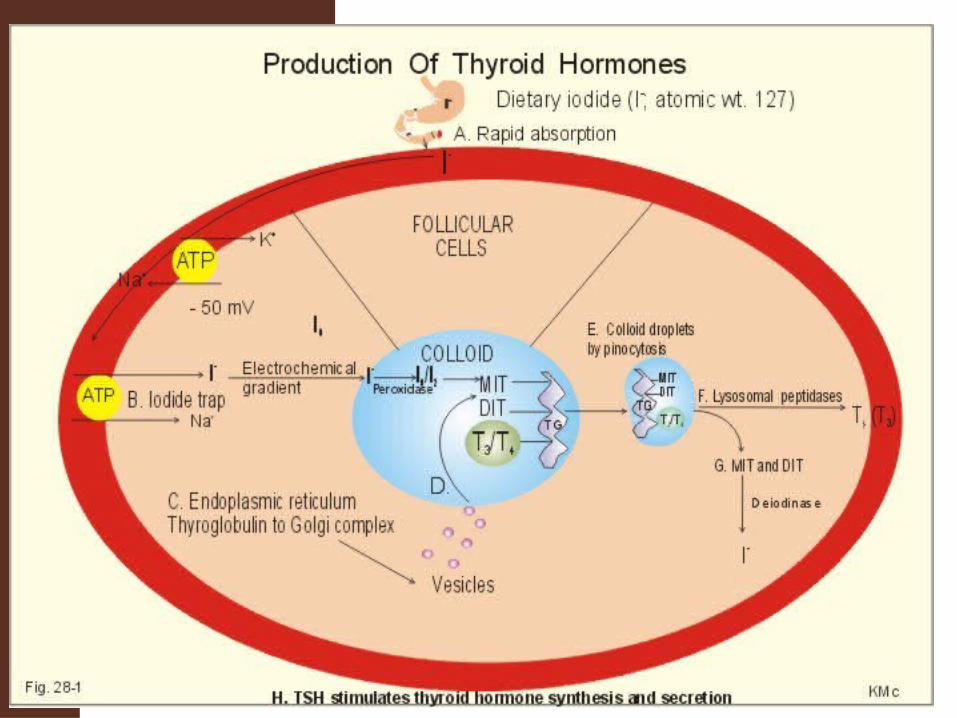
Thyroid Hormones
TSH (Thyrotropin) from Ant. Pituitary stimulates production of Thyroxine
Tri-iodothyronine is mainly produced in target peripheral tissues from Thyroxine
Tri-iodothyronine is more potent and rapidly acting being calorigenic (stimulate oxygen uptake and energy expenditure)
Thyroid Hormones
Essential for RNA synthesis Increase in metabolic rate Increased thyroxine causes:
– weight reduction; – increased heart rate and force of contraction; – increased nervous system activity
Thyroid Hormones
Cretins seldom appear hypothyrotic until several weeks after birth but do have retarded bone growth at birth
They can have irreparable brain damage although therapy was started within 1 or 2 months
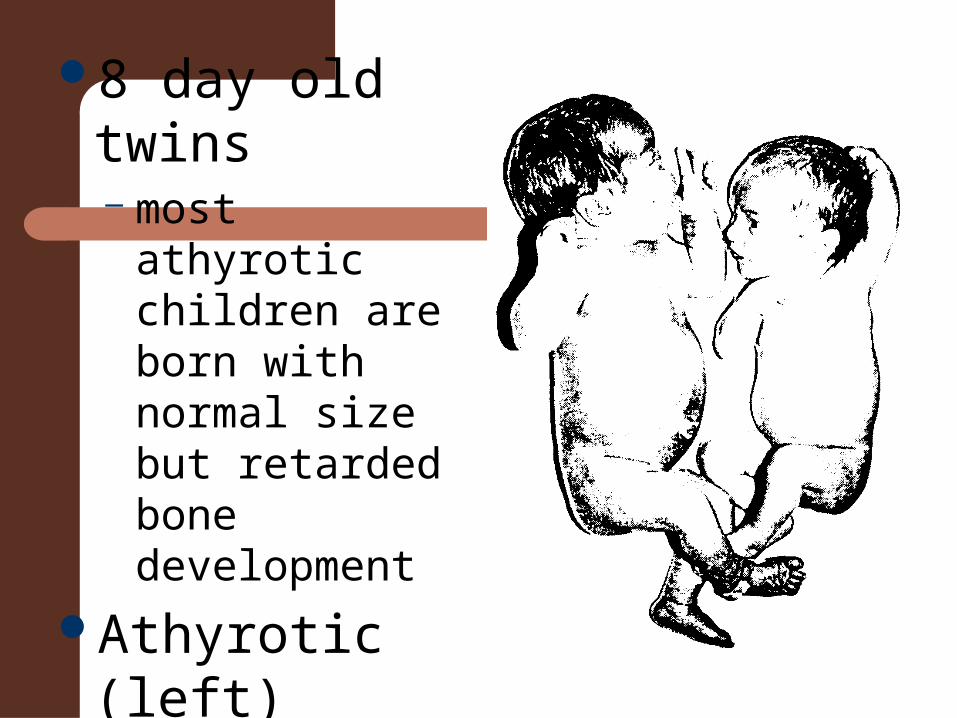
8 day old twins– most athyrotic
children are born with normal size but retarded bone development
Athyrotic (left) – 3.5 kg, 53cm
Euthyrotic (right)– 2.9 kg, 50cm
Hyperthyroidism
Graves’ disease– Autoimmune
disease– Exopthalmus
“bug-eyes”– High metabolic
Rate– Early death from
heart attacks
Marty Feldman
-”bug-eyed” British comedian
- Died at 39 of a heart attack
- Video– Young Frankenstein

Parathyroids
Parathyroids - Parathormone
Essential for regulation of calcium and phosphate metabolism
Particularly important for normal bone and tooth development
Maintains stable plasma calcium concentrations by stimulating osteoclastic activity
Thyrocalcitonin (from thyroid) has opposite effects
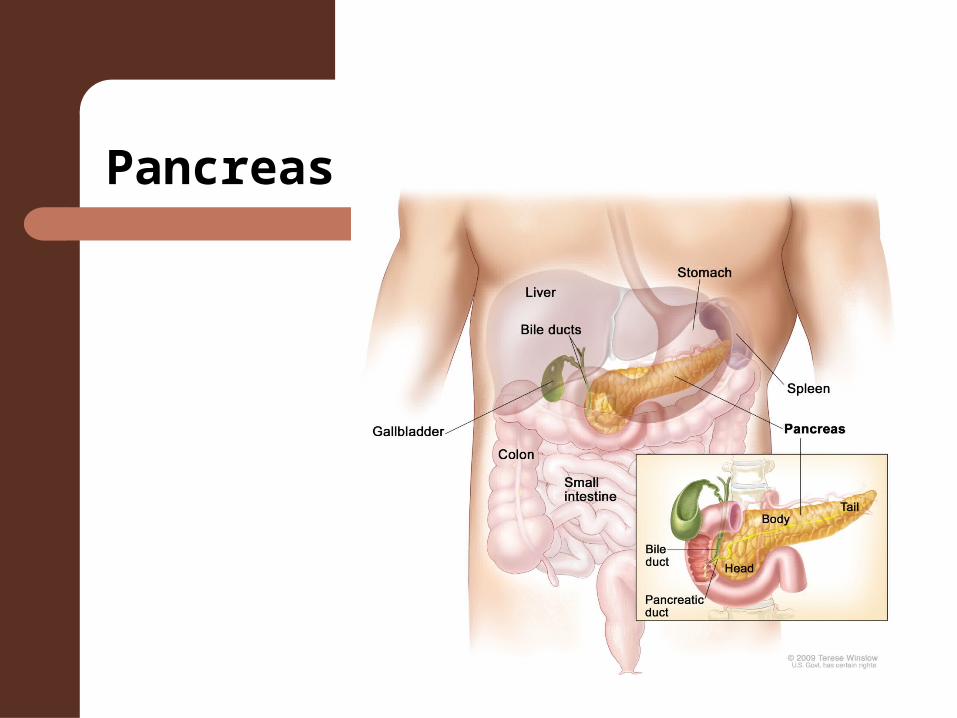
Pancreas
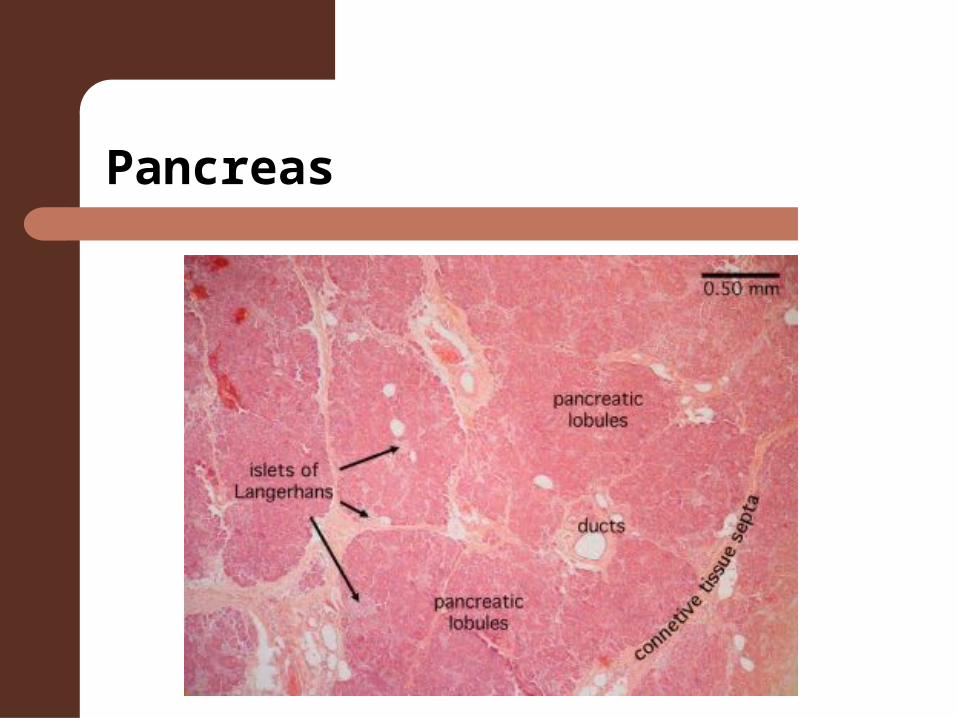
Pancreas
INSULIN
CARBOHYDRATES– used preferentially and excess is stored as fat
ABSENCE OF INSULIN– Fatty acids are mobilized and utilized in place of
carbohydrates
Potent effects of Insulinon Protein Metabolism
Increased rate of transport of amino acids through cell membrane
Increased formation of RNA Increased formation of protein by
ribosomes
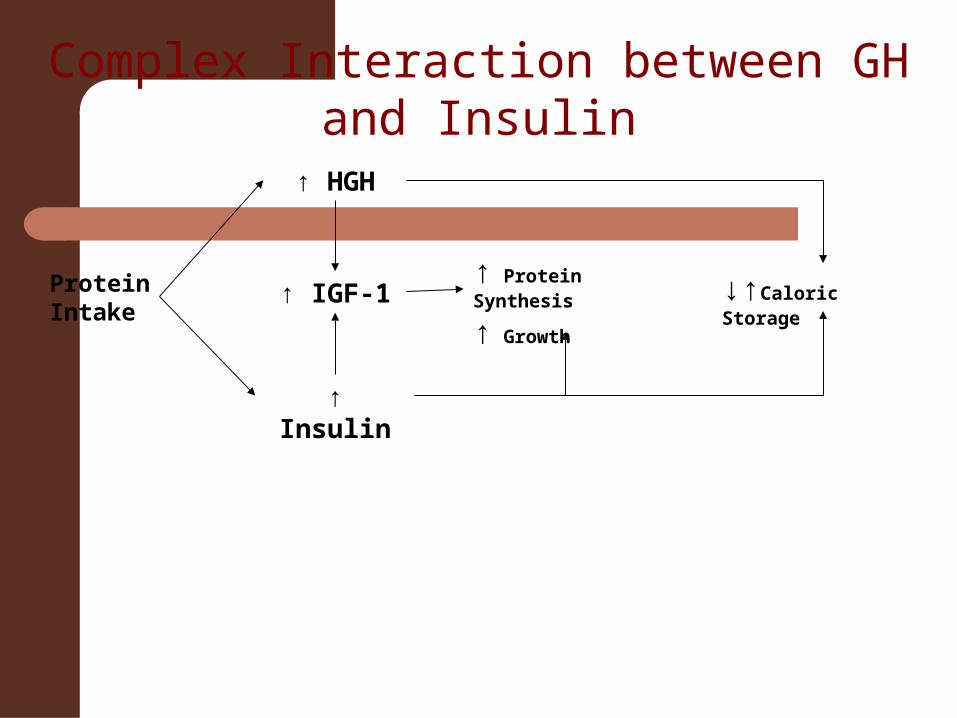
↑ HGH
↑ Insulin
↑ IGF-1↑ Protein Synthesis
↑ Growth
↓↑Caloric Storage
Protein Intake
Complex Interaction between GH and Insulin
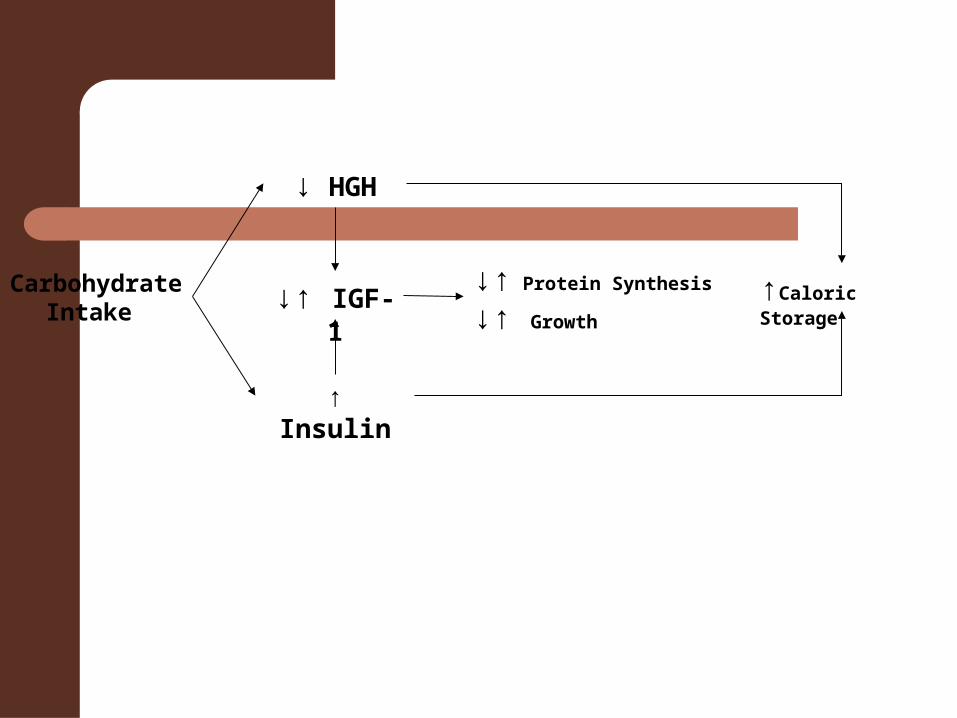
↓ HGH
↑ Insulin
↓↑ IGF-1↓↑ Protein Synthesis
↓↑ Growth
↑Caloric Storage
Carbohydrate Intake

↑ HGH
↓ Insulin
↓ IGF-1↓ Protein Synthesis
↓ Growth
↑Caloric Mobilization
Fasting
Insulin Imbalance
Insulin Deficiency• Can retard growth nearly as much as GH
deficiency
Hyperinsulinism• Can result in accelerated growth
– (but also accelerated maturity rate)
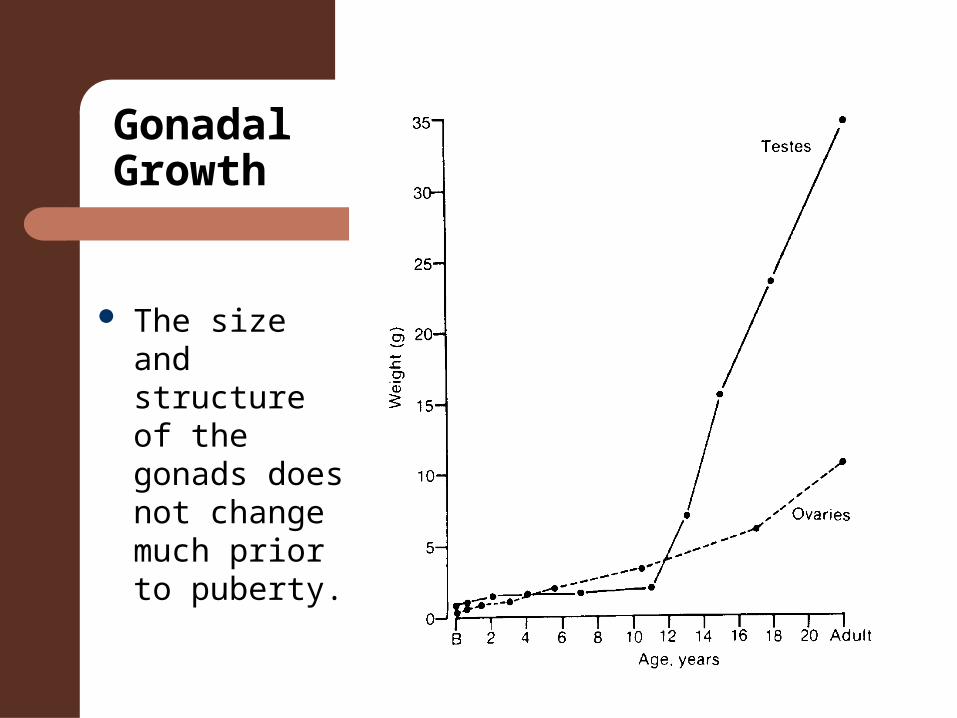
Gonadal Growth
The size and structure of the gonads does not change much prior to puberty.
Gonadal Hormones
Both sexes: Androgens & estrogens (adrenals) in small, constant levels in the urine
Gonadotrophins from Ant. pituitary stimulate development and function of the gonads
Androgens and Estrogens also produced by Adrenals.
Increased production at puberty.
Biological Activity of Androgens
Relative influence of gonadal or adrenal sources unknown.
Testicular androgens have greater biological activity than adrenal androgens– Young castrates: Adrenals not able to compensate for lost
testicular production IN FEMALES: After puberty most androgenic effects are
produced by the adrenals – Majority of testosterone produce in the liver
IN MALES: Testes secrete estrogens
Sexual Development
Males and females follow the same pattern of growth to 6 weeks of gestation
At 12 weeks sex can be determined by external appearance
Sexual Development
Removal of gonads leads to female developmentLocal application of high concentrations of androgens causes: –development of Wolffian elements; no effect on mullerian elements Destruction of one testis can lead to: –normal male development on unaffected side mullerian structures developing on affected side
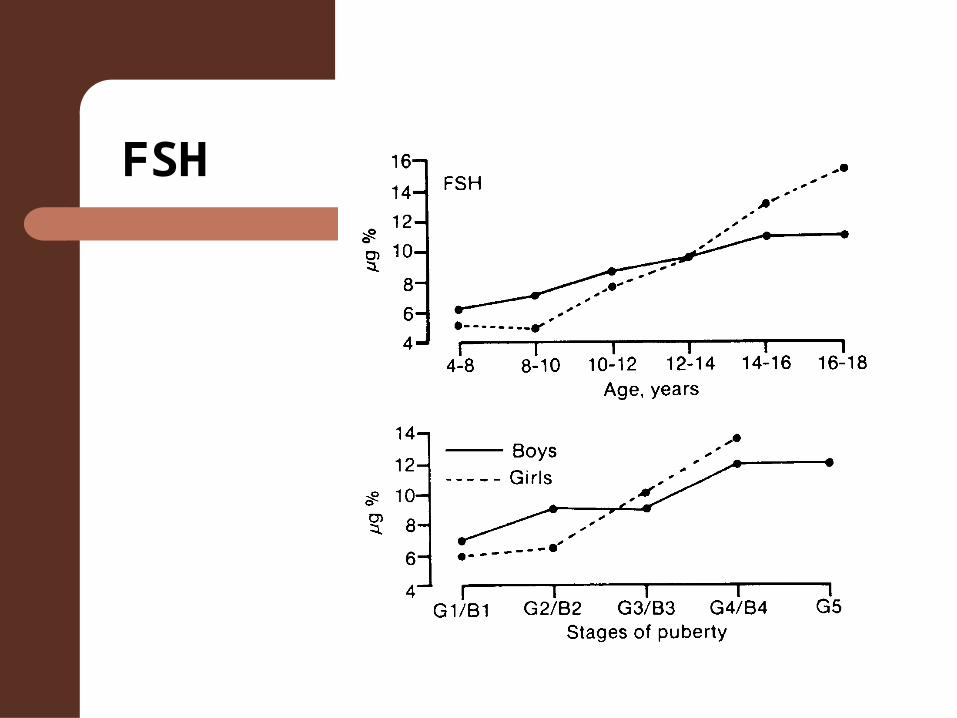
FSH
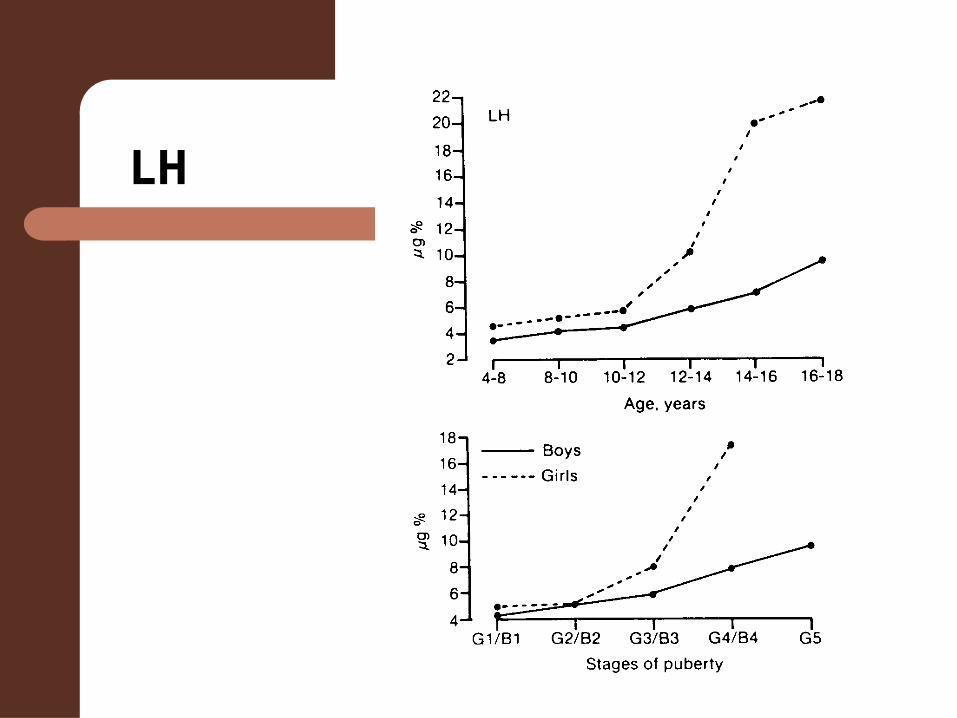
LH
Testosterone
FSH (ICSH (ant. pit.)) causes release of testosterone
Androgens are also produced by the testes
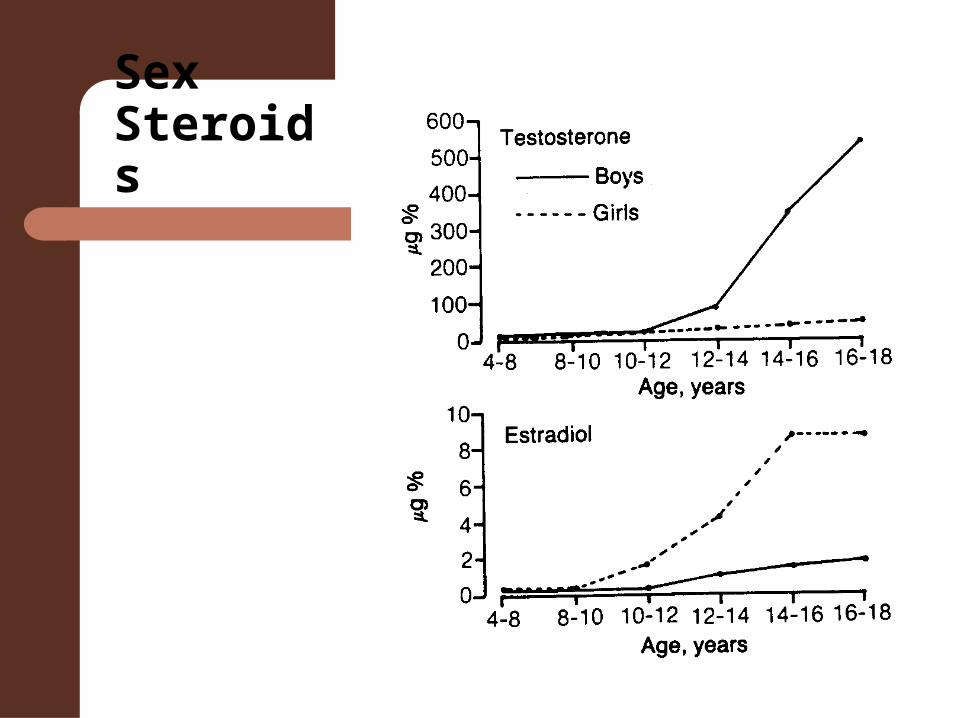
Sex Steroids
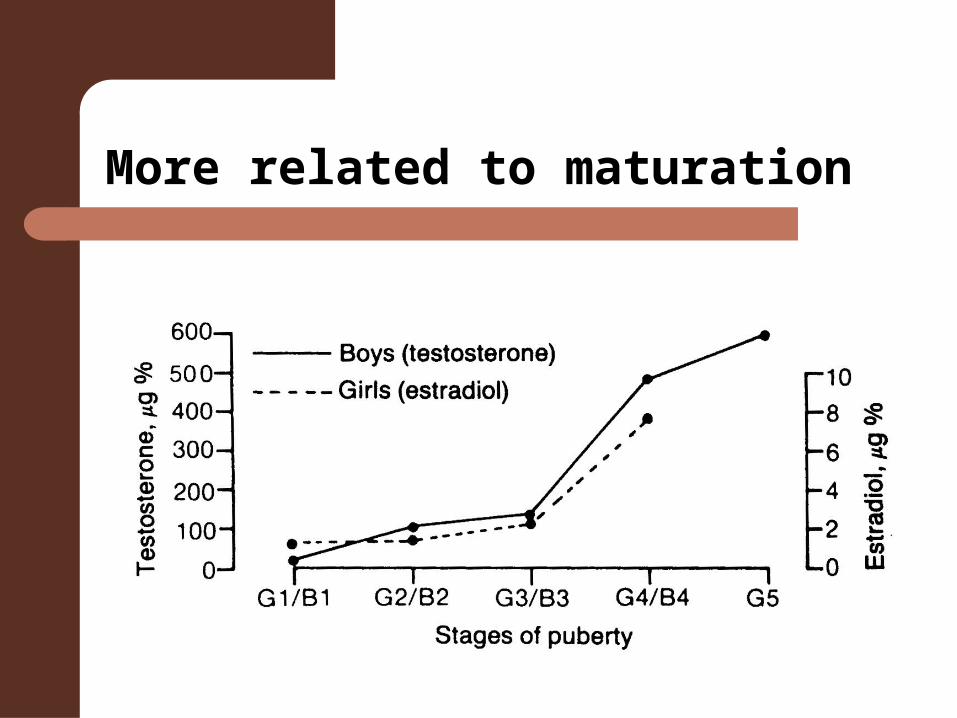
More related to maturation
Metabolic action of Testosterone
Protein anabolism dependent on critical level of insulin– increased protein formation – increased cholesterol, triglycerides and
F.F.A. production – decrease in phospholipids – increased retention of sodium, chlorides &
potassium – increased muscular development
Metabolic action of Testosterone
Increased rate of skeletal maturation and closure of epiphyses. – closure of epiphyses more affected than
linear growth – greater effect closer to puberty– facial development– Spermatogenesis complete 2 to 3 years
after puberty.
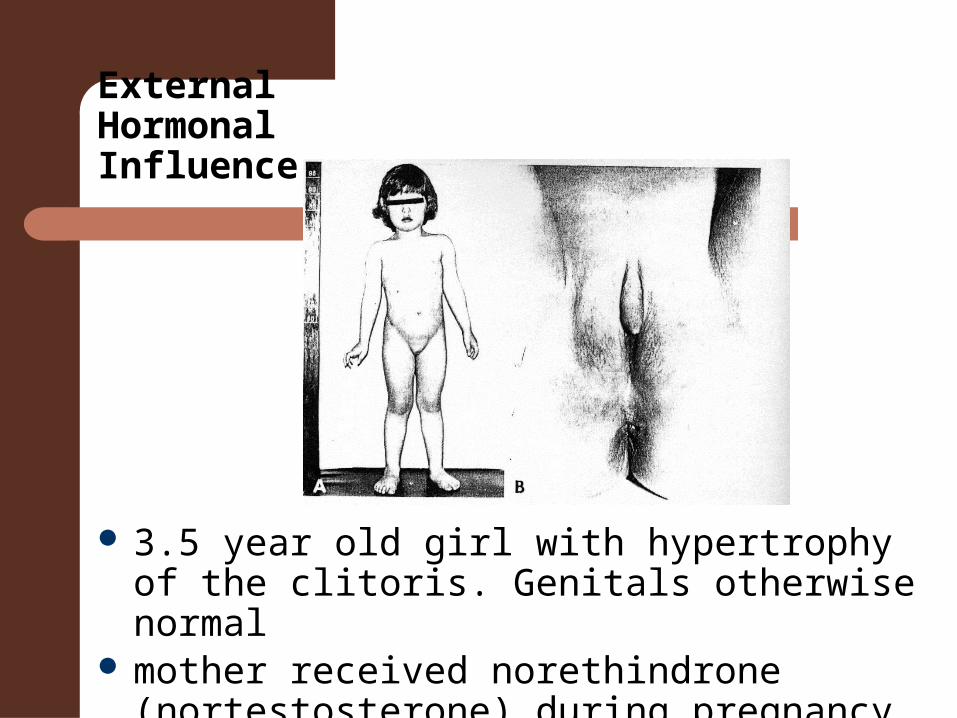
External Hormonal Influence
3.5 year old girl with hypertrophy of the clitoris. Genitals otherwise normal
mother received norethindrone (nortestosterone) during pregnancy for habitual abortion
Androgens
Larger more vascular penis Scrotum, prostate & seminal Vesicles Laryngeal development Genital and facial hair
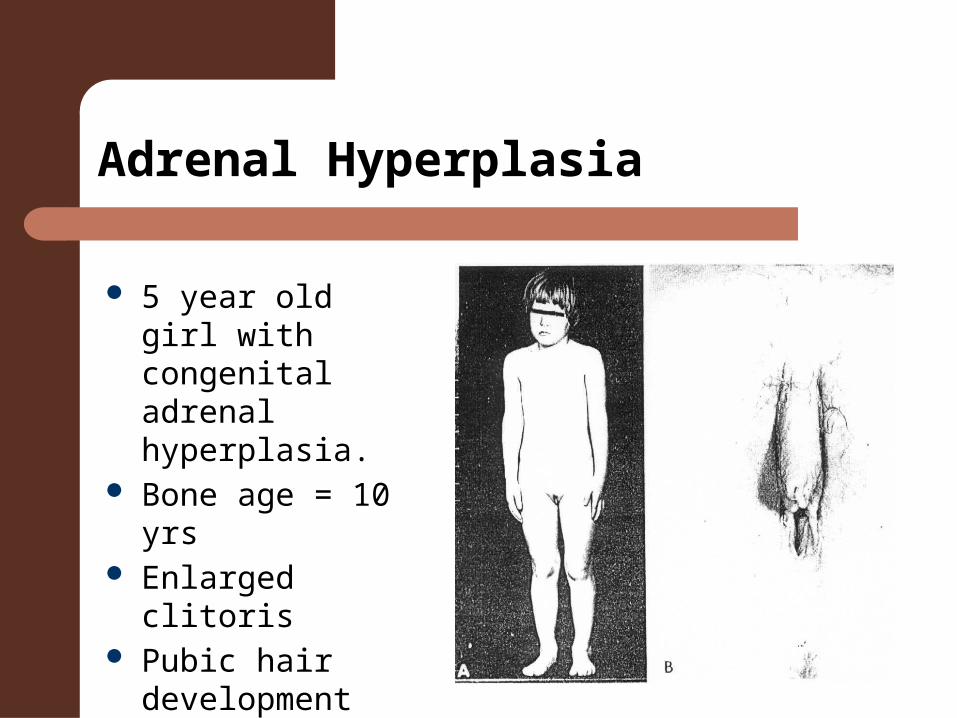
Adrenal Hyperplasia
5 year old girl with congenital adrenal hyperplasia.
Bone age = 10 yrs Enlarged clitoris Pubic hair
development
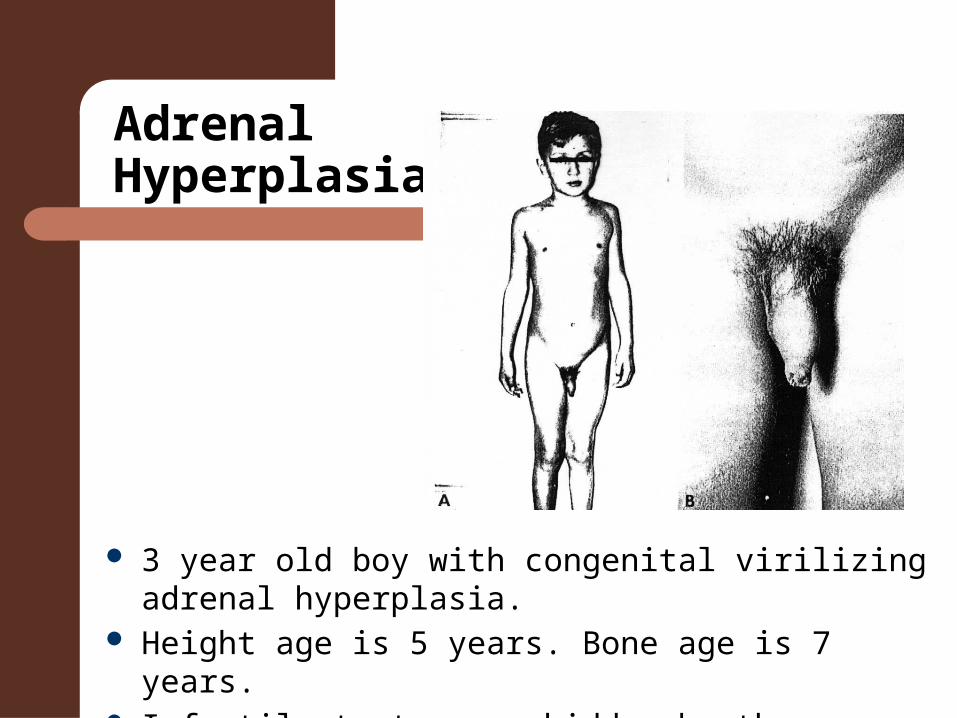
Adrenal Hyperplasia
3 year old boy with congenital virilizing adrenal hyperplasia.
Height age is 5 years. Bone age is 7 years. Infantile testes are hidden by the adolescent-sized penis
Estrogens
At puberty– Linear growth – Accelerate maturation of skeleton – Growth & development of genitalia– Increase lipid metabolism in adipose tissue – Breasts are earliest sign of puberty
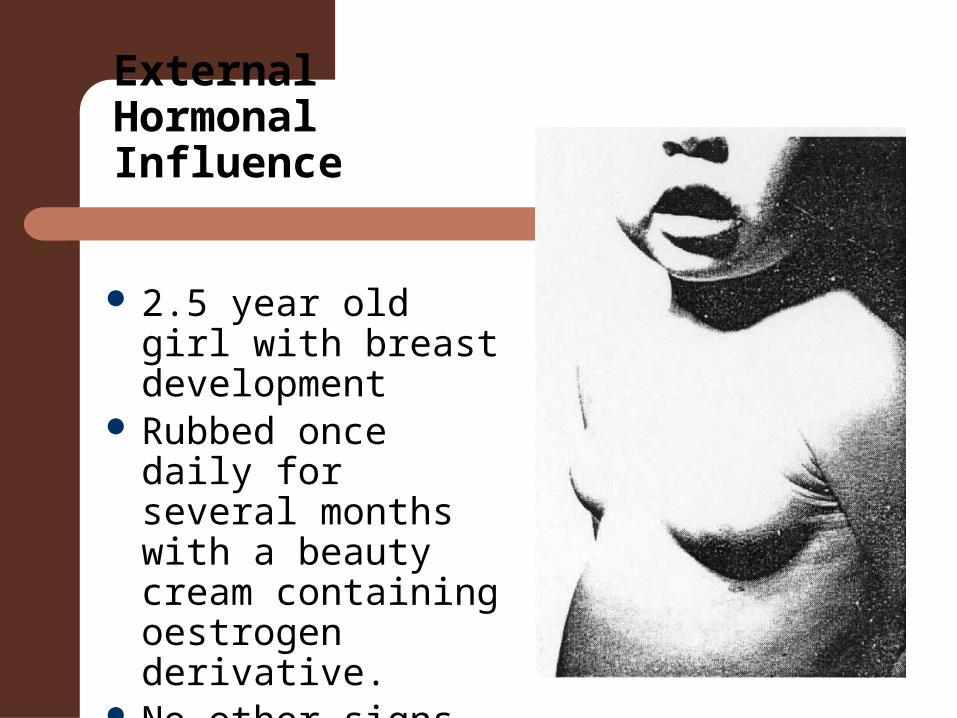
External Hormonal Influence
2.5 year old girl with breast development
Rubbed once daily for several months with a beauty cream containing oestrogen derivative.
No other signs of precocious puberty
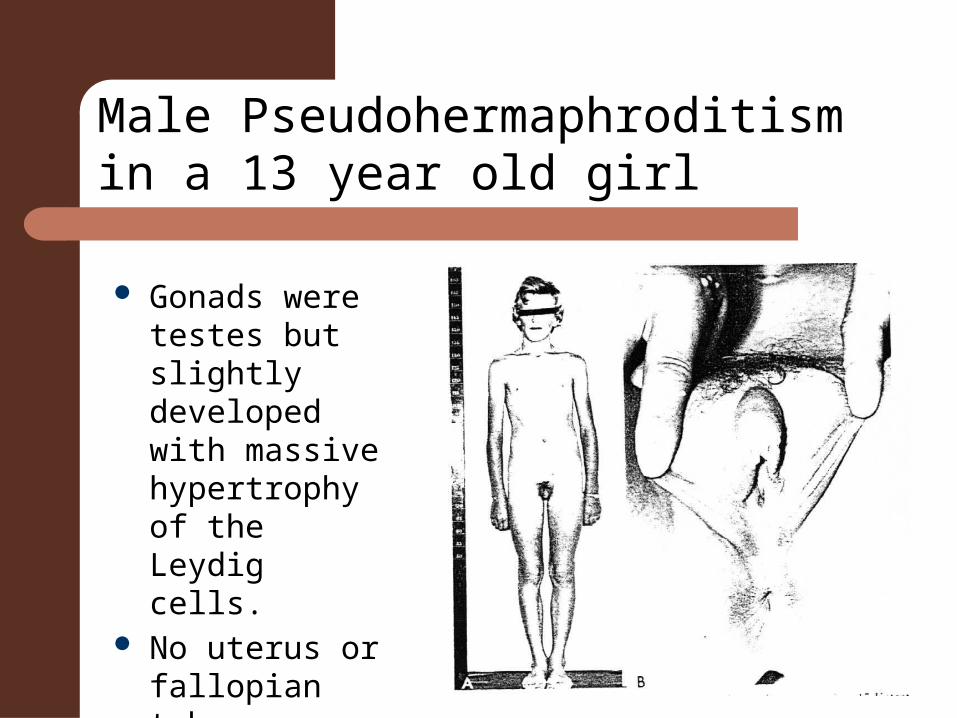
Gonads were testes but slightly developed with massive hypertrophy of the Leydig cells.
No uterus or fallopian tubes present
Male Pseudohermaphroditismin a 13 year old girl
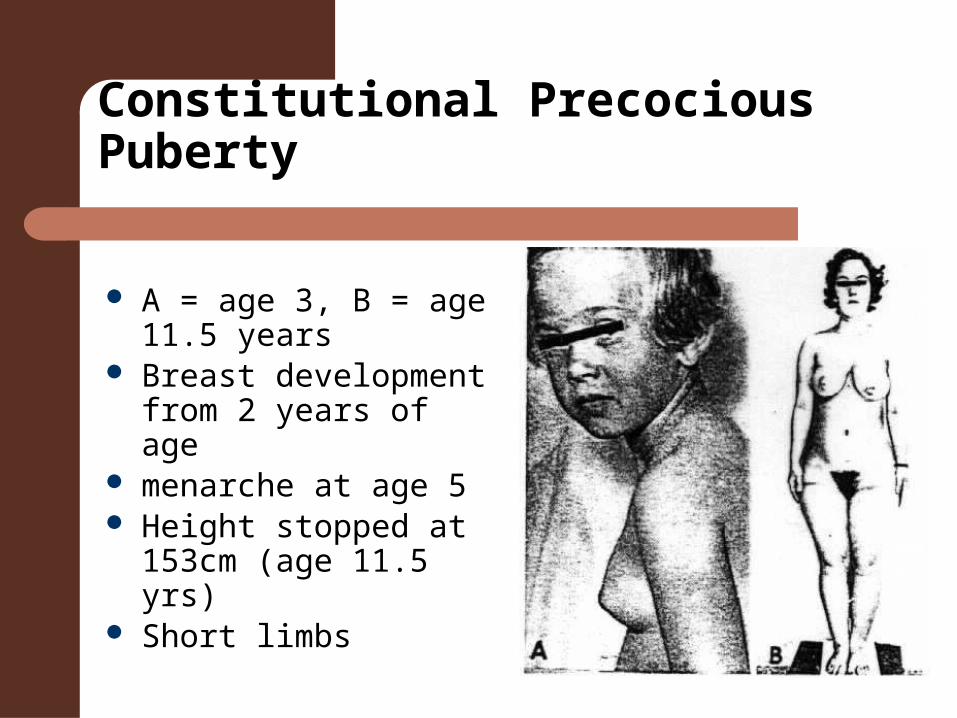
Constitutional Precocious Puberty
A = age 3, B = age 11.5 years
Breast development from 2 years of age
menarche at age 5 Height stopped at 153cm
(age 11.5 yrs) Short limbs

Precocious puberty
1.5 year old boy with precocious puberty caused by tumour of the third ventricle.
Puberal development began at 6 months of age
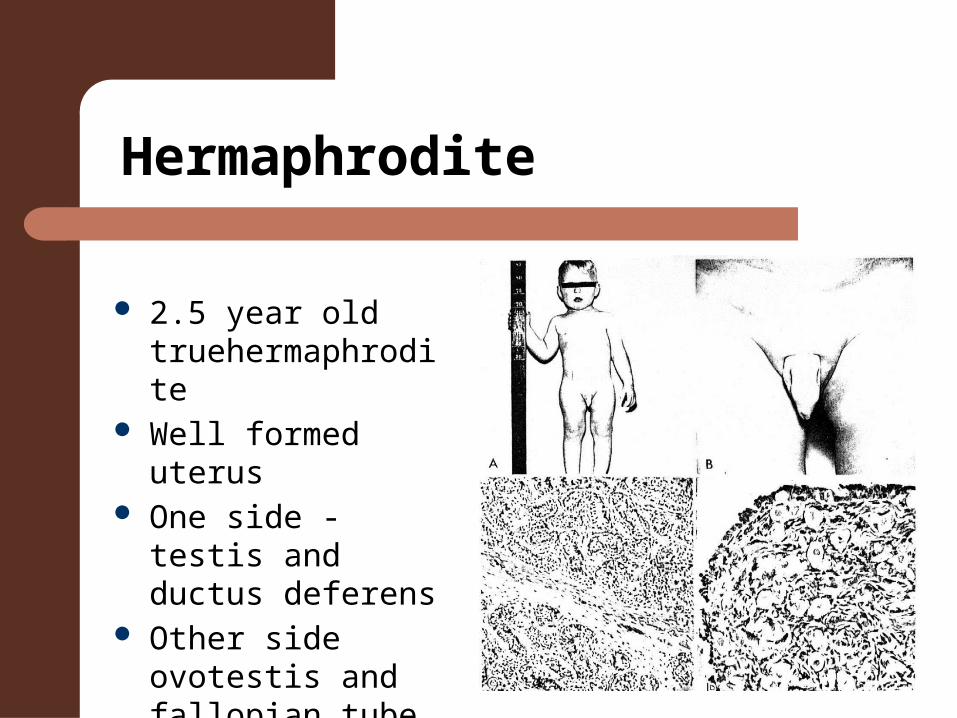
Hermaphrodite
2.5 year old truehermaphrodite
Well formed uterus One side - testis
and ductus deferens
Other side ovotestis and fallopian tube