emergency medicine and its future ... medicine and its future development in bangladesh by prof....
TRANSCRIPT

EMERGENCY MEDICINE AND ITS FUTURE DEVELOPMENT
IN BANGLADESH
BYPROF. MOHAMMAD OMAR FARUQ
MD, FACP, FACEP, FCPS(AMERICAN BOARD CERTIFIED IN INT. MEDICINE &
EMERGENCY MEDICINE)PROF. OF CRITICAL CARE MEDICINE,
BIRDEM.FEB 22, 2009

DO YOU RECOGNIZE THIS ROOM ?

DO YOU RECOGNIZE THIS WARD?
What you see are the two extremes of thespectrum of emergency care in Bangladesh
MEDICAL BASIS FOR EMERGENCY MEDICAL SERVICES
1. Emergency Cardiac Care2. Trauma Care3. Adult Medical Care4. Pediatric Care5. Rural EMS

PHILOSOPHY OF EMERGENCY CARE
Does it work in Bangladesh ?
A successful EMS system ensures that all individualshave access to emergency care regardless of theirability to pay or type of insurance coverage
An important principle of EMS is that all individualsdeserve timely access to the system when necessary
EMS (EMERGENCY MEDICAL SERVICE)
Constitutes the extension of emergencymedical care into the community involving thehospital and its emergency department

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
1. Personnel2. Training3. Communication4. Transportation5. Facilities6. Critical Care units7. Public safety agencies8. Access to care9. Transfer of care10. Public information and education11. Disaster linkage

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Personnel:
EMT Citizen volunteers etc.

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Training:
FR (First Responder) eg. Police, Firefighters
EMT (Emergency Medical Technicians)
EMT.B (Emergency Medical Technician Basic)
EMT.I (Emergency Medical Technician Intermediate)
EMT.P (Emergency Medical Technician Paramedic)

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Communication:
911 in USA, Canada 000 in Australia 999 in U.K. 112 in E.U.
What about Bangladesh ?

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Transportation:
Ground Ambulances BLS Ambulances ALS Ambulances Air Transport

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Facilities:
Closest appropriate hospital Designated trauma centers

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Critical Care Units:
Tertiary care facilities for: Trauma Neonatal Intensive Care High Risk Obstetrics Burns Neurosurgical and Cardiac Care

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Public Safety Agencies:
Police Department Fire Department

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Access to Care:
Regardless of ability to pay Timely access

LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Transfer of Care:
From one facility to another facility
LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Public Information and Education:
How to use the system
LOCAL ROLE IN EMERGENCY MEDICAL SERVICES
Disaster Linkage:
Integral part of disaster preparedness Involves in planning and practice drills

EMERGENCY ROOM IN BANGLADESH
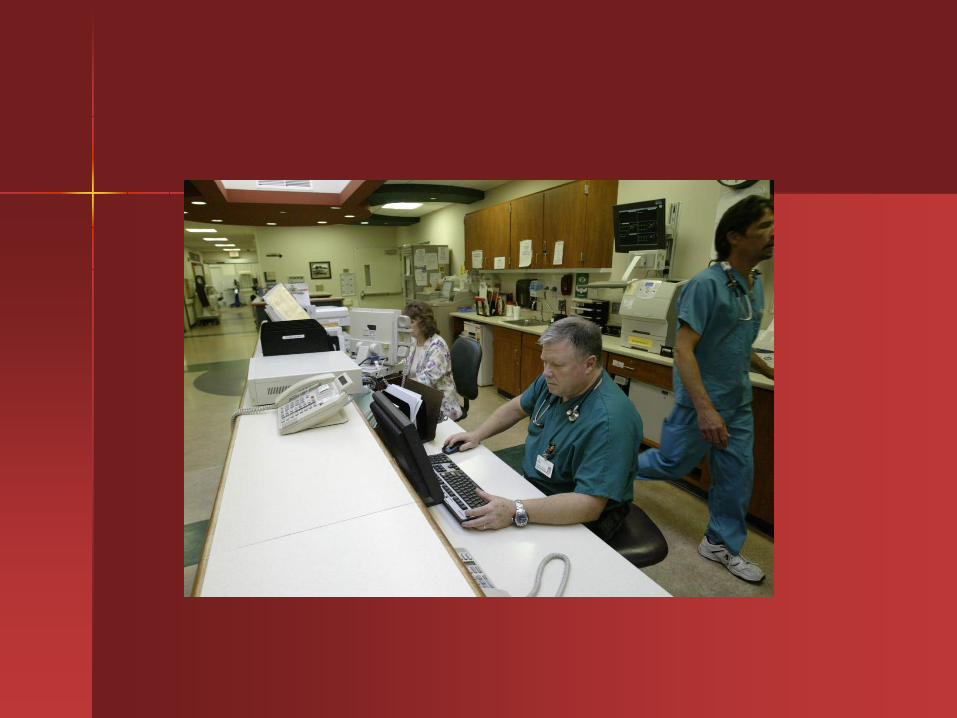
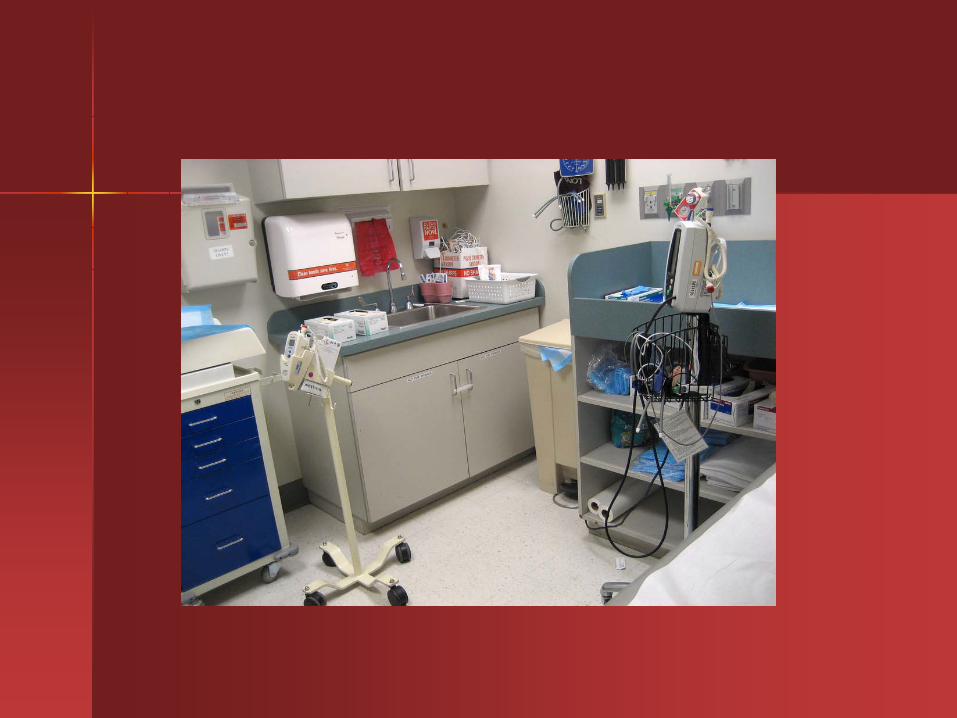
Typical Emergency Room in a Western Country



FACTS ABOUT BANGLADESH
Emergency Facilities are urban centered Semi-urban facilities are less adequate Rural facility absent

FACTS ABOUT BANGLADESH
Our only hope in a large city is the Medical CollegeHospital Emergency Room
TYPICAL SCENERIO IN A MEDICAL COLLEGE HOSPITAL ER
EMO triages the patient and hurriedly admits thepatient into different services after filling out theadmission form
First aid/minor laceration attended upon During day patient may be referred to O.P.D. Arrested patients are usually pronounced dead or
sent to inpatient for resuscitation


TYPICAL SCENERIO IN A MEDICAL COLLEGE HOSPITAL ER
The luckiest patient is someone who is seen by thedepartmental professor or consultant, who happensto be there at the right time
TYPICAL SCENERIO IN A MEDICAL COLLEGE HOSPITAL ER
There is nothing called “NO VACANCY” All admissible patients will be admitted If the ward is full they will be kept lying on cement
floors of wards, corridors or even the lobby areas

TYPICAL SCENERIO IN A MEDICAL COLLEGE HOSPITAL ER
In the worst situation, patients’ family may be told totake patient elsewhere as patient care facility is notavailable

SCENERIO IN A PRIVATE CLINIC/ HOSPITAL
Patient is either admitted directly or told to go toanother facility/specialty Government facility
If he is poor, told to go to MEDICAL (Medical CollegeHospital).

FACT FINDING:DHAKA MEDICAL COLLEGE HOSPITAL
1200-1500 BED INPATIENTER:
Daily census:600-700 Yearly census:219000-255500 In-charge: Trauma RS On duty EMO:2-3 per shift No CPR facility No cardiac monitoring or ECG No other lab facility Nebulisation facility for asthmatic Gastric lavage for poisoning Hospital has ICU/CCU.


OBSERVATION ROOM






FACT FINDING:IBN SINA HOSPITAL180 BED INPATIENT
ER: Daily census:30 Yearly census:11000 No on duty doctor, on call doctor available In-charge: S.M.O on duty CPR done with help of ICU doctors Defibrillator available Hospital has ICU



FACT FINDING:BIRDEM HOSPITAL
500 BED INPATIENTER:
Daily census:150(includes walk in D.M patients) Yearly census:48000 On duty EMO:2 per shift In-charge: RP CPR done with the help of ICU doctors Defibrillator out of order Nebulisation facility available Hospital has ICU/CCU







FACT FINDING:SQUARE HOSPITAL
280 BED INPATIENTER:
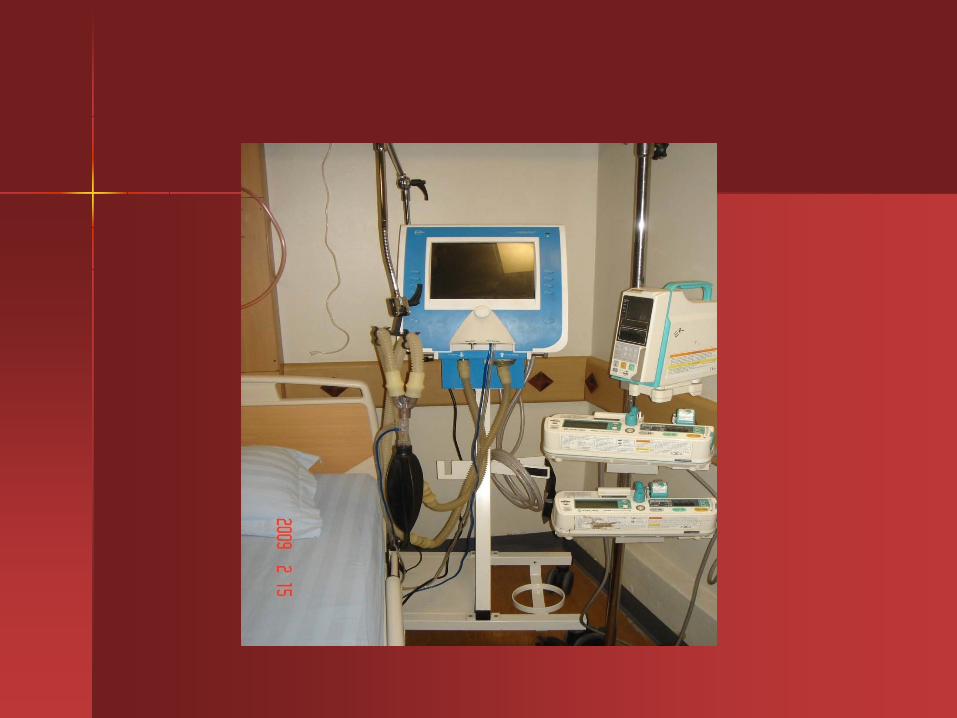
Daily census:40 Yearly census:15000 In-charge: Consultant Pediatrics surgery On duty EMO:2-3 per shift CPR (ACLS) done in ICU Cardiac monitor in all beds, portable X-ray available Mini O.T Observation room Mechanical ventilator Most staff CPR trained Hospital has ICU/CCU

SQUARE HOSPITAL






Floor space of DMCH ER and Square ER are almostsame
However, DMCH handles 700 patients per day, whereas Square handles only 40 patients a day
Please compare resource and service allocation perER patient between the two
Please comment on the disparity

IS AN EMERGENCY ROOM A
Glorified Walk in Clinic orA Triage Center orA First Aid Station ?

WHAT IS NEEDED IN AN IDEAL E.R OPERATION
Prompt triaging. Trained manpower : Credential of doctors & nurses
Space, equipment, supplies Backup consultation services Critical care facilities: ICU, CCU CME Organized EMS system

TRAUMA CARE IN BANGLADESH
Our country is famous for road traffic accidents

TRAUMA CARE IN BANGLADESH
We need Trauma centers:
Level I Level II Level III Level IV
LEVEL I: TRAUMA CENTER
Provides the highest level of surgical care to traumapatients
It has a full range of equipments 24 hours a day Has an education program, preventive and research
program

LEVEL I: TRAUMA CENTER
24 hour in house coverage by general surgery and prompt availability of care in varying specialties like:
Orthopedic surgery Neurosurgery Plastic surgery Anesthesiology Emergency medicine Radiology Internal medicine Oral & maxillofacial Vascular surgery


Level I & II do not exist in Bangladesh
DMCH is the only officially recognized trauma unit inthe whole country
It has a separate burn unit It can be labeled at somewhere between level III &
level IV
NITOR (Pongu Hospital) claims to be a traumacenter, but it is not so

TRAUMA WARD OF DMCH

Our best bet is in developing primary, secondary &tertiary care hospitals within the Government healthcare system, using the medical college hospitals astertiary care hospitals and as level III Trauma center
To develop DMCH, CMCH, RMCH, SMCH as theregional level I & II trauma centers

REGIONAL TRAUMA CENTERSIN BANGLADESH (proposed)

Do you know that department of Roads & Highways(Ministry of Communication) oversees planning fortrauma care in Bangladesh?

Proposal for establishment of an Acute Trauma Care Center in Bangladesh


DISASTER MANAGEMENT
Disaster Management is the discipline that involvespreparing for disaster before it occurs & disasterresponse when it occurs.

DISASTER MANAGEMENT IN BANGLADESH
Role of EMS system


4Rs OF DISASTER MANAGEMENT
Reduction = Mitigation Readiness = Preparedness Response Recovery
IN COLLABORATION WITH

EMERGENCY CARE IN RURAL BANGLADESH AND DISASTER PREPAREDNESS
EMERGENCY CARE IN RURAL BANGLADESH

CALENDER FOR DOCTORS AT THANA LEVEL
In case of snake bitenever waste your timegoing to traditionalhealer
Send the patientimmediately to nearesthealth facilities whereanti-venom is available

EMERGENCY MANAGEMENT IN BANGLADESH: REALITIES
Concept of modern day emergency care is unknown to our medical graduates
Pre-hospital EMS system exists in a very primitive form where ambulances are nothing but patient carriers
Most ERs with exception of 2-3 large private hospitals function as glorified triage stations or walk in clinics
EMOs are merely “Traffic Police” directing patient disposition EMOs are the most under recognized, poorly trained & future-less group of young physicians

EMERGENCY MANAGEMENT IN BANGLADESH: REALITIES
CPR not available in 99% of ER Emergency medicine as a specialty is virtually
unknown among our senior colleagues The burden of emergency care has fallen on inpatient
units, ICU, CCU

We need Govt. patronage to establishemergency care delivery in Bangladesh
Why ?
FACTS ABOUT BANGLADESH
Private hospitals are least interested in developingE.R rather than in establishing ICU/ CCU becauseICU/CCU are profitable

FACTS ABOUT BANGLADESH
Emergency is the most important department in ahospital in terms of service to the community but it isthe most expensive and least profitable in terms ofmanagement

FACTS ABOUT BANGLADESH
Who will pay for the cost of emergency care ?
We cannot afford to have a nationalized health services like those of Canada or Sweden

FEW RECOMMENDATIONS
A. Update medical colleges & nursing curriculum: Emergency medicine, Critical Care , CPR, all should be stressed appropriately
B. Develop EMS Training AcademyC. Government recognition of emergency medicine as
a specialty: Eventually postgraduate courses should be developed in our medical colleges
D. Public education using mass media: BLS, First Aid, Trauma prevention & disaster preparedness
E. Trauma center: Regional & local.
We also recommend that disaster planning &preparedness, EMS, emergency facilities should becoordinated by a separate directorate now underDepartment of Health, Government of Bangladesh
EPR (Emergency preparedness & response) programshould be upgraded

Story of an Unfortunate Son of Soil: Victim of Trauma

Story of a Fortunate Cardiac Arrest Victim
We want emergency care for everyone as ourbirth right - any kind, any time, any where -not as an exception and not as a favor ofluck blessed from the sky
We do not want to see the repetition of thescenario of the unlucky leader of our nation


FOR BANGLADESH WE ARE HOPEFUL. THERE ARE WAYS TO SURVIVE
EMERGENCIES

THANK YOU