emergency care of the newborn tina m. slusher, md associate professor of pediatrics university of...
TRANSCRIPT

Emergency Care of the Newborn
Tina M. Slusher, MDAssociate Professor of PediatricsUniversity of [email protected]
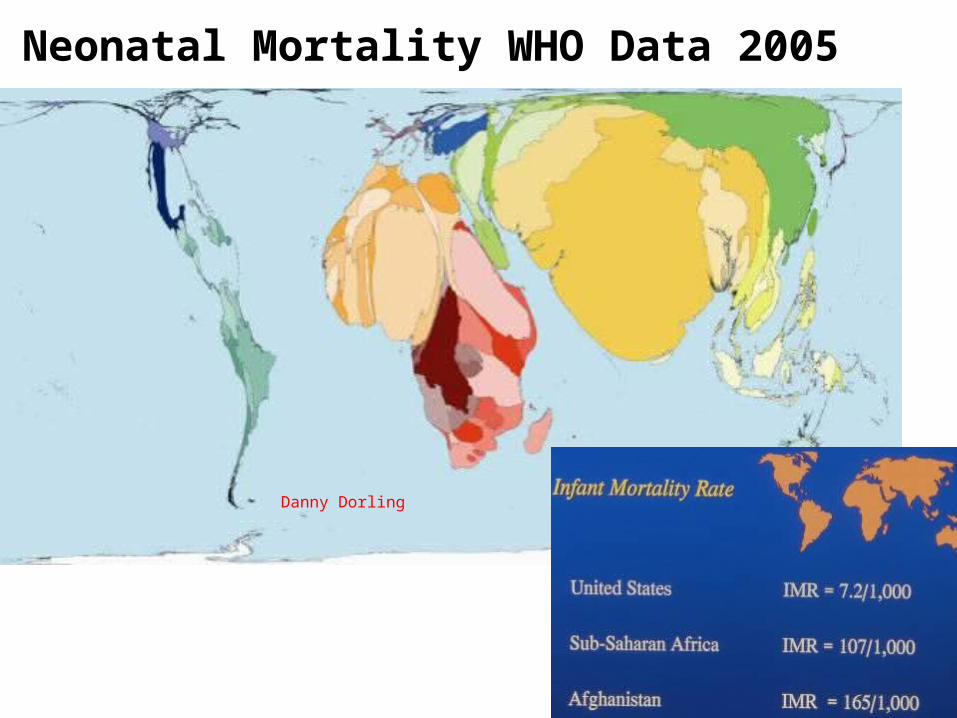
Neonatal Mortality WHO Data 2005
Danny Dorling
Center for Global Pediatrics

The 3 leading recognized causes of neonatal death world wide
are:
A. B. C. D.
5%
15%
36%
44%A. Prematurity, infection,
congenital anomalies B. Prematurity, infection,
asphyxiaC. Diarrheal diseases,
asphyxia, prematurityD. Prematurity, infection,
neonatal tetanus

World World Preterm 28%Preterm 28%
Infections 26%Infections 26%Asphyxia 23%Asphyxia 23%
Congenital Congenital anomalies 8%anomalies 8%
Tetanus 7%Tetanus 7%Other 7%Other 7%
Diarrheal 3%Diarrheal 3%
USAUSAPreterm 23%Preterm 23%Congenital Congenital
anomalies 22%anomalies 22%Sepsis 4%Sepsis 4%
Asphyxia/Hypoxia 3%Asphyxia/Hypoxia 3%

Lawn et al. Lancet, 2005.
Center for Global Pediatrics
Daily Risk of Neonatal Death

Newborn resuscitation*/ Respiratory distress
Delayed umbilical clamping*
Umbilical cord antisepsis*
Hypothermia prevention* & management/Kangaroo Care*
Hypoglycemia prevention and management*
Breastfeeding*
Sepsis (Pneumonia*)
Hyperbilirubemia screening*
Traditional birth attendant (TBA)/CHW training*
Vit K prophylaxis*
Hepatitis B vaccination*
Neonatal Vit A supplementation*
Topical Emollient therapy*
Prevention & treatment of ophthalmia neonatorum*
PostnatalInterventions
*Community Based interventionsZulfiqar et al; Pediatrics
2005;115;519-617

Percentage of Neonatal Resuscitation Doable at most
hospitals/clinics in the developing world
A. B. C. D.
17%
39%
23%22%
A. <50%B. >90%C. <70%D. >70%

Appropriate neonatal resuscitation is easily adjusted to the resources available!!!!!
95% of resuscitation as taught by NRCP guidelines is “doable” at most hospitals & many clinics in the developing world!!!

Basic Resuscitation Equipment
• Warm delivery room (w/out draft - w/ fans off)• Two pieces of cloth used to dry and wrap newborn to prevent heat
loss• Mucous extractor or DeLee Aspirator• Positive Pressure Bag (“Ambu” bag) and mask or device to give
positive pressure ventilation (mouth-to-mouth may be appropriate in some situations)

What is most important in neonatal resuscitation
A. B. C. D. E.
20%
50%
30%
1%0%
A. OxygenB. VentilationC. EpinephrineD. Sodium
BicarbonateE. Meconium aspirator
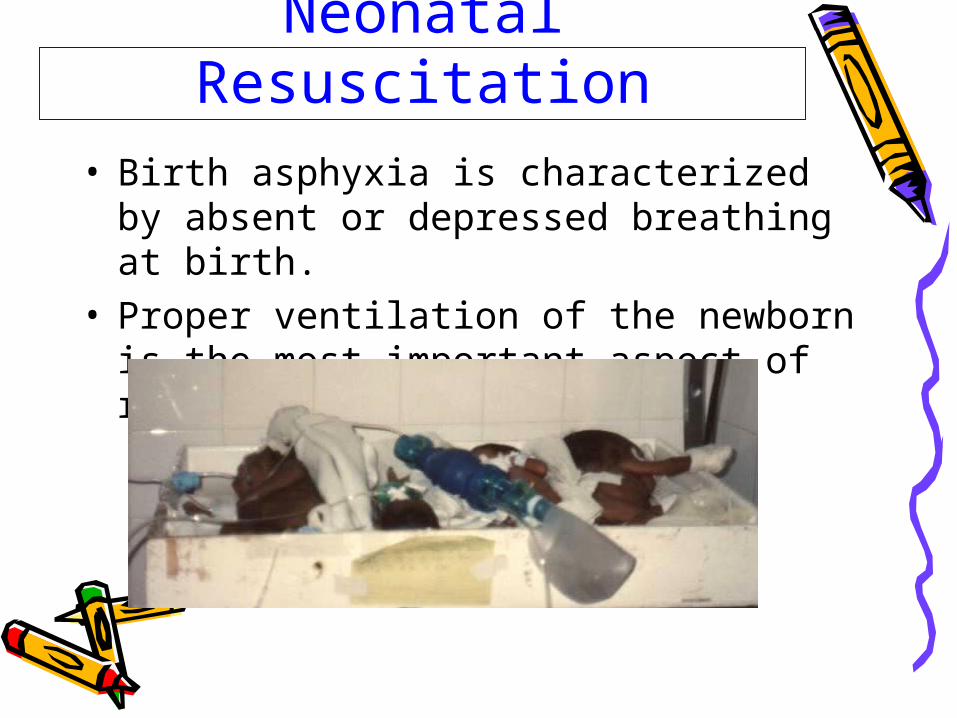
Neonatal Resuscitation• Birth asphyxia is characterized by
absent or depressed breathing at birth. • Proper ventilation of the newborn is the
most important aspect of resuscitation.
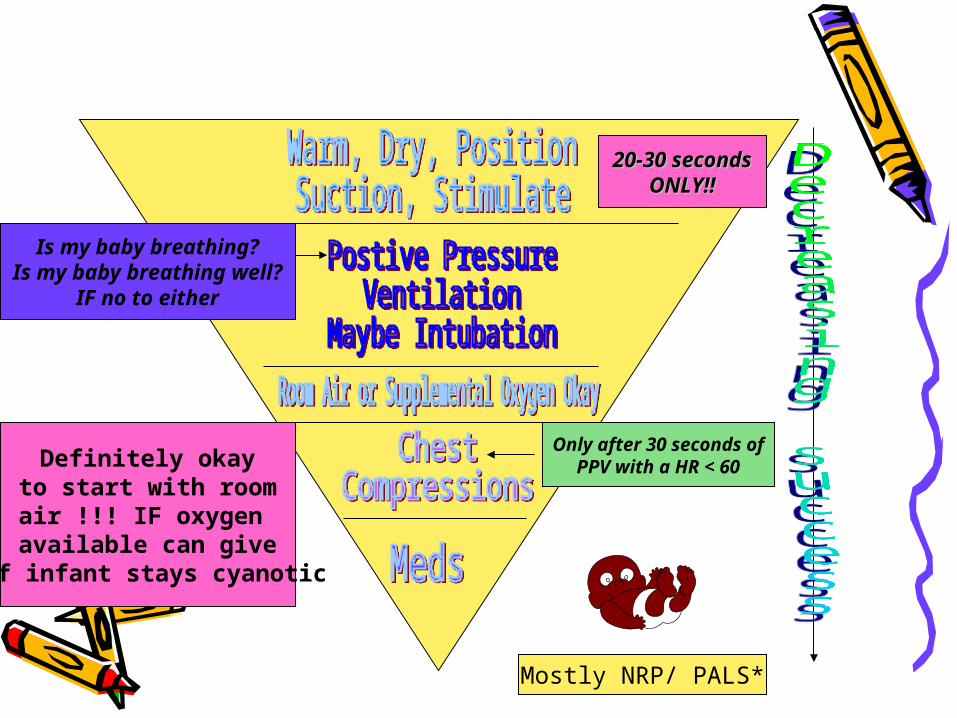
Mostly NRP/ PALS*
Is my baby breathing?Is my baby breathing well?
IF no to either
Only after 30 seconds ofPPV with a HR < 60
20-30 seconds20-30 secondsONLY!!ONLY!!
Definitely okayto start with roomair !!! IF oxygen
available can give if infant stays cyanotic
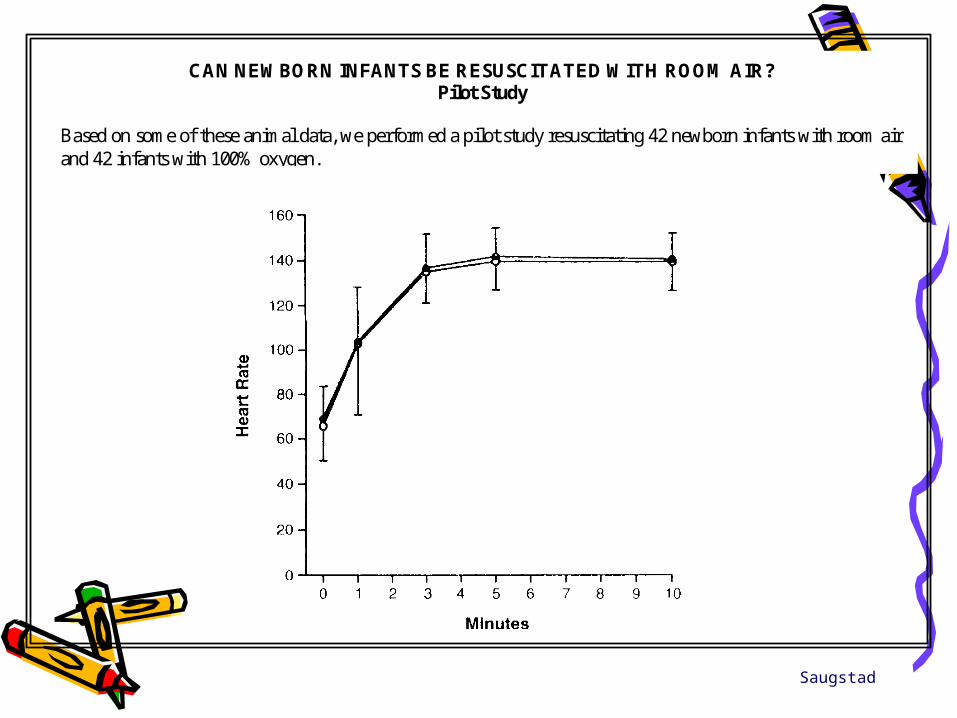
CAN NEWBORN INFANTS BE RESUSCITATED WITH ROOM AIR?Pilot Study
Based on some of these animal data, we performed a pilot study resuscitating 42 newborn infants with room airand 42 infants with 100% oxygen.
Saugstad

Emphasize Time
• Remember first block warm, dry, position, suction, stimulate should be accomplished in NO MORE than 20-30 seconds
• By 30 seconds you should be positive pressure ventilating any infant who is not breathing or not breathing well
Suction Mouth First then Nose, Stimulate AppropriatelySuction Mouth First then Nose, Stimulate Appropriately

HR is the 1° sign of improved ventilation during neonatal resuscitation
• In community based resuscitation focus on ventilation—most “resusciatatable” infants resuscitated with ventilation NOT chest compressions and drugs
• Some programs teaching family members to do mouth to mouth secondary to concerns about infections in places where positive pressure bags not an option

Respiratory Distress• Keep oxygen flow in preemie low- aim for pink
infant or O2 sats 87-95% (minimize risk of eye damage & limit oxygen toxicity).
• In term infants at risk for pulmonary hypertension keep oxygen high.
• Respiratory distress > 1st hr of life always think sepsis/pneumonia & Rx accordingly.
• Apnea of prematurity is treated w/ aminophylline. Dilute IV form w/ clean water and give po/ngt if solution not available. (Caffeine OK too)
• Aminophylline– Load 5-6 mg/kg IV or po– Maintenance 1-2 mg/kg/dose q 6-8-12h IV/po
• Continuous Positive Airway Pressure (CPAP) may be useful in mild-moderate respiratory distress or apnea without a ventilator

Depth of tubeDepth of tubeIn water determinesIn water determines
CPAP deliveredCPAP delivered

Delayed umbilical clamping
• May increase newborn infants iron stores and reduce incidence of iron deficiency anaemia in infancy-important public health importance.
• (BMJ 1996;312:136-137, Grajeda et al Am J Clin Nutr. 1997;65:425-431)

Maintenance of Body Temperature
Hypothermia occurs when body temp (axillary) drops below 36.5C (97.7F). Neonatal cold injuries are common worldwide.
• Ethiopian hospital - 67% of LBW and high-risk infants admitted to NICU from outside were cold.
• India - mortality rate of hypothermic infants was twice that of infants without hypothermia.

• Cold infants are more difficult to resuscitate.
• Hypothermia clearly morbidity/ mortality in newborns.
• Skin-to-skin contact immediately upon delivery & in nursery greatly risk of hypothermia or cold injury.
• **Exception is asphyxiated infant---data NOT complete so can not yet recommend cooling but absolutely should NOT overheat asphyxiated infants!!


Hypoglycemia
• Defined as <40-45 mg/dL• IF possible confirm strips w/ blood glucose• Major cause of morbidity especially in
groups such as premies, SGA, and IDM • Most cost effective strategy for preventing
hypoglycemia is early frequent breast feeding (cup & spoon or NGT if not able to feed @breast)

Hypoglycemia cont.
• IF breast feeding not possible glucose can be treated in mild group w/ 5% glucose by mouth 4-8cc/kg
• IF glucose <25mg/dL treat w/IV D10W 2-4cc/kg (not D25 or D50)

• Exclusive is KEY! • Especially if mother is HIV+

Sepsis• Sepsis is major cause of death
world-wide in neonates• Think about early & cover broadly
until able to rule-out • REMEMBER-Any deviation from
normal can be sepsis temperature, WBC, lethargy, glucose, vomiting, diarrhoea, any feeding intolerance, respiratory distress beyond 1st hour, etc, etc,

Sepsis continued
• Amp/Gent reasonable choices • Consider cloxacillin if staph likely
in your nursery.• Cefotaxime good choice for
resistant gram neg organisms or meningitis if available
• DO NOT use Ceftriaxone in Neonates!

Hyperbilirubemia
• May be largest “unrecognized” or silent cause of neonatal morbidity/mortality in the developing world
• Need to think about it, look for it, and when severe treat it---all huge challenges in most of the developing world.

Traditional birth attendant (TBA)/CHW training
• Most babies in developing world (60-80%+) still born at home~half without access to skilled care)
• Trained TBA’s do a better job of taking care of newborns than untrained TBA’s!
• Continued training important as it is for all of us

9/18/08
The EndReference list
included-bulk fromBhutta et al, Pediatric
2005:115;519-617)
Thanks Thanks