elevated liver tests - medicine.umich.edu
TRANSCRIPT
Elevated Liver Tests Lisa M. Glass, MD October 19, 2017
Clinical Case 1:
HPI: 67 year old woman with a h/o chronic UTIs presents with a several month history of fatigue and epigastric pain that progressed to include intermittent fevers (Tmax of 101ºF)
PMH: Sjogren’s syndrome, SLE, Breast cancer: partial mastectomy with XRT, Obesity
Meds: Omeprazole 40mg daily, Macrodantin 50mg po QHS
Social Hx: Married with two adult children EtOH use: minimal throughout life IV or intranasal DU: never Tattoos, blood transfusions: none
Clinical Case 1:
• Physical Exam: – VS: T: 98.7 HR: 85 BP: 137/78 – Gen: Alert, oriented, NAD – HEENT: Icteric sclera – Abd: Nondistended, bowel sounds present, tender to palpation in RUQ, no
rebound/guarding – Skin: Notable jaundice; no palmar erythema, spider angiomas
• Labs: – Cr 0.8 – Alb: 3.3/AST 584/ ALT 345/ AP 159/ TB 13 – WBC 6.5/HGB 12.8/ Plt 234 – INR 1.1
1. Schedule PCP follow-up in 2 weeks 2. Refer to liver clinic next available (4-6 weeks) 3. Refer to liver clinic urgent (within 10 days) 4. Direct hospital admission 5. Send to emergency department
Next step in management: what would you do now?
• Acute Liver failure: – Mental status changes – Hepatitis/Jaundice – Coagulopathy
• Other worrisome features: – Fever – Acute abdominal pain – Rapid ascites accumulation
Patient Triage: Red-flag signs in acute liver disease
• History: – Medications/herbs, drug or alcohol use – Exposures to others with hepatitis – Parenteral risks: blood transfusion, needle sticks, or tattoos – Travel, diet, raw seafood, shellfish – Previous hepatitis or jaundice – Autoimmune diseases
• Keys to Physical Assessment: – Careful Neurologic assessment
• Asterixis or altered mental status • Tremor: withdrawal • Movement disorder or pyschiatric disturbance
– Look for stigmata of chronic liver disease • Telangectasia, palmar erythema, palpable spleen, umbilical hernia , caput
medusae, ascites
Initial Approach:
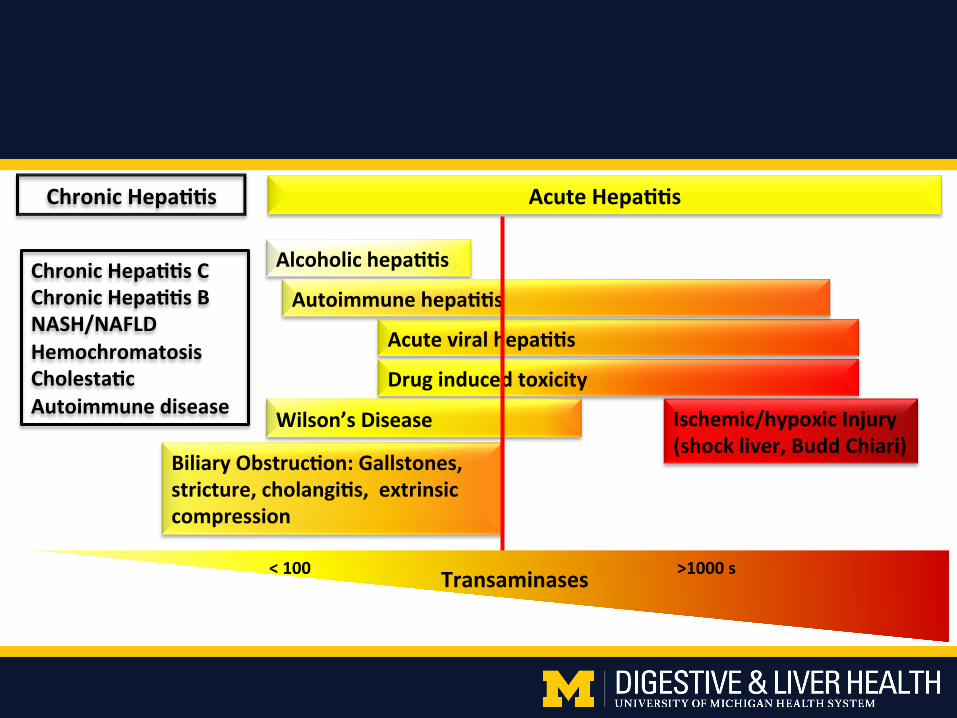
AcuteHepa**s
Acuteviralhepa**s
Alcoholichepa**sChronicHepa**sCChronicHepa**sBNASH/NAFLDHemochromatosisCholesta*cAutoimmunedisease
ChronicHepa**s
Autoimmunehepa**s
Druginducedtoxicity
Ischemic/hypoxicInjury(shockliver,BuddChiari)
BiliaryObstruc*on:Gallstones,stricture,cholangi*s,extrinsiccompression
Wilson’sDisease
<100>1000sTransaminases
• History: – Significant EtOH intake
(>100g/day) – Symptoms can start days to
weeks after EtOH cessation
• Presentation: – Rapid onset of jaundice,
abdominal distension, ascites – +/- Fever – Encephalopathy – Enlarged and tender liver
• Laboratory studies: – AST > 2x ULN
• rarely above 300 IU/ml – AST/ALT ratio >2 – Leukocytosis – Increased bilirubin, INR,
creatinine – Hemolysis
• Treatment: – Steroids for Maddrey’s DF >32
• Absence of infection, renal failure and GI Bleeding
– Abstinence is the only predictor of improved long-term mortality
Differential Diagnosis: Acute alcoholic hepatitis
• Background: – Responsible for 10% of all cases
of acute hepatitis – Most common cause of liver
failure in the U.S. – Culprit Medications:
1. Acetaminophen 2. Antibiotics: Augmentin
• History: – Timing: 5 days – 3 months
typical – Exclude other possible
causes
Differential Diagnosis: Drug induced liver injury
• Presentation: – Varied: asymptomatic liver
test elevation to fulminant failure
– +/- Fever – Fatigue – Rash – Nausea and vomiting
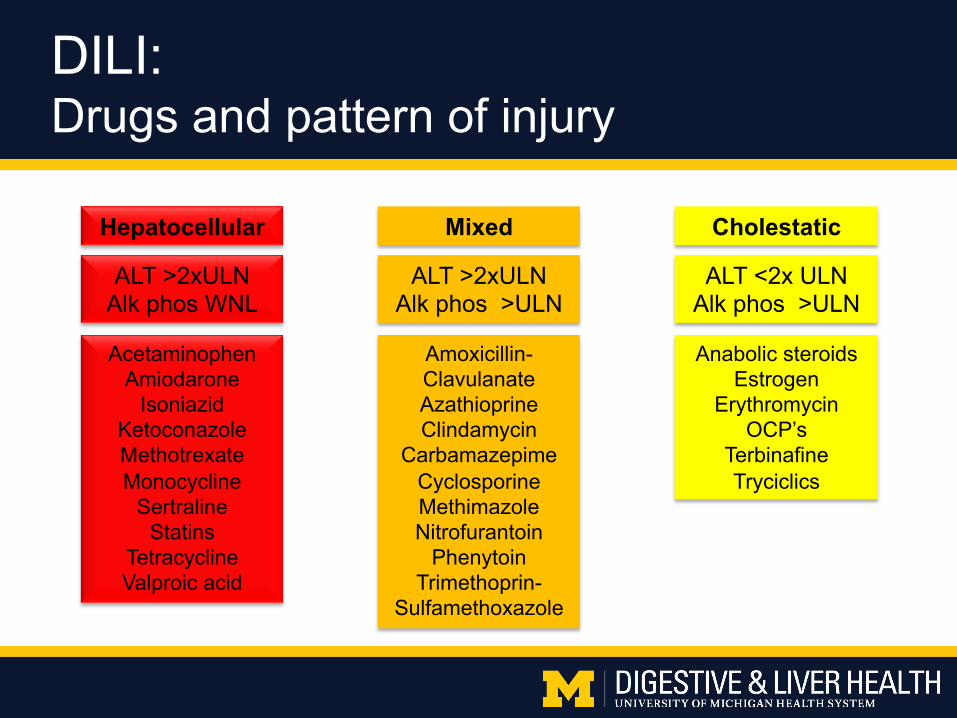
Hepatocellular Mixed
ALT <2x ULN Alk phos >ULN
ALT >2xULN Alk phos >ULN
Acetaminophen Amiodarone
Isoniazid Ketoconazole Methotrexate Monocycline
Sertraline Statins
Tetracycline Valproic acid
Amoxicillin-Clavulanate Azathioprine Clindamycin
Carbamazepime Cyclosporine Methimazole Nitrofurantoin
Phenytoin Trimethoprin-
Sulfamethoxazole
Anabolic steroids Estrogen
Erythromycin OCP’s
Terbinafine Tryciclics
ALT >2xULN Alk phos WNL
Cholestatic
DILI: Drugs and pattern of injury
Is there a role for Acetaminophen in known chronic liver disease?
1. Yes, absolutely it is a safe drug because the toxic range is understood
2. No, one must avoid this drug in patients with any known liver disease
3. Not sure
Is there a role for statins in known chronic liver disease?
1. Yes, absolutely it is a safe drug, even in patients with chronic liver disease
2. No, one must avoid this drug in patients with any known liver disease
3. Not sure
• History: – Identify risk for recent exposure: Drug
use, blood transfusion, new sexual partner, needlestick, travel/restaurants
• Presentation: – Frequently asymptomatic – Fatigue – Nausea and vomiting – Jaundice – RUQ pain
• Laboratory studies: – Depends on timing of presentation – Serologic evaluation to diagnose
• Treatment: – Supportive care – HAV post-exposure prophylaxis
(within 14 days of exposure) • Healthy persons aged 1-40 years: HAV
vaccine • Persons +41 years, <12 months,
Immunocompromised: Immune globulin
– Monitor for progressive or acute liver failure, typically only in acute HBV
– Antiviral medications in some cases of acute HBV
Differential Diagnosis: Acute Viral Hepatitis
1. Anti-HAV IgG; Anti-HBc IgM; Anti-HCV
2. Anti-HAV IgM; Anti-HBc IgG; HCV RNA PCR
3. Anti-HAV total; HBs Ag; Anti-HCV
4. Anti-HAV IgM; Anti-HBc IgM; HCV RNA PCR
Testing for Acute Hepatitis:
• Initial Presentation: – Wide range of signs and symptoms:
• Asymptomatic to arthralgia and fatigue to acute liver failure – Incidence:
• 1-2/100,000 persons in US – Female to male ratio: 3.6:1 – Peak ages 16-30 years:
• 50% >30 years, 23% ≥ 60 years • Diagnosis:
– Elevation of ALT or AST – Elevation of IgG (>1.5x the ULN more suggestive) – ANA, anti-smooth muscle Ab, or anti–Liver Kidney Microsomal-1 Ab – Other autoimmune disorders in 15-34%
• Autoimmune thyroiditis, synovitis, celiac disease, and IBD
Differential Diagnosis: Autoimmune Hepatitis
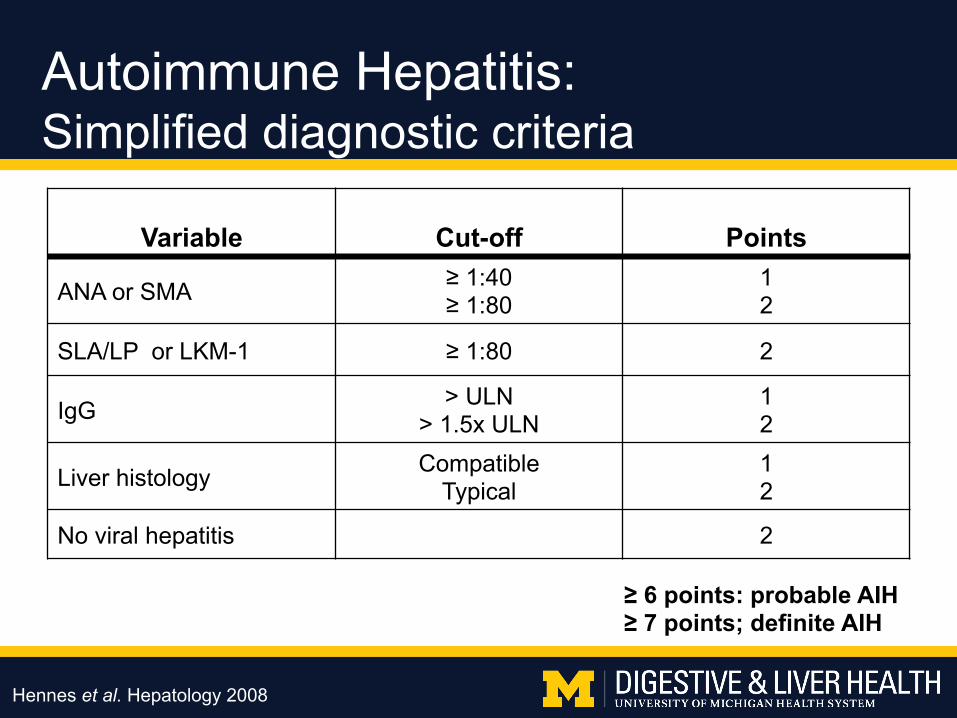
Variable Cut-off Points
ANA or SMA ≥ 1:40 ≥ 1:80
1 2
SLA/LP or LKM-1 ≥ 1:80 2
IgG > ULN > 1.5x ULN
1 2
Liver histology Compatible Typical
1 2
No viral hepatitis 2
Autoimmune Hepatitis: Simplified diagnostic criteria
≥ 6 points: probable AIH ≥ 7 points; definite AIH
Hennes et al. Hepatology 2008
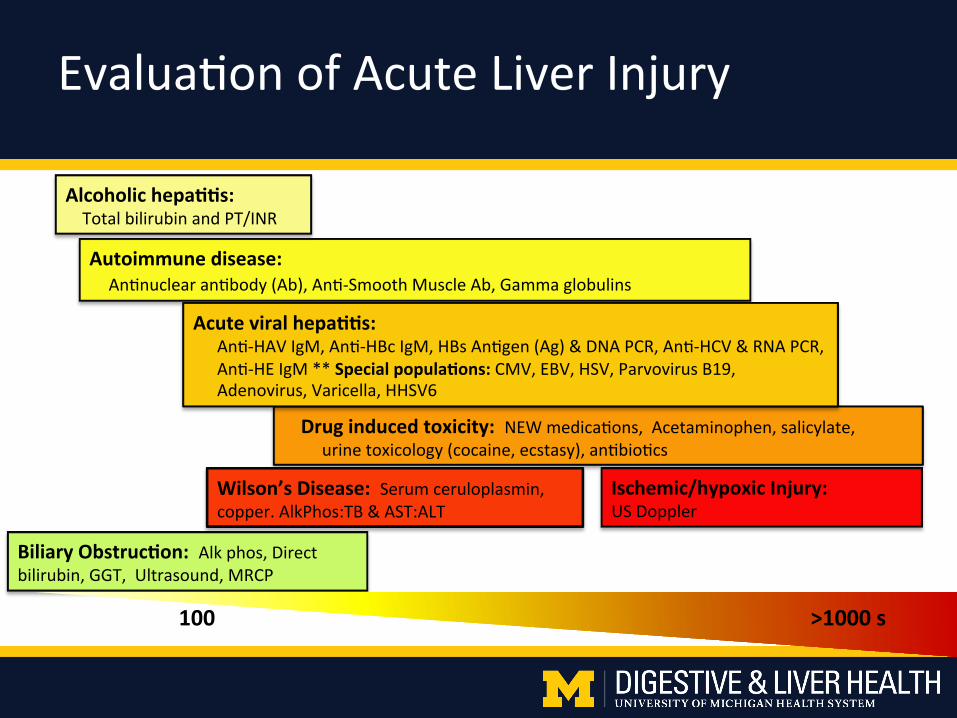
Druginducedtoxicity:NEWmedica+ons,Acetaminophen,salicylate,urinetoxicology(cocaine,ecstasy),an+bio+cs
Ischemic/hypoxicInjury:USDoppler
Autoimmunedisease:An+nuclearan+body(Ab),An+-SmoothMuscleAb,Gammaglobulins
Acuteviralhepa**s:An+-HAVIgM,An+-HBcIgM,HBsAn+gen(Ag)&DNAPCR,An+-HCV&RNAPCR,An+-HEIgM**Specialpopula*ons:CMV,EBV,HSV,ParvovirusB19,Adenovirus,Varicella,HHSV6
BiliaryObstruc*on:Alkphos,Directbilirubin,GGT,Ultrasound,MRCP
Wilson’sDisease:Serumceruloplasmin,copper.AlkPhos:TB&AST:ALT
Alcoholichepa**s:TotalbilirubinandPT/INR
100>1000s
Evalua+onofAcuteLiverInjury
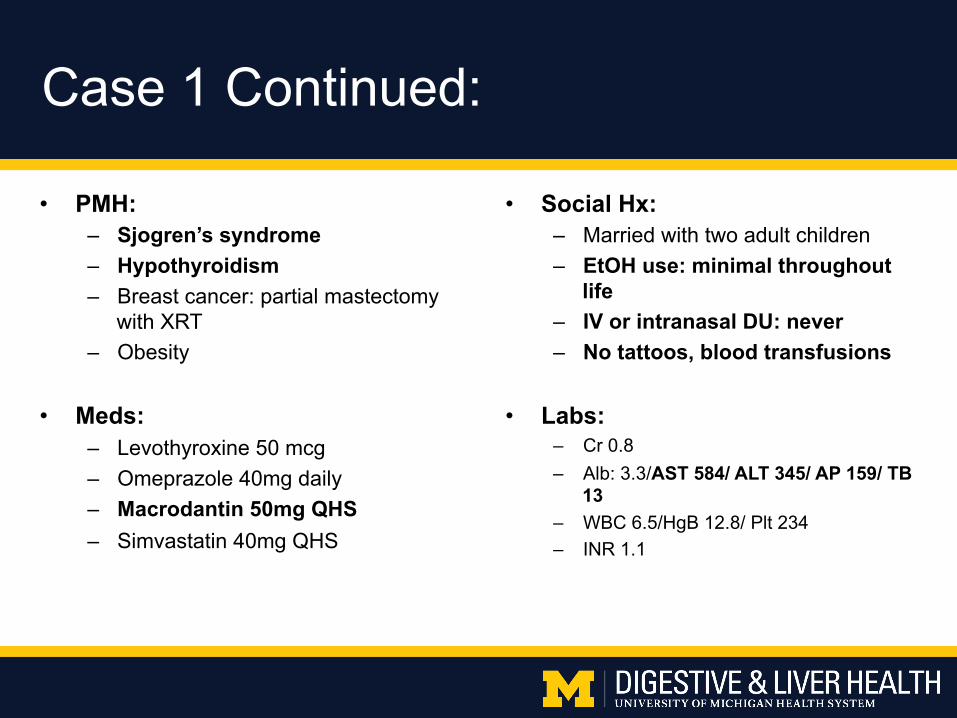
• PMH: – Sjogren’s syndrome – Hypothyroidism – Breast cancer: partial mastectomy
with XRT – Obesity
• Meds: – Levothyroxine 50 mcg – Omeprazole 40mg daily – Macrodantin 50mg QHS – Simvastatin 40mg QHS
• Social Hx: – Married with two adult children – EtOH use: minimal throughout
life – IV or intranasal DU: never – No tattoos, blood transfusions
• Labs: – Cr 0.8 – Alb: 3.3/AST 584/ ALT 345/ AP 159/ TB
13 – WBC 6.5/HgB 12.8/ Plt 234 – INR 1.1
Case 1 Continued:
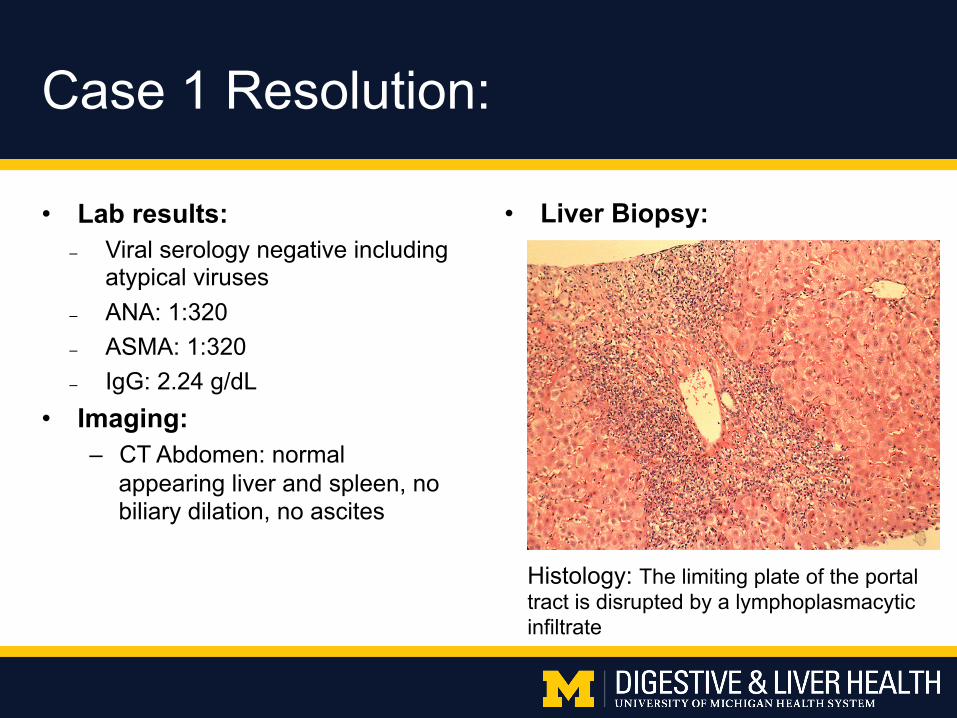
• Lab results: – Viral serology negative including
atypical viruses – ANA: 1:320 – ASMA: 1:320 – IgG: 2.24 g/dL
• Imaging: – CT Abdomen: normal
appearing liver and spleen, no biliary dilation, no ascites
Case 1 Resolution:
Histology: The limiting plate of the portal tract is disrupted by a lymphoplasmacytic infiltrate
• Liver Biopsy:
• Treatment: – Stop Macrodantin – Prednisone 60mg daily x 1 week followed by taper – Week 3: Consider Azathioprine 50 mg daily
Case 1 Resolution:
• HPI: • 45 year old man with HTN presents
with abnormal liver tests for 5 years. • Meds:
• Losartan, HCTZ, Viagra, ASA, MVI, Simvastatin
• Social History: • EtOH: social • Tobacco: 40 pack year Hx, quit 2010 • Illicits: none
• PE: • BP: 152/80; BMI 37 • Normal exam • No spider angiomas, no nail changes, no
palmar erythema
• Labs: – Alb 4.6/AST 57/ALT 107/AP 73/TB
0.9; Hgb 13.5/Plt 283 – Alpha one antitrypsin testing, TSH,
viral hepatitis, TTG IgA, fasting glucose were all normal/negative
– Autoimmune panel: • ANA: neg; ASMAb: 1:40; IgG: 1.41g
– Iron studies: • Ferritin 295; TSAT 40%
• Imaging: – RUQ US: Increased echogenicity
of the liver, normal spleen size
Clinical Case 2:
• Additional Work-up: – ? HFE mutation analysis
• No sign of iron overload: – Ferritin is <330 (patient is male) and TSAT is <45%
– ? Liver biopsy to evaluate for autoimmune hepatitis • ASMAb is mildly elevated while ANA is negative and IgG
level is normal: findings are non-specific and often found in NAFLD
– NAFLD fibrosis score (NFS): • 0.013 (indeterminate)
Clinical Case 2:
1. Do nothing, as so many Americans have fatty liver
2. Immediate Fibroscan
3. Immediate liver biopsy
4. Stop statin
5. Counsel patient on weight loss, recheck liver tests in 6 months, then consider liver biopsy/Fibroscan
Clinical Case 2: