electrodiagnosis- tarsal tunnel · pdf fileelectrodiagnosis- tarsal tunnel revisited tarsal...
TRANSCRIPT
Differential Diagnosis of Subcalcaneal Heel Pain by Mohammad A. Saeed, M. D. - Soft Tissue - Neurologic
1 Plantar Fasciitis 1 Tarsal Tunnel Syndrome (TTS) 2 Periostitis 2 Inferior Calcaneal Neuropathy 3 Painful Heel Pad 3 Medial Calcaneal Neuropathy 4 Subcalcaneal bursitis 5 Tenosynovitis (FHL & FDL) 6 Calcaneal Apophysitis
For recalcitrant heel pain, EMG/NCV study can be very helpful to R/O a neurologic cause, particularly Inferior Calcaneal Neuropathy or Neuropathy of “Baxter’s” nerve
1
* Founded 1981
Surinderjit Singh, M. D., M. S. * †
Mohammad A. Saeed, M. D., M.S. * † Edgar S. Steinitz, M. D. * † ‡
Tabassum Saeed, M. D., M. S. * † Irfan Ansari, M. D. * Srini Sundarum, M. D., M.P.H. *
May 1999
Volume 2, Issue 2 Board Certified AAPM&R *, ABEM †, AAPM ‡
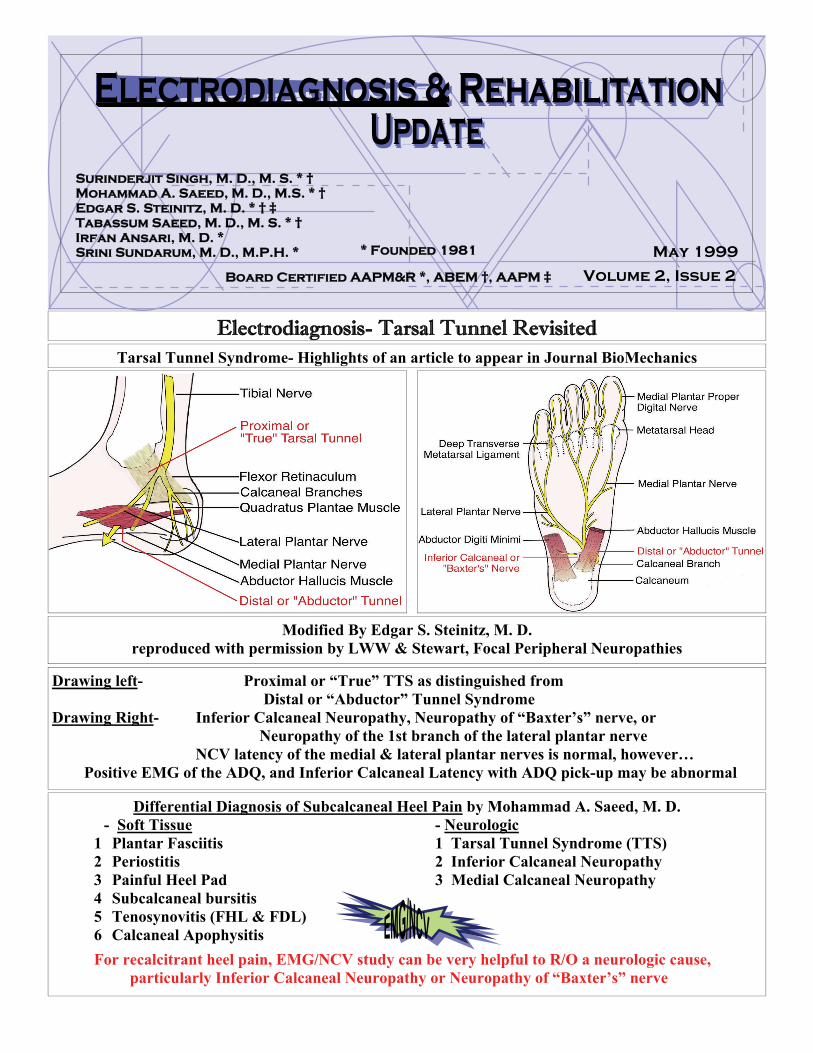
Electrodiagnosis- Tarsal Tunnel Revisited Tarsal Tunnel Syndrome- Highlights of an article to appear in Journal BioMechanics
Modified By Edgar S. Steinitz, M. D. reproduced with permission by LWW & Stewart, Focal Peripheral Neuropathies
Drawing left- Proximal or “True” TTS as distinguished from Distal or “Abductor” Tunnel Syndrome Drawing Right- Inferior Calcaneal Neuropathy, Neuropathy of “Baxter’s” nerve, or Neuropathy of the 1st branch of the lateral plantar nerve NCV latency of the medial & lateral plantar nerves is normal, however… Positive EMG of the ADQ, and Inferior Calcaneal Latency with ADQ pick-up may be abnormal
Electrodiagnosis and Rehabilitation Associates
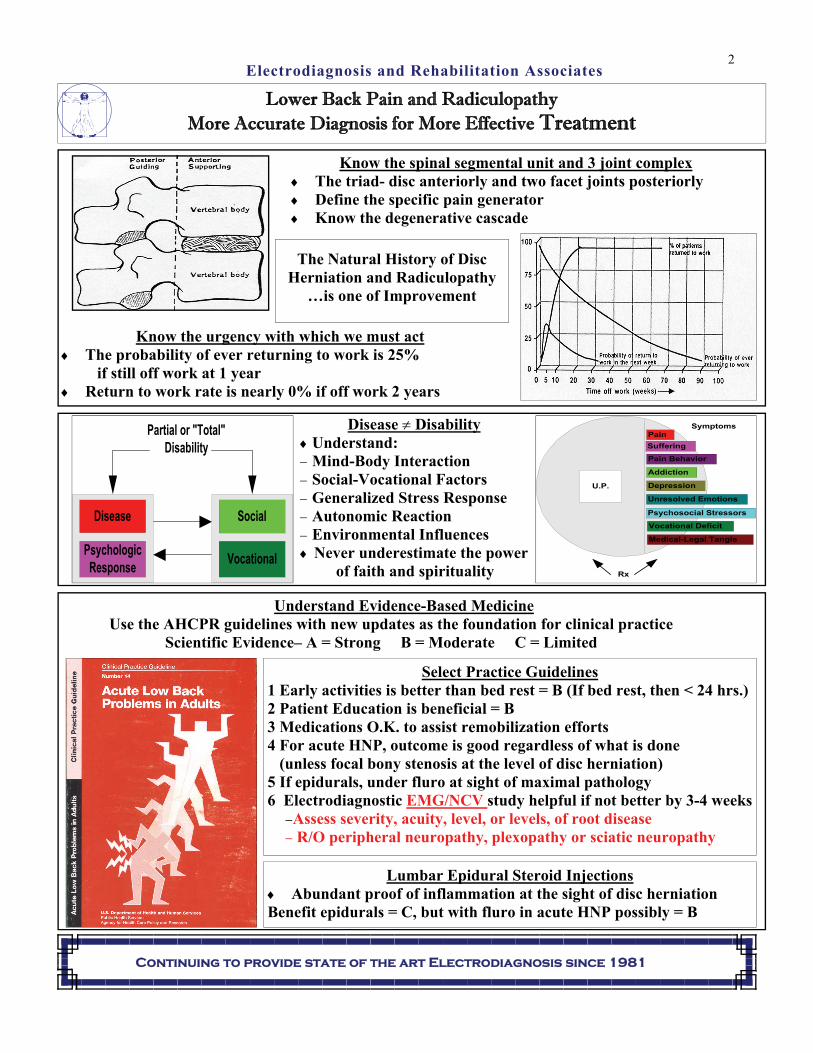
U.P.
Pain
Suffering
Pain Behavior
Unresolved Emotions
Medical-Legal Tangle
Addiction
Vocational Deficit
Psychosocial Stressors
Depression
Symptoms
Rx
Continuing to provide state of the art Electrodiagnosis since 1981
Know the spinal segmental unit and 3 joint complex The triad- disc anteriorly and two facet joints posteriorly Define the specific pain generator Know the degenerative cascade
PsychologicResponse
Disease Social
Vocational
Partial or "Total"Disability
Know the urgency with which we must act The probability of ever returning to work is 25% if still off work at 1 year Return to work rate is nearly 0% if off work 2 years
Disease Disability Understand: Mind-Body Interaction Social-Vocational Factors Generalized Stress Response Autonomic Reaction Environmental Influences Never underestimate the power of faith and spirituality
Understand Evidence-Based Medicine Use the AHCPR guidelines with new updates as the foundation for clinical practice Scientific Evidence– A = Strong B = Moderate C = Limited
The Natural History of Disc Herniation and Radiculopathy
…is one of Improvement
Lumbar Epidural Steroid Injections Abundant proof of inflammation at the sight of disc herniation Benefit epidurals = C, but with fluro in acute HNP possibly = B
Select Practice Guidelines 1 Early activities is better than bed rest = B (If bed rest, then < 24 hrs.) 2 Patient Education is beneficial = B 3 Medications O.K. to assist remobilization efforts 4 For acute HNP, outcome is good regardless of what is done
(unless focal bony stenosis at the level of disc herniation) 5 If epidurals, under fluro at sight of maximal pathology 6 Electrodiagnostic EMG/NCV study helpful if not better by 3-4 weeks
Assess severity, acuity, level, or levels, of root disease R/O peripheral neuropathy, plexopathy or sciatic neuropathy
Lower Back Pain and Radiculopathy More Accurate Diagnosis for More Effective Treatment
2