electrocardiogram during exercise - homepage |...
TRANSCRIPT

The Electrocardiogram During Exercise
Findings in Bipolar Chest Leads of 1,449 Middle-Aged Men,at Moderate Work Levels
By HENRY BLACKBURN, M.D., HENRY L. TAYLOR, PH.D.,
C. Luis VASQUEZ, M.D., AND THOMAS C. PUCHNER, M.D.
ELECTROCARDIOGRAPHIC (ECG) re-cording during exercise, employed for
years by work physiologists, has only recentlyarrived on the scene of cardiovascular inves-tigations in clinical, epidemiological, andsports medical areas. This has come aboutfrom interest in the import of ECG events ob-served during activity, from the improvedsafety provided by monitoring performancetests, and from technical innovations whichhave led to more convenience and better qual-ity in recordings.The extension of investigations in this area
and certain reasons of expediency have ledto use of many nonstandard testing andmonitoring procedures. These include non-standard configurations of ECG electrodesacross the chest, the upright posture, FMradio transmission of the ECG, numerousother developments in instrumentation, anddifferent modes of imposing work stress.
Standardization of method in exercise elec-trocardiography is not yet possible or desir-able, because of rapid developments inquantitative cardiography and work physiol-ogy.1 Though it is not clear whether most ofthe nonstandard methods now used are de-sirable for the long run, they are neverthelessin use, and some quantitative base for thediagnostic and prognostic information soughtfrom these methods is of interest.
This report concerns a specific applicationin which nonstandard electrocardiography
Work supported by Grant HE-03088 from theU. S. Public Health Service and by grants from theAmerican Heart Association, the Minnesota HeartAssociation, and from the U. S. Public Health Ser-vice to the University of Minnesota Medical School(HE-06314).
during exercise was employed, between re-cordings of conventional standard supine rest-ing and post-exercise electrocardiograms. Theresults apply to middle-aged working men,walking on a treadmill at an energy ex-penditure comparable to other common stresstests, in an examination situation with practi-cal limitations of time, and in which twocommon types of simple bipolar chest ECGleads were employed.An earlier report from this laboratory' de-
scribed the characteristics of S-T segmentdisplay in some of the multiple chest electrodeconfigurations which have been employedfor ECG monitoring (fig. 1).
Method
Each of two bipolar leads used has an ex-ploring electrode at the standard left chest posi-tion C5 (V5) while the lead called "CM5" has areference electrode on the upper part of themanubrium sternum and that called "CC5" em-ploys a reference electrode in the same but op-posite position on the right chest (fig. 2).
Records were made in 1,449 men, ages 45through 64 years, part of a sample of railwayworkers under long-term observation within thecontext of a study into the influence of occupation-al activity on the attack rate of coronary heartdisease. Details of the statistical sampling pro-cedure are given elsewhere.3 4 The overall re-sponse rate of the sample, 60 to 75%, precludesclaims that this population is representative ofanything other than a large group of middle-aged volunteers, actively employed in clericaland yard positions on rail lines operating in thenorthwest quadrant of the United States.
Specifically excluded from the exercise test (inaddition to nonrespondents to the survey invita-tion) were subjects with clinically manifest cor-onary heart disease in the form of documentedmyocardial infarction, angina pectoris with anabnormal resting ECG, or severely disabling ill-ness of any kind. Included in the exercise test
Circulation, Volume XXXIV, December 19661034
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELECTROCARDIOGRAM AND EXERCISE
Figure 1Differences in magnitude and contour of S-T segment depression in one case recorded withdifferent lead configurations. CH, forehead to chest; CR, right arm to chest; CC, right to leftchest; CB, right back to chest; CM, sternum to chest; CS, right subelavicle to chest; 0, rightsubclavicle to left back; X, right-to-left chest; A, manubrium to sacrum; B, right lower-to-leftlower chest; CN, lower neck to chest; V, Wilson leads; RV, modified Wilson leads; R, right-to-left chest; L, ear-ensiform-precordial system.
group were subjects with chest complaints hav-ing normal resting ECG's, subjects with equivo-cal types of chest pain, hypertension, and asymp-tomatic minor and borderline rest ECG findings.In total, 96% of all study respondents were will-ing and able to perform the 3-minute walk.
Recordings were made in an air-conditionedconverted Pullman car laboratory at the work-site of the men at the conclusion of the medicalexamination and the conventional supine restingECG. During the recording the subject stoodquietly before exercise, and after 15 seconds,14 minutes, and 2/34 minutes of a 3-minute tread-mill walk at 3 miles per hour, on a 5% grade.The average oxygen consumption of men at this Figure 2work level is approximately 1.4 L per minute.A Sanborn model 100 direct-writer (time con- Electrode positions for the two bipolar leads
stant verified at greater than 2 seconds), with CC .Circulation, Volume XXXIV, December 1966
CM5 and
1035
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from

BLACKBURN ET AL.
direct cable-coupling or FM radio telemetry*was used (time constant of the entire telemetry-recording system was verified at 1.6 seconds).No important difference in the quality of therecords was obtained at this level of work be-tween these two recording modes.
Eighty-eight per cent of the records were ofadequate quality for eyeball classification of S-Tand T findings from the CM5 lead, while 43%were adequate from the CC5 lead. The codingwas found to be reasonably reproducible withone observer (intra-observer agreement in repeti-tions on presence or absence of a finding was 90%;agreement to agreements plus disagreements).
Specialized methods of improving the ECGsignal in respect to the record "noise,"5 and new
electrodest have now considerably improved boththe yield of technically good records, even duringmuch higher work levels, and the ability toquantitate the ECG findings.The ECG items classified in the resting and in
each exercise record are listed in table 1.
Results
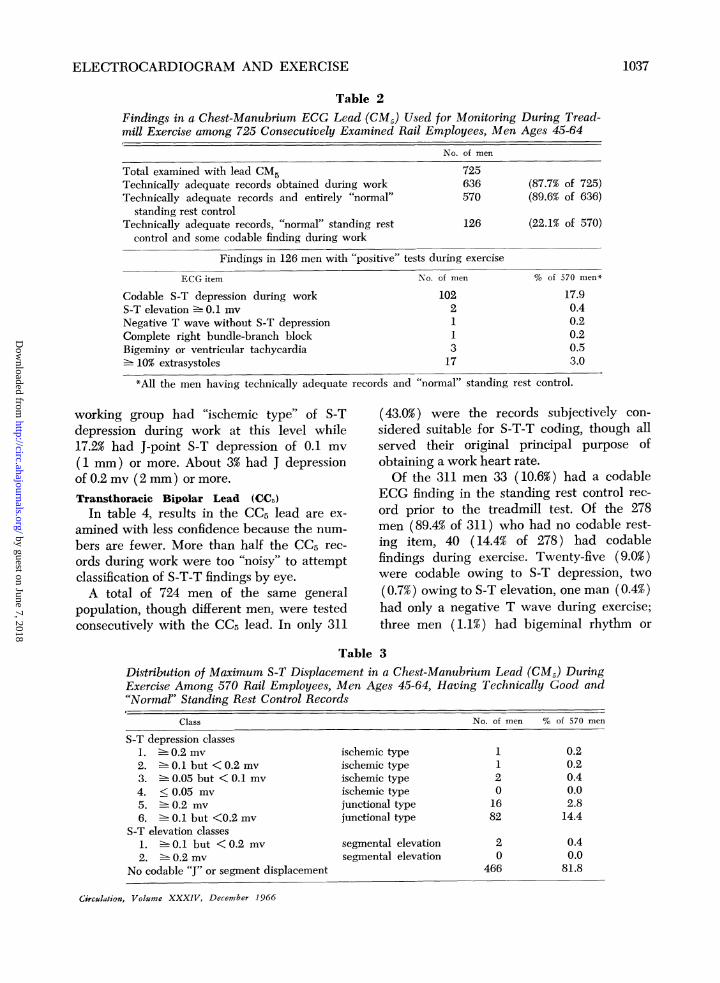
Manubrium-CO Bipolar Lead (CM5)Table 2 presents findings for this lead in
725 consecutively examined working men, ages
45 through 64 years. Records subjectively con-
sidered adequate for eyeball classification were
*Medtronic Inc. Model 16085 Transmitter, Model16080 Receiver and Model 2050 Monitor Scope,Minneapolis, Minnesota.tBeckman Biopotential Skin Electrodes, Spinco
Division, Palo Alto, California. "M & L electrodes."6
obtained in 636 (87.7% of the total). Sixty-sixmen (10.4% of men with technically good rec-ords) had one or more codable findings on
the standing control record (S-T depressionor elevation, negative T waves, bundle-branchblock, frequent extrasystoles, or atrial fibril-lation). Conversely, 570 men (89.6% of menwith technically good records) had "normal"standing control records prior to exercise.Of the 570 men with technically adequate
and normal control records, 126 (22.1%) de-veloped a codable ECG finding during the3-minute walk, and 102 (17.9%) developedsome codable item of S-T depression, prin-cipally at the latest recording of the 3-minutetest. Two men (0.4% of 570) developed somecodable item of S-T elevation; one man (0.2%)developed a transient complete right bundle-branch block during effort, and three men(0.5%) developed a bigeminal rhythm or runs
of two or more ventricular premature beats.Seventeen men (3.0% of 570) developed iso-lated premature beats to the extent of 10% orgreater of recorded heart cycles, and one man
(0.2%) developed a codable negative Twave (in the absence of any codable S-T de-pression).
In table 3 is the distribution of S-T dis-placement (absolute rather than relative to theresting level) for the population under theconditions described. Fewer than 1% of this
Table 1
Code Definition
IV-0 J point depression1 J point depression2 J point depression3 J point depression4 = J point depression5 J point depression6 Segment elevation7 Segment elevation
V- T wave negative 0.5 mv
2 T wave negative 0.1 but < 0.5 mv
3 T wave negative < 0.1 mv4 = T wave low or notched
VII-1 Complete left bundle-branch block2 = Complete right bundle-branch block
VIII-1 10% premature beats2 = Bigeminy or runs of premature beats3 = Atrial fibrillation
0.2 my ischemic (horizontal or downward slope)0.1 but <0.2 my ischemic (horizontal or downward slope)0.05 but <0.1 mv ischemic (horizontal or downward slope)
<0.05 my ischemic (horizontal or downward slope)0.2 nv junctional (upward S-T slope)
~- 0.1 but <0.2 my junctional (upward S-T slope)0.1 but < 0.2 mv junctional (upward S-T slope)0.2 mv
Circulation, Volume XXXIV, Deccmber 1966
1036
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM AND EXERCISE
Table 2Findings in a Chest-Manubrium ECG Lead (CM.) Used for Monitoring During Tread-mill Exercise among 725 Consecutively Examined Rail Employees, Men Ages 45-64
No. of men
Total examined with lead CM5 725Technically adequate records obtained during work 636 (87.7% of 725)Technically adequate records and entirely "normal" 570 (89.6% of 636)
standing rest controlTechnically adequate records, "normal" standing rest 126 (22.1% of 570)
control and some codable finding during work
Findings in 126 men with "positive" tests during exercise
ECG item No. of men % of 570 men*
Codable S-T depression during work 102 17.9S-T elevation - 0.1 mv 2 0.4Negative T wave without S-T depression 1 0.2Complete right bundle-branch block 1 0.2Bigeminy or ventricular tachycardia 3 0.5in 10% extrasystoles 17 3.0
*All the men having technically adequate records and "normal" standing rest control.
working group had "ischemic type" of S-Tdepression during work at this level while17.2% had J-point S-T depression of 0.1 mv(1 mm) or more. About 3% had J depressionof 0.2 mv (2 mm) or more.
Transthoracic Bipolar Lead (CC5)In table 4, results in the CC5 lead are ex-
amined with less confidence because the num-
bers are fewer. More than half the CC5 rec-
ords during work were too "noisy" to attemptclassification of S-T-T findings by eye.
A total of 724 men of the same generalpopulation, though different men, were testedconsecutively with the CC5 lead. In only 311
(43.0%) were the records subjectively con-
sidered suitable for S-T-T coding, though allserved their original principal purpose ofobtaining a work heart rate.Of the 311 men 33 (10.6%) had a codable
ECG finding in the standing rest control rec-
ord prior to the treadmill test. Of the 278men (89.4% of 311) who had no codable rest-ing item, 40 (14.4% of 278) had codablefindings during exercise. Twenty-five (9.0%)were codable owing to S-T depression, two
(0.7%) owing to S-T elevation, one man (0.4%)had only a negative T wave during exercise;three men (1.1%) had bigeminal rhythm or
Table 3Distribution of Maximum S-T Displacement in a Chest-Manubrium Lead (CM5) DuringExercise Among 570 Rail Employees, Men Ages 45-64, Having Techlnically Good and"Normal" Standing Rest Control Records
Class No. of men % of 570 men
S-T depression classes1. 0.2 mv ischemic type 1 0.22. 0.1 but <0.2 mv ischemic type 1 0.23. 0.05 but < 0.1 mv ischemic type 2 0.44. < 0.05 mv ischemic type 0 0.05. 0.2 mv junctional type 16 2.86. 0.1 but <0.2 mv junctional type 82 14.4
S-T elevation classes1. 0.1 but < 0.2 mv segmental elevation 2 0.42. 0.2 mv segmental elevation 0 0.0
No codable "J" or segment displacement 466 81.8
Circulation, Volume XXXIV, December 1966
1037
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from

BLACKBURN ET AL.
Table 4Findings in a Bipolar Transthoracic ECG Lead (CCJ) Used for Monitoring DuringTreadmill Exercise among 724 Consecutively Examined Rail Employees, Men Ages45-64 Years
No. of men
Total examined with lead CC5 724Technically adequate record obtained during work 311 (43.0% of 724)Technically adequate records and entirely "normal" 278 (89.4% of 311)
standing rest controlTechnically adequate records, "normal" standing rest 40 (14.4% of 278)
control and some codable finding during work
Findings in 40 men with "positive" test during exercise
ECG item No. of men % of 278 men*Codable S-T depression during work 25 9.0S-T elevation > 0.1 mv 2 0.7Negative T wave without S-T depression 1 0.4Complete right bundle-branch block 0 0.0Bigeminy or ventricular tachycardia 3 1.1> 10% extrasystoles 9 3.2
*All the men having technically adequate records and "normal" standing rest control.
runs of ventricular premature beats; and nine(3.2% of 278) had frequent isolated prematurebeats.There were no ventricular conduction de-
fects during exercise in those with technicallyadequate and normal resting control CC5records. However, the proportion of thesefindings was similar to the CM5 examinedgroup if the technically poor CC3 records are
considered in the analysis.In table 5, among the 27 men with S-T-T
displacement in lead CC-, 25 (9.0% of 278)had codable S-T depression while two hadS-T elevation of at least 0.1 but less than 0.2
mv (0.7% of 278). However, only four men
(1.4% of 278) had S-T junctional (J) depres-sion of as much as 0.2 mv, while none hadischemic type depression.Overall Findings
In table 6 are pooled items for all men forthose ECG findings largely unrelated to thelead system or technical quality of the records(since these items are easily identified even
in "noisy" tracings) in order to boost the
confidence levels for their prevalence estimatesin a middle-aged group of working men. The1,305 men who did not have ECG findingsin the resting control record provide the
Table 5Distribution of Maximum S-T Displacement in a Bipolar Transthoracic ECG Lead (CC)During Exercise Among 278 Rail Employees, Men Ages 45-64 Years, Having TechnicallyGood and Normal Control Records During Standing Rest
Class No. of men % of 278 men
S-T depression classes1. >. 0.2 mv ischemic type2. > 0.1 but < 0.2 mv ischemic type3. > 0.05 but < 0.1 mv ischemic type4. < 0.05 mv ischemic type5. > 0.2 mv junctional type6. 5. 0.1 but < 0.2 mv junctional typeS-T elevation classes1. 5 0.1 but < 0.2 mv segmental elevation2. > 0.2 mv segmental elevationNo codable J or segment displacement
0
0
0
0
421
20
251
0.00.00.00.01.47.6
0.70.0
90.3
Circulation, Volume XXXIV, December 1966
1038
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELECTROCARDIOGRAM AND EXERCISE
Table 6Overall Prevalence of Frequent (10o) Premature Beats, Conduction Defects, and Ar-rhythmias During a Three-Minute Moderate-Exercise Treadmill Test, Among 1,305Working Railmen, Ages 45-64 Years, in Whom the Control Record at Standing Rest DidNot Contain These ECG Findings
ECG item No. of men % of 1,305 men*
, 10% of extrasystoles 30 2.3Bigeminy or ventricular tachycardia 10 0.8Complete right bundle-branch block 1 0.1Atrial fibrillation 1 0.1
*All the men without these findings in the resting control record.
denominator. Thirty men (2.3% of 1,305) hadisolated extrasystoles in as many as 10% ofrecorded beats during exercise. Ten men
(0.8% of 1,305) had bigeminal rhythm or runs
of two or more ventricular premature beats.One (0.1%) developed complete right bundle-branch block and another atrial fibrillationduring effort.
Finally the paradox of a T-wave "anom-aly" at rest, disappearing during effort, was
tabulated. Forty-nine among 1,449 men (3.2%)had either a notched, flat, diphasic, or dis-tinctly inverted T wave in the resting standingcontrol record. Of these 49, 20 (40.8%) showedno such T abnormality during exercise.
Discussion
TechniqueThe C5-to-manubrium chest lead (CM5)
yielded, under field conditions, twice the pro-
portion of records susceptible to detailed S-Tclassification by eye as the transthoracic leadCC5. However, its use in a consecutive seriesof examinations followed use of the CC5 lead,and improvements over time in electrodes andother techniques perhaps exaggerate the su-
periority of the CM5 configuration. Neverthe-less, in an earlier study2 with other variableskept constant, several bipolar leads werecompared during increasing levels of physicalwork, from deep breathing to running at 7mph (fig. 3). The CM5 lead was demonstrablysuperior to CC5 in regard to base-line shift(0.17 mv CM5 versus 0.32 mv CC5 mean peak-to-peak amplitude of shift) and in strengthof the ECG signal compared to the base-line"noise" (9.6 signal-to-noise ratio in CM5 ver-
sus 3.8 in CC5). This superiority is based
Circulation, Volume XXXIV, December 1966
largely on the fact that few muscle potentialsoccur and motion is minimal, under the sternalreference electrode. These technical differ-ences in lead systems have now been re-duced as a result of newer developments inskin-electrode contact. A number of electrodesand lead configurations are under systematicstudy using more quantitative assessments ofperformance, by a U. S. Public Health Ser-vice Technical Group on Exercise Electrocar-diography.
Findings at RestThe identical total prevalence of codable
ECG findings in the standing control recordsfor the two lead systems (10.4 versus 10.6%)speaks for comparability of the two groups ofrailway workers tested consecutively.
In any search for lead configurations givingmaximal and predominantly upright QRSdeflections, the lead vector may be sufficientlyposteriorly oriented to place the mean hori-zontal plane T vector near 90° from theQRS.2 Consequently, with very small pos-terior shifts of mean QRS which may occuron assumption of the upright posture, a smallproportion of subjects develop notched, lowamplitude, or negative T waves.7 The clinicalsignificance of this phenomenon is not known.The problem must be considered if standard-ization of electrode position is desired and, aswas found here, as many as 3.2% of 1,449 work-ing men have such notched, flat diphasic, ordistinctly negative T waves while standing atrest. Almost identical proportions of orthostaticT-wave findings are reported in several normalgroups.8 9 The problem applies to convention-al and other lead arrangements as well. A
1039
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from

BLACKBURN ET AL.
Figure 3
Relative performance during work of five nonstandard leads used for monitoring exercise, otherconditions equal.Activity: 1, deep breathing; 2, arm swinging; 3, 2-step test; 4, 3 mph 5% treadmill walk; and 5,7 mph 5% treadmill run.
similar order of frequency of "abnormal" rest-ing T waves has been found in this laboratoryin precordial lead V5 on assuming the uprightfrom the supine posture (unpublished observa-tions). Semler has found this postural T waveless prevalent in a bipolar lead with the ref-erence electrode under the right clavicle.7Model studies here indicate that this producesa slightly more anteriorly directed lead vector.The postural effect is perhaps not so seri-
ous (1) if the testing posture is similar forrest, work, and recovery records, (2) if meansare devised for quantitating the change in theS-T-T region between rest, exercise and re-covery, (3) if S-T depression itself, in contrastto T-wave amplitude, is little affected, andeventually, (4) if orthogonal leads can beemployed and vectorial changes in spaceanalyzed.Findings During Exercise
Similar prevalence of premature beats, afrequent finding during work (3.0 versus3.2%), in leads CC5 and CM5 also suggeststhat the workers compared were not different.This in turn would confirm that the two-leadsystems truly differ in regard to "sensitivity"of display of S-T segment depression phenom-ena, since codable S-T depression occurred
in only 9.0% of CC5 records versus 17.9%of CM-, records. This difference in S-T dis-play has been previously demonstrated insimultaneous records of the same individualshaving S-T depression at rest2 and is shownin figure 1. It has recently been found insimultaneous records of cases with S-T de-pression during work.10 Though much of thelead differences in S-T display are attributableto differences in lead strength with regardto QRS forces, some is undoubtedly due tooptimal lead orientation for S-T vector dis-play.2The frequently observed phenomenon of
negative T waves at rest which become "nor-mal" or upright during or immediately afterexercise requires clarification best achievedthrough studies with orthogonal ECG leadsand follow-up observation. In 40% of the casesof standing rest T anomalies in these simplebipolar leads, the "paradox" of T becomingupright was observed during effort. The clin-ical significance of this is not clear since inthe other 60% of these cases the negative Twave persists or becomes more negative.Standards
Within the conditions of this study, employ-ing simple bipolar chest leads in middle-aged
Circulation, Volume XXXIV, December 1966
1040
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from
ELECTROCARDIOGRAM AND EXERCISE
working men, under a moderate work loadcomparable to clinical step tests (±+ 1.4 L 02/min), the following may be considered "ab-normal" responses during effort, on the basisof a statistical approach to the total distribu-tion in which findings in excess of the 95%upper limits are regarded abnormal:
1. Ischemic S-T depression of any percep-tible degree (0.05 mv or more).
2. Junctional S-T depression of 0.2 mv ormore.
3. S-T segment elevation of 0.1 mv or more.
4. Arrhythmias, ventricular conduction de-fects, and 10% or more frequency of pre-mature beats.
Significance and Conclusions
The use of simple bipolar chest leads inexercise electrocardiography may not, in theend, be preferable to conventional leads, or-thogonal leads, or specially "distorted" leads.At least in this country where conventionallimb and Wilson chest leads are standard forrest and recovery periods, their use formonitoring during work, assuming technicallygood records are obtainable, is logical untilinformation from other lead derivations isdemonstrated to be comparable or supe-rior.6 11
Nevertheless, during this period of chang-ing methodology and improving instrumenta-tion, the empirically developed bipolar chestleads have given practical advantages of few-er electrodes and cables, fewer artifacts dur-ing motion, and displays of wave forms suf-ficiently similar to the familiar central terminalleft precordial leads to permit qualitativeevaluation of the ECG response to work.The findings and suggested criteria for ab-
normal responses to moderate work in theseleads recorded from middle-aged working menare similar to those derived from convention-al leads in post-exercise records.8 9,1113 Theywould probably not apply to high levels ofwork load near maximal work capacity, duringwhich greater changes, in a much higher pro-portion of men, have been reported."1 14, 15
If the facts&are considered that conventionalCirculation, Volume XXXIV, December 1966
Wilson chest lead V5 probably gives 90% ofthe information obtainable from the exerciseECG response,16 and that some bipolar chestleads have greater lead strength and sensitivityto S-T depression display than V5,2 it is likelythat this type of lead configuration is ratheroptimally sensitive for monitoring and screen-ing purposes. If in addition the confirmatoryinformation and extensive experience of Scan-dinavian work physiologists,9 17 and investi-gators in the space program and in physicaleducation'8 are considered, it appears thatsimple bipolar chest lead ECG systems maybe practically and profitably employed inscreening and monitoring programs until anacceptable standard quantitative approachis available.The question of diagnostic discrimination
between normals and subjects with coronaryinsufficiency is not examined in this presen-tation of distributions in a working popula-tion. Semi-quantitative approaches similar tothis one have indicated that the exercise ECGresponse at comparable work levels is nothighly discriminatory.8 19 Quantitation of theECG response, at higher work levels, prom-ises better discrimination and predic-tion.11, 14, 15, 17
The important question of response fidelityat the lower end of the recording system de-termining the S-T response is not here con-sidered. Berson and Pipberger20 most recentlyexamined this problem and found that thelow-frequency cut-off of instruments with thedecay time characteristics of those used in thisstudy might result in 3% of the records having0.1 mv or more error in the S-T amplitude.This error is dependent on the form of theQRS, whether predominantly up or down or
equiphasic and the symmetry of the waveslopes. They proposed reducing these errorsby one half through lowering the lower fre-quency filter pass to 0.05 cps in the situationin which the amplitude decreases to one halfwhen the frequency decreases to one half(6 db per octave roll-off ) .
Studies are now being made to synthesizethe ECG curves faithfully by playing these
1041
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLACKBURN ET AL.
taped records through circuits with the in-verse characteristics of the recording instru-ments.2' It is hoped thereby to obtain a bet-ter approximation of the instrument error inS-T segment displacement.
Summary and Conclusions
Nonstandard ECG leads and recordingprocedures are being applied in monitoringthe ECG response during performance tests.Detailed systematic studies in well-definedpopulations with adequate control of thenumerous variables of electrode position, bodyposture, the type, amount, and duration ofwork, recording intervals, and instrumentationare required before the "dynamic" ECG re-sponse may be interpreted with confidence.This study reports the distribution of ECG
findings during moderate treadmill exercise ina group of 1,449 working men in the railroadindustry of ages 45 to 64. Two bipolar chestleads commonly used in work monitoringwere compared, each with the exploring elec-trode at chest position C, one with the ref-erence opposite at C5R (CC,5) and the otheron the manubrium (CM-). Ninety-six per centof the examined men, excluding those withmanifest cardiac or other disabilities, weresubjected to a 3-minute treadmill walk at 3mph on a 5% grade, and the maximal codableS-T or other findings was used in the analysis.About 90% of all men had standing control
records free of any codable ECG finding. Lessthan 1% of these developed ischemic type ofS-T depression during work. About 2% de-veloped J (junctional) type of S-T depressionof 0.2 mv (2 mm) or greater. Less than 1%developed significant ventricular blocks orarrhythmias, and about 3% developed frequentextrasystoles. Any of these findings duringmoderate exercise may then, on a statisticalbasis, be considered an "abnormal" response.The discriminative diagnostic power of theECG responses during exercise is poor, how-ever, and evidence about its predictive importfor future disease risk requires careful quan-titation and follow-up studies.
Standardization of methods for exercise elec-trocardiography is not yet possible because of
rapid developments in theory and instrumen-tation. When it is not feasible to obtain gooddata from conventional limb and precordialleads, information from simple bipolar chestleads may be profitably utilized in screeningand monitoring programs. This should be atemporary expedient, until a practical andacceptable quantitative approach is availablefor exercise electrocardiography.
References1. BLACKBURN, H.: The electrocardiogram in car-
diovascular epidemiology: Problems in stan-dardized application. Ann NY Acad Sci 126:882, 1965.
2. BLACKBURN, H., TAYLOR, H. L., OKAMOTO, N.,MITCHELL, P. L., RAUTAHARJU, P. M., ANDKERKHOF, A. C.: The exercise electrocardio-gram: A systematic comparison of chest leadconfigurations employed for monitoring duringexercise. In Physical Activity and the Heart.Edited by M. Karvonen and A. Barry, Spring-field, Illinois, Charles C Thomas, Publisher,1966.
3. TAYLOR, H. L., BLACKBURN, H., BROZEK, J.,PARLIN, R. WV., AND PUCHNER, T.: Coronaryheart disease among selected railroad occupa-tions. In Keys, A. and Collaborators: Popula-tion Studies Related to Coronary Heart Dis-ease. Acta Med Scand (suppl.) 1966.
4. BLACKBURN, H., TAYLOR, H. L., PARLIN, R. WV.,KIHLBERG, J., AND KEYS, A.: Relation of oc-cupational physical activity and cigarettesmoking to ventilatory function and respira-tory symptoms. Arch Environ Health (Chi-cago) 10: 312, 1965.
5. RAUTAHARJU, P., AND BLACKBURN, H.: Theexercise electrocardiogram: Experience in anal-ysis of "noisy" cardiograms with a small com-puter. Amer Heart J 69: 515, 1965.
6. MASON, R. E., AND LIKAR, I.: A new systemof multiple lead exercise electrocardiography.Amer Heart J 71: 196, 1966.
7. LACHMAN, A. B., SEMLER, H. J., AND GUSTAF-SON, R. H.: Postural ST-T wave changes inthe radioelectrocardiogram simulating myo-cardial ischemia. Circulation 31: 557, 1965.
8. LEPESCHKIN, E., AND SURAWICz, B.: Character-istics of true-positive and false-positive re-sults of electrocardiographic Master two-stepexercise tests. New Eng J Med 258: 511, 1958.
9. STRANDELL, T.: Electrocardiographic findingsat rest, during and after exercise in healthyold men compared with young men. Acta MedScand 174: 479, 1963.
Circulazion. Volume XXXIV, December 1966
1042
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from

ELECTROCARDIOGRAM AND EXERCISE
10. BLACKBURN, H., RAUTAHARJU, P., AND MAZ-ZARELLA, J.: Comparative findings in com-monly used bipolar ECG monitoring leads.In preparation.
11. SHEFFIELD, L. T., HOLT, J. H., AND REEVES,T. J.: Exercise graded by heart rate in elec-trocardiographic testing for angina pectoris.Circulation 32: 622, 1965.
12. MATTINGLY, T. W.: The post-exercise electro-cardiogram: Its value in the diagnosis andprognosis of coronary arterial disease. AmerJ Cardiol 9: 395, 1962.
13. ROBB, G. P., AND MARKS, H. H.: Latent coro-nary artery disease. Amer J Cardiol 603:1964.
14. BLOMQVIST, G.: The Frank lead exercise electro-cardiogram: A quantitative study based onaveraging technique and digital computeranalysis. Acta Med Scand 178: (suppl. 440)1965.
15. DOAN, A. E., PETERSON, D. R., BLACKMON,J. R., AND BRUCE, R. A.: Myocardial ischemia
after maximal exercise in healthy men. AmerHeart J 69: 11, 1965.
16. BLACKBURN, H., AND KATIGBAK, R.: What elec-trocardiographic leads to take after exercise?Amer Heart J 67: 184, 1964.
17. ASTRAND, I.: Exercise electrocardiograms in afive year follow-up study. Acta Med Scand173: 257, 1963.
18. BRUCE, R. A., MAZZARELLA, J. A., JORDON, J. W.,AND GREEN, E.: Quantitation of QRS andS-T segment responses to exercise. Amer HeartJ 71: 455, 1966.
19. FRIEDBERG, C. K., JAFFE, H. L., PoRDY, L.,AND CHESKY, K.: The two-step exercise elec-trocardiogram: A double-blind evaluation of itsuse in the diagnosis of angina pectoris. Cir-culation 26: 1254, 1962.
20. BERSON, A. S., AND PIPBERGER, H. V.: Thelow-frequency response of electrocardiographs,a frequent source of recording errors. AmerHeart J 71: 779, 1966.
21. SCHMITT, 0. H.: Averaging techniques employ-ing several simultaneous physiological vari-ables. Ann NY Acad Sci 115: 952, 1964.
Twenty-five Years Ago
No nation can isolate itself. No progress is possible if the mind is shackled with theauthority of this or that system, merely because it is national. ...We should not be in the grip of the dead past, nor should we be awed by authority
but we may not forget that the past has claims over us. The evolution of modemmedicine is a series of successes over false beliefs. The present is the child of the past,and, to understand it properly, a historical outlook is essential. Physicians with suchan outlook do not hanker after miracles and are not easily lured away from the scientificpath by the false promises of pseudoscience, quackery and the fashionable cults of theday.-Editorial: About Ourselves. Indian Physician 1: 2, 1942.
Circulation, Volume XXXIV, December 1966
1()43
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from

C. PUCHNERHENRY BLACKBURN, HENRY L. TAYLOR, C. LUIS VASQUEZ and THOMAS
1,449 Middle-Aged Men, at Moderate Work LevelsThe Electrocardiogram During Exercise: Findings in Bipolar Chest Leads of
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1966 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.34.6.1034
1966;34:1034-1043Circulation.
http://circ.ahajournals.org/content/34/6/1034.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 7, 2018http://circ.ahajournals.org/
Dow
nloaded from