predictive accuracyofcoronaryartery calcification...
TRANSCRIPT

VOL 62, No 6, DECEMBER 1980
tion of the circumflex branch of the left coronary artery in con-scious dogs. Circ Res 22: 237, 1968
57. Buckberg GD, Fixler DE, Archie JP, Hoffman JIE: Ex-perimental subendocardial ischemia in dogs with normal cor-onary arteries. Circ Res 30: 67, 1972
58. Bache RJ, Cobb FJ, Greenfield JC: Myocardial blood flow dis-tribution during ischemia induced coronary vasodilatation in
the unanesthetized dog. J Clin Invest 54: 1462, 197459. Ball RM, Bache RJ: Distribution of myocardial blood flow in
the exercising dog with restricted coronary artery inflow. CircRes 38: 60, 1976
60. Young DF, Cholvin NR, Roth AC: Pressure drop across ar-tificially induced stenoses in the femoral arteries of dogs. CircRes 36: 735, 1975
Predictive Accuracy of Coronary Artery Calcificationand Abnormal Exercise Test for Coronary Artery
Disease in Asymptomatic Men
RENE A. LANGOU, M.D., EDWIN K. HUANG, M.D., MICHAEL J. KELLEY, M.D.,AND LAWRENCE S. COHEN, M.D.
SUMMARY To determine the predictive accuracy of fluoroscopically detected coronary artery calcification(CAC) and a positive submaximal exercise test, 129 asymptomatic men were screened; 13 had both coronaryartery calcification and positive exercise test (2 1.0 mm ST-segment depression). These 13 men were studiedat coronary arteriography. They had a mean age of 44 years (range 41-56 years); none had history or symp-toms of heart disease and all had normal resting ECGs at entry.CAC was detected in one artery in 10 men, in two arteries in two men, and in three arteries in one man.
Coronary artery disease (CAD) was considered clinically significant if any major coronary branch wasnarrowed > 50%. Coronary arteriography revealed 12 men with clinically significant CAD (one-vessel CAD infour, two-vessel CAD in five and three-vessel CAD in three men) and one man with minor one-vessel CAD. Thepredictive accuracy was 100% for minor CAD and 92% for clinically significant CAD. The location of CACand CAD correlated, but the absence of CAC did not rule out the presence of CAD at coronary arteriography.Furthermore, CAC did not indicate the location of the highest stenotic (most occlusive) lesions seen atarteriography. Follow-up for the 13 patients was 36 months; three patients developed typical angina and one
patient developed a transmural myocardial infarction.This study suggests that the predictive accuracy of CAC and a positive exercise test in the middle-aged non-
hyperlipidemic asymptomatic male is very high (100% for CAD and 92% for clinically significant CAD) andthat CAC and a positive exercise test predict an early appearance of angina or myocardial infarction inpreviously asymptomatic men.
THE EMPHASIS on early diagnosis and preventionof ischemic heart disease has stimulated a search forreliable noninvasive methods of detection.1 3 Risk fac-tor screening and resting ECGs are useful in epi-demiologic and mass screening programs but are notdiagnostically helpful in the asymptomatic subject.Although exercise electrocardiography4`6 is widely
used as a noninvasive procedure to diagnose coronaryartery disease, the large proportion of false-positiveand false-negative results precludes its use as a stan-dard screening device in the asymptomatic person.7-9Clinical or laboratory markers that might identifythose with asymptomatic coronary artery diseasewould be useful. Previous reports have established the
From the Department of Internal Medicine, Cardiology Section,and the Department of Diagnostic Radiology, Yale UniversitySchool of Medicine, New Haven, Connecticut.
Address for correspondence: Rene A. Langou M.D., CardiologySection, Yale University School of Medicine, 333 Cedar Street, 87LMP, New Haven, Connecticut 06510.
Received January 16, 1980; revision accepted April 1, 1980.Circulation 62, No. 6, 1980.
positive relationship between the presence of coronarycalcification on fluoroscopy and angiographicallydemonstrated coronary artery disease in symptomaticpatients. 12-12
In this study we used exercise electrocardiographyand cardiac fluoroscopy to screen asymptomatic sub-jects as part of a prospective clinical researchprotocol. This report presents the value of combiningthe electrocardiographic response to exercise andfluoroscopically detected coronary artery calcificationin asymptomatic subjects and the clinical course ofasymptomatic subjects that have both an abnormalelectrocardiographic response to exercise and cor-onary artery calcification on fluoroscopy.
Materials and MethodsThe study group of 129 middle-aged males vol-
unteered for two-part examinations consisting of (1)cardiac fluoroscopy and a submaximal exercise stresstest; and (2) cardiac catheterization in subjects whohad coronary artery calcification on fluoroscopy andan abnormal electrocardiographic response to sub-
1196 CIRCULATION
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

CAD DETECTION IN ASYMPTOMATIC MEN/Langou et al.
maximal exercise. In addition, complete clinicalfollow-up information was gathered in the cohortpopulation.
This prospective research protocol was reviewedand approved by the Yale University School ofMedicine Human Investigation Committee. Allvolunteers gave informed consent before they were in-cluded in this study. No subject who participated inthe study had a known history of congenital or ac-quired heart disease and all considered themselves ingood health, without chronic illness or recenthospitalization. A questionnaire supplemented bydirect questioning excluded any history of angina pec-toris, myocardial infarction or congestive heartfailure. The diagnosis of recent or remote myocardialinfarction by ECG was excluded by the criteria estab-lished by the New York Heart Association.13 Any ab-normal cardiac rhythm, a resting diastolic bloodpressure greater than 100 mm Hg or an S3 gallop atrest were also bases for exclusion from the protocol.Additional data obtained included screening forhistory of hypertension (diastolic systemic pressuregreater than 100 mm Hg); diabetes mellitus; lipid ab-normalities (Frederickson classification); obesity(body weight 10% over ideal weight for sex and age); afamily history of ischemic heart disease (angina pec-toris, myocardial infarction, congestive heart failureand sudden death); and cigarette use (average dailyconsumption). Diabetes mellitus, lipid abnormalities,obesity, or smoking were not bases for exclusion fromthe protocol.
Cardiac Fluoroscopy
Cardiac fluoroscopy was performed by an exper-ienced cardiovascular radiologist. It consisted in se-quential visualization of the heart in four views (leftlateral, 600 left anterior oblique, posteroanterior and450 right anterior oblique), using a standard 10-inchcesium iodine image intensifier with a 0.6-mm smallfocal spot, a 1-mm focal spot and an adjustable shut-ter. The x-ray unit was equipped with a videotape re-corder. All studies were reviewed for confirmation ofinitial impressions.
Criteria for identification of coronary calcificationand classification according to its location has beenpublished by this laboratory.'4 In summary, coronarycalcification was considered present if calciumdeposits appeared during suspended respiration assmall, rapidly moving densities distributed throughoutthe proximal portion of the coronary arteries overly-ing the cardiac image. Calcification was classified bylocation in the left anterior descending, left circumflexor right coronary artery. We did not attempt tospecify lesions located in the peripheral coronary treeor to distinguish proximal left anterior descendingfrom left main coronary artery calcification.
Exercise Stress Testing
A resting ECG and a physical examination wereperformed before the stress test. Subjects were in-structed to fast for 2 hours before the examination.
Exercise testing was completed on a bicycle ergometeraccording to a method previously described.15 Weattempted to exercise each subject to 90% of his age-predicted maximal heart rate. Premature terminationof the exercise test most often resulted from fatigue,dyspnea or leg pain. No subject had severe anginalpain or electrocardiographic ST-segment depressiongreater than 3 mm from baseline. One person wasasked to stop when premature ventricular complexesappeared in pairs. All ECGs were reviewed by one ofthe investigators, who had no knowledge of the car-diac fluoroscopic findings. An abnormal exercise elec-trocardiographic response was defined as equal to orgreater than 1 mm of horizontal or downsloping ST-segment depression in any of the four continuouslyrecorded leads. These leads included three orthogonaland a bipolar V5 (CC5). We required that these abnor-malities be present during or immediately after exer-cise and persist for at least 2 minutes in the recoveryperiod. One hundred eight of the original 129 subjectscompleted the submaximal exercise protocol byachieving at least 90% of their age-predicted maximalheart rate; these subjects make up the cohort popula-tion for this study.
Cardiac Catheterization
Cardiac catheterization was performed on all 13subjects who demonstrated both coronary arterycalcification on fluoroscopy and a positive exercisestress test. This study included routine hemodynamicmeasurements; a single-plane, 300 right anterioroblique, left ventriculogram; and selective coronaryarteriography. This procedure was performed only insubjects who had both coronary artery calcification onfluoroscopy and an abnormal exercise ECG. All ofthese subjects had a cardiac catheterization an averageof 8 months (range 5-12 months) after entering intothe study.Coronary artery disease was considered present
when any major coronary artery (left anterior descend-ing, circumflex or right coronary artery) or theirrespective large branches had at least a 30% discreteor diffuse reduction in caliber. Arterial stenoses wereestimated by percent of narrowing of the vessel.Significant coronary artery disease was consideredpresent if at least one major coronary artery or one ofits major branches had a 50% or greater obstruction;insignificant coronary artery disease was present if thenarrowing was 30-50%.
All angiographic data were read independently bythe attending cardiologist and by one of the authors.When differences in interpretation occurred, theangiograms were reevaluated and a consensus wasreached.
Follow-up
Since the initiation of this protocol in September1976, all subjects were interviewed every 12 months. Adetailed questionnaire was answered, with specificquestions regarding the appearance of angina pectoris,myocardial infarction and congestive heart failure.
1197
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 62, No 6, DECEMBER 1980
Subjects with coronary calcification on fluoroscopyand an abnormal exercise ECG were interviewed at 6-month intervals. In addition, follow-up physical ex-aminations, resting ECGs and exercise stress testswere performed at yearly intervals.Angina pectoris was defined as: (1) definite- a sub-
sternal, shoulder, jaw or arm discomfort precipitatedby exertion, relieved by rest and/or nitroglycerin inless than 10 minutes, and with a typical radiation;(2) probable - having most of the features of classicangina but in some aspects not entirely typical; and (3)probably not angina - a constellation of symptomsthat did not fit the description of definite angina.
Myocardial infarction was diagnosed if there was ahistory of myocardial infarction in which the hospitalrecords, including information on cardiac enzymesand copies of the ECG were available. Probable myo-cardial infarction was diagnosed if the history waspositive for electrocardiographic and enzyme changes(records not available), the patient had been hospital-ized for longer than 2 weeks, but the current ECG didnot show definite myocardial infarction, or there wasno clear history of myocardial infarction but the cur-rent ECG showed previous myocardial infarction.
Congestive heart failure was diagnosed if there wereclinical symptoms and/or radiographic signs ofpulmonary congestion or evidence of elevatedsystemic venous pressure, congestive hepatomegaly,ascites or peripheral edema. An associated ventriculargallop, although often present, was not required.
PopulationThe mean age of the 108 men was 46 years (range
40-64 years). Of these 108 subjects, 85 (79%) had ahistory of smoking and 35 (32%) had a positive familyhistory for ischemic heart disease. Eighteen subjects(16%) had hypertension; 45 (41%) were obese; two(1.8%) had diabetes mellitus; and eight (7%) hadhyperlipidemia. The resting ECG was normal in 92(85%) of the subjects and it revealed minimal, non-specific ST-T-wave changes in 16 (15%) subjects. Onlyfour of the 108 men (4%) had a previous exercise stresstest as part of a routine annual physical examinationand none had any abnormalities.
Analysis of Data and Statistical MethodsPredictive accuracy was obtained using the formula
True positive testsTrue positive + false positive tests
and was expressed as percent.Chi-square analysis was used to examine all data.
Uncorrected chi-square values were used in all in-stances, except for the 2 X 2 matrixes where Fisher'sexact values were used.`6 A p value of less than 0.05was considered statistically significant.
ResultsCardiac Fluoroscopy
Calcification of at least one coronary artery was de-tected by fluoroscopy in 37 (34%) of the 108 subjects.
Left coronary artery calcification accounted for 34 ofthe 40 observed calcified vessels. The left anteriordescending artery calcification was significantly morecommon than left circumflex (47.5% vs 37.5%) or theright coronary artery (15%). Solitary calcification ofthe right coronary artery was uncommon. Only threeof the six subjects with right coronary artery calcifica-tion had a fluoroscopically normal left coronarysystem. Two- and three-vessel calcification was rare.
Exercise Stress Testing
Sixteen of the 108 subjects (15%) had an abnormalexercise ECG. Thirteen of the 16 (81%) had at leastone calcified coronary artery on fluoroscopy. In con-trast, 13 (35%) of the 37 subjects with coronary arterycalcification of at least one coronary artery had apositive exercise test. Table 1 lists the results of car-
diac fluoroscopy vs exercise stress testing.
Excluded Subjects
The 21 subjects who failed to attain heart rateswithin 10 beats of their target goal of the exercise testwere considered to have insufficient stress on their car-
diovascular systems to completely rule out exercise-in-duced ischemia. Although excluded from the analysisand report, they did not differ significantly from theremainder of the population in demographic, clinicalor fluoroscopic findings.
Cardiac Fluoroscopy and Exercise Stress Testing
Thirteen of the original 108 subjects had at least onecalcified coronary artery on fluoroscopy and an abnor-mal exercise ECG. These 13 men had a mean age of 44years (range 41-56 years); eight (6 1%) had a history ofsmoking and seven (54%) had a positive history ofischemic heart disease in their family. None hadhypertension and three (23%) had hyperlipidemia.Coronary artery calcification was detected in one
artery in 10 subjects; in two arteries in two subjects;and in all three arteries in only one subject. The dis-tribution of calcification in the coronary tree followedthe general trend seen in the overall group of 108 sub-jects. The left anterior descending artery was involvedin 10 instances (eight as one-artery calcification andtwo as part of two- and a three-vessel calcifications);the left circumflex artery was affected in five instances(two as single artery calcification and three as part oftwo- and three-vessel calcifications); and the right cor-
TABLE 1. Exercise Stress Test Results vs Coronary ArteryCalcification on Fluoroscopy
Exercise stress test (ECG)Normal respornse Abnormal response Total
n %7 n '7
No coronarycalcification 68 96 3 4 71
Coronarycalcification 24 65 13 35 37
Total 92 85 16 15 108
1198 CI RCULATION
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

CAD DETECTION IN ASYMPTOMATIC MEN/Langou et al.
TABLE 2. Correlation Between Angiographic Coronary Stenosesj Coronary Artery Calc~fwcation and ExerciseStress Test in Asymptomatic Men
CoronaryAngiography calcification Exercise test
Age No. No. ST depressionNo. (years) vessel Location % stenoses LV gram vessel Location Pain (mm)1 43 2 LAD 70% Normal 1 LAD Yes 1.5
Cix 50%2 49 1 LAD 80% Normal 1 LAD No 1
3 48 3 LAD 85% IW hypok 3 LAD No 1.5Cix 90% Ap hypok CixRCA 70% RCA
4 42 2 LAD 70% Normal 2 LAD Yes 2Cix 50% Cix
5 45 2 LAD 50% Normal 1 Cix No 1Cix 80%
6 47 1 LAD 30% Normal 1 LAD No 1.57 44 2 LAD 60% Normal 1 LAD No 2
RCA 80%8 49 1 LAD 90% Normal 1 LAD No 2
9 54 3 LAD 90% Normal 2 LAD No 1Cix 50% CixRCA 70% Cix
10 41 1 LAD 60% Normnal 1 LAD No 1.511 44 2 LAD 50% Normal 1 Cix Yes 2
Cix 70% LAD12 43 1 LAD 80% Normal 1 Cix No 2.513 41 3 LAD 70% Normal 1 LAD Yes 1
Cix 80%RCA 75%
Abbreviations: Ap = apical; Cix = circumflex artery; Hypok hypokinesis; IW = inferior wall; LAD =left anterior descending coronary artery; RCA = right coronary artery.
onary artery was calcified in only one instance (as partof a three-vessel calcification).Coronary arteriography revealed 12 men with
significant coronary artery disease (. 50% stenoses):one-vessel coronary artery disease in four subjects,two-vessel disease in five subjects and three-vessel dis-ease in three subjects. In addition, one subject had in-significant coronary artery disease (< 50% stenoses)that affected a single coronary artery (table 2).Although correlation was found between the locationof coronary artery calcification detected atfluoroscopy and the location of angiographicallydetected coronary artery stenoses, coronary arterycalcification did not necessarily indicate the presenceof coronary artery stenosis (case 12; table 2). Also, theabsence of coronary artery calcification did not ruleout the presence of coronary artery disease at cor-onary arteriography.The predictive accuracy of a calcified coronary
artery at fluoroscopy and an abnormal submaximalexercise test for clinically significant angiographicallyproved coronary artery disease was 92% [ (12/12 + 1)X 100].
Furthermore, including the additional subject withnonsignificant coronary artery disease, the predictiveaccuracy of combining both noninvasive tests to detect
angiographically proved coronary artery disease was100% (table 3). Note that these results were obtainedin the subgroup of subjects who underwent cardiaccatheterization. No information was obtained regard-ing sensitivity or specificity of an abnormal exercisetest or positive coronary calcification on fluoroscopyin these asymptomatic men because subjects havingonly one abnormal test were not catheterized.
Follow-up
A ngina Pectoris
Of the 108 subjects, five developed definite anginapectoris during the 36-month follow-up period, giving
TABLE 3. Predictive Accuracy of Coronary Artery Calcifi-cation at Fluoroscopy and Abnormal Exercise Stress Test
No.pts Significant CAD CAD
Coronary calcification+ 13 12 13
Abnormal exercise test
Predictive accuracy 92% 100%
1199
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from
VOL 62, No 6, DECEMBER 1980
a calculated occurrence of angina pectoris of 5% over
this period. Of the five subjects with definite anginapectoris, three had at least one calcified coronaryartery on fluoroscopy and an abnormal exercise ECG,one subject had coronary calcification and a normalexercise stress and one had neither coronary arterycalcification nor an abnormal exercise stress test. Con-versely, of the 13 subjects with coronary artery cal-cification and an abnormal exercise stress test, three(23%) developed definite angina pectoris. Of the 24subjects with coronary artery calcification and a nor-mal exercise stress test, one subject (4%) developeddefinite angina pectoris; and of the 68 subjects with no
coronary artery calcification and a normal exercisestress test, one subject (1.5%) developed definiteangina pectoris.
Three of the 108 subjects developed probable angina
pectoris over the follow-up period: two of the 13 sub-jects (15%) with coronary artery calcification and an
abnormal exercise stress test and one of the 68 sub-jects (1.5%) with no coronary artery calcification anda normal exercise stress test. Five of the 108 subjectsdeveloped chest pain that was considered to be
probably not angina. All five subjects were not iden-tified as having coronary artery calcification and anabnormal exercise stress test (table 4).
Myocardial Infarction
Two of the 108 subjects sustained a myocardial in-farction during the follow-up period, giving an in-cidence of 1.8% over a 36-month period one of the13 subjects (8%) with coronary artery calcification andan abnormal exercise test and another one of the 68subjects (1.5%) with no coronary artery calcificationand normal exercise stress test. One of the 108 sub-jects had a probable myocardial infarction, and thisman was in the group with no coronary calcificationand a normal exercise stress test.
Correlation Between Exercise Stress Testand Clinical Follow-up
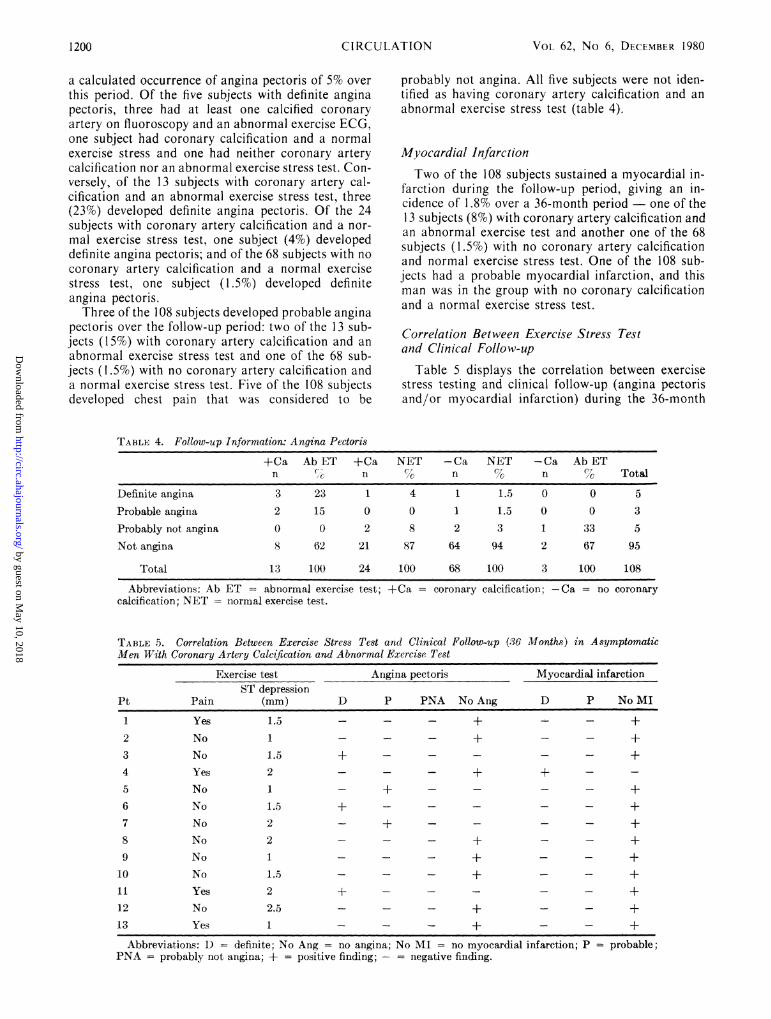
Table 5 displays the correlation between exercisestress testing and clinical follow-up (angina pectorisand/or myocardial infarction) during the 36-month
TABLE 4. Follow-up Information: Angina Pectoris
+Ca Ab ET +Ca NET -Ca NET -Ca Ab ETn c n n n % Total
Definite angina 3 23 1 4 1 1.5 0 0 5Probable angina 2 15 0 0 1 1.5 0 0 3
Probably not angina 0 0 2 8 2 3 1 33 5
Not angina 8 62 21 87 64 94 2 67 95
Total 13 100 24 100 68 100 3 100 108
Abbreviations: Ab ET = abnormal exercise test; +Ca = coronary calcification; -Ca = no coronarycalcification; NET = normal exercise test.
TABLE 5. Correlation Between Exercise Stress Test and Clinical Follow-up (36 Months) in AsymptomaticMen With Coronary Artery Calcification and Abnormal Exercise Test
Exercise test Angina pectoris Myocardial infarctionST depression
Pt Pain (mm) D P PNA No Ang D P No MI
1 Yes 1.5 - - - + - - +2 No 1 - - - + - - +3 No 1.5 + - - - - - +4 Yes 2 - - - + +5 No 1 - + - - - - +6 No 1.5 + +7 No 2 - + - - - - +8 No 2 - - - + - - +9 No 1 - - - + - - +10 No 1.5 - - - + - - +11 Yes 2 + - - - - - +12 No 2.5 - - - + - - +13 Yes 1 - - - + - - +
Abbreviations: D - definite; No Ang = no angina; No MI no myocardial infarction; P = probable;PNA = probably not angina; + = positive finding; - = negative finding.
CI RCULATION1200
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

CAD DETECTION IN ASYMPTOMATIC MEN/Langou et al.
period in the 13 asymptomatic men who had coronaryartery calcification on cardiac fluoroscopy and an ab-normal exercise ECG. Exercise-induced chest painand the magnitude of exercise-induced ST-segmentdepression were not predictive of angina pectoris orthe development of myocardial infarction in this group.
Discussion
Coronary Artery Calcification as a Predictorof Coronary Artery Disease
Despite considerable evidence from clinical andpostmortem results that suggest the diagnostic valueof detecting coronary artery calcification onfluoroscopy, only a few studies'0' 11, 17 have correlatedcardiac fluoroscopy with coronary arteriographic find-ings. Data derived from symptomatic patients under-going cardiac catheterization indicated that approxi-mately 90% of patients with coronary calcifications onfluoroscopy have significant coronary artery dis-ease.10 11 17 In a subgroup of 93 asymptomatic pa-tients from 181 type II hyperlipoproteinemic patients,Aldrich et al.17 found that the predictive accuracy ofcoronary artery calcifications to detect significant cor-onary artery disease was 46%. However, the predictiveaccuracy of a particular diagnostic test is largelydetermined by the prevalence of disease in the testedpopulation.
Abnormal Exercise Test as a Predictorof Coronary Artery Disease
Since Master completed his pioneering studies onthe use of exercise to induce electrocardiographicevidence of myocardial ischemia in the early 1940s,stress testing has been used widely as a simple, nonin-vasive method for diagnosis of coronary artery dis-ease. Angiographic studies have confirmed itsdiagnostic accuracy in predicting coronary artery dis-ease in symptomatic populations.'8 20
However, investigators2" 22 have challenged thediagnostic accuracy of the exercise ECG in predictingcoronary artery disease among asymptomatic sub-jects. Angiographic studies in asymptomatic pop-ulations with abnormal exercise stress tests haveshown a very high false-positive rate. Indeed, in thestudy of Froelicher et al.2' the rate of false-positive ex-ercise test was 56%, and in the study of Borer et al. itwas 63%.22
Coronary Artery Calcification and Abnormal ExerciseTest as Predictors of Coronary Artery Disease
Theoretically, cardiac fluoroscopy and exercisestress tests are complementary techniques forevaluating coronary artery disease, because the find-ing of coronary artery calcification provides anatomicevidence of coronary sclerosis, whereas abnormalelectrocardiographic response to exercise (exercise-induced ST-segment depression) suggests hemody-namic impairment to coronary flow.Arteriographic data for combinations of cardiac
fluoroscopy and exercise testing were reported byAldrich et al.'7 in type II hyperlipoproteinemicpatients. They reported that the predictive accuracy todetect coronary artery disease when both tests wereabnormal was 75% or higher, regardless of symp-tomatic status. When their asymptomatic group wasconsidered alone, the predictive accuracy was still veryhigh (82%).The present study reports similar findings, but the
cohort population was asymptomatic and had no cor-onary risk factors. In 13 asymptomatic males withboth coronary artery calcifications on fluoroscopy andabnormal submaximal exercise stress test, the predic-tive accuracy was 92% if coronary arterial lesions thatcaused greater than 50% stenosis were considered asevidence of coronary artery disease. However, if theangiographic criteria for coronary artery disease wasmodified to include any irregularity in the course ofthe major coronary arteries on angiography, thepredictive accuracy was 100%. These findings are notsurprising if a quantitative estimate of the diagnosticpotential of this approach is made. The combined useof cardiac fluoroscopy and exercise testing may sub-stantially enhance diagnostic reliability when testresults are concordant.23
Aldrich et al.'7 selected 181 patients from aNational Heart, Lung, and Blood Institutes Type IICoronary Intervention Program. All those patientshad type II hyperlipoproteinemia. Sixty-one patients(33%) had clinical evidence of ischemic heart disease(typical angina pectoris, myocardial infarction orboth) and 27 (15%) had clinical manifestationssuggestive of ischemic heart disease (atypical chestpain). The major criticism of that study is that theystudied and reported on a highly selected populationthat may not resemble the general population. Theauthors defended their study by pointing out thatalthough their patient population was selected, noclinical study is totally unselected. They indicated thatbecause their patients were young (below 55 years ofage), did not have hypertension or diabetes and mostwere not highly symptomatic, that their populationwas appropriate for testing reliability of noninvasivetechniques.
The present study has overcome the major deficitsof the study of Aldrich et al. Subjects were recruitedfrom a general population of healthy young males froma large service corporation based in Connecticut. Theywere asymptomatic and did not have hyperlipopro-teinemia, hypertension or diabetes. Moreover, ap-propriate clinical follow-up was obtained over a 3-yearperiod. Therefore, the results could be applied to ageneral asymptomatic population of males. Despitethe disparity between these two studies, the clinical in-terpretation is significantly similar. Cardiac fluoros-copy and exercise stress testing deserve a stronger in-vestigative effort and a wider clinical application.
Although the location of coronary calcification onfluoroscopy and the location of angiographicallydetected coronary stenoses were correlated, thepresence of fluoroscopically detected coronarycalcification did not necessarily indicate the presence
1201
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 62, No 6, DECEMBER 1980
of a major coronary stenosis. Conversely, the absenceof coronary calcification did not indicate a normalcoronary artery.
Clinical Follow-up
Investigators have noted that up to 46% ofasymptomatic persons with documented abnormalexercise stress tests develop coronary events over a5-year follow-up period. The risk ratio among asymp-tomatic abnormal stress test responders for develop-ing clinical manifestation of coronary artery diseasehave ranged from eight to 14 times that of normalresponders.24 27 However, while epidemiologicstudies24-27 showed a high risk ratio for a populationwith an abnormal exercise stress test, the actualnumber of asymptomatic persons who go on tomanifest a coronary event is extremely low. Thus, alow predictive value limits the usefulness of exercisetesting for asymptomatic subjects.Hudson and Walker,28 who reported epidemiologic
data relating to coronary artery calcifications and sur-vival, failed to demonstrate a significant difference insurvival between patients with coronary calcificationand those without; but this study did have majordeficits (population age - 85% were older than 60years; failure to identify cause of death; and relatingmortality to coronary results).To our knowledge, no comparable studies in an
asymptomatic population have been made. Definiteand probable angina pectoris occurred in five of the 13subjects with coronary calcification and abnormal ex-ercise tests over the 36 months follow-up period.Furthermore, one of these 13 had a myocardial infarc-tion during follow-up. Therefore, the calculated in-cidence of future coronary events over 36 months inthis population with coronary calcifications and ab-normal exercise test is 45%, which is higher than ex-pected from previous epidemiologic studies.24-27 Thus,the results from this small population sample suggestthat the addition of cardiac fluoroscopy to sub-maximal exercise stress test could improve the lowpredictive value of exercise testing alone in largerepidemiologic and clinical studies.A criticism to our follow-up data is obvious. Angina
pectoris is a very subjective endpoint. Furthermore,our methodologic study design required a more fre-quent follow-up interview for subjects who had bothtests positive than for the rest. Thus, the search forangina may have been subconsciously more diligent inthis group, and a bias could have been introduced inthis study.
Clinical Implications
Coronary artery calcification on fluoroscopy andcoronary artery stenoses on angiography are not syn-onymous; postmortem and clinical studies in symp-tomatic and asymptomatic populations havedemonstrated the clinical relevance of coronary arterycalcification. The present study indicates (1) that thepredictive accuracy of coronary artery calcificationsand an abnormal exercise stress test in the middle-
aged, nonhyperlipidemic asymptomatic male is veryhigh (100% for some degree of coronary narrowingand 92% for clinically significant coronary stenoses);and (2) that coronary artery calcification and an ab-normal exercise stress test predict an early appearanceof clinical manifestations of coronary artery disease inpreviously asymptomatic men. However, the exerciseelectrocardiographic criteria we used were verystringent, and they should be carefully noted in apply-ing these observations to other tested populations.
References
1.Epstein F: Detection of individual susceptibility toward coro-nary disease. Prog Cardiovasc Disease 13: 324, 1971
2. Friedberg CK: The early diagnosis of coronary artery disease.Critical review. Adv Cardiol 8: 1, 1973
3. Moore CB: The early detection of coronary artery disease. JLouisiana State Med Soc 123: 57, 1971
4. Bruce RA, McDonough JR: Stress testing in screening for car-diovascular disease. Bull NY Acad Med 54: 1288, 1969
5. Kannell WB, Castelli WP, McNamara PW: The coronaryprofile: twelve-year follow-up in the Framingham study. J Oc-cup Med 9: 611, 1967
6. Froelicher VF, Thompson AJ, Longo MR Jr, Triebwasser JH,Lancaster MC: Value of exercise testing for screening asymp-tomatic men for latent coronary artery disease. Prog Car-diovasc Disease 16: 265, 1976
7. Redwood DR, Borer JS, Epstein SE: Whither the ST segmentduring exercise. Circulation 54: 703, 1976
8. Borer JS, Brensike JF, Redwood DR, Itscoritz SB, PassamaniER, Stone NJ, Richardson JM, Levy RI, Epstein SE:Limitations of the electrocardiographic response to exercise inpredicting coronary artery disease. N Engl J Med 293: 367,1975
9. Froelicher VF, Thompson AJ, Wolthuis R, Fuchs R, BalusekR, Longo MR, Triebwasser JH, Lancaster MC: Angiographicfindings in asymptomatic aircrewmen with electrocardiographicabnormalities. Am J Cardiol 39: 32, 1977
10. Bartel AG, Chem JT, Peter RH, Behar VS, Kong Y, LesterRG: The significance of coronary calcification detected byfluoroscopy. Circulation 49: 1247, 1974
11. Hamby RI, Tabrah F, Wisoff BG, Hartstein ML: Coronaryartery calcification: clinical implications and angiographic cor-relates. Am Heart J 87: 565, 1974
12. Oliver MF, Samuel E, Morley P, Young GB, Kapur PL: Detec-tion of coronary artery calcification during life. Lancet 1: 891,1964
13. New York Heart Association Criteria Committee:Nomenclature and Criteria for Diagnosis of Disease of theHeart and Great Vessels, 7th ed. Boston, Little, Brown and Co,1973, pp 95-124
14. Kelley MJ, Huang EK, Langou RA: Correlation offluoroscopically detected coronary artery calcification with ex-ercise stress testing in asymptomatic men. Radiology 129: 1,1978
15. Langou RA, Cohen LS: Cardiovascular exercise physiologyand stress testing. Conn Med 40: 522, 1976
16. Colton T: Statistics in Medicine. Boston, Little, Brown and Co,1974
17. Aldrich RF, Brensike JF, Batteglini JW, Richardson JM, Loh1K, Stone NJ, Passamani ER, Ackerstein H, Seuinger R, BorerJS, Levy RI, Epstein SE: Coronary calcifications in the detec-tion of coronary artery disease and comparison with electrocar-diographic exercise testing. Circulation 59: 1113, 1979
18. Mason RE, Likar I, Biern RO, Ross RS: Multiple-lead exerciseelectrocardiography: experience in 107 normal subjects and 67patients with angina pectoris, and comparison with coronarycinearteriography in 84 patients. Circulation 36: 517, 1967
19. Kattus AA: Exercise electrocardiography: recognition of theischemic response, false-positive and false-negative patterns. InExercise in Cardiovascular Health and Disease, edited by
1202 CIRCULATION
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

CAD DETECTION IN ASYMPTOMATIC MEN/Langou et al.
Amsterdam EA, Wilmore JH, DeMaria AN. New York, YorkMedical Books, 1977, pp 161-178
20. Weiner DA, Ryan TJ, McCabe CM, Kennedy JW, Schloss M,Tristani F, Chaitman BR, Fisher LD: Exercise stress testing:correlations among history of angina, ST segment response andprevalence of coronary artery disease in the Coronary ArterySurgery Study (CASS). N Engl J Med 301: 230, 1979
21. Froelicher VF, Yanowitz FG, Thompson AJ, Lancaster MC:The correlation of coronary angiography and the electrocar-diographic response to maximal treadmill testing in 76 asymp-tomatic men. Circulation 48: 597, 1973
22. Borer JS, Brensike JF, Redwood DR, Itscoitz SB, PassamaniER, Stone NJ, Richardson JM, Levy RI, Epstein SE:Limitations on the electrocardiographic response to exercise inpredicting coronary artery disease. N Engl J Med 293: 367,1975
23. Ripkin RD, Parisi AF, Folland E: Coronary calcification inthe diagnosis of coronary artery disease. Am J Cardiol
44: 141, 197924. Aronow WS, Cassidy J: Five year follow-up of double Master's
test maximal treadmill stress test, and resting and post exerciseapexcardiogram in asymptomatic persons. Circulation 52: 616,1975
25. Froelicher VF, Thomas MM, Pillow C, Lancaster MC:Epidemiologic study of asymptomatic men screened by max-
imal treadmill testing for latent coronary artery disease. Am JCardiol 34: 770, 1974
26. Kattus AA, Jorgensen CR, Worden RE, Alvaro AB: ST seg-
ment depression with near-maximal exercise in detection ofpreclinical coronary heart disease. Circulation 44: 585, 1971
27. Cumming GR, Samm J, Borysyk L, Kich L: Electrocar-diographic changes during exercise in asymptomatic men:
three-year follow-up Can Med Assoc J 112: 578, 197528. Hudson WM, Walker JK: The prognostic significance of cor-
onary artery calcification seen on fluoroscopy. Clin Radiol 27:545, 1976
1203
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from

R A Langou, E K Huang, M J Kelley and L S Cohencoronary artery disease in asymptomatic men.
Predictive accuracy of coronary artery calcification and abnormal exercise test for
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1980 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.62.6.1196
1980;62:1196-1203Circulation.
http://circ.ahajournals.org/content/62/6/1196the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 10, 2018
http://circ.ahajournals.org/D
ownloaded from