ehstg assessment handbook
TRANSCRIPT

FEDERAL DEMOCRATIC REPUBLIC OF ETHIOPIA
MINISTRY OF HEALTH
ETHIOPIAN HOSPITAL MANAGEMENT INITIATIVE
ETHIOPIAN HOSPITAL
TRANSFORMATION GUIDELINES
Assessment Handbook, September 2016

Federal Democratic Republic of Ethiopia
Ministry of Health
ETHIOPIAN HOSPITAL
TRANSFORMATION GUIDELINES
Assessment Handbook
Ethiopian Hospital Management Initiative
Version 1.0

Assessment Tool for Operational Standards of the EHTG
CHAPTER 1 HOSPITAL LEADERSHIP, MANAGEMENT AND GOVERNANCE
# Standard Method of evaluation Met Unmet
1. The hospital has a functional governing board that meets
regularly to oversee the service delivery of the hospital.
The board is established in accordance with a relevant
legislation
Meets in accordance with a relevant legislation (every quarter)
Minutes are taken at each meeting and agendas are relevant
2. The hospital has a functional SMT that meets regularly
to manage and execute the overall hospital activities.
Obtain a copy of the hospital’s organogram and check it with
the membership SMT
SMT Meets every week
Check whether minutes are taken at each meeting and agendas
are relevant
ToR is prepared and signed by all members
Standing committees are established (quality committee…)
There is an annual plan cascaded to each unit using the
balanced score card(BSC) framework
The SMT submits regular report to the board and relevant
bodies.
3. Hospital has a well-functioning hospital development
army.
There is a functional health development army established as
per the guideline
Regular hospital-community forums conducted every quarter.
Regular hospital management-staff forums conducted every
month.
Citizen charter is prepared and communicated well to the
clients and community
Verify if timely feedbacks are given for issues raised in the
various meeting sessions

4. The hospital governing board mobilizes resources from
diverse sources and makes sure resources are utilized
effectively and efficiently.
Annual budget of the hospital is approved by the board
Check if there is a plan to mobilize additional resources for the
hospital
Check resources are mobilized based on the plan
Internal and external audit reports are reviewed by the board
and findings and recommendations are attended.
5. There is a system and practice of measuring performance
and results in the hospital.
View the BSC documents and performance expectations/plans
are submitted by each units/ departments and are approved by
SMT
The performance of each units/departments are reviewed and
feedback is provided every month
A system of recognition is established for each
units/departments and health workers who meet established
standards.
Decisions are made based on performance data for quality
improvement
6. The hospital has good ethical practice promotion, ethics
violation reporting and responding mechanism.
The hospital has established a complaints handling system
Verify that the hospital assigns a unit to timely collect, properly
document, and submit reports of violation and takes proper
actions.
Suggestion boxes and logbooks are in place at each services
area, and suggestions are reviewed, analyzed and discussed on
SMT meeting every month.
A functional medical ethical committee is established

CHAPTER 2 LIASON, REFERRAL AND SOCIAL SERVICES
# Standard Method of Evaluation Met Unmet
1. The Hospital has established management structures
and job descriptions which detail roles and
responsibilities for:
Reception service
Liaison and referral service
Social service
Check if the hospital has reception service near at the gate of
the hospital with adequately trained staff, stretcher and
wheelchair
The hospital has established liaison unit
adequate number of social workers are assigned
2. The hospital should provide liaison services 24 hours
in a day and 7 days a week throughout the year.
Interview the head of the unit.
3. The hospital has a written protocol for the admission
and discharge of patients that is known, and adhered to,
by all relevant staff.
Check for hospital specific admission and discharge protocol
Interview staff for their knowledge and adherence
7. The hospital has a regular capacity building program for
governing board members and senior management.
Check if there is both a formal and ongoing orientation
program for the governing body on their role, responsibilities,
and accountabilities, organizational structure, regulations and
directives, guideline, policies, procedures and hospitals’
operation.
New members receive a thorough orientation before attending
their first governing body meeting.
Obtain a minute of a meeting held on self-
assessment.(conducted every six month)
8. The CEO is evaluated every six months, consistent with
FMOH or Regional Legislation to ensure he/she is
meeting operational and strategic plans as established by
the Board and the CEO collectively.
Check whether the CEO is evaluated by the board by obtaining
a copy of performance appraisal
Check whether the appraisal result is submitted to MOH or
their respective RHB/Zonal health office.
TOTAL _____
_
______
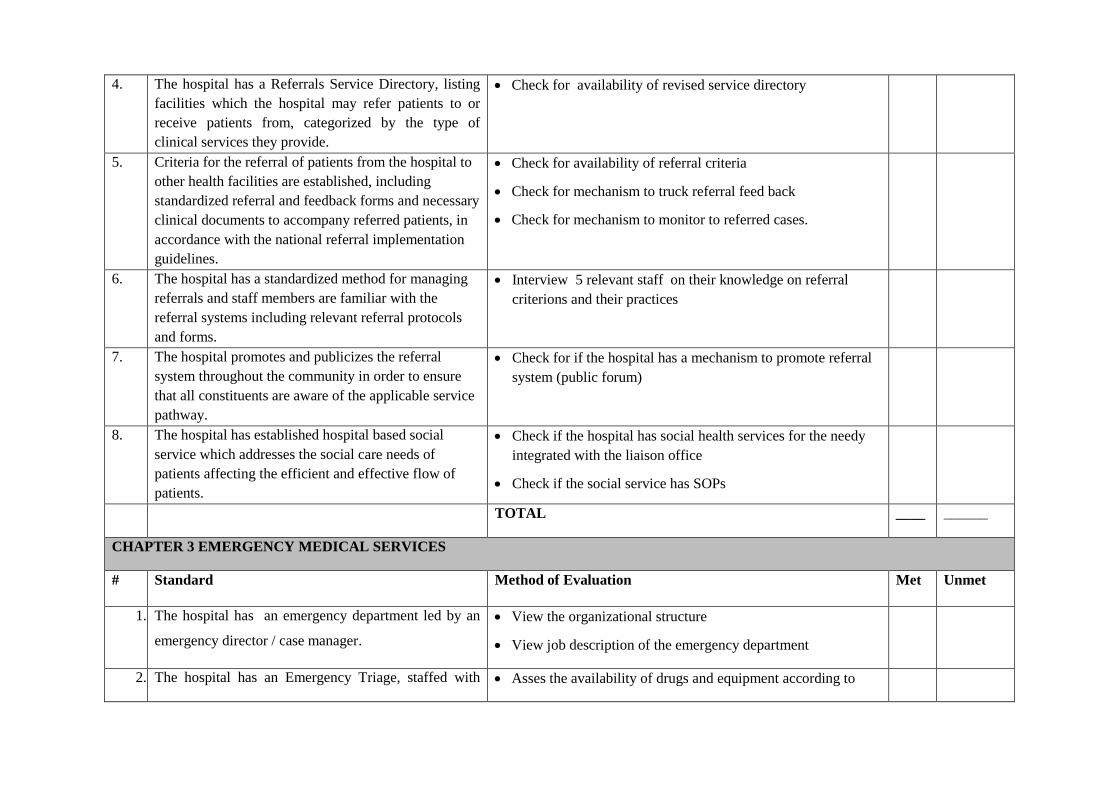
4. The hospital has a Referrals Service Directory, listing
facilities which the hospital may refer patients to or
receive patients from, categorized by the type of
clinical services they provide.
Check for availability of revised service directory
5. Criteria for the referral of patients from the hospital to
other health facilities are established, including
standardized referral and feedback forms and necessary
clinical documents to accompany referred patients, in
accordance with the national referral implementation
guidelines.
Check for availability of referral criteria
Check for mechanism to truck referral feed back
Check for mechanism to monitor to referred cases.
6. The hospital has a standardized method for managing
referrals and staff members are familiar with the
referral systems including relevant referral protocols
and forms.
Interview 5 relevant staff on their knowledge on referral
criterions and their practices
7. The hospital promotes and publicizes the referral
system throughout the community in order to ensure
that all constituents are aware of the applicable service
pathway.
Check for if the hospital has a mechanism to promote referral
system (public forum)
8. The hospital has established hospital based social
service which addresses the social care needs of
patients affecting the efficient and effective flow of
patients.
Check if the hospital has social health services for the needy
integrated with the liaison office
Check if the social service has SOPs
TOTAL ____ ______
CHAPTER 3 EMERGENCY MEDICAL SERVICES
# Standard Method of Evaluation Met Unmet
1. The hospital has an emergency department led by an
emergency director / case manager.
View the organizational structure
View job description of the emergency department
2. The hospital has an Emergency Triage, staffed with Asses the availability of drugs and equipment according to

necessary infrastructure, appropriately trained
personnel and equipped with necessary equipment,
drugs and supplies needed to provide quality
emergency medical services.
emergency medical services management chapter
Interview the head of the department about adequacy of staff
Check whether the staffs are trained to conduct emergency
patient triage and emergency care.
3. The hospital has easily accessible Emergency
department with an ambulance parking area.
Check whether the ER unit is labeled properly and visible
from the distance
Confirm that the emergency unit is located near to the gate
View the ambulance parking area and confirm that it is
appropriate for parking
4. The hospital shall establish efficient flow of Patients in
the emergency department.
Confirm that the emergency unity is organized based on the
following areas;
o Patient assistant area at Emergency gate
o Triage area
o Waiting area for non-critical emergency patients
o Examination area
o Isolation room
o Resuscitation area
o Procedure area
o The observation and treatment area(beds for 24hrs)
o Emergency OR or easy access to main OR
5. The Emergency Department or Unit shall use a triage
system of screening and classifying patients to
determine their priority needs and to ration patient care
efficiently.
Observe the triage area
Interview ER staff on how to triage patients
6. The hospital provides emergency medical service 24 View presence of emergency

hours a day and 365 days a year with a 24-hours’
access to diagnostic laboratory, radiology and
pharmacy services.
o Pharmacy
o Laboratory
o Mobile x-ray and ultrasound or 24hrs access
7. There is emergency response plan for both internal and
external disasters with a system to alarm or
communicate personnel and other stake holders.
View emergency response plan
Check the assignment of emergency response coordinator and
ask his duty in case of disaster
8. Emergency department or Unit has policies, protocols,
flowcharts, consultation and treatment guidelines for
running ED/EU.
View presence of policies, protocols, flowcharts, consultation
and treatment guidelines
TOTAL ____ ______
CHAPTER 4 OUTPATIENT SERVICES
# Standard Method of Evaluation Met Unmet
1. The Hospital has established management structures
and job descriptions that detail the roles and
responsibilities of each discipline within
services/departments/units, including reporting
relationships.
Check organogram of the hospital
Assigned director/case team manager with JD
Plan/monthly, quarterly and annual
Report/monthly, quarterly and annual
Quality improvement plan
2. The hospital has well-equipped service specific OPD
rooms with necessary equipment and supplies as per
hospital tier level of care.
Check availability of necessary equipment and supplies
3. The hospital has established outpatient specific
diagnostic laboratory, radiology, and pharmacy service
units.
Functional Outpatient lab
Functional outpatient pharmacy
Functional radiology
Sample collection unit

4. The hospital has an outpatient department waiting area
with adequate lightening, ventilation and multimedia
facilities.
Check availability of adequate waiting area in comparison
with volume of patient
Waiting area is ventilated and lightened
Multimedia service is available (like TV, Radio etc)
Chairs are comfortable
5. The hospital has an OPD staffed with adequate and
appropriately trained personnel and OPD service rooms
are managed by at least a GP and specialty clinics by a
service specific specialist/ sub- specialty clinic by sub
specialist as per hospital tier level of care.
Check clinics arranged as per specialty
Check specialty clinics are run by specialist
Check referred patients seen by next level
professional(General practitioner -Specialist-Sub Specialist
6. Outpatient department (OPD) specific central triage
procedure is established to ensure efficient patient
flow; and seek to reduce patient crowding.
Protocol for managing queue
Registration for appointment
Observation MR, Pharmacy and Examination
7. The hospital has established OPD patient appointment
and queuing management systems.
Composition and number of staff
Patient to physician ratio
Equipment’s and supplies
TOTAL ____ ______
CHAPTER 5. INPATIENT SERVICE MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The Hospital has established management structures
and job descriptions that detail the roles and
responsibilities of each discipline within
services/departments/units, including reporting
relationships
Check organogram of the hospital
Assigned director/case team manager with JD
Plan/monthly, quarterly and annual
Report/monthly, quarterly and annual
Quality improvement plan

2. IPD specific admission and discharge procedures are
established to reduce the unnecessary inpatient length
of stay.
Take 10 patient chart and check Discharge and care plan for
each patient
IPD Admission and Discharge Protocol
Hospital access/security for all IPD
Appointment systems for IPD
3. All admitted patients have medical and
nursing/midwifery care plans that describes medical
and nursing/midwifery interventions to address their
needs. The plans are regularly reviewed and updated as
required.
Randomly take 10 charts to check presence complete and
revised history sheet, progress note, discharge summery and
death summery
4. The hospital implements a minimum of daily
multidisciplinary team patient rounds and visit
services.
Check round schedule
Observe round program on the day of visit
Check round team composition
5. The Hospital has IPD service specific facilities as per
hospital tier level.
Mental health
ICU service
Surgical service
6. The hospital has IPD staffed with adequate and
appropriately trained personnel and equipped with
necessary equipment and supplies for Inpatient as per
tier level of care
Composition and number of staff
Patient to physician ratio
Equipment’s and supplies
7. The Hospital has established guidelines for verbal and
written communication about patient care, including
verbal orders and patient handover by discipline and
between disciplines
Communication guideline
Interview 10 staffs about the communication ways between
staffs and coordinators
Shift hand over protocol
8. The Hospital has established procedure for and inter-
professional and departmental consultation and transfer
of patients’ care to ensure continuity of care.
Consultation protocol
9. The Hospital has a policy for accompanying all
patients by appropriately trained health provider/s
during out of IPD diagnostic services and transfer
between wards/departments.
Observe patient transportation
Patient transportation protocol
Interview 10 admitted patients about their experience

TOTAL ____ ______
CHAPTER 6. MEDICAL RECORDS MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. Unique medical record number is assigned to a patient
during his/her first visit of care.
Verify that unique medical record numbers are given to all
patients.
2. The hospital shall have a single unified medical
registration unit for all patients’ registration.
Interview Head of Medical Records Department (or
equivalent) and confirm that only one registration system
exists for ALL patients, including inpatients, outpatients,
emergency patients, and specialty clinic patients.
3. The hospital utilizes paper and computer-based
systems to register and retrieve medical records.
Identify the Master Patient Index
View MR tracking system.
4. The hospital avails and utilizes a standard set of
formats that comprise a complete medical record for
continuum of patient’s care.
Randomly sample 10 inpatient medical records of patients
admitted in the past year, and confirm that each, as a
minimum, contains: physician admission assessment,
progress notes, nursing care plan, discharge summary
5. The hospital shall implement and comply with national
guidelines to manage access to patient’s medical
records.
Interview medical records staff and confirm national
guidelines on handling and confidentiality of medical records
are known by all staff.
6. The hospital performs medical record auditing, data
quality checks, archiving/culling procedures and takes
corrective actions on a regular basis.
View audit reports
Randomly select 10 medical records and check for proper
completion of the forms (at least look for date, utilization of
standard formats, discharge summary for discharged patients,
and name and signature of the physician.
View proper shelving of medical records
View store for keeping medical records that are not active for
more than 5 years
7. The hospital ensures patient’s medical records return
from different service units to medical records unit at
Check the use of tracer card to identify the location of

the end of each service day in accordance with medical
record tracing system.
medical records at all times
View the mechanism of getting all medical records back at
the end of each service day
8. The hospital shall automate health information system
through implementation of integrated electronic
medical record system.
View and confirm implementation of electronic medical
record systems
TOTAL ____ _____
CHAPTER 7. NURSING AND MIDWIFERY CARE SERVICES MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital has established nursing/midwifery service
management structures and job descriptions that detail
the roles and responsibilities of each nursing and
midwifery professional, including reporting
relationships.
Check for nursing representation in the SMT;
Does a system exist to supervise nursing activities?
Has the hospital established management structures that detail
the roles and responsibilities of nursing/midwifery
professionals, including reporting and communication
relationships?
Does the hospital have a nursing/midwifery workforce plan that
addresses nurse/midwifery staffing requirements according to
the standard set for hospitals?
Do the hospitals provide written policies describing the
responsibilities of nurses/midwives on prevention, promotion,
rehabilitative and curative care as well as nursing and
midwifery care process?
Is there a prepared budget and operational yearly plan r
regarding nursing and midwifery practice and has it been
submitted to the SMT?
2. The hospital has a nursing and midwifery workforce
plan that addresses nurse /midwife staffing
requirements and sets minimum nurse /midwife to
Obtain copy of nursing staffing plan and confirm this
establishes nurse to patient ratios for each service area (e.g.
inpatient wards, ER, surgical suite, labour and delivery).

patient ratios in each service area. Confirm the plan identifies mechanisms to reassign nursing
staff or call in extra staff to ensure that minimum nurse to
patient ratios are maintained at all times
3. The hospital has written policies describing the
responsibilities of nurses and midwives for the
nursing/midwifery process including the admission
assessment, planning, implementation and evaluation
of nursing/midwifery care.
Identify written policies that describe the nursing process.
Verify that the following are addressed:
o Nursing admission assessment
o Nursing care planning, implementation and
evaluation
4. All admitted and emergency patients/clients have a
nursing/midwifery care plan that describes holistic
nursing/midwifery interventions to address their needs.
The plan is regularly reviewed and updated as required.
Select a random sample of 10 inpatient records from different
wards. Confirm that each contains a nursing care plan.
5. All hospital nurses/midwives comply with the
professional code of conduct and ethics which governs
their professional practice.
Does the hospital provide a written professional code of conduct
and ethics to all nurses and midwives?
Does the hospital provide complete uniforms for
nurses/midwives and do nurses/midwives comply with the
institutions dress code and all nurses are wearing the specific
uniform?
Are nurses /midwives in complete uniform at all times?
Does the hospital have a system to report illegal, incompetent or
impaired practice?
6. The hospital has established guidelines for verbal and
written communication about patient/client care that
involves nurses/midwives and their patients/clients,
families, other case team professionals of the disciples,
including verbal orders and timely documentation of
accomplished activities.
Does the hospital provide written guidelines regarding verbal
and written communication and documentation?
Do nurses and midwives attend nursing rounds on a regular
basis?
Do nurses and midwives provide safe, effective, efficient, and
patient-centered care to patient/clients?
Do nurses/midwives engage in self-evaluation on a regular

basis?
Do nurses and midwives seek constructive feedback regarding
their own practice?
Does the hospital have a systematic peer review? Regularly,
supervise, mentor and coach the senior nurse to support the
junior nurses?
Do the nurses/midwives have perform one hour rounds?
7. The hospital has standardized procedures for the safe
and proper administration of medications by nurses or
designated clinical staff.
Identify written procedures for process of medication of
administration.
Verify that procedure addresses safety, proper administration,
and administration authority.
Review 10 Medication Administration Records from different
wards and confirm that each is completed correctly with the
signature of the transcriber and of the individual who
administered each medicine dose.
8. The hospital has established nursing/midwifery care
practice audit programme, including the documentation
of completed audits and resulting practice
improvements.
Does the Hospital have a Nursing/midwifery Audit
Committee?
Does the Nursing/midwifery Audit Committee meet regularly
and conduct a nursing/midwifery service audit?
Do Nurses/midwives collect data to monitor the quality of
nursing/midwifery practice?
Do Nurses/midwives participate in critical review and/or
evaluation of policies, procedures, and guidelines to improve
the quality of healthcare?
Do Nurses/midwives collaborate with the inter-professional
team to implement quality improvement plans and
interventions?
Do Nurses/midwives analyze trends in healthcare quality

data?
Do Nurses/midwives incorporate evidence based best
practices to improve health outcomes?
Look for a nursing/midwifery audit report
Look for action plans that address gaps identified by audits
Observe implementation of the action plans
9. The hospital implements regular nursing/midwifery
eight hours’ shift, hourly rounds, and central
medication cabinet or room.
Is the hospital implementing 8 hours shift of nurses/midwifes?
Do the nursing/ midwife staffs conduct hourly patient rounds?
Does the hospital implements central medication management
system to ensure medications are not placed at patient side?
10. The hospital has a centralized nursing/midwifery
station set-up in each ward with adequate space,
equipment and consumables.
Does each unit have the necessary equipment and supplies to
accomplish nursing and midwifery care practice?
Does the unit have equipment for specific minor procedures?
Does the nurse/midwife assess equipment necessary to
accomplish the nursing and midwifery practice related to safety,
effectiveness and availability?
TOTAL ____ ______
CHAPTER 8. MATERNAL, NEONATAL AND CHILD HEALTH SERVICES MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital ANC unit provides individualized, client
centered and evidence based care to clients on all
working days and high risk mothers should be seen in
the referral clinic.
The ANC clinic provides service for pregnant women 8
working hours in a day:
All care providers in ANC clinic are trained on focused
ANC:
ANC services in ANC clinic keep visual and auditory

privacy of Pregnant women:
All ANC service are being provided free of charge:
Investigation results should be given on the same day by
prioritizing pregnant mothers in the laboratory:
Invitation letter for Partners are given with counseling to all
ANC clients to improve partner involvement:
Ensuring the women holds her own medical record summary
at 36 weeks:
Mother infant follow up at ANC clinic until 18 months of
discharge:
There has to be a referral clinic for high risk mother and the
clinic should be run by OBGYN specialist or IESO, open
twice per week and 75% of referred ANC mothers should be
seen by referral clinic for consultation :
2. The hospital should ensure provision of
Comprehensive Emergency Maternal and Newborn
Care (CEmONC) services
Ensure all 10 signal functions are available (see annex) :
Safe surgery check list is used always at least for 75% :
Spinal anesthesia rate should be monitored and should be
more than 75%:
Audit to assess completeness of documentation should be
done every three month: (see MNCH QoC audit assessment
tool):
The rate and indications for C/S should be displayed in white
board every month:
No administrative barrier:
3. The hospital should ensure women and child friendly
services at all MNCH units including pain
management.
Rooms should be well ventilated and temperature of the
room should be good (nether hot nor cold):
There should be screens or curtain to maintain privacy and
has sufficient space to walk around:
The rooms should have a working bath room and toilet with
door that is accessible to laboring mothers that has a hand
washing basin with soap and water for both labour and post-

natal ward:
Family member/support person is allowed to remain with
woman constantly during labour and birth:
Mother is offered oral fluids and light food during labour and
allowed to deliver in their preferred position:
Pain management:
4. The hospital ensures all equipment, essential drugs,
supplies and reference materials are available in
maternity and pediatric units
See MNCH QI assessment tool or annex 1, 2, 4, 5, 6, 7, 8, &
9 on MNCH service chapter on EHSTG.
5. The hospital should ensure the provision of intra-partal
care as per national protocols
Identification and previous obstetric history are properly
documented:
Date and time of admission finding properly recorded:
Basic and essential Laboratory investigation Hgb, blood
group and Rh and HIV test is done routinely during
Intrapartum care:
FHB is monitored at least every 30 minutes and recorded in
the Partograph and chart:
Cervical dilation assessed every 4hrs and documented:
Maternal Blood Pressure measured at least every 2-4 hours
and pulse rate every half hour:
Delivery summary is properly documented:
Safe child birth checklist used consistently:
Oxytocin 10 IU IM given just after delivery of the
baby(AMSTL):
Neonate is given vitamin K 1 mg, TTC eye ointment and
vaccinated with BCG and OPV 0:
6. The hospital should provide comprehensive postnatal
care in the facility as per national standards
Mothers have checked for vaginal bleeding, uterine
contraction, fundal height, temperature and heart rate
routinely immediately after birth every 15min for the first
2hours, if normal hourly during her stay in the hospital:.
Neonates checked for breathing problems, color; pulse rate,

fever, breast feeding and cord tie security:
Mother should be counseled for danger signs for both mother
and neonate and should be documented.
The hospital should ensure provision of family planning
(with focus on long term:
7. The hospital should ensure provision of family
planning (with focus on long term methods) and
comprehensive abortion care services following the
national guideline and policies.
Trained health professional were assigned to provide
counseling on contraception, unintended pregnancy and
abortion;
demonstrate competent skills and the services should be
evidence based:
Comprehensive health and obstetric, gynecologic and
reproductive health history taken and physical examination
done:
Care, support and referral or treatment for the HIV positive
woman and HIV counselling and testing for women who do
not know their status provided:
Prescribe, dispense, furnish or administer a broad range of
contraceptive methods, including IUDs, implants, injectable
emergency contraceptives and women advised about
management of side effects and problems with use of family
planning methods:
Perform vacuum aspiration (manual or electric) for
pregnancies of gestational age up to 12–14 weeks according
to the national guideline.
Medical methods of abortion available for pregnancies of
gestational age up to 9 weeks, or up to 12 weeks if the
woman can stay in the facility until the abortion is complete
according to the national guideline;
Clinical stabilization, provision of antibiotics, and uterine
evacuation provided for women with complications of
abortion;

Referral women who needing unavailable services in the
hospital or HCs.
8. Maternity and pediatric units should undertake CQI
activities by conducting regular review meetings and
audit programmes.
Maternity and pediatric unit should perform audit every
month
Maternity unit should perform MDSR
Client/mom’s satisfaction survey should perform every 3
months
Data should be displayed on White board at ANC, Labour
and delivery and postnatal ward and updated
Community involvement ( Pregnant mother forum,
community forum) at least one activity in 3 months
Regular review meetings (at least every week) to discuss
audit findings
The pediatric department should conduct regular QoC audits
in respective units as to the proper checklist.
Pediatric unit should perform death audit.
9. Hospitals have established separate pediatric OPD,
emergency and triage services.
Observe that the pediatric OPD is separate from adult OPD
Observe that the hospital has established separate pediatric
triage and adjacent emergency treatment area (room) within
pediatric OPD
Check by observation that children are sent directly to the
pediatric triage area upon arrival in the hospital (before
registration)
Confirm that professionals assigned at pediatric triage and
emergency unit are trained in ETAT
Check that emergency box containing all emergency drugs
and equipment is available in the pediatric ER
Check that ETAT guidelines and job aides are available in
the triage area and ER (see Annex 3)
Verify that the equipment and drugs listed in Annex 1 are
available and functional

10. Hospitals have comprehensive Neonatal Care service
that includes NICU, KMC, mother’s room and
isolation rooms.
Check the hospital has established neonatal unit
Confirm the neonatal unit is composed of:
- Neonatal ICU
- Kangaroo mother care (KMC) room
- Mothers’ waiting room
- Isolation room for neonates with communicable
infections
- Procedure/resuscitation room
Confirm that all the equipment, supplies and essential drugs
listed in annex2 are available and functional
Check that infants admitted to the neonatal unit are managed
by a neonatologist (if available),a pediatrician or a
professional with special training on neonatal care (NICU
care)
Check that guidelines and jobs aids listed in Annex 3 are
available for neonatal unit
Confirm that LBW infants (<2000 gr) that are clinically
stable are given KMC starting soon after birth
Confirm from mothers’ and infant charts that prophylactic
antibiotics are given for neonates with documented risk
factors (ROM >18 hr, maternal fever, foul smelling amniotic
fluid)
Check that thermal environment is maintained for the sick
infants:
Young infant is kept dry and well wrapped
Room is kept warm (at least 25oC)
Attention is given to avoid chilling the infant during
examination or investigation
Infants’ temperature is regularly checked to maintain b/n 36-
37oC axillary (36.5-37.5oC core)
11. Hospitals have separate Pediatric Wards composed of
separate critical, general, SAM, isolation and
Check that the hospital has pediatric ward separate from adult
ward

procedure rooms. Check that the pediatric ward is composed of the following
rooms:
- Therapeutic feeding room for children with
complicated SAM
- Pediatric ICU or at least dedicated room for critically
ill children next to the nursing station
- Isolation room for children with communicable
diseases
- Clean, ventilated procedure room with good light
source
Observe that the ward room paintings are child friendly
Confirm the presence of national guidelines and job aids
listed in Annex 3, and supplies and equipment listed in
Annex 6 are available and functional
From patient charts, check the following:
- Children admitted to the wards are evaluated by
physicians (preferably pediatricians) on daily basis (
twice per day for critical children)
- Critically sick children are evaluated by registered
clinical nurses every 4 hours
- Vital signs are measured every 6 hrs for admitted
children (more frequently if ordered by a physician)
- Growth monitoring is performed for all U5 children
admitted to the ward
Admission and discharge notes, vital sign sheets, and
discharge or death summaries are attached to the patient
charts
12. Midwives should implement the midwifery process at
all hospitals for all admitted patients.
Midwives assess and record pertinent data using evidence
based assessment.
Midwives’ assessment data able to reach to proper diagnoses

Midwives ‘care plan is according to the assessment and
diagnosis
Midwives appropriately implemented and executed the care
plan
Midwives re-evaluate and re planed if necessary
Midwives record and document all data in the clients’ chart
TOTAL ____ ______
CHAPTER 9. LABORATORY SERVICES MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital has a clear laboratory management
structure and accountability arrangement with well-
defined roles and responsibilities for the provision of
laboratory services organized into central, emergency
and inpatient laboratory services.
View organization chart.
View central, emergency and inpatient laboratories
Interview senior staff member of Central Laboratory and
confirm that Central Lab has functional overview of all
laboratory services.
2. The hospital laboratory management has established
system for management of documents and records that
are maintained, controlled, reviewed and approved to
ensure the provision of quality laboratory services.
Obtain evidence whether the laboratory have document and
record generation, identification, approval, use, control and
disposal procedure
View the laboratory-produced quality manual, safety manual,
sample management guideline and laboratory handbooks
Confirm the availability of standard operating procedures
for all Technical and Managerial procedures in work place
Confirm the availability of Guidelines, Formats , Job aids
and instructions in work place
3. The hospital laboratory has established system to
monitor the effectiveness of its customer service
programme.
View laboratory handbook in all services areas.
View customer satisfaction survey report.
View presence of suggestion box to collect customers
suggestions
View posted available test menu with current price and
standard TAT to customers.

Refer list of tests and equipment’s in Appendix B
Confirm the laboratory staffs communicated the available
tests to their clients and advisory service given
Confirm the established Complaint monitoring system
Check Suggestion box and/or suggestion book in place
4. The hospital laboratory has and implements a proper
management system for its equipment that includes the
calibration, maintenance and inventory to ensure the
provision of accurate, reliable and timely test results.
Confirm if there is a proper and functional equipment
management system in place
Obtain evidence on equipment management system include
ways of participation on consultation, selection,
specification, installation, calibration, maintenance, retiring
and disposal
5. The hospital has a laboratory supplies management
system.
Ensure that an effective supply chain management system is
in place to select, quantify, transport, store, distribute and
keep records of all reagents and supplies.
Confirm the laboratory have functional inventory system for
resource management
View laboratory has mini store for lab supplies and reagents
View Bin cards are used to manage laboratory supplies and
reagents
View stock status report
6. The hospital laboratory shall implement a process
control system that monitors the processes from pre
analytical to post analytical phases of testing, including
an established internal quality control (IQC) and
participates in external quality assurance (EQA).
Pre-analytical
View well established and isolated sample collection area.
View sample collection manual ready for use in work place.
Analytical phase
Obtain records of valid IQC for all tests in regular manner
Confirm whether the laboratory participates in any
recognized EQA (PT scheme) or intra laboratory evaluation
and scored ≥80% for tests included in that scheme.
Post-Analytical
Confirm a system to review results before release
independent of testing personnel

View a TAT established for every test and evaluated
7. The hospital laboratory has established incident
handling and reporting system which includes errors or
near errors (also called near misses).
view records occurrences or incidence
View identified and registered occurrences or deviations
from standard assessed and put for improvement
8. The hospital has established laboratory management
information system.
View written procedure for the laboratory information
management system
Confirm the system prevents patient data loss or proves
confidentiality, accessibility, accuracy, timeliness, security,
and privacy of patient information.
9. The hospital laboratory should be designed and
organized at least for bio safety level 2 or above and
work environment is clean and well maintained at all
times.
View if The hospital laboratory have enough working space
Ensure a laboratory safety program is in place and
performed accordingly
make sure availability of safety equipments and supplies (
first aid kit, spill kit, fire extinguisher, and emergency
shower, eye wash, PPE etc)
Interview selected lab staff in order to check relevant safety
awareness among staff
Observe for restricted access when work is in progress
Work stations ,floor and walls are easily cleanable,
10. The laboratory shall design a backup laboratory service
through availing back laboratory equipment or and
through backup laboratory facility.
Confirm if a system designed for back-up laboratory service
View lists of backup laboratory facilities
View developed and signed MOU by all responsible bodies
View back-up equipment in case of equipment failure
11. The hospital laboratory has appropriate storage and
stock management systems for blood and blood
products received from blood banks.
View the mini blood bank
Obtain list of transfusion committee members and focal
person with their official letters
Obtain singed MoU b/n hospital and Blood Bank Services
Obtain equipment inventory list and check their functionality
status
View documents and records for blood received ,blood
issued and compatibility test and SOPs

12. The hospital laboratory blood bank service in
collaboration with respective regional blood back
service shall have mobilization of blood donation
strategy through community awareness programs.
Obtain number of awareness creation program in the year
View number of notification letters for awareness creation
session
View the list of potential blood donors in the hospital
identify notification letter written to blood bank service so as
to collect blood for VNBDS in hospital
13. The hospital laboratory blood bank service shall have
appropriate cold chain system for blood and blood
products received from blood bank service until used
by prescribers.
View SOP for cold chain system
Randomly check Temperature control chart
Check the following equipments
a. Blood bank refrigerator 2-6Oc
b. Blood bank deep freezer <-18oC
c. Platelet Agitator 20-24Oc
d. Bench top centrifuge
e. Blood group or Cross match plate
f. Blood group reagents (Anti-A,B and Anti-D
g. Anti-human globulin antisera
h. Biohazard bag
i. Blood warmer
j. Water bath
14. The hospital laboratory blood bank service shall report
blood administration and patient safety information to
respective regional blood banks.
Check blood request forms and see for completeness
Check whether the transfusion committee has a meeting
plans/schedule
Check minutes of blood transfusion committee meeting and
check status and approval
View blood transfusion committee TOR and check for
implementation
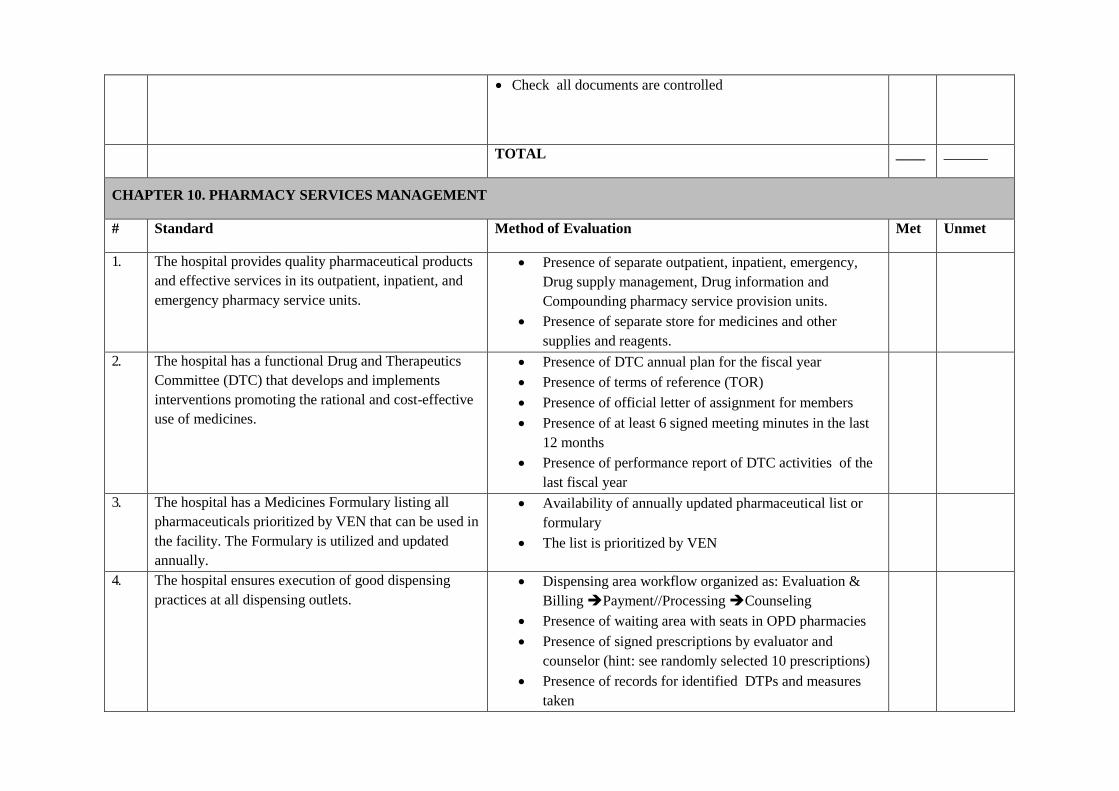
Check all documents are controlled
TOTAL ____ ______
CHAPTER 10. PHARMACY SERVICES MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital provides quality pharmaceutical products
and effective services in its outpatient, inpatient, and
emergency pharmacy service units.
Presence of separate outpatient, inpatient, emergency,
Drug supply management, Drug information and
Compounding pharmacy service provision units.
Presence of separate store for medicines and other
supplies and reagents.
2. The hospital has a functional Drug and Therapeutics
Committee (DTC) that develops and implements
interventions promoting the rational and cost-effective
use of medicines.
Presence of DTC annual plan for the fiscal year
Presence of terms of reference (TOR)
Presence of official letter of assignment for members
Presence of at least 6 signed meeting minutes in the last
12 months
Presence of performance report of DTC activities of the
last fiscal year
3. The hospital has a Medicines Formulary listing all
pharmaceuticals prioritized by VEN that can be used in
the facility. The Formulary is utilized and updated
annually.
Availability of annually updated pharmaceutical list or
formulary
The list is prioritized by VEN
4. The hospital ensures execution of good dispensing
practices at all dispensing outlets.
Dispensing area workflow organized as: Evaluation &
Billing Payment//Processing Counseling
Presence of waiting area with seats in OPD pharmacies
Presence of signed prescriptions by evaluator and
counselor (hint: see randomly selected 10 prescriptions)
Presence of records for identified DTPs and measures
taken

Presence of report on patient knowledge on correct
dosage and satisfaction
5. The hospital implements auditable, transparent and
accountable pharmaceutical transactions and services
(APTS).
Presence of properly recorded and filed prescriptions,
sales tickets and registers at dispensaries
Adequate human resource is deployed in each pharmacy
services units (hint: based on workload analysis: number
of prescriptions and bed size)
Pharmacy premises are arranged so as to keep patient
safety and privacy
Implementation of coding to uniquely identify medicines
Bin ownership is implemented
Presence of monthly reports for products, finance and
services
Presence of audit report (internal)
Wastage rate in monetary value is <2%
Presence of annual report on ABC and VEN analyses
6. The hospital provides clinical pharmacy services at
inpatient, outpatient and emergency departments.
Completed patient medication profile form,
pharmaceutical care progress recording form and
medication reconciliation forms are part of the patient
chart (hint: see randomly selected 10 patient charts at an
inpatient ward)
Ward pharmacy available in each major ward and
functions for 24 hrs.
Unit dose dispensing is implemented at ward pharmacies
(medicines are dispensed only for 24 hrs.)
Regular participation of pharmacists in ward rounds,
morning sessions and seminars (ask a physician and a
nurses in major wards)
7. The hospital provides drug information services to
health care providers, patients and the public.
Presence of properly filled query receiving and
answering forms (see the previous month records)
Presence of recently prepared sample drug
alert/newsletter, therapy update, drug monograph

Presence of updates on stock availability to the hospital
community (ask health care team or see records)
Presence of medicine use education for patients (ask the
appropriate unit)
Has started providing poison information
Presence of survey report on patient satisfaction of
overall pharmacy services
8. The hospital has a functional compounding service. Separate premises for compounding service
Availability of equipment, materials and chemicals
Availability of SOP for all compounding procedures
Recorded documents for all compounded items
9. The hospital has efficient and effective pharmaceutical
logistics management system that reduces the
frequency of stock-outs, wastage, over supply and drug
expiry.
Presence of procurement policy
Presence of annual pharmaceutical quantification and
supply plan
Report that shows percentage of procured items from the
hospital list.
Presence of updated bin card (check randomly selected
10 bin cards)
Good storage practice is being followed
10. The hospital has appropriate paper/computer-based
inventory management system.
Presence of properly recorded and filed Vouchers at store
Availability of paper based or electronic inventory
management tool
Presence of physical inventory report for dispensaries
for stores
Presence of stock status analysis report.
11. The hospital has an established system for regular
monitoring medication use and safety.
Presence of semi-annual prescription monitoring report
Presence of annual DUE Report
Presence of ADE report
Presence of WHO drug use indicator study report
Presence of update on (high alert medications,
error prone abbreviations, look-alike and sound alike

medication list …)
12. The hospital conducts continuous segregation,
documentation and safe disposal of pharmaceutical
wastes
Presence of SOP for disposal for the hospital
Presence of list of disposed products with description
Expired medicines are separately segregated
Presence of certificate for disposed medicines (minutes
during disposal)
TOTAL ____ ______

CHAPTER 11. RADIOLOGICAL AND IMAGING SERVICES MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital has a separate well designed and
equipped radiology unit and qualified personnel
that oversees radiological and imaging services.
Confirm that:
Radiology unit is established with service provided 24/7
The head is a member of SMT and hospital medical
equipment committee
The unit has strategic and annual plan with budgets
approved by SMT
2. The radiology unit has all the necessary layout and
infrastructure, personnel and equipments as per
FMHACA and ERPA standards.
Confirm if
Hospital received Yearly ERPA certification
Adequate number and mix of professionals (radiographer
technicians, radiographer technologists, radiologists etc are
maintained as per FMHACA and / or ERPA standards
Adequate utilities are ensured including 24 hour water and
electricity supply, toilets (gender separate), telephone line,
3. All radiological and imaging equipment users are
appropriately trained on the operation and
maintenance of such equipment with standard
operating procedures readily available to the
service providers.
Confirm if
SOPs are developed and in use for the regular operation and
maintenance of all equipments in the unit
All equipment users are appropriately trained on the
operation and maintenance of medical equipment with
standard operating procedures readily available to the user
Regular orientation and refreshment training is given for all
workers on how to operate the equipments
4. The hospital has established procedures for the
maintenance, calibration, capability, quality
control testing and functionality of all radiological
and imaging equipment.
Confirm if
All new equipment undergoes acceptance testing prior to its
initial use to ensure the equipment is in good operating
condition.
All new Equipment is installed and commissioned in
accordance with the manufacturer’s specifications

There is a schedule for inspection, testing and preventive
maintenance for each piece of equipment as guided by the
manufacturer’s recommendations and that schedule is
appropriately implemented
There is a notification and work order system for the repair
of medical equipment
5. The hospital has and implements written policies,
procedures, protocols and guidelines for the
delivery of all radiological services, interpretations
and timely reporting of results for all patients.
Confirm if SOPs are developed and implemented for the following
activities
Request reviewing
Client communication and consenting
Turnaround time
Patient preparation and positioning
Radiation Safety protocols
Contrast administration
Management of specific situations (pediatric patients,
pregnancy, clients needing sedation, emergency patients and
prioritization protocols)
Quality improvement activities (identification of quality
gaps, action plan development and implementation)
6. The hospital has a paper or computer based system
for recording and reporting of all radiological and
imaging procedures carried out and for archiving
all patients’ results that are periodically audited for
quality assurance, service improvement and
expansion.
Confirm if the hospitals has and implements
Reporting formats and standards
Policies and procedures for recording and reporting
(including remote reporting)
Communication policy with the unit and other clinical
departments
TOTAL ______ ______
CHAPTER 12. REHABILITATIVE AND PALLIATIVE CARE SERVICES MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital should have a rehabilitation and
palliative care service with necessary equipment,
There is a designated area in the hospital, including area for
rehabilitation and palliative care services

aids and appropriate human resources. Relevant equipment and resources has been procured
Trained rehabilitation, at least a physiotherapist and palliative
care professionals has been recruited and employed
Rehabilitation and palliative care treatment protocol are in place
Rehabilitation service has education programs in place for
patients receiving rehabilitation
2. With regard to rehabilitation, the hospital should
at least provide a physical therapy/physiotherapy
service and if possible, occupational, speech and
Prosthetics Osthotic Technology.
A physiotherapist is available in the hospital
A physiotherapy centre is equipped with the minimum
equipment required
3. With regard to palliative care services, the hospital
should at least provide good pain and symptom
control for both in and out patients.
Essential palliative care drugs mainly consisting of pain
management, are available in the hospital
Pain assessment is established as a fifth vital sign in the hospital.
4. The hospital should have a written standard
operational procedure and patient record
management for all rehabilitative and palliative
care services.
There is written guidelines and SOPs for the assessment,
implementation and evaluation of rehabilitation and palliative
care services
Patient health records identify the patient and document
rehabilitation assessment, goals, intervention and outcomes
5. The hospital should establish a mechanism for
referral and transfer of rehabilitation and palliative
care services through in-patient and outpatient and
in the case of palliative care, linkage to services
that provide home-based care.
Community partners are engaged for patient care in the home
Protocols related to information sharing communication and
confidentiality developed
TOTAL _____ ______
CHAPTER 13. INFECTION PREVENTION AND PATIENT SAFETY
# Standard Method of Evaluation Met Unmet
1. The hospital has strategies and operational plan for
IPPS as well as a management system to monitor
and evaluate the activities.
Interview CEO/medical director to confirm that CASH/IPPS
committee is in place and functional(check updated and printed
TOR of the committee,)
Check regular monthly minutes of the committee
Check the hospital has strategies/ policies
Does the committee have an operational plan on CASH and
IPPS

Check the activities planned are implemented based on the
schedule(check performance reports)
2. Hand hygiene practice is implemented and
facilities are provided at all service points at all
time
Check the presence of hand washing facilities(at minimum with
soap , water and functional faucets ) at all different service
outlets with access to clients and attendants
Check the hospital has continuous water supply at point of use
with backup.
Check hand washing posters are posted at a visible location
Randomly Spot check 5-10 staff from different service points
washing hands/interview about steps and critical hand washing
times.
3. All the necessary commodities and supplies of
IPPS are routinely available and utilized at the
designated service areas.
Check the availability and adequacy of necessary PPE’s at(
labor ward, OR, procedure rooms/minor OR, Laundry,
Housekeeping/waste handlers staff
utilization of PPEs at ( labor ward, OR, procedure rooms/minor
OR, Laundry, TB rooms, housekeeping and waste handling
spots
4. The hospital has ensured that safe surgical
procedures and practices are in place to minimize
risks to clients and providers
Check the usage of WHO surgery safe surgery checklist for 5-10
clients.
Check the presence of standard surgical antiseptics at all
procedure rooms.
Spot check /interview whether safe practices are implemented in
the OR
5. Safe injection practices are implemented to
minimize risk to all surrounding community and
management of adverse event related to injection
are in place.
Check
the presence of client education to avoid unnecessary injections
Spot check /interview whether recapping of used syringes is not
practiced
Check safety boxes are available at right spot, disposed timely
including proper incineration
6. The hospital practices health care waste
management following the national IPPS
guidelines
Observe
Presence of color coded bins
practice of waste segregation,
Presence of primary waste storage area
Presence of well-designed functional incinerator with ash pit
and proper use
Presence of fenced and ventilated placenta pit with tight fitting

cover( if applicable)
Check /interview if safety boxes are disposed safely (quantified,
properly stored and observed) during the incineration.
Proper disposal of liquid wastes check presence of septic tank/
absence of leakage of the sewerage system (waste should not be
discharged without treatment)
If treatment plant is available the quality of discharge should be
acceptable and checked periodically.
7. The hospital ensures the cleanliness and
housekeeping activities
Cleaning audit should be conducted based on the CASH audit
tool schedule
Interventions/solutions are provided to solve the gaps based on
the audit finding(check monthly report collected from
departments/teams
Check/observe the hospital compound cleanliness and
Check /observe service areas are visibly clean and absence of
bad odor and well ventilated
8. The hospital ensures the availability of adequate
and functional toilets, hand washing sinks and
showers
Check
The number of functional toilets are adequate to clients(1 toilet
for20-24 clients
Hand washing facilities are available at all service units
Functional showers at all wards
Proper and separate storage of washed lines
Presence of Hand washing facility
9. The hospital ensures Adequate and functional
laundry service
The facility has adequate laundry space
The hospital has at least two functional washing machines with
ironing
Separate doors for entrance of dirty and clean linen
Separate storage room for clean linen.
Separated cart for clean and soiled linen
Adequate detergents and disinfectants
10. All reusable medical equipment are processed
according to the national IPPS guidelines
Check whether proper decontamination procedures are in place
Check functionality and how they operate autoclave and dry heat
oven or chemicals for sterilization
Check whether proper high level disinfection procedures are in
place
Check whether processed items are properly stored in well-
designed rooms.
11. The hospital has a procedure in place to regulate
traffic flow
Check how the facility handles traffic at procedure rooms as
well as in the premises,

The facility has zoning restriction at OR
Does the Hospital have defined visiting hours, number of
attendants
12. The hospital has a monitoring system to ensure
safety of food and water served in the premises.
Check
the cleanliness of the kitchen
if kitchen staff/food handlers have periodic medical check up
Interview patients/clients to assess that the food served is in
hygienic way and spot check the kitchen utility
If all water sources are lab tested periodically every 3 months.
13. The hospital has a clients’ education system to for
IPPS improvement.
Check
the presence of client education schedule where relevant IPPS
contents is included,
Educational materials and supplies related to IPPS
14. The hospital ensures all the post exposure and
preventive interventions and procedures are in
place in case of occurrence of occupational risks.
Check
If surgical site infections are recorded
If documented action taken to reduce health facility acquired
infections based on observed infection pattern
15. The hospital develops hospital acquired infections
tracking and monitoring system
Check
Recording of surgical site infection and other HAIs
TOTAL ______ ______
CHAPTER 14. FEDERAL AND TEACHING HOSPITAL SERVICES MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital has established functional
management and governance structure that
integrates patient care, medical education and
research.
Check the membership and functionality of the governing board
View the organogram of the hospital
View the JD of CED, CARD,CCD,CAD
View minutes of the executive committee, SMT, Strategic and
annual plan
2. The hospital implements an orientation programme
View the orientation guidelines
Interview five students/interns/residents randomly to check if

for students/interns/residents on hospital policies
and procedures prior to clinical attachments.
they have taken the orientation before clinical attachments.
Interview department head and ward head nurses for
students/interns/residents compliance on policies and
procedures
3. The hospital has established system to ensure care
provided and students’ practice maintains patients’
confidentiality and privacy at all times.
View protocols for conducting teaching on patients.
Interview 10 patient from different wards on their privacy,
confidentiality and their involvement on the care process.
Observe patient care areas
check presence of sill labs and simulation centers
4. The hospital has established protocols/policies and
procedures for ward rounds and bedside students’
teaching to maximize patients’ benefit.
Check for presence of protocol
Interview staff for their knowledge on the protocol and
adherence
Check if student to patient ratio is defined
Time spent for bedside and round teachings is defined (
shouldn’t exceed one hour on one patient)
Consultant’s recommendation on bedside/rounds are
implemented
5. The hospital ensures students/interns/residents’
patient care provided is supervised by their
respective teachers/hospital based instructors at all
times.
View posted program listing supervisors/teachers for specific
unit and for specific date.
Beside the students/interns/residents the hospital assigns a staffs
accountable and responsible for all their respective patient care
activities at all times.
6. The hospital has established guidelines,
memoranda of understanding and procedures for
affiliation with other teaching institutions,
communities and field activities.
View the guidelines/MoU for affiliation, community and field
activities
Check for mechanism to monitoring implementations of
guidelines/MoU
TOTAL _____ ______
CHAPTER 15. MEDICAL EQUIPMENT MANAGEMENT
# Standard Method of Evaluation Met Unmet

1. The hospital has in-house Medical Equipment
Management unit with an operational plan,
required staff and led by a biomedical personnel.
Confirm that hospital has Medical equipment management unit
with the necessary staff
Confirm that the unit is led by a biomedical personnel
2. The Hospital has a Medical Equipment
Management Committee composed of doctors,
nurses, technicians, pharmacists, and
administrative personnel that oversees the medical
equipment management programme.
Review MEC TOR and ensure the following responsibilities are
included: develop and monitor implementation of medical
equipment strategy; oversee establishment of medical equipment
inventory; develop a model medical equipment list; develop and
implement medical equipment policies; determine annual budget
for medical equipment strategy; review incident reports related
to medical equipment.
Verify that MEC membership consists of doctors, nurses,
technicians, pharmacists and administrative personnel.
3. The hospital has an appropriately equipped medical
equipment maintenance workshop.
Check availability of maintenance workshop
Confirm that the workshop is well equipped with the necessary
tools
4. The Hospital has a paper-based and computer-
based or automated inventory management system
that tracks all equipment and spare parts included
in the equipment management programme.
View inventory management system and confirm updated
within past year.
Confirm (by interview with Head of Equipment Maintenance (or
equivalent)) that all medical equipment in the equipment
management program is listed in the inventory.
Confirm (by interview with Head of Equipment Maintenance (or
equivalent)) that the inventory system is used to manage the
stock of spare parts
5. An Equipment History File is maintained for all
medical equipment containing all key documents
for the equipment.
Take a random sample of 10 Equipment History Files and check
that each includes: SOP for equipment use, inventory data
collection form and risk assessment form.
6. The hospital has policies and procedures in place
for acquisition of new medical equipment,
commissioning, decommissioning and disposal of
Obtain copy of policies and procedures for medical equipment
management and verify that they address acquisition,
commissioning, decommissioning, disposal, donations, and
outsourcing technical services.

equipment, the receipt of donations, and
outsourcing technical services for medical
equipment repair and maintenance.
7. All new equipment undergoes acceptance testing
prior to its initial use to ensure the equipment is in
good operating condition, and are installed and
commissioned in accordance with the
manufacturer’s specifications.
Request list of all equipment purchased in the past year.
Randomly select 10 items (or all items if less than 10 were
purchased) and review Equipment Log File. Confirm that this
contains a copy of the Acceptance Test Log Form.
8. All equipment operators and personnel are trained
on proper operation, safety, and maintenance of
medical equipment with standard operating
procedures readily available to the user.
Visit a minimum of 3 different departments/case teams (for
example ER, laboratory, pharmacy, delivery, patient wards etc).
Select two items of medical equipment in each department.
View SOP for each item. Interview staff on duty and confirm
that each one has received training on the use and maintenance
(where relevant) of the item.
9. There is a schedule for inspection, testing and
preventive maintenance for each piece of
equipment as guided by the manufacturer’s
recommendations and that schedule is
appropriately implemented.
For the 10 randomly selected Equipment History Files confirm
that the schedule for Inspection, testing, and maintenance is
present in the equipment history file and confirm that inspection,
testing and maintenance has been conducted as described in the
schedule.
10. There is a notification and work order system for
corrective maintenance and calibration of medical
equipment based on their level of risk.
Identify written protocol for medical equipment work orders.
Review at least 5 copies of notification and work order and
reports.
TOTAL _____ ______
CHAPTER 16. FACILITY MANAGEMENT

# Standard
Method of Evaluation Met Unmet
1 The hospital complies with relevant laws,
regulations, and facility inspection requirements.
Interview CEO to identify any relevant laws, regulations or
inspection requirements and confirm that the hospital complies
with these.
2 Designated hospital staff members are assigned
for facility maintenance and safety functions.
View organization chart.
Confirm on organization chart (or by interview with HR Dept
Head) that the hospital has assigned individuals for the following,
as a minimum: masonry, plumbing, electrical installation,
landscape and garden, sewerage.
3 The hospital grounds are regularly inspected,
maintained, and, when appropriate, improved to
ensure cleanliness of grounds and safety of
patients, visitors and staff.
Interview Facilities Manager (or equivalent). Check
process/schedule for grounds inspection and maintenance.
View patient and staff areas (garden, waiting areas etc). Confirm
that these are tidy, clean and free from hazards (e.g. discarded
equipment or other materials).
4 Potable water is available 24 hours a day, seven
days a week through regular or alternate sources
to meet essential patient care.
Interview CEO or Head of Facilities. Confirm that an alternative
source of water exists (e.g. tank, well). Obtain documentary
evidence that the alternate source/ and or mains source are tested
for safety at a minimum every six months.
5 Electrical services are available 24 hours a day,
seven days a week through regular or alternate
sources to meet essential patient care.
Interview CEO or Head of Facilities. Confirm that an alternative
power source is available. Confirm that this is sufficient to
provide power to essential patient areas including wards,
emergency room, labour and delivery and laboratory.
6 The hospital has a maintenance center with
technical personnel, sufficient space and adequate
ventilation to conduct maintenance and repair
work on the facility operating systems (e.g.,
electrical, water, sanitation, sewerage and
ventilation) and equipment. This includes proper
hand washing facilities, proper disinfection and
cleaning of equipment facilities, a storage area,
and a library.
View maintenance center. Confirm that this has adequate space
and is not crowded. Confirm that the medical equipment service
is separated from the general maintenance area. Confirm that
there are hand-washing facilities, facilities for cleaning and
disinfection, a storage area and a library.
7 The maintenance centre has appropriate tools and
Interview Head of Maintenance Dept. (or equivalent). Confirm
that sufficient tools are available for all maintenance functions

testing equipment to perform repairs, as well as
procedures to ensure the routine calibration of the
testing equipment is performed as required.
and that routine calibration of testing equipment is performed as
required.
8 The hospital conducts regular preventive and
corrective maintenance for all facilities and
operating systems (e.g., electrical, water,
sanitation, sewerage and ventilation) to ensure
patient and staff safety and comfort.
Interview Head of Maintenance Dept. (or equivalent). Confirm
that regular preventive and corrective maintenance is conducted.
View maintenance logs. Confirm that maintenance logs exist for,
as a minimum: electrical systems, water and sewerage.
9 There is a notification and work order system for
facility and operating system (e.g., electrical,
water, sanitation, sewerage and ventilation)
repairs.
Interview Head of Maintenance Dept. (or equivalent). Confirm
that a notification and work order system exists.
View at least 5 recent work order requests and reports.
10 The hospital has a transport policy for the use of
and access to hospital vehicles.
View transport policy.
View logs of two hospital vehicles and confirm that vehicle use
complies with transport policy
11 The hospital has a policy addressing access to the
hospital premises.
View policy.
Visit two wards and confirm that all caregivers are wearing
appropriate ID badges.
Confirm that all staff interviewed in the course of this assessment
are wearing ID badges.
12 The hospital has a fire safety plan that addresses
both the prevention and response to fires. A ‘Fire
and Evacuation Drill’ is conducted at least
annually.
View fire safety plan.
Obtain documented evidence of most recent Fire Drill and
confirm that this was conducted within the past one year.
13 The hospital has a plan for responding to likely
community or hospital emergencies, epidemics
and natural or other disasters.
View response plan.
14 Staff members are trained and knowledgeable
about their roles in the plans for fire safety,
Interview 10 randomly selected staff members from different
Case Teams. Confirm that each one knows what action to take
and their individual responsibility in the event of a fire, security

security, hazardous materials, and emergencies. threat or other emergency.
TOTAL _____ ______
CHAPTER 17. HUMAN RESOURCE MANAGEMENT
# Standard
Method of Evaluation Met Unmet
1. The hospital has a Human Resources
Management Directorate/Department/ Support
Process staffed by individuals who possess
management knowledge, skills and experience
dealing with individual personnel matters and
teams.
Identify designated staff members of the HR case team
Check experience of case team members and confirm that
personnel staff have requisite skills (training and personnel
management experience).
2. The Human Resources Directorate/Department/
Support Process maintains a personnel file for
each and every hospital employee.
Interview Head of HR Case Team. Confirm that the hospital has
personnel files for all grades of employees
Take a random sample of 10 personnel files from different case
teams/departments and ensure that they contain at a minimum:
personal contact information, appointment letter, employee job
description, medical certificate and performance evaluation.
3. The hospital establishes and institutionalizes
Human Resources Information Management
Systems (HRIS) that enhance the HR
management functions.
Confirm implementation of HRIS through viewing
Check information are up to date
4. The Human Resource Head (or equivalent) is a
member of the hospital Senior Management
Team.
Obtain list of SMT members from CEO and confirm that Head of
HR Case Team is a member.
5. The hospital has a human resource development
plan that addresses staff numbers, skill mix and
staff training and development.
Review a copy of the human resource development plan.
Ensure that it addresses staff numbers, skill mix and staff training
and development.
6. Each employee’s responsibilities are defined in a
See standard 11.2 above. Confirm that the 10 randomly selected
files contain a signed employee job description.

current job description, which has been signed by
the employee and filed in the personnel file.
7. The hospital has policies and procedures for
recruitment and hiring of staff.
Identify written policies for recruiting and hiring staff.
8. The Human Resource Directorate/Department/
Support Process provides services to employees
to ensure satisfactory productivity, motivation,
and morale as evidenced by effective policies and
procedures for personnel retention, compensation
and benefits, training and development and
employee recognition.
Identify documented policies that support employee motivation
and retention including as a minimum: policy for compensation
and benefits, training and development and employee recognition.
9. Human Resource policies are documented in an
Employee Hand Book that is distributed to all
staff and updated, at a minimum, every 3 years.
The employee hand book contains policies and
procedures that define employee/employer
relations, the rights and obligations of employees/
employer, employee services and benefits,
promotion and employee development
procedures.
Obtain a copy of the hospital’s Employee Manual
Ensure that it contains Hospital personnel policies and procedures
such as working hours, leave, benefits.
Ensure that it has been updated and is current (within 3yr renewal
window).
Verify that it has been disseminated among staff by interviewing
a random sample of 10 staff and asking them if they have a copy
of the employee manual.
10. The hospital has a Code of Conduct and
Professional Ethics that is known, and adhered to,
by staff.
Obtain a copy of employee code of conduct.
See 11.8 above: interview 10 random staff members from
different Case Teams and ask if they are familiar with the Code
of Conduct and ask each to describe (in general terms) the areas
covered in the Code of Conduct. Confirm that each has a general
understanding of the principles and main provisions of the Code
of Conduct.
11. The hospital has a performance management
process and reward policies in which all
employees are formally evaluated at least semi-
annual, higher performers are recognized and
See Standard 11.2 above. Confirm that the 10 randomly sampled
files contain a performance evaluation conducted within the past
year (with the exception of new employees who are currently in
their probation period). Where relevant, confirm that there is a
documented action plan for any staff member with poor
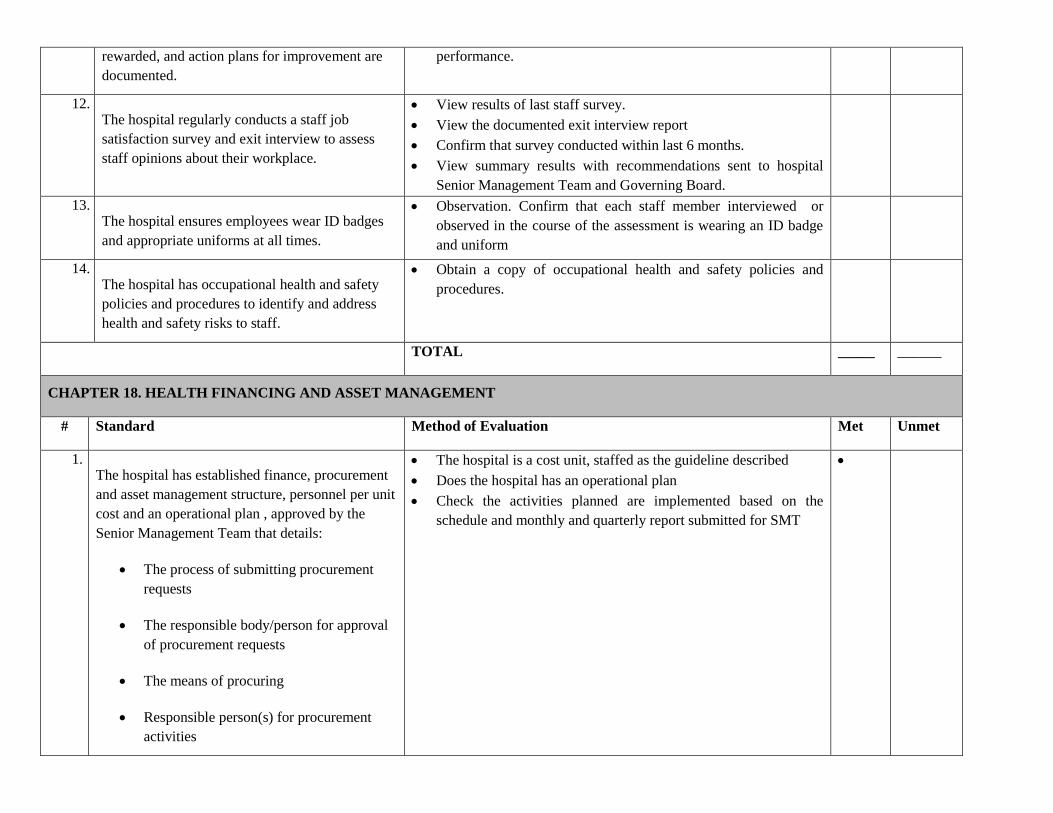
rewarded, and action plans for improvement are
documented.
performance.
12. The hospital regularly conducts a staff job
satisfaction survey and exit interview to assess
staff opinions about their workplace.
View results of last staff survey.
View the documented exit interview report
Confirm that survey conducted within last 6 months.
View summary results with recommendations sent to hospital
Senior Management Team and Governing Board.
13. The hospital ensures employees wear ID badges
and appropriate uniforms at all times.
Observation. Confirm that each staff member interviewed or
observed in the course of the assessment is wearing an ID badge
and uniform
14. The hospital has occupational health and safety
policies and procedures to identify and address
health and safety risks to staff.
Obtain a copy of occupational health and safety policies and
procedures.
TOTAL _____ ______
CHAPTER 18. HEALTH FINANCING AND ASSET MANAGEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital has established finance, procurement
and asset management structure, personnel per unit
cost and an operational plan , approved by the
Senior Management Team that details:
The process of submitting procurement
requests
The responsible body/person for approval
of procurement requests
The means of procuring
Responsible person(s) for procurement
activities
The hospital is a cost unit, staffed as the guideline described
Does the hospital has an operational plan
Check the activities planned are implemented based on the
schedule and monthly and quarterly report submitted for SMT

A five year plan for major capital
purchases
2. Bilingual service fee schedule posters are
displayed beside each departmental reception desk,
in all waiting areas and at all cash points. Each
poster shows the fees and advises patients to obtain
and keep receipts for all payments.
Visit different departments (OPD, ER, and inpatient wards and
cash collection points) and confirm that bilingual service fee
schedule posters are clearly displayed.
Confirm that the poster shows fees and
advises that patients should to keep receipts for all payments.
3. The hospital provides exempted services in
accordance with the relevant Federal/Regional
Legislation and displays a list of exempted services
at appropriate locations through the hospital for the
information of patients, staff and the public.
Obtain relevant Federal/Regional Health Care Finance Reform
Directive.
Obtain list of all exempted services that are provided by the
hospital.
Confirm that the list displayed at appropriate place in the hospital
and matches the list in the federal/Regional Directive.
4. The hospital provides all services indicated in
health insurance benefit package in accordance
with the agreement and should be displayed at
appropriate locations through the hospital for
information for the patients, staff and the public.
Get the contractual document
Take sample patient records and visit each department and
confirm whether the services indicated in the benefit package are
properly provided to beneficiaries.
Check proportion of services provided within the hospital or in
facilities with insourcing contracts
Check out of pocket payment s by beneficiaries and compare with
compliments.
5. The hospital submits timely payment
requests/claims /reimbursements for services to the
Health Insurance Agency and fee waiver
beneficiaries in accordance with established
standards and formats.
Ensure that claim request formats are appropriate and are
available both in hard and soft copy
Confirm that claim documents are properly prepared and timely
submitted to insurance schemes
Confirm that all visits by health insurance beneficiaries are
properly recorded and documented
6. The hospital keeps records of services provided to
Confirm that financial records of health insurance, fee waiver and
exempted service beneficiaries properly (separately) kept and

eligible health insurance, fee waiver and exempted
service beneficiaries and related financial
information as appropriate and, reported to the
relevant body
documented
View most recent two quarters reports submitted to concerned
bodies
Take list of samples beneficiaries and confirm that whether the
beneficiaries are included in the list of eligible health insurance,
fee waiver and exempted service beneficiaries
7. The hospital ensures a private wing service is
established in accordance with the required federal
/regional directives and approved by the Hospital
Governing Board.
Establishment of private wing services was approved by the
board
The private wing services fees are approved by the board
Staff performance at private wing is equivalent with the regular
hours
check for mechanisms of reimbursing supplies of the hospitals
that are utilized for private wing services
8. In a hospital where services are outsourced,
procedures are in place to monitor the contract and
services provided and contractual agreements
comply with relevant government directives.
Confirm that an assessment of the feasibility of outsourcing
services has been undertaken and project plan developed.
Confirm Contractual agreement procedures have been developed
that define the outsourcing process and what services are
outsourced
view the most recent performance reports of outsourced service
9. The hospital establishes multi-year budgeting and
expenditure which link to programs and priorities
of each department and fiscal information is
channeled through various medium of
communication.
Confirm that Existence of hospital strategies with multi-year
Costing of recurrent and capital expenditure.
Verify that there is a linkage between capital budgets and forward
expenditure estimate by reviewing multiyear budget Document.
Expenditures are linked to technical programs, MOH Priorities,
and expected results.
Capital budgets are consistently selected on the basis of relevant
hospital strategies and recurrent cost implications in accordance
with hospital budget allocations and included in forward budget
estimates for the hospital.
Obtain Annual budget documentation (a complete set of
documents can be obtained by the public through appropriate
means when it is approved by GB.
Confirm that In-year budget execution reports (the reports are
routinely made available to the public through appropriate
means within one month of their completion).

External audit reports (all reports on consolidated operations are
made available to the public through appropriate means within
six months of completed audit).
Contract awards (award of all contracts with value above approx.
ETB 100,000 equiv) are published at least quarterly through
appropriate means).
10. The hospital stock management ranging from
identifying the need for a property to materials and
supplies in order to receive, use and dispose
complies with the relevant guidelines and
disaggregated by each department.
View annual procurement plan that is approved by the hospital
leadership.
Use of competitive procurement methods(When contracts are
awarded by methods other than open competition, they are
justified in accordance with the legal requirements)
View reports and confirm assets are included in annual inventory
11. The hospital stock management ranging from
identifying the need for a property to materials and
supplies in order to receive, use and dispose
complies with the relevant guidelines and
disaggregated by each departments
There is effective internal controls comprise the comprehensive
set of rules and procedures that serve to reduce the risk of
mistakes and fraud and safeguard assets.
Verify Degree of compliance with rules for processing, recording,
use and disposal of stokes with relevant guidelines.
12. The Hospital accounting system should produce
and access periodic reports to the relevant bodies
at all levels.
View last 3 month financial report and confirm that each
provides details of credit granted, credit repaid and balance
outstanding
Routine data collection or accounting systems provide reliable
information on all types of resources received in cash and in-kind
by departments across the hospital. The information is
compiled into reports at least quarterly
Verify that regular, timely, and accurate information on actual
budget performance is produced at least quarterly and used for
decision by SMT and GB.
13. Internal audit on quarterly basis and external audit
at least once in a year conducted and reports are
reviewed by the senior management and
Governing Board.
Internal audit is operational for the hospital and generally meets
professional standards. It is focused on systemic issues.
Reports adhere to a fixed schedule and are distributed to the
SMT, GB, and relevant bodies.
Action by management on internal audit findings is prompt and
comprehensive.

TOTAL _____ ______
CHAPTER 19. CLINICAL GOVERNANCE AND QUALITY IMPROVEMENT
# Standard Method of Evaluation Met Unmet
1. The hospital has a Clinical Governance and
Quality Improvement Unit that is led by an
assigned Senior Physician or General Practitioner.
Interview head of the CG&QI unit and check the organogram of
the Hospital
Ensure that the Head is a motivated senior Physician or a General
Practitioner
View TOR and list of members of Quality Committee.
Check the minutes of the Quality Committee to ensure whether
regular meetings are being conducted and the content of meetings
Receive a copy of the unit’s annual plan
2. The hospital should develop a clinical governance
and quality improvement strategy and an operation
plan that addresses the key components of quality.
View Clinical Governance and Quality Improvement strategy.
Ensure that the strategy includes:
o Safety and risk management
o Clinical effectiveness
o Professional competence
o Patient focused care
o Patient and public involvement
o Benchmarking
Confirm (by interview with Unit Head or documentary evidence)
that reports on implementation of CG&QI strategy are received
by Senior Management Team from the CG&QI unit.
3. Procedures are established to monitor clinical
practices and standards through services’ specific
process and outcome measures to enable the
hospital to address any problems identified.
Interview chair of CG&QI unit head and ask for list of clinical
outcome measures that are monitored regularly.
Ask CG&QI unit head to show the most recent results of at least 3
clinical outcome measures.
Determine (by interview with CG&QI unit head) that appropriate
action was taken in response to the outcome measures.
Check and confirm with selected staff from various service areas
whether they are aware of clinical outcome measures in their
respective service areas

Check that the hospital has a continuous quality improvement
systems that is used to provide safe and quality service
4. The hospital implements a regular clinical audit
program in each service area. Such program
encourages the participation of all clinical staff and
includes the implementation of a quality
improvement plan derived from audits.
Get documented reports of clinical audits.
Check and ensure that all relevant clinical service areas are
audited.
Check the composition audit team. The audit report should
demonstrate that all relevant service unit staff and service users
(when mandatory) are involved.
Check whether re-audits are conducted to close gaps identified
during previous audits. Determine if there is an improvement.
5. Procedures are established to assess and minimize
risk arising from the provision and delivery of
health care. A system is also in place for reporting
and analyzing incidents, errors and near misses
View risk assessments of inpatient, outpatient and ER case teams
and other departments.
Check date of risk assessment and confirm that it was conducted
within the previous 1 year.
Check to ensure that appropriate system for gathering, recording
and evaluating quality and safety of care is available
Confirm that the hospital has an Incident Officer who has a job
description that outlines his/her duties in relation to Incident
Investigation and management.
View two recent Incident Reports (if any) and confirm that the
reported incidents were investigated and any necessary follow up
action documented by the Incident Officer.
Confirm that the hospital has a system to identify, analyze and
monitor risks, adverse events, incidents, errors and near misses.
6. The hospital adopts a statement of patient rights
and responsibilities, which is posted in public
places in the hospital.
View statement of patient rights and responsibilities.
Visit patient service areas (as a minimum OPD, ER and inpatient
wards) and confirm that statement is clearly displayed.
7. The hospital continuously and systematically
reviews and improves all aspects of its activities
that directly affect patient safety and apply best
practice in assessing and managing risks to
patients, staff and others.
View patient Involvement strategy.
Confirm (by interview with CEO or Chair of QC) that at least two
of the following activities have been conducted within the past 6
months:
o Suggestion boxes in patient service areas
o Complaints procedures
o Public meetings
o Establishment of patient groups

o Activities to engage marginalized groups
8. The hospital monitors patients’ experiences with
care through patient and satisfaction surveys
conducted on a quarterly basis.
View results of last patient satisfaction survey.
Confirm that survey conducted within last 6 months.
Check and confirm that actions were taken as a results of patient
satisfaction survey
9. The hospital implements a strategy for the
involvement of patients and the public in service
design and delivery including procedures to be
followed when engaging with patients and the
public.
View minute document of the Hospital’s Public Forum
Confirm that public forums or town hall meetings are conducted
at least every quarter.
Check whether the hospital informs the public through
o Patient information leaflets
o Poster displays in hospital or community
o Publications in local press
o Presentations at public meetings
Check and confirm suggestion box is used in the hospital and that
suggestions are compiled, analyzed and acted up on.
Confirm Community representation on hospital Governing Board
10. The hospital develops and implements a strategy to
provide patient focused care which incorporates,
compassion, respect and dignity for patients,
effective communication, better hotel services and
involvement of patients in the care delivery.
View hospital Compassionate, Respectful and Caring Healthcare
Professional Strategy
View and confirm whether the strategy covers issues about
respect and dignity, effective communication, better hotel
services (housekeeping, nursing care, balanced diet (food)
services, laundry services)
Randomly ask and confirm patients and care givers in ward if
patients concerns are taken into account and they are involved in
the care delivery.
11. The hospital participates in benchmarking
activities to learn from and share good practice
with other hospitals.
Confirm (by interview with CEO or other documented evidence)
that hospital participates in benchmarking activities. For example
regular attendance at regional hospital/RHB meetings;
participation in hospital cluster activities etc.
Check and confirm that the hospital attends EHAQ Cluster
meetings
Check and confirm with selected hospital staff that they are aware of
EHAQ Change Package

TOTAL _____ ______
CHAPTER 20. MONITORING AND REPORTING
Std # Standard Method of Evaluation Met Unmet
1. The hospital has an HMIS Monitoring Team (or
equivalent) which collaborates with the CG&QIU
in reviewing the HMIS indicators and takes action
to address any areas of concern.
Interview CEO. Confirm that HMIS/KPI Performance Monitoring
Team (or equivalent) is in place.
View TOR of HMIS/KPI Monitoring Team to confirm that role
includes review of indicators.
View minutes of last 3 HMIS/KPI performance monitoring team
meetings to confirm that HMIS/KPI indicators are reviewed and
action taken as a result.
2. The hospital conducts a self-assessment of its own
performance at a minimum every quarter, using
HMIS indicators and any additional local
indicators determined by hospital management.
View copy of last 3 self-assessment meetings. Confirm that
frequency was monthly.
Check with relevant staff whether there is an action plan as a result
of the self-assessment.
Check whether there is an implementation plan in place to
implement those action plans
3. The hospital submits monthly, quarterly and
annual HMIS reports to the relevant higher office
within the agreed timelines.
View HMIS/KPI reports for last year. Confirm that monthly,
quarterly and annual reports were submitted as per schedule.
Check whether the report submitted is accurate and timely
4. The correspondence between data reported on
HMIS forms and data recorded in registers and
patient / client records, as measured by Data
Quality Assurance (DQA) and Lot Quality
Assurance Sample (LQAS) is ≥85%.
View LQAS result on last 3 HMIS/KPI reports.
Confirm LQAS is > 85%.
5. In collaboration with the Governing Board through
the CEO, the Clinical Governance and Quality
Improvement Unit have established performance
indicators for the hospital that are described in
hospital performance reports presented by the CEO
to the Governing Board as a minimum every
quarter.
View last 3HMIS and KPI reports submitted to Governing Board.
Confirm that frequency of HMIS and KPI reports to Governing
Board was quarterly as a minimum.

6. Indicators included in the hospital performance
monitoring system are a combination of
national/regional indicators and other local
indicators as determined by the Governing Board.
View list of KPI indicators and confirm that some are national
indicators (HMIS) while others are local indicators set by the RHB
7. Hospital staff receive orientation on all
performance indicators and case
teams/departments determine indicators and
monitor their own performance using the process
improvement model.
Check and verify with selected staff about their awareness of
KPI’s.
Check availability of data owners from each case team/service
area.
View reports/minutes of case team on performance data utilization.
TOTAL _____ ______

Summary Table
Chapter Number of Standards
Met
% of Standards
Unmet
Hospital Leadership, Management and Governance (8
standards)
Liaison, Referral and Social Services (8 standards)
Emergency Medical Services (8 standards)
Outpatient Services (7 standards)
Inpatient Services (9 standards)
Medical Records Management (8 standards)
Nursing and Midwifery Care Services (10standards)
Maternal, Neonatal and Child Health Services (12
standards)
Laboratory Services (14 standards)
Pharmacy Services (12 standards)
Radiological and Imaging Service Management (6
standards)
Rehabilitative and Palliative Care (5 standards)
Infection Prevention and Patient Safety (15 standards)
Federal and Teaching Hospitals Management (6
standards)
Medical Equipment Management (10 standards)
Facility Management (14 standards)
Human Resource Management (14 standards)
Health Financing and Asset Management (13 standards)
Clinical Governance and Quality Improvement (11
standards)
Monitoring and Reporting (7 standards)

Total (197 standards)
Name of Hospital: Region:
Date of assessment: Name of lead assessor:
Signature:
Contact telephone: Contact email: