effects of liraglutide on heart rate and heart rate ...reduced heart rate variability (hrv) and...
TRANSCRIPT
Effects of Liraglutide onHeartRateand Heart Rate Variability: ARandomized, Double-Blind,Placebo-Controlled CrossoverStudyDiabetes Care 2017;40:117–124 | DOI: 10.2337/dc16-1580
OBJECTIVE
Reduced heart rate variability (HRV) and increased heart rate (HR) have beenassociated with cardiovascular mortality. Glucagon-like peptide 1 receptor ago-nists (GLP-1 RAs) increase HR, and studies have suggested that they may reduceHRV. We examined the effect of the GLP-1 RA liraglutide on HRV and diurnalvariation of HR in overweight patients with newly diagnosed type 2 diabetes(T2D) and stable coronary artery disease (CAD).
RESEARCH DESIGN AND METHODS
Liraglutide or placebo was administrated to a backbone therapy of metformin inthis double-blind, placebo-controlled 12 + 12–week crossover study. SD of beat-to-beat (NN) intervals (SDNN) was assessed by 24-h Holter monitoring as a mea-sure of HRV. Diurnal HR variation and sympathovagal balance analyzed by rootmean square of successive differences (RMSSD) in NN intervals and high-frequency (HF) and low-frequency (LF) power were assessed.
RESULTS
Compared with placebo, liraglutide decreased SDNN in 27 subjects (233.9 ms; P <0.001, paired analysis); decreased RMSSD (20.3 log-ms; P = 0.025); and increasedthemean HR (8.1 beats/min; P = 0.003), daytime HR (5.7; P = 0.083), and nighttimeHR (6.3; P = 0.026). In a multivariable regression analysis, the decrease in SDNNremained significant after adjustment for metabolic and HR changes. Liraglutidereduced HF power (20.7 log-ms2; P = 0.026) without any change in LF/HF ratio.
CONCLUSIONS
In overweight patients with CAD and newly diagnosed T2D, liraglutide increasedHR and reduced HRV despite significant weight loss and improvement in meta-bolic parameters. The increase in nightly HR in conjunction with a decrease inparameters of parasympathetic activity suggests that liraglutide may affect sym-pathovagal balance.
Autonomic imbalance, characterized by increased sympathetic and decreased para-sympathetic activity, is associated with various pathological conditions, such ascoronary artery disease (CAD) (1), cardiovascular death (2), and heart failure (3).Heart rate variability (HRV), a measure of beat-to-beat variation in heart rate (HR),
1Department of Cardiology, Copenhagen Uni-versity Hospital of Bispebjerg, Copenhagen,Denmark2Department of Internal Medicine, CopenhagenUniversity Hospital of Amager, Copenhagen,Denmark3Department of Endocrinology, CopenhagenUniversity Hospital of Hvidovre, Copenhagen,Denmark4Clinical Research Center, Copenhagen Univer-sity Hospital of Hvidovre, Copenhagen, Denmark
Corresponding author: Preman Kumarathurai,[email protected].
Received 22 July 2016 and accepted 1 October2016.
Clinical trial reg. no. NCT01595789, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc16-1580/-/DC1.
This article is featured in a podcast available athttp://www.diabetesjournals.org/content/diabetes-core-update-podcasts.
© 2017 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
Preman Kumarathurai,1
Christian Anholm,2 Bjørn S. Larsen,1
Rasmus Huan Olsen,1 Sten Madsbad,3
Ole Kristiansen,1 Olav W. Nielsen,1
Steen B. Haugaard,2,4 and
Ahmad Sajadieh1
Diabetes Care Volume 40, January 2017 117
CARDIOVASCULA
RANDMETA
BOLIC
RISK

provides information on autonomic bal-ance and is impaired in patients withtype 2 diabetes (T2D) (4). The SD ofbeat-to-beat (NN) intervals (SDNN), de-rived from 24-h time domain compo-nents of Holter monitoring, is a widelyused measure of HRV and regarded as amore-sensitive assessment method ofautonomic balance than single auto-nomic reflex tests in subjects with T2D(5). Both reduced SDNN and increasedHR are associated with an increased riskof cardiovascular mortality (1,6). High-frequency (HF) and low-frequency (LF)powers are components of the fre-quency domain parameters of HRV. HFpower primarily represents respiratoryvariation, is mediated by parasympa-thetic activity, and is highly correlated tothe rootmean square of successive differ-ences (RMSSD) inR-R variability. LF powerreflects primarily the oscillatory rhythmof the baroreceptors and is modulatedby both the parasympathetic and thesympathetic nervous systems (7,8). Bothtime and frequency domain componentsprovide information on the sympathova-gal balance and have prognostic value invarious populations, such as patients withdiabetes (6,9), myocardial infarction (10),and heart failure (11).Glucagon-like peptide 1 receptor ag-
onists (GLP-1 RAs) have emerged as apromising treatment option in patientswith T2D and have been shown to re-duce glycated hemoglobin (HbA1c) andinduce weight loss (12). Although inten-sified treatment and improvement inglucose metabolic parameters havebeen associated with HRV improvement(13), some experimental studies havesuggested that GLP-1 and GLP-1 RAsmay reduce HRV (14–16). Furthermore,some concerns have been raised aboutthe observed increased HR during GLP-1RA therapy (17). Only a few data exist onhow GLP-1 RAs affect long-term HRV inconjunction with changes in glucometa-bolic parameters. Hence, this study ex-amined the effects of 12 weeks oftreatment with the long-lasting GLP-1RA liraglutide on HR and HRV in over-weight patients with newly diagnosedT2D and stable CAD.
RESEARCH DESIGN AND METHODS
Study Design and ParticipantsThis is a randomized, double-blind, placebo-controlled 12 + 12–week crossover study
with a 2-week washout period. The de-tails of the study protocol have beenpublished previously (18). Briefly, pa-tients with newly diagnosed T2D andstable CAD underwent 12 weeks of lir-aglutide and placebo treatment addedto a backbone therapy of metformin.Patients were recruited through pa-tient files from May 2012 to October2014 from selected hospitals in Copen-hagen, Denmark. Patients who were tak-ing antidiabetic treatment before thestudy underwent a minimum 2-weekwashout period before the baseline visit.Subcutaneous injections of liraglutide/placebo and metformin tablets were ti-trated in an identical manner in both pe-riods. An initial dose of 0.6 mg o.d.liraglutide/placebo + 500 mg b.i.d. met-formin was increased after 14 days to1.2 mg o.d. + (1,000 mg + 500 mg) dailyand to 1.8 mg o.d. + 1,000 mg b.i.d. after28 days. Efforts were made to give sub-jects the same dosage of study drug inboth periods and to keep the back-ground cardiovascular medication un-changed throughout the study. Subjectswere instructed not to perform anytasks or physical activity that may influ-ence the recordings. Each subject un-derwent 48-h Holter monitoring beforeand after each intervention for a total offour times (weeks 0, 12, 14, and 26). Acomputer was used to perform 1:1 ran-domization (placebo first or liraglutidefirst). Subjects, investigators, and allcaregivers were blinded to the treatmentsequence, which was concealed until theend of the study.
Holter MonitoringHolter monitoring for up to 48 h wasperformed (Rozinn RZ 153+12; RozinnElectronics). All recordings were per-formed with seven leads to create athree-channel electrocardiogram out-put. The sampling rate for the electro-cardiogram recordings was 180/s. Theprimary editing and analyses of Holterrecordings were performed by an expe-rienced technician from the Holter lab-oratory of the Copenhagen UniversityHospital of Bispebjerg. If the frequencyof ectopic complexes constituted .20%of QRS complexes in a segment, that seg-ment was deleted. If noise implied unde-tectable QRS complexes in all three leads,the corresponding segment was deleted.All HRV analyseswere based on variationsin normal complexes. Frequency domain
components of HRVwere calculated afterfast Fourier transformation of the R-R in-terval data using Cooley-Tukey algorithmwith 300-s data segments as input. Timedomain components of HRV were ana-lyzed and compared using recordings ofequal length (full 24 h) for each subject,and the following parameters were iden-tified: the mean value of all NN intervalsand SDNN, RMSSD, SD of the averages ofNN intervals in all 5-min segments(SDANN), and SDNN for all 5-min seg-ments of the entire recording (SDNN-index)(7). In frequencydomain analysis, the spec-tral results were obtained from 5-minsegments and averaged over 24 h, andthe following parameters were as-sessed: LF power (0.04–0.15 Hz), HFpower (0.15–0.4 Hz), total power (TP)(#0.4 Hz), and LF/HF ratio. Furthermore,normalized units of LF and HF powerwere calculated to obtain values inde-pendent of total variability (LFnorm =LF/TP; HFnorm = HF/TP). Changes inSDNN-index and RMSSD were assessedunder more standardized conditionsduring nighttime (2:00–3:00 A.M.). MeanHR, minimum HR, maximum HR, and di-urnal variation in HR were assessed. Di-urnal HR variation was analyzed usingfull recording time, and hourly HR wascalculated as the average from 2 consec-utive days, when available. In addition,diurnal variations of the following parame-ters were assessed: SDNN-index, RMSSD,LF, HF, LF/HF ratio, LFnorm, and HFnorm.Daytimewas defined as 7:00 A.M.–10:00 P.M.
and nighttime as 11:00 P.M.–6:00 A.M.
Statistical AnalysisDistribution of data (normal or nonnormal)was evaluated by visual assessment ofhistograms and by Shapiro-Wilk test(19,20). Log-transformation of data wasused to normalize variables with skeweddistribution (SDNN index, RMSSD,SDANN, LF, HF, LF/HF ratio, LFnorm,and HFnorm) (8,19). Treatment effectsof liraglutide and placebo werecompared by using the paired t test.For nonnormally distributed data, Wil-coxon signed rank test was used. Theassociation between variables of interestwas examined by using linear regression.Intention-to-treat (ITT) population wasdefined as subjects with valid Holterrecordings for a minimum of one period.ITT analysis was performed for SDNN byusing a linear mixed model with randomeffects for subjects and fixed effects for
118 Effects of Liraglutide on Heart Rate Variability Diabetes Care Volume 40, January 2017
period and treatment. Prespecifiedpower analysis provided a statisticalpower of 90% for 16 subjects in pairedanalyses at P , 0.05 (18). A two-sidedP , 0.05 was considered statisticallysignificant. All statistical analyses wereperformed with Stata 13.1 software(StataCorp, College Station, TX).
Ethics and DisseminationThis trial was carried out in accordancewith the International Conference onHarmonization Good Clinical Practicestandards and complies with the Decla-ration of Helsinki. The Good ClinicalPractice Unit for Eastern Denmark per-formed the monitoring. Written in-formed consent was obtained fromeach subject. This trial was approvedby the Regional Committee on Bio-medical Research Ethics of the CapitalRegion of Denmark and the DanishMed-icines Agency.
RESULTS
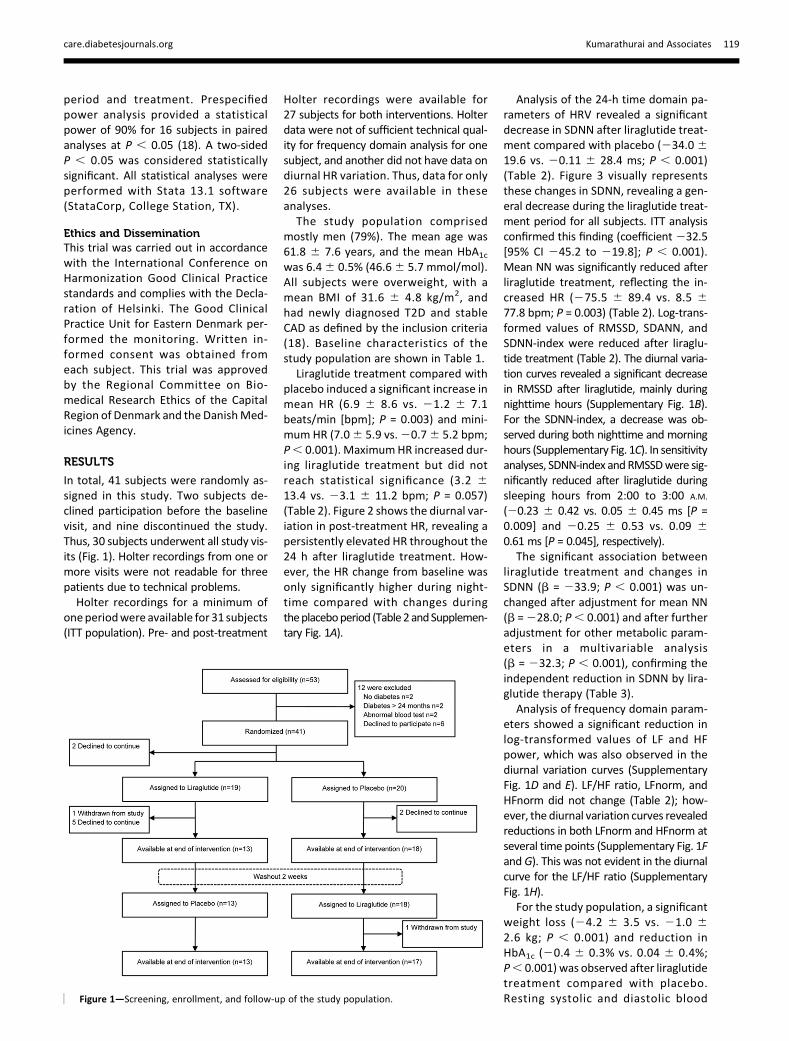
In total, 41 subjects were randomly as-signed in this study. Two subjects de-clined participation before the baselinevisit, and nine discontinued the study.Thus, 30 subjects underwent all study vis-its (Fig. 1). Holter recordings from one ormore visits were not readable for threepatients due to technical problems.Holter recordings for a minimum of
oneperiodwere available for 31 subjects(ITT population). Pre- and post-treatment
Holter recordings were available for27 subjects for both interventions. Holterdata were not of sufficient technical qual-ity for frequency domain analysis for onesubject, and another did not have data ondiurnal HR variation. Thus, data for only26 subjects were available in theseanalyses.
The study population comprisedmostly men (79%). The mean age was61.8 6 7.6 years, and the mean HbA1cwas 6.46 0.5% (46.66 5.7 mmol/mol).All subjects were overweight, with amean BMI of 31.6 6 4.8 kg/m2, andhad newly diagnosed T2D and stableCAD as defined by the inclusion criteria(18). Baseline characteristics of thestudy population are shown in Table 1.
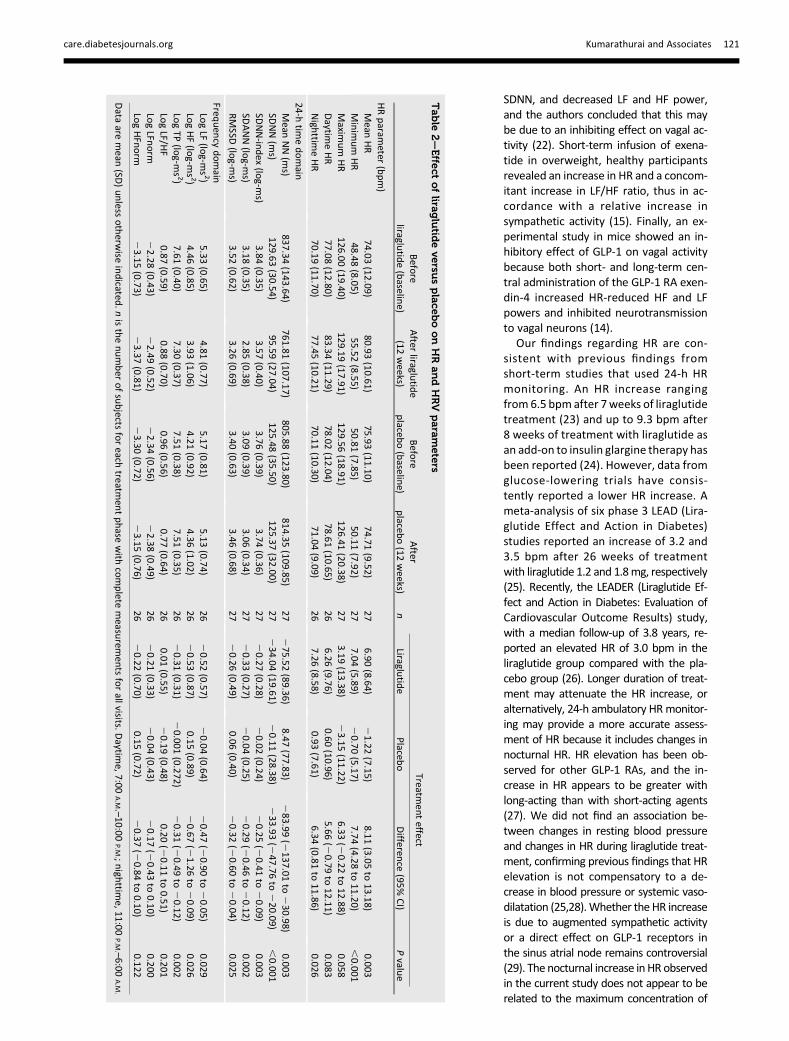
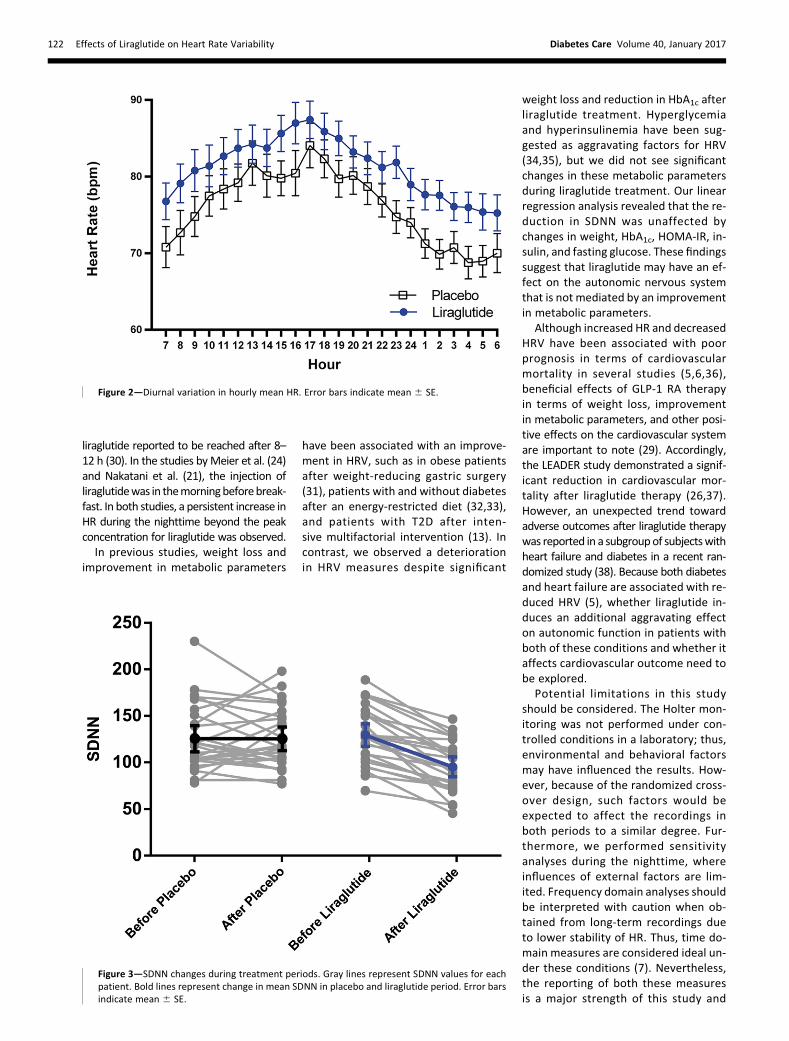
Liraglutide treatment compared withplacebo induced a significant increase inmean HR (6.9 6 8.6 vs. 21.2 6 7.1beats/min [bpm]; P = 0.003) and mini-mum HR (7.06 5.9 vs.20.76 5.2 bpm;P, 0.001). MaximumHR increased dur-ing liraglutide treatment but did notreach statistical significance (3.2 613.4 vs. 23.1 6 11.2 bpm; P = 0.057)(Table 2). Figure 2 shows the diurnal var-iation in post-treatment HR, revealing apersistently elevated HR throughout the24 h after liraglutide treatment. How-ever, the HR change from baseline wasonly significantly higher during night-time compared with changes duringtheplaceboperiod (Table2andSupplemen-tary Fig. 1A).
Analysis of the 24-h time domain pa-rameters of HRV revealed a significantdecrease in SDNN after liraglutide treat-ment compared with placebo (234.0619.6 vs. 20.11 6 28.4 ms; P , 0.001)(Table 2). Figure 3 visually representsthese changes in SDNN, revealing a gen-eral decrease during the liraglutide treat-ment period for all subjects. ITT analysisconfirmed this finding (coefficient232.5[95% CI 245.2 to 219.8]; P , 0.001).Mean NN was significantly reduced afterliraglutide treatment, reflecting the in-creased HR (275.5 6 89.4 vs. 8.5 677.8 bpm; P = 0.003) (Table 2). Log-trans-formed values of RMSSD, SDANN, andSDNN-index were reduced after liraglu-tide treatment (Table 2). The diurnal varia-tion curves revealed a significant decreasein RMSSD after liraglutide, mainly duringnighttime hours (Supplementary Fig. 1B).For the SDNN-index, a decrease was ob-served during both nighttime and morninghours (Supplementary Fig. 1C). In sensitivityanalyses, SDNN-index andRMSSDwere sig-nificantly reduced after liraglutide duringsleeping hours from 2:00 to 3:00 A.M.
(20.23 6 0.42 vs. 0.05 6 0.45 ms [P =0.009] and 20.25 6 0.53 vs. 0.09 60.61 ms [P = 0.045], respectively).
The significant association betweenliraglutide treatment and changes inSDNN (b = 233.9; P , 0.001) was un-changed after adjustment for mean NN(b =228.0; P, 0.001) and after furtheradjustment for other metabolic param-eters in a multivariable analysis(b = 232.3; P , 0.001), confirming theindependent reduction in SDNN by lira-glutide therapy (Table 3).
Analysis of frequency domain param-eters showed a significant reduction inlog-transformed values of LF and HFpower, which was also observed in thediurnal variation curves (SupplementaryFig. 1D and E). LF/HF ratio, LFnorm, andHFnorm did not change (Table 2); how-ever, the diurnal variation curves revealedreductions in both LFnorm and HFnorm atseveral time points (Supplementary Fig. 1Fand G). This was not evident in the diurnalcurve for the LF/HF ratio (SupplementaryFig. 1H).
For the study population, a significantweight loss (24.2 6 3.5 vs. 21.0 62.6 kg; P , 0.001) and reduction inHbA1c (20.4 6 0.3% vs. 0.04 6 0.4%;P, 0.001) was observed after liraglutidetreatment compared with placebo.Resting systolic and diastolic bloodFigure 1—Screening, enrollment, and follow-up of the study population.
care.diabetesjournals.org Kumarathurai and Associates 119
pressure, fasting blood glucose, HOMAof insulin resistance (HOMA-IR), plasmainsulin, and LDL cholesterol did notchange significantly (SupplementaryTable 1).Regression coefficients for the as-
sociation between changes in HR andSDNN and changes in selected vari-ables of interest for both interventionperiods are shown in SupplementaryTable 2. No associations among changesin blood pressure, changes in metabolicfactors, and changes in SDNN werefound during liraglutide therapy. A sig-nificant correlation between changes inRMSSD and changes in total HF powerand normalized HF power was found
(R2 = 0.77 [P , 0.001] and 0.62 [P ,0.001], respectively), during the lira-glutide period. A full list of adverseevents are provided in SupplementaryTable 3.
CONCLUSIONS
We demonstrate that 12 weeks of lira-glutide treatment induced a significantincrease in HR and reduction in long-term HRV in patients with newly diag-nosed T2D and stable CAD. We showthat the reduction in HRV was not medi-ated by the increased HR observed afterliraglutide therapy. To our knowledge,this randomized placebo-controlled
study is the first to assess the effectsof a GLP-1 RA on long-term HRV in a clin-ical setting.
The chronotropic effect of liraglutidemay be mediated through the GLP-1 re-ceptor on the sinoatrial node and influ-ence the measures of HRV. However,the multivariable regression analysis re-vealed no significant association be-tween changes in mean NN and SDNN.Furthermore, the association betweenliraglutide treatment and SDNN reduc-tionwas still significant after adjustmentfor mean NN. These findings suggestthat the impaired HRV may be due toa direct influence on sympathovagalbalance.
The time domain parameter RMSSDdecreased significantly during liraglu-tide treatment. Of note, this decreasewas mainly during nighttime hours,where vagal activity is considered domi-nant. The correlation analyses showed arelatively large R2 value for RMSSD andHF power, thus confirming the close as-sociation between these two parameters(7). A significant decrease during night-time hours was also evident for SDNN-index. Although, the normalized values ofLF and HF power did not decrease in con-trast to the absolute values, the diurnalvariation curve revealed a trend for de-crease. The less-pronounced reduction innormalized values probably reflects theconcomitant reduction in TP. The LF/HFratio, which is also considered reflectiveof sympathovagal balance, did notchange. However, LF power is subject toboth sympathetic and vagal influences,whereas the reduction in both LF andHF power may be attributable to a de-crease in mainly parasympathetic activ-ity (7). Taken together, the increase innighttime HR in conjunction with the sig-nificant decrease in SDNN and RMSSD,suggest an impairment of parasympa-thetic activity. The decrease in HF powertogether with the trend for decrease indiurnal HFnorm also suggest an impair-ment of vagal activity after liraglutidetherapy.
This hypothesis is supported by find-ings from previous studies. In a random-ized study in 30 patients with T2D,liraglutide induced an increase in HR inconjunction with an increase in the LF/HFratio during several time points of the day(21). Furthermore, in a small study ofseven patients with T2D, 24 weeks of lira-glutide treatment increasedHR, decreased
Table 1—Baseline characteristics of the study population (n = 39)
Characteristic Value
Clinical characteristicsAge (year) 61.8 (7.6)Male sex, n (%) 31 (79)Weight (kg) 96.9 (17.1)BMI (kg/m2) 31.6 (4.8)Waist (cm) 110.4 (11.2)Systolic BP (mmHg) 139.3 (19.4)Diastolic BP (mmHg) 80.2 (10.1)HR (bpm) 71.7 (12.1)
Risk factors, n (%)Smoker 14 (36)Hypertension 29 (74)CADPrevious MI 23 (59)Previous CABG 13 (33)Previous PCI 25 (64)Coronary stenosis, medical therapy only 2 (5)
BiochemistryFasting blood glucose (mmol/L) 6.5 (1.4)HbA1c (%) 6.4 (0.5)HbA1c (mmol/mol) 46.6 (5.7)LDL cholesterol (mmol/L) 2.3 (0.7)eGFR (mL/min/1.73 m2) 80.5 (11)HOMA-IR 4.02 (2.96, 7.49)Fasting insulin (pmol/L) 93 (64, 155)
Medication, n (%)b-Blockers 24 (62)Calcium antagonists 21 (54)ACE-I/ARB 26 (67)Statins 37 (95)Ivabradine 1 (3)Diuretics 11 (28)Nitrate 11 (28)Aspirin 37 (95)
Prestudy diabetes medication, n (%)Biguanide (metformin) 15 (38)Sulfonylurea 1 (3)Diet and lifestyle therapy only 24 (62)
Data are mean (SD) or median (interquartile range) unless otherwise indicated. ACE-I, ACEinhibitor; ARB, angiotensin receptor blocker; BP, blood pressure; CABG, coronary arterybypass graft; eGFR, estimated glomerular filtration rate; MI, myocardial infarction; PCI,percutaneous coronary intervention.
120 Effects of Liraglutide on Heart Rate Variability Diabetes Care Volume 40, January 2017
SDNN, and decreased LF and HF power,and the authors concluded that this maybe due to an inhibiting effect on vagal ac-tivity (22). Short-term infusion of exena-tide in overweight, healthy participantsrevealed an increase in HR and a concom-itant increase in LF/HF ratio, thus in ac-cordance with a relative increase insympathetic activity (15). Finally, an ex-perimental study in mice showed an in-hibitory effect of GLP-1 on vagal activitybecause both short- and long-term cen-tral administration of the GLP-1 RA exen-din-4 increased HR-reduced HF and LFpowers and inhibited neurotransmissionto vagal neurons (14).
Our findings regarding HR are con-sistent with previous findings fromshort-term studies that used 24-h HRmonitoring. An HR increase rangingfrom 6.5 bpm after 7weeks of liraglutidetreatment (23) and up to 9.3 bpm after8 weeks of treatment with liraglutide asan add-on to insulin glargine therapy hasbeen reported (24). However, data fromglucose-lowering trials have consis-tently reported a lower HR increase. Ameta-analysis of six phase 3 LEAD (Lira-glutide Effect and Action in Diabetes)studies reported an increase of 3.2 and3.5 bpm after 26 weeks of treatmentwith liraglutide 1.2 and 1.8mg, respectively(25). Recently, the LEADER (Liraglutide Ef-fect and Action in Diabetes: Evaluation ofCardiovascular Outcome Results) study,with a median follow-up of 3.8 years, re-ported an elevated HR of 3.0 bpm in theliraglutide group compared with the pla-cebo group (26). Longer duration of treat-ment may attenuate the HR increase, oralternatively, 24-h ambulatory HRmonitor-ing may provide a more accurate assess-ment of HR because it includes changes innocturnal HR. HR elevation has been ob-served for other GLP-1 RAs, and the in-crease in HR appears to be greater withlong-acting than with short-acting agents(27). We did not find an association be-tween changes in resting blood pressureand changes in HR during liraglutide treat-ment, confirming previous findings that HRelevation is not compensatory to a de-crease in blood pressure or systemic vaso-dilatation (25,28).Whether the HR increaseis due to augmented sympathetic activityor a direct effect on GLP-1 receptors inthe sinus atrial node remains controversial(29). The nocturnal increase in HR observedin the current study does not appear to berelated to the maximum concentration of
Table
2—Effe
ctoflira
glutid
eve
rsusplace
boonHRandHRV
parameters
Befo
reliraglu
tide(baselin
e)After
liraglutid
e(12
weeks)
Befo
replaceb
o(baselin
e)After
placeb
o(12
weeks)
n
Treatmen
teffect
Liraglutid
ePlaceb
oDifferen
ce(95%
CI)
Pvalu
e
HRparam
eter(bpm)
Mean
HR
74.03(12.09)
80.93(10.61)
75.93(11.10)
74.71(9.52)
276.90
(8.64)21.22
(7.15)8.11
(3.05to
13.18)0.003
Minim
um
HR
48.48(8.05)
55.52(8.55)
50.81(7.85)
50.11(7.92)
277.04
(5.89)20.70
(5.17)7.74
(4.28to
11.20),0.001
Maxim
um
HR
126.00(19.40)
129.19(17.91)
129.56(18.91)
126.41(20.38)
273.19
(13.38)23.15
(11.22)6.33
(20.22
to12.88)
0.058Daytim
eHR
77.08(12.80)
83.34(11.29)
78.02(12.04)
78.61(10.65)
266.26
(9.76)0.60
(10.96)5.66
(20.79
to12.11)
0.083Nigh
ttimeHR
70.19(11.70)
77.45(10.21)
70.11(10.30)
71.04(9.09)
267.26
(8.58)0.93
(7.61)6.34
(0.81to
11.86)0.026
24-htim
edomain
Mean
NN(m
s)837.34
(143.64)761.81
(107.17)805.88
(123.80)814.35
(109.85)27
275.52
(89.36)8.47
(77.83)283.99
(2137.01
to230.98)
0.003SD
NN(m
s)129.63
(30.54)95.59
(27.04)125.48
(35.50)125.37
(32.00)27
234.04
(19.61)20.11
(28.38)233.93
(247.76
to220.09)
,0.001
SDNN-in
dex
(log-m
s)3.84
(0.35)3.57
(0.40)3.76
(0.39)3.74
(0.36)27
20.27
(0.28)20.02
(0.24)20.25
(20.41
to20.09)
0.003SD
ANN(lo
g-ms)
3.18(0.35)
2.85(0.38)
3.09(0.39)
3.06(0.34)
2720.33
(0.27)20.04
(0.25)20.29
(20.46
to20.12)
0.002RMSSD
(log-m
s)3.52
(0.62)3.26
(0.69)3.40
(0.63)3.46
(0.68)27
20.26
(0.49)0.06
(0.40)20.32
(20.60
to20.04)
0.025
Frequen
cydomain
LogLF
(log-m
s2)
5.33(0.65)
4.81(0.77)
5.17(0.81)
5.13(0.74)
2620.52
(0.57)20.04
(0.64)20.47
(20.90
to20.05)
0.029LogHF(lo
g-ms2)
4.46(0.85)
3.93(1.06)
4.21(0.92)
4.36(1.02)
2620.53
(0.87)0.15
(0.89)20.67
(21.26
to20.09)
0.026LogTP
(log-m
s2)
7.61(0.40)
7.30(0.37)
7.51(0.38)
7.51(0.35)
2620.31
(0.31)20.001
(0.272)20.31
(20.49
to20.12)
0.002LogLF/H
F0.87
(0.59)0.88
(0.70)0.96
(0.56)0.77
(0.64)26
0.01(0.55)
20.19
(0.48)0.20
(20.11
to0.51)
0.201LogLFn
orm
22.28
(0.43)22.49
(0.52)22.34
(0.56)22.38
(0.49)26
20.21
(0.33)20.04
(0.43)20.17
(20.43
to0.10)
0.200LogHFnorm
23.15
(0.73)23.37
(0.81)23.30
(0.72)23.15
(0.76)26
20.22
(0.70)0.15
(0.72)20.37
(20.84
to0.10)
0.122
Data
aremean
(SD)unless
otherw
iseindicated
.nisthenumber
ofsubjects
foreach
treatmen
tphase
with
complete
measu
remen
tsforallvisits.
Daytim
e,7:00A.M.–10:00
P.M.;nigh
ttime,11:00
P.M
.–6:00A.M
.
care.diabetesjournals.org Kumarathurai and Associates 121
liraglutide reported to be reached after 8–12 h (30). In the studies byMeier et al. (24)and Nakatani et al. (21), the injection ofliraglutidewas in themorningbeforebreak-fast. In both studies, a persistent increase inHR during the nighttime beyond the peakconcentration for liraglutide was observed.In previous studies, weight loss and
improvement in metabolic parameters
have been associated with an improve-ment in HRV, such as in obese patientsafter weight-reducing gastric surgery(31), patients with and without diabetesafter an energy-restricted diet (32,33),and patients with T2D after inten-sive multifactorial intervention (13). Incontrast, we observed a deteriorationin HRV measures despite significant
weight loss and reduction in HbA1c afterliraglutide treatment. Hyperglycemiaand hyperinsulinemia have been sug-gested as aggravating factors for HRV(34,35), but we did not see significantchanges in these metabolic parametersduring liraglutide treatment. Our linearregression analysis revealed that the re-duction in SDNN was unaffected bychanges in weight, HbA1c, HOMA-IR, in-sulin, and fasting glucose. These findingssuggest that liraglutide may have an ef-fect on the autonomic nervous systemthat is not mediated by an improvementin metabolic parameters.
Although increased HR and decreasedHRV have been associated with poorprognosis in terms of cardiovascularmortality in several studies (5,6,36),beneficial effects of GLP-1 RA therapyin terms of weight loss, improvementin metabolic parameters, and other posi-tive effects on the cardiovascular systemare important to note (29). Accordingly,the LEADER study demonstrated a signif-icant reduction in cardiovascular mor-tality after liraglutide therapy (26,37).However, an unexpected trend towardadverse outcomes after liraglutide therapywas reported in a subgroupof subjectswithheart failure and diabetes in a recent ran-domized study (38). Because both diabetesand heart failure are associated with re-duced HRV (5), whether liraglutide in-duces an additional aggravating effecton autonomic function in patients withboth of these conditions and whether itaffects cardiovascular outcome need tobe explored.
Potential limitations in this studyshould be considered. The Holter mon-itoring was not performed under con-trolled conditions in a laboratory; thus,environmental and behavioral factorsmay have influenced the results. How-ever, because of the randomized cross-over design, such factors would beexpected to affect the recordings inboth periods to a similar degree. Fur-thermore, we performed sensitivityanalyses during the nighttime, whereinfluences of external factors are lim-ited. Frequency domain analyses shouldbe interpreted with caution when ob-tained from long-term recordings dueto lower stability of HR. Thus, time do-main measures are considered ideal un-der these conditions (7). Nevertheless,the reporting of both these measuresis a major strength of this study and
Figure 3—SDNN changes during treatment periods. Gray lines represent SDNN values for eachpatient. Bold lines represent change in mean SDNN in placebo and liraglutide period. Error barsindicate mean 6 SE.
Figure 2—Diurnal variation in hourly mean HR. Error bars indicate mean 6 SE.
122 Effects of Liraglutide on Heart Rate Variability Diabetes Care Volume 40, January 2017

provides a more thorough assessmentof the influence of GLP-1 RA treatmenton sympathovagal balance. The con-founding effects of background medica-tion are considered minimal because aneffort wasmade to not change themed-ication during the study. However, theuse of HR-limiting medications, such asb-blockers and ivabradine, may have at-tenuated the chronotropic effect of liraglu-tideand influenced theHRVmeasurements.Sensitivity analyses based on HR-limitingmedications were not performed becauseof a small and unequal distribution of pa-tients in these subgroups. The gastrointesti-nal adverse effects or hypoglycemia due toliraglutide therapy may have influenced theHRV measurements. However, the studydrug was uptitrated to a maximum doseafter 4 weeks, and because Holter monitor-ingwasperformedat12weeks, themajorityof adverse effects are expected to be re-duced. Furthermore, no severe hypoglyce-mic events were observed during thestudy. Nevertheless, any treatment-related temporary or persistent adverseeffects that may influence HRV may beclinically important. Because of the ho-mogeneity of the cohort, we cannot ex-trapolate the results to other patientgroups, such as those with long-standingand poorly controlled diabetes or thosewith severe CAD or heart failure. Theeffect on HRV beyond 12weeks of treat-ment was not assessed, although wecannot exclude the possibility thatHRV changes may attenuate over time.Thus, the effect of GLP-1 RA treatmenton HRV needs to be explored in otherpatient groups and with a longer treat-ment duration.In conclusion, liraglutide increased
HR and reduced HRV in overweightpatients with newly diagnosed T2Dand stable CAD despite significantweight loss and improvement in glu-cometabolic parameters. Liraglutideinduced changes in time and frequency
domain parameters of HRV, whichsuggests an effect on sympathovagalbalance.
Acknowledgments. The AddHope2 investiga-tors thank the patients who participated in thisstudy.Funding. This study was supported by NovoNordisk with an unrestricted grant for investi-gator-initiated studies. Additional funding wasprovided by the Danish Heart Foundation; TheAPMøller Foundation; the Department of Inter-nal Medicine, Amager Hospital; the ClinicalResearch Centre, Hvidovre Hospital; and theBispebjerg Hospital Research Foundation.Duality of Interest. During the past 3 years,S.M. has participated on advisory boards forNovartis, Novo Nordisk, Merck Sharp & Dohme,Sanofi, AstraZeneca, Johnson & Johnson, Roche,HumanKind, Boehringer Ingelheim, ZealandPharma, Eli Lilly, and Intarcia Therapeutics andhas received honoraria for lectures from NovoNordisk, Merck Sharp & Dohme, AstraZeneca,Johnson & Johnson, Roche, Schering-Plough,Sanofi, Novartis, Eli Lilly, and Bristol-MyersSquibb. O.W.N. has received funding of educa-tional and research tasks from ResMed and par-ticipated on advisory boards for Novartis. S.B.H.has received funding of educational and re-search tasks from Novo Nordisk, Abbott, Eli Lilly,Pfizer, Boehringer Ingelheim, Bristol-MyersSquibb, and Merck Sharp & Dohme. No otherpotential conflicts of interest relevant to thisarticle were reported.Author Contributions. P.K. acquired data,performed the statistical analyses, interpreteddata, and drafted and revised themanuscript forimportant intellectual content and approvedthe final version. C.A. and B.S.L. acquired data,interpreted data, and revised the manuscriptfor important intellectual content andapprovedthe final version. R.H.O., S.M., O.K., and O.W.N.interpreted data and revised themanuscript forimportant intellectual content and approvedthefinal version. S.B.H. conceived anddesigned thestudy, interpreted data, and revised the manu-script for important intellectual content andapproved the final version. A.S. conceived anddesigned the study, interpreted data, contrib-uted to the statistical analyses, and revised themanuscript for important intellectual contentand approved the final version. P.K. is theguarantor of this work and, as such, had fullaccess to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.
Prior Presentation. Parts of this study werepresented as a poster at the European Soci-ety of Cardiology Congress, Rome, Italy, 27–31August 2016.
References1. Dekker JM, Crow RS, Folsom AR, et al. Lowheart rate variability in a 2-minute rhythm strippredicts risk of coronary heart disease and mor-tality from several causes: the ARIC study. Ath-erosclerosis Risk in Communities. Circulation2000;102:1239–12442. Algra A, Tijssen JG, Roelandt JR, Pool J,Lubsen J. Heart rate variability from 24-hourelectrocardiography and the 2-year risk for sud-den death. Circulation 1993;88:180–1853. Floras JS, Ponikowski P. The sympathetic/parasympathetic imbalance in heart failure withreduced ejection fraction. Eur Heart J 2015;36:1974–1982b4. Vinik AI, Maser RE, Mitchell BD, Freeman R.Diabetic autonomic neuropathy. Diabetes Care2003;26:1553–15795. Vinik AI, Ziegler D. Diabetic cardiovascularautonomic neuropathy. Circulation 2007;115:387–3976. Hillis GS, Woodward M, Rodgers A, et al.Resting heart rate and the risk of death andcardiovascular complications in patients withtype 2 diabetes mellitus. Diabetologia 2012;55:1283–12907. Task Force of the European Society of Cardi-ology; North American Society of Pacing and Elec-trophysiology. Heart rate variability. Standards ofmeasurement, physiological interpretation, andclinical use. Eur Heart J 1996;17:354–3818. Stein PK, Bosner MS, Kleiger RE, Conger BM.Heart rate variability: a measure of cardiac au-tonomic tone. Am Heart J 1994;127:1376–13819. Makimattila S, Schlenzka A, Mantysaari M,et al. Predictors of abnormal cardiovascular au-tonomic function measured by frequency do-main analysis of heart rate variability andconventional tests in patients with type 1 dia-betes. Diabetes Care 2000;23:1686–169310. Bigger JT, Fleiss JL, Rolnitzky LM, SteinmanRC. Frequency domainmeasures of heart periodvariability to assess risk late after myocardialinfarction. J Am Coll Cardiol 1993;21:729–73611. Makikallio TH, Huikuri HV, Hintze U, et al.;DIAMOND Study Group (Danish Investigationsof Arrhythmia andMortality on Dofetilide). Frac-tal analysis and time- and frequency-domain mea-sures of heart rate variability as predictors ofmortality in patientswith heart failure. Am J Cardiol2001;87:178–18212. Meier JJ. GLP-1 receptor agonists for indi-vidualized treatment of type 2 diabetes melli-tus. Nat Rev Endocrinol 2012;8:728–74213. Gaede P, Vedel P, Parving H-H, Pedersen O.Intensified multifactorial intervention in pa-tients with type 2 diabetes mellitus and micro-albuminuria: the Steno type 2 randomisedstudy. Lancet 1999;353:617–62214. Griffioen KJ, Wan R, Okun E, et al. GLP-1receptor stimulation depresses heart rate vari-ability and inhibits neurotransmission to cardiacvagal neurons. Cardiovasc Res 2011;89:72–7815. Bharucha AE, Charkoudian N, Andrews CN,et al. Effects of glucagon-like peptide-1, yohim-bine, and nitrergic modulation on sympatheticand parasympathetic activity in humans. Am J
Table 3—Linear regression models showing the association between liraglutidetreatment and changes in SDNN
Liraglutide treatment b-Coefficient 95% CI P value
Univariable analysis 233.9 247.2 to 220.6 ,0.001
Adjusted for changes in mean NN 228.0 242.9 to 213.1 ,0.001
Multivariable analysis† 232.3 249.5 to 215.0 ,0.001
†Multivariable linear regression analysis with adjustment for changes in mean NN, weight,HbA1c, systolic blood pressure, HOMA-IR, and insulin; dependent variable, changes in SDNN;independent variable, treatment (liraglutide).
care.diabetesjournals.org Kumarathurai and Associates 123

Physiol Regul Integr Comp Physiol 2008;295:R874–R88016. Berkelaar M, Eekhoff EMW, Simonis-BikAMC, et al. Effects of induced hyperinsulinae-mia with and without hyperglycaemia on mea-sures of cardiac vagal control. Diabetologia2013;56:1436–144317. Smilowitz NR, Donnino R, Schwartzbard A.Glucagon-like peptide-1 receptor agonists fordiabetes mellitus: a role in cardiovascular dis-ease. Circulation 2014;129:2305–231218. Anholm C, Kumarathurai P, Klit MS, et al.;AddHope2 Trial Study Group. Adding liraglutideto the backbone therapy of biguanide in pa-tients with coronary artery disease and newlydiagnosed type-2 diabetes (the AddHope2study): a randomised controlled study protocol.BMJ Open 2014;4:e00594219. Altman DG. Practical Statistics for MedicalResearch. Boca Raton, FL, CRC Press, 1991, p.136–14620. Shapiro SS,Wilk MB. An analysis of variancetest for normality (complete samples). Biome-trika 1965;52:591–61121. Nakatani Y, Kawabe A, Matsumura M, et al. Ef-fects of GLP-1 receptor agonists on heart rate andthe autonomic nervous system using Holter electro-cardiography and power spectrum analysis of heartrate variability. Diabetes Care 2016;39:e22–e2322. Hara K, Aso Y, Komatsu T, et al. Liraglutideincreases 24-h heart rate by reducing the car-diac parasympathetic activity of patients withtype 2 diabetes: power spectral analysis of heartrate variability on 24-h Holter ECG recordings.Diabetol Int 2015;6:26–3223. von Scholten BJ, LajerM, Goetze JP, PerssonF, Rossing P. Time course and mechanisms ofthe anti-hypertensive and renal effects of liraglu-tide treatment. Diabet Med 2015;32:343–352
24. Meier JJ, Rosenstock J, Hincelin-Mery A,et al. Contrasting effects of lixisenatide and lir-aglutide on postprandial glycemic control, gas-tric emptying, and safety parameters in patientswith type 2 diabetes on optimized insulin glar-gine with or without metformin: a randomized,open-label trial. Diabetes Care 2015;38:1263–127325. Fonseca VA, Devries JH, Henry RR,Donsmark M, Thomsen HF, Plutzky J. Reduc-tions in systolic blood pressure with liraglutidein patients with type 2 diabetes: insights from apatient-level pooled analysis of six randomizedclinical trials. J Diabetes Complications 2014;28:399–40526. Marso SP, Daniels GH, Brown-Frandsen K,et al.; LEADER Steering Committee; LEADER TrialInvestigators. Liraglutide and cardiovascularoutcomes in type 2 diabetes. N Engl J Med2016;375:311–32227. Robinson LE, Holt TA, Rees K, Randeva HS,O’Hare JP. Effects of exenatide and liraglutideon heart rate, blood pressure and body weight:systematic review andmeta-analysis. BMJ Open2013;3:e00198628. Smits MM, Muskiet MHA, Tonneijck L, et al.Exenatide acutely increases heart rate in paral-lel with augmented sympathetic nervous sys-tem activation in healthy overweight males.Br J Clin Pharmacol 2016;81:612-62029. Ussher JR, Drucker DJ. Cardiovascular ac-tions of incretin-based therapies. Circ Res 2014;114:1788–180330. Novo Nordisk. Victoza: EMA product infor-mation [Internet], 2014. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001026/WC500050017.pdf. Accessed 3 February2016
31. Karason K, Mølgaard H, Wikstrand J,Sjostrom L. Heart rate variability in obesityand the effect of weight loss. Am J Cardiol1999;83:1242–124732. Akehi Y, Yoshimatsu H, Kurokawa M, et al.VLCD-induced weight loss improves heart ratevariability in moderately obese Japanese. ExpBiol Med (Maywood) 2001;226:440–44533. Sjoberg N, Brinkworth GD, Wycherley TP,Noakes M, Saint DA. Moderate weight loss im-proves heart rate variability in overweight andobese adults with type 2 diabetes. J Appl Physiol(1985) 2011;110:1060–106434. Schroeder EB, Chambless LE, Liao D, et al.;Atherosclerosis Risk in Communities (ARIC)Study. Diabetes, glucose, insulin, and heartrate variability: the Atherosclerosis Risk in Com-munities (ARIC) study. Diabetes Care 2005;28:668–67435. Valensi P, Chiheb S, Fysekidis M. Insulin-and glucagon-like peptide-1-induced changesin heart rate and vagosympathetic activity: whythey matter. Diabetologia 2013;56:1196–120036. Anselmino M, Ohrvik J, Ryden L; Euro HeartSurvey Investigators. Resting heart rate in pa-tients with stable coronary artery disease anddiabetes: a report from the Euro Heart Surveyon Diabetes and the Heart. Eur Heart J 2010;31:3040–304537. Pfeffer MA, Claggett B, Diaz R, et al.; ELIXAInvestigators. Lixisenatide in patients withtype 2 diabetes and acute coronary syndrome.N Engl J Med 2015;373:2247–225738. Margulies KB, Hernandez AF, Redfield MM,et al.; NHLBI Heart Failure Clinical Research Net-work. Effects of liraglutide on clinical stabilityamong patients with advanced heart failureand reduced ejection fraction: a randomizedclinical trial. JAMA 2016;316:500–508
124 Effects of Liraglutide on Heart Rate Variability Diabetes Care Volume 40, January 2017