eating disorders review lecture, 2015 dr. leanna isserlin, md, frcpc assistant professor university...
TRANSCRIPT
EATINGEATING DISORDERSDISORDERSReview Lecture, 2015Review Lecture, 2015
Dr. Leanna Isserlin, MD, FRCPCDr. Leanna Isserlin, MD, FRCPCAssistant ProfessorAssistant ProfessorUniversity of OttawaUniversity of [email protected]@cheo.on.ca

Eating Disorders Eating Disorders OverviewOverview
• DiagnosisDiagnosis
• EpidemiologyEpidemiology
• Understanding Eating DisordersUnderstanding Eating Disorders– Etiology, Risk Factors, and PowerEtiology, Risk Factors, and Power
• Medical ComplicationsMedical Complications
• Principles of TreatmentPrinciples of Treatment
• OutcomeOutcome

Types of Eating Types of Eating DisordersDisorders1.1. Anorexia NervosaAnorexia Nervosa
– Restricting TypeRestricting Type– Binge-eating/Purging subtypeBinge-eating/Purging subtype
2.2. Bulimia Nervosa Bulimia Nervosa
3.3. Binge Eating DisorderBinge Eating Disorder
4.4. Other Specified Feeding or Eating DisorderOther Specified Feeding or Eating Disorder
5.5. Unspecified Eating DisorderUnspecified Eating Disorder

Types Types ofof Eating Eating DisordersDisorders6. Pica6. Pica
7. Rumination Disorder7. Rumination Disorder
8. ARFID – NEW!8. ARFID – NEW!
Definitions: Anorexia Definitions: Anorexia NervosaNervosa
A. Restriction leading to A. Restriction leading to Significantly Low Body weight Significantly Low Body weight
for age, sex, dev traj, healthfor age, sex, dev traj, health
B. B. Intense fearIntense fear of gaining weight of gaining weight or or behavior interferes with wt behavior interferes with wt gaingain
C. C. Distorted body imageDistorted body image - or Undue - or Undue influence of influence of weight on self-worth, weight on self-worth, - or Denial of seriousness of - or Denial of seriousness of the low weightthe low weight
Anorexia Nervosa cont’dAnorexia Nervosa cont’d• Specify (in last 3 months)Specify (in last 3 months)::
– Restricting Type Restricting Type – Binge-Eating / Purging TypeBinge-Eating / Purging Type
• SeveritySeverity(adults)(adults): BMI: BMI– Mild Mild ≥17≥17– ModerateModerate ≥16≥16– SevereSevere ≥15≥15– ExtremeExtreme <15<15
Purging - Vomiting- Laxatives- Diuretics- Enemas

Common Symptoms of A.N.:Common Symptoms of A.N.:
• Restricting intakeRestricting intake
• ExercisingExercising
• Standing, moving, restlessnessStanding, moving, restlessness
• Weighing excessivelyWeighing excessively
• Label reading/cal countingLabel reading/cal counting
• Wanting to prepare own foodsWanting to prepare own foods
• Self-induced vomitingSelf-induced vomiting
• Diet pills, laxativesDiet pills, laxatives

Bulimia NervosaBulimia NervosaA. A. Recurrent Recurrent Binge EatingBinge Eating::
1.1. Eating a very large amount Eating a very large amount of food in a discrete period of food in a discrete period of timeof time
2. 2. Lack of controlLack of control during the during the episodeepisode
B.B. Recurrent Recurrent CompensatoryCompensatory behaviorbehavior
to prevent weight gain to prevent weight gain (vomiting, laxatives, fasting, (vomiting, laxatives, fasting,
over-exercising…)over-exercising…)
Bulimia NervosaBulimia Nervosa
C.C. A.A. and and B.B. occur at least: occur at least:• 1x / week for 3 months1x / week for 3 months
D.D. Self-worthSelf-worth unduly influenced by unduly influenced by shape and weightshape and weight
E.E. Not A.N.Not A.N.
Bulimia NervosaBulimia Nervosa
• Specify severity:Specify severity:– Mild – 1-3 compensatory Mild – 1-3 compensatory
behaviours/weekbehaviours/week– Moderate – 4-7 comp behaviours/weekModerate – 4-7 comp behaviours/week– Severe – 8-13 comp behaviours/weekSevere – 8-13 comp behaviours/week– Extreme – 14+ comp behaviours/weekExtreme – 14+ comp behaviours/week

The Bulimic CycleThe Bulimic Cycle• A binge is almost A binge is almost
always the result of always the result of dieting and food dieting and food restriction.restriction.
• Purging is the result of:Purging is the result of:
– Fear of weight gainFear of weight gain
– The perception of The perception of stomach discomfortstomach discomfort
– Shame caused by the Shame caused by the loss of control over loss of control over eatingeating
RestrictRestrict
BingeBinge
CompComp
behaviourbehaviour
Binge Eating DisorderBinge Eating Disorder1.1.BingesBinges 1X / week , 3 months1X / week , 3 months
2.2.Binges associated with 3 or more of Binges associated with 3 or more of • Eating – rapidlyEating – rapidly
- until uncomfortably full- until uncomfortably full
- large amounts when not hungry,- large amounts when not hungry,
- alone - alone
• Feeling disgusted /depressed /guilty Feeling disgusted /depressed /guilty afterwardsafterwards
3.3.No compensatory behaviourNo compensatory behaviour
Binge Eating DisorderBinge Eating Disorder
• Specify severity:Specify severity:– Mild – 1-3 binges/weekMild – 1-3 binges/week– Moderate – 4-7 binges/weekModerate – 4-7 binges/week– Severe – 8-13 binges/weekSevere – 8-13 binges/week– Extreme – 14+ binges/weekExtreme – 14+ binges/week

Other Specified Feeding Other Specified Feeding or Eating Disorder or Eating Disorder
Patient does not meet all the criteria Patient does not meet all the criteria for an eating disorder. For example:for an eating disorder. For example:
- Atypical AN- Atypical AN- Partial BNPartial BN- Partial BEDPartial BED- Purging DisorderPurging Disorder- Night Eating Syndrome Night Eating Syndrome
Unspecified Feeding or Unspecified Feeding or Eating Disorder Eating Disorder
• Insufficient information to define Insufficient information to define specific type of eating/feeding specific type of eating/feeding disorderdisorder
PicaPica
• Persistent eating of non-nutritive, Persistent eating of non-nutritive, nonfood substances x1monthnonfood substances x1month
• Not normal for dev levelNot normal for dev level
• Not culturally sanctioned practiceNot culturally sanctioned practice
• Out of proportion if occurs in another Out of proportion if occurs in another mental disordermental disorder
Rumination DisorderRumination Disorder
• Repeated regurgitation of food Repeated regurgitation of food x1monthx1month
• Not due to medical disorderNot due to medical disorder
• Not exclusive to another Not exclusive to another eating/feeding disordereating/feeding disorder
• Out of proportion in occurs with Out of proportion in occurs with another mental disorderanother mental disorder
Avoidant/Restrictive Avoidant/Restrictive Food Intake Disorder Food Intake Disorder (ARFID)(ARFID)• Persistent failure to meet nutritional Persistent failure to meet nutritional
needs evidenced by:needs evidenced by:– Wt LossWt Loss– Nutritional deficiencyNutritional deficiency– Dependence on enteral feeding or oral suppDependence on enteral feeding or oral supp– Interference with functioningInterference with functioning
• Not due to lack of food available or cultureNot due to lack of food available or culture
• Not due to AN/BN or medical d/oNot due to AN/BN or medical d/o

Avoidant/Restrictive Avoidant/Restrictive Food Intake Disorder Food Intake Disorder (ARFID)(ARFID)• Lack of interest in food (poor Lack of interest in food (poor
appetite)appetite)
• Sensory disordersSensory disorders
• Aversive consequences of eating Aversive consequences of eating (vomiting/illness)(vomiting/illness)
Avoidant/Restrictive Avoidant/Restrictive Food Intake Disorder Food Intake Disorder (ARFID)(ARFID)• High comorbidity, severity must High comorbidity, severity must
exceed that routinely seen in other exceed that routinely seen in other disorders:disorders:– Anxiety DisordersAnxiety Disorders– ASDASD– OCDOCD– ADHDADHD
Eating Disorders Eating Disorders OverviewOverview
• DiagnosisDiagnosis
• EpidemiologyEpidemiology
• Understanding Eating DisordersUnderstanding Eating Disorders– Etiology, Risk Factors, and PowerEtiology, Risk Factors, and Power
• Medical ComplicationsMedical Complications
• Principles of TreatmentPrinciples of Treatment
• OutcomeOutcome
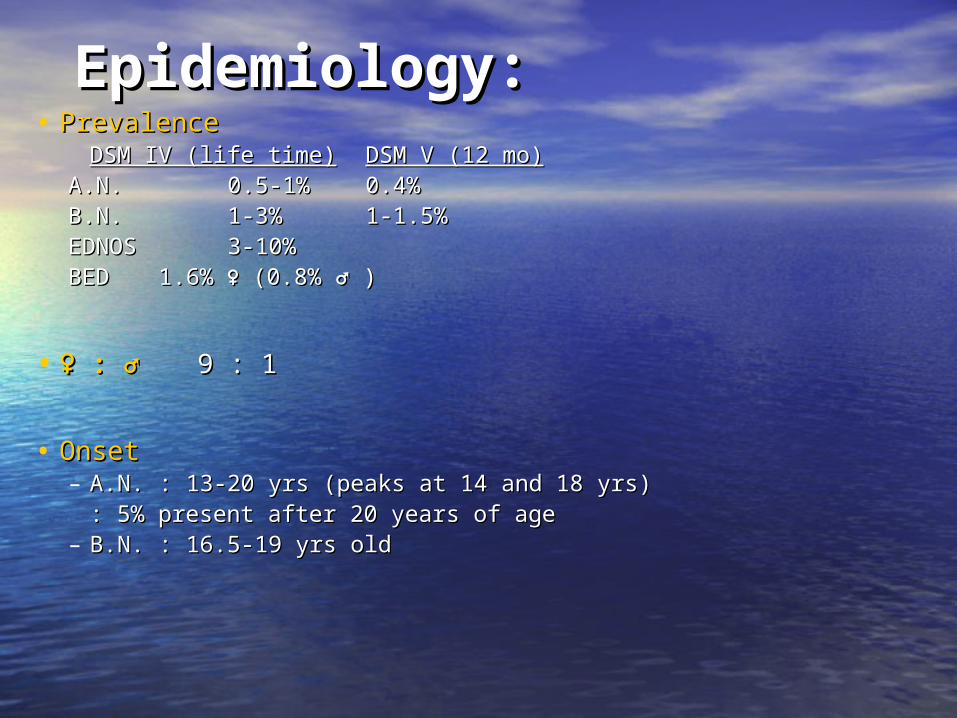
Epidemiology:Epidemiology:• PrevalencePrevalence
DSM IV (life time)DSM IV (life time) DSM V (12 mo)DSM V (12 mo)A.N.A.N. 0.5-1%0.5-1% 0.4%0.4% B.N.B.N. 1-3% 1-3% 1-1.5%1-1.5%EDNOS EDNOS 3-10%3-10%BEDBED 1.6%1.6% ♀ ♀ (0.8%(0.8% ♂♂ ) )
• ♀♀ : ♂: ♂ 9 : 19 : 1
• OnsetOnset– A.N.A.N. : 13-20 yrs (peaks at 14 and 18 yrs): 13-20 yrs (peaks at 14 and 18 yrs)
: 5% present after 20 years of age: 5% present after 20 years of age– B.N.B.N. : 16.5-19 yrs old: 16.5-19 yrs old

Eating Disorders Eating Disorders OverviewOverview
• DiagnosisDiagnosis
• EpidemiologyEpidemiology
• Understanding Eating DisordersUnderstanding Eating Disorders– Etiology, Risk Factors, and PowerEtiology, Risk Factors, and Power
• Medical ComplicationsMedical Complications
• Principles of TreatmentPrinciples of Treatment
• OutcomeOutcome
Understanding Eating Understanding Eating DisordersDisorders
• Up to 90% of teenage girls will go on Up to 90% of teenage girls will go on a diet. What happens to the 5%, a diet. What happens to the 5%, (and the boys), that go on to develop (and the boys), that go on to develop Eating Disorders?Eating Disorders?

The Development of an EDThe Development of an ED
Vulnerable Youth-Risk factors-Comorbidities-Low self-esteem/”not good enough”
Stressors
Need to create order / Feel Better
Dieting
Sense of Achievement (feel “good enough”)
Increased Dieting
Snowballing of behaviours
Eating Disorder

Risk Factors for ANRisk Factors for ANCulturalCultural FamilyFamily IndividualIndividualIdealization of Idealization of thinness, thinness, “normative “normative discontent” for discontent” for female body imagefemale body image
Family History of Family History of ED / Anxiety / Mood ED / Anxiety / Mood disorder / OCPDdisorder / OCPD
Female GenderFemale Gender
Gay malesGay males Early life Early life “overprotective / “overprotective / high concern high concern parenting”parenting”
Perfectionism / Perfectionism / ObsessionalityObsessionality
Activity where Activity where thinness = success thinness = success e.g. modeling / e.g. modeling / actingacting
Low self-esteem / Low self-esteem / Sense of Sense of ineffectivenessineffectiveness
Competitive sports Competitive sports with emphasis on with emphasis on thinness: e.g.. thinness: e.g.. gymnastics / balletgymnastics / ballet
Eagerness to please Eagerness to please / High sensitivity/ High sensitivity
PubertyPuberty

Risk Factors for BNRisk Factors for BN
CulturalCultural FamilyFamily IndividualIndividualIdealization of Idealization of thinnessthinness
Family Hx of Family Hx of obesityobesity
FemaleFemale
Specific sports / Specific sports / activities as ANactivities as AN
Family Hx of Mood Family Hx of Mood /Anxiety / ED / or /Anxiety / ED / or Substance Abuse / Substance Abuse / Cluster B PDCluster B PD
Low self-esteem / Low self-esteem / Sense of Sense of ineffectivenessineffectiveness
Critical comments Critical comments re. weight / re. weight / shape / eatingshape / eating
Hx of sexual Hx of sexual abuseabuse
Volatile / Volatile / conflicted family conflicted family environmentsenvironments

Culture of DietingCulture of Dieting
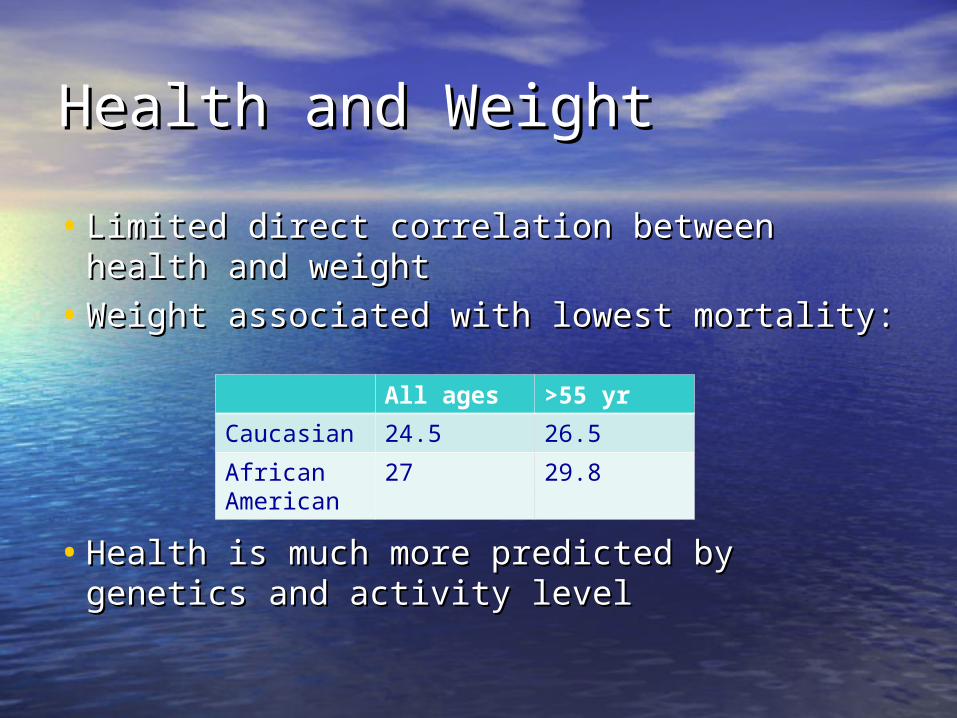
Health and WeightHealth and Weight
• Limited direct correlation between health Limited direct correlation between health and weightand weight
• Weight associated with lowest mortality:Weight associated with lowest mortality:
• Health is much more predicted by Health is much more predicted by genetics and activity levelgenetics and activity level
All ages >55 yr
Caucasian 24.5 26.5
African American
27 29.8
Co-Morbidity of A.N.:Co-Morbidity of A.N.:
• >50% Depression (i.e. #1 comorbidity)>50% Depression (i.e. #1 comorbidity)
• 50% Anxiety Disorders (esp. OCD, 50% Anxiety Disorders (esp. OCD, GAD, and Social Phobia)GAD, and Social Phobia)
• PerfectionismPerfectionism
• ““Cluster ‘C’ P.D. traits, e.g.. OCPD Cluster ‘C’ P.D. traits, e.g.. OCPD (rigidity, restraint, obsessiveness)(rigidity, restraint, obsessiveness)

Comorbidity of B.N.:Comorbidity of B.N.:
• Depression >50%, #1 comorbidity Depression >50%, #1 comorbidity
• Anxiety in >50% (esp. GAD and Social Anxiety in >50% (esp. GAD and Social Phobia)Phobia)
• Impulsivity/risk-taking behaviorsImpulsivity/risk-taking behaviors
• Substance AbuseSubstance Abuse
• Borderline Personality Disorder traitsBorderline Personality Disorder traits
• PTSDPTSD
• Bipolar Spectrum disordersBipolar Spectrum disorders

E.D. SpectrumE.D. Spectrum• A.N.-------------A.N./B-P--------------B.N.A.N.-------------A.N./B-P--------------B.N.
• Perfectionistic ChaoticPerfectionistic Chaotic
• Compliant Unstable Compliant Unstable moodsmoods
• Anxious Substance Anxious Substance abuseabuse
• Sensitive ImpulsiveSensitive Impulsive
• Possible OCPD Possible BPDPossible OCPD Possible BPD

What makes What makes
an Eating an Eating
Disorders soDisorders so
Powerful?Powerful?
Why so powerful? Why so powerful? Understanding the Eating Understanding the Eating DisorderDisorder
• Effects of starvationEffects of starvation
• Meaning of the IllnessMeaning of the Illness
• Experience of Eating DisorderExperience of Eating Disorder
• Poor InsightPoor Insight
Effects of StarvationEffects of Starvation
• Ancel Keys, University of Minnesota, Ancel Keys, University of Minnesota, during WWIIduring WWII
• Psychologically “Normal” men, with Psychologically “Normal” men, with superior “psychobiological stamina”superior “psychobiological stamina”
Semi-starvation Semi-starvation
(lost 25% body weight)(lost 25% body weight)

Effects of StarvationEffects of Starvation
• Change of Eating HabitsChange of Eating Habits– Started to eat in silence, prolonged time, Started to eat in silence, prolonged time,
unusual mixing of foodunusual mixing of food
• Social ChangesSocial Changes– Men became withdrawn, decrease wish to Men became withdrawn, decrease wish to
socializesocialize– Less humourLess humour
• Cognitive ChangesCognitive Changes– Impaired concentrationImpaired concentration– Impaired comprehension and judgmentImpaired comprehension and judgment

Effects of StarvationEffects of Starvation
• Emotional ChangesEmotional Changes– Depression,Depression,– Irritability,Irritability,– Frequent outbursts of anger,Frequent outbursts of anger,– Extreme mood swings,Extreme mood swings,– High levels of anxiety (including nail biting), High levels of anxiety (including nail biting), – Almost 20% experienced extreme emotional Almost 20% experienced extreme emotional
deterioration (some hospitalized), deterioration (some hospitalized),
– Most changes persisted through refeeding, Most changes persisted through refeeding, became worse for somebecame worse for some
The Meaning of the Eating The Meaning of the Eating DisorderDisorder
• The Eating Disorder is “one thing I am The Eating Disorder is “one thing I am good at”good at”
• Not eating allows me “to feel in control of Not eating allows me “to feel in control of my life” my life”
• Not eating allows “all my other worries to Not eating allows “all my other worries to go away”go away”
• The Eating Disorder “makes me feel The Eating Disorder “makes me feel powerful, special and in control”powerful, special and in control”
• The Eating Disorder means “I don’t have to The Eating Disorder means “I don’t have to grow up”grow up”
• Eating means “I am weak and a failure”Eating means “I am weak and a failure”• The Eating disorder is “who I am”The Eating disorder is “who I am”
Experience of an EDExperience of an ED
• Follow the rulesFollow the rules– Relief of anxiety, empowered, strong, Relief of anxiety, empowered, strong,
focusedfocused
• Do not follow the rulesDo not follow the rules– Tortured by Eating Disorder voiceTortured by Eating Disorder voice– Shame / guilt and high anxietyShame / guilt and high anxiety
Poor Insight and DenialPoor Insight and Denial


Eating Disorders Eating Disorders OverviewOverview
• DiagnosisDiagnosis
• EpidemiologyEpidemiology
• Understanding Eating DisordersUnderstanding Eating Disorders– Etiology, Risk Factors, and PowerEtiology, Risk Factors, and Power
• Medical ComplicationsMedical Complications
• Principles of TreatmentPrinciples of Treatment
• OutcomeOutcome

Medical Complications of Medical Complications of Eating DisordersEating Disorders
• StarvationStarvation– Body shutting down one system at a Body shutting down one system at a
timetime
• PurgingPurging
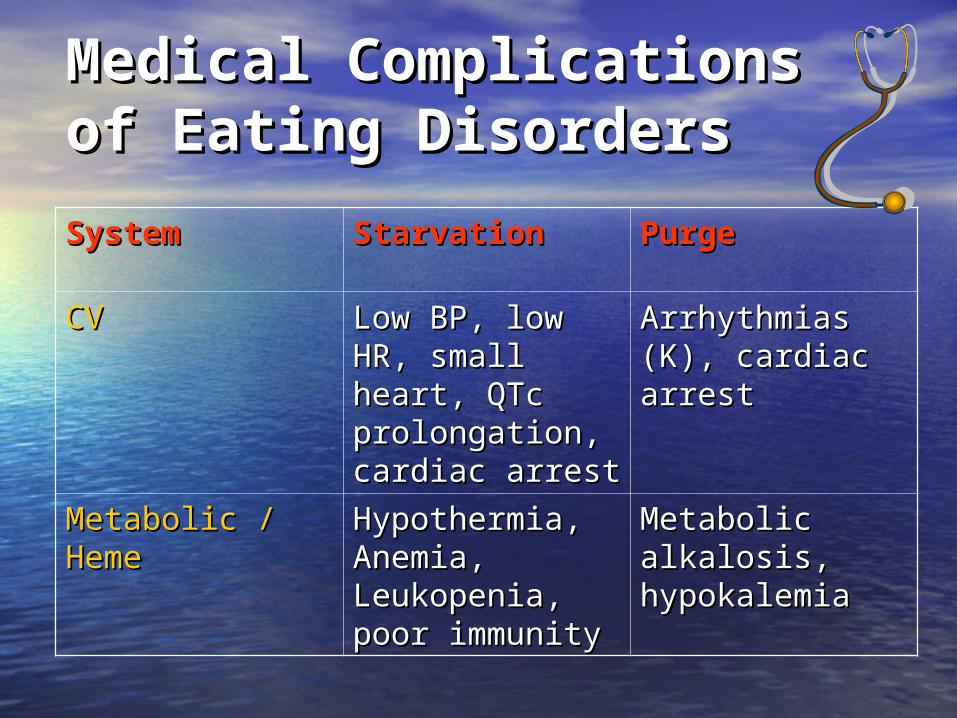
Medical Complications Medical Complications of Eating Disordersof Eating Disorders
SystemSystem StarvationStarvation PurgePurge
CVCV Low BP, low HR, Low BP, low HR, small heart, QTc small heart, QTc prolongation, prolongation, cardiac arrestcardiac arrest
Arrhythmias (K), Arrhythmias (K), cardiac arrest cardiac arrest
Metabolic / Metabolic / HemeHeme
Hypothermia, Hypothermia, Anemia, Anemia, Leukopenia, Leukopenia, poor immunitypoor immunity
Metabolic Metabolic alkalosis, alkalosis, hypokalemiahypokalemia
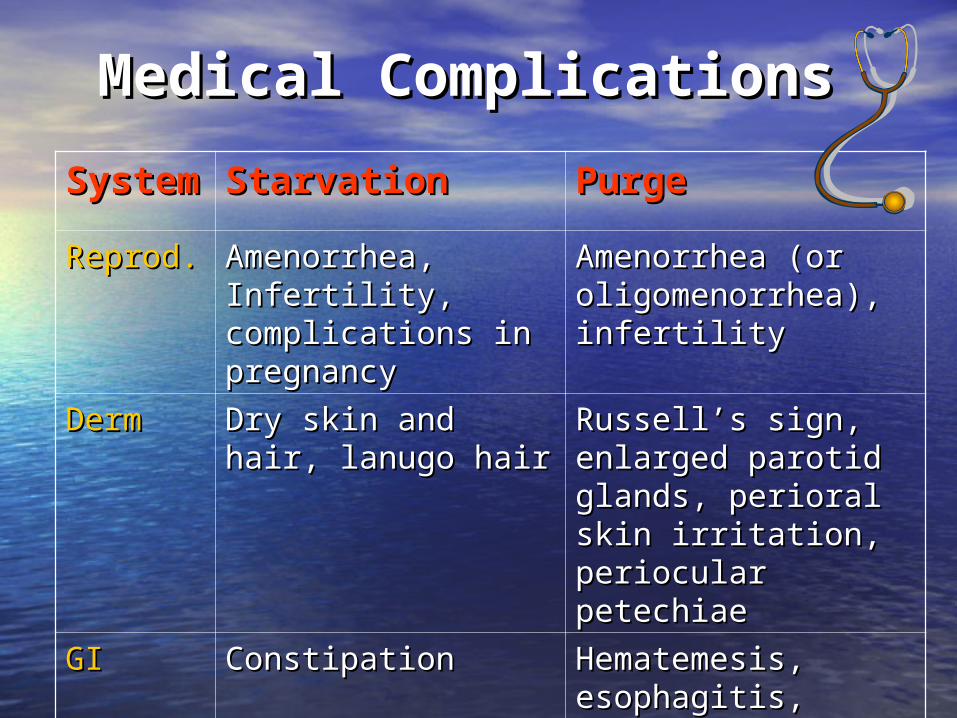
Medical Complications Medical Complications
SysteSystemm
StarvationStarvation PurgePurge
Reprod.Reprod. Amenorrhea, Amenorrhea, Infertility, Infertility, complications in complications in pregnancypregnancy
Amenorrhea (or Amenorrhea (or oligomenorrhea), oligomenorrhea), infertilityinfertility
DermDerm Dry skin and hair, Dry skin and hair, lanugo hair lanugo hair
Russell’s sign, Russell’s sign, enlarged parotid enlarged parotid glands, perioral skin glands, perioral skin irritation, periocular irritation, periocular petechiaepetechiae
GIGI ConstipationConstipation Hematemesis, Hematemesis, esophagitis, reflux, esophagitis, reflux, poor muscle tone in poor muscle tone in colon (laxative colon (laxative abuse)abuse)
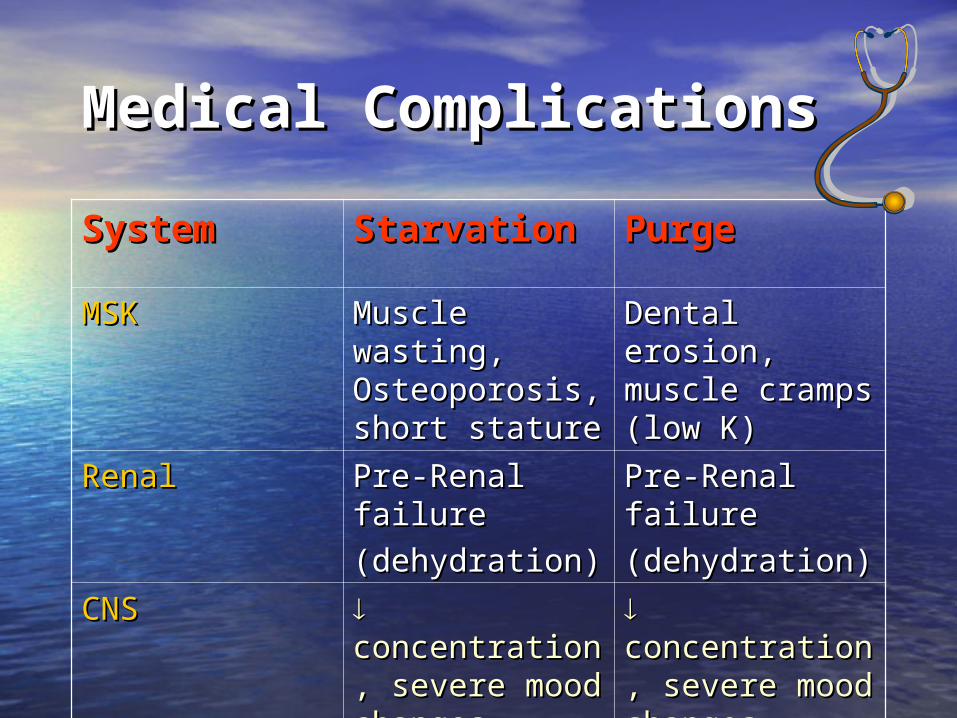
Medical ComplicationsMedical Complications
SystemSystem StarvationStarvation PurgePurgeMSKMSK Muscle Muscle
wasting, wasting, Osteoporosis, Osteoporosis, short statureshort stature
Dental erosion, Dental erosion, muscle cramps muscle cramps (low K)(low K)
RenalRenal Pre-Renal Pre-Renal failurefailure
(dehydration)(dehydration)
Pre-Renal Pre-Renal failurefailure
(dehydration)(dehydration)
CNSCNS concentration, concentration, severe mood severe mood changes, changes, white & gray white & gray mattermatter
concentration, concentration, severe mood severe mood changeschanges

Labs in Eating Labs in Eating Disorders:Disorders:
•BUN (dehydration)
•Amylase (vomiting)
•Cholesterol
(starvation)
*Labs often normal in AN
despite sig malnutrition!
•Na, K, CL (vomiting/laxatives)
•LH, FSH, estrogen
(starvation)
•RBCs (starvation)
•WBCs (starvation)
•T3

Clinical features of a Clinical features of a Patient at Higher Risk of Patient at Higher Risk of DeathDeath1.1. Very low weight at admissionVery low weight at admission
2.2. BradycardiaBradycardia
3.3. No medical follow-upNo medical follow-up
4.4. Longer duration of illnessLonger duration of illness
5.5. Multiple purging methodsMultiple purging methods
6.6. Chronic self-harm or suicide attemptsChronic self-harm or suicide attempts
7.7. Amphetamine or cocaine useAmphetamine or cocaine use
8.8. Severe alcohol abuseSevere alcohol abuse
Eating Disorders Eating Disorders OverviewOverview
• DiagnosisDiagnosis
• EpidemiologyEpidemiology
• Understanding Eating DisordersUnderstanding Eating Disorders– Etiology, Risk Factors, and PowerEtiology, Risk Factors, and Power
• Medical ComplicationsMedical Complications
• Principles of TreatmentPrinciples of Treatment
• OutcomeOutcome

Principles of Treatment Principles of Treatment for E.D.’s:for E.D.’s:1.1. Start with a thorough assessmentStart with a thorough assessment
a.a. Biopsychosocial formulationBiopsychosocial formulation
2.2. Multidisciplinary treatment team Multidisciplinary treatment team (physician, dietician, therapist…)(physician, dietician, therapist…)a.a. A psychological illness with medical and A psychological illness with medical and
nutritional consequencesnutritional consequencesb.b. Importance of medical and psychological Importance of medical and psychological
aspects of treatment togetheraspects of treatment together
3.3. Importance of Education Importance of Education

Treatment of Anorexia Treatment of Anorexia Nervosa:Nervosa:
• Medical and NutritionalMedical and Nutritional::– reversal of the effects of starvation; reversal of the effects of starvation;
re-feedingre-feeding– ““food is the medicine”food is the medicine”– meal plan, “mechanical eating” meal plan, “mechanical eating” – medical management and weighingmedical management and weighing– No medication found to be effective; No medication found to be effective;
(recent use of atypical antipsychotics); (recent use of atypical antipsychotics); SSRI’s not effective at low weightSSRI’s not effective at low weight
Treatment of A.N. Treatment of A.N. cont’d:cont’d:
• PsychologicalPsychological• Therapeutic AllianceTherapeutic Alliance• Supportive, compassionate, empathicSupportive, compassionate, empathic• Understanding the illness, educationUnderstanding the illness, education• Externalize the illness, lift blame and Externalize the illness, lift blame and
shame, challenging EDshame, challenging ED• Motivational techniques; exploring Motivational techniques; exploring
pros and cons, comparing to OCDpros and cons, comparing to OCD• Exploring and treating co-morbiditiesExploring and treating co-morbidities

Treatment of A.N. Treatment of A.N. cont’d:cont’d:
– Family Therapy for Children and Family Therapy for Children and Adolescents (evidence based)Adolescents (evidence based)
– CBT; IPT; motivational therapy; groupsCBT; IPT; motivational therapy; groups

Treatment of A.N. Treatment of A.N. cont’d:cont’d:
• Inpatient vs. Inpatient vs.
Day Treatment Programs vs.Day Treatment Programs vs.
Outpatient (stepped-care approach)Outpatient (stepped-care approach)
• Treatment of co-morbidities e.g.. Treatment of co-morbidities e.g.. anxiety, depressionanxiety, depression

Treatment of Bulimia Treatment of Bulimia Nervosa:Nervosa:• Use of high-dose SSRIs (Prozac)Use of high-dose SSRIs (Prozac)
• CBT (manualized); IPT; GroupsCBT (manualized); IPT; Groups
• Importance of a meal planImportance of a meal plan
• PsychoeducationPsychoeducation
• Treatment of co-morbidities, e.g.. Treatment of co-morbidities, e.g.. substance abuse, PTSD...substance abuse, PTSD...
Eating Disorders Eating Disorders OverviewOverview
• DiagnosisDiagnosis
• EpidemiologyEpidemiology
• Understanding Eating DisordersUnderstanding Eating Disorders– Etiology, Risk Factors, and PowerEtiology, Risk Factors, and Power
• Medical ComplicationsMedical Complications
• Principles of TreatmentPrinciples of Treatment
• OutcomeOutcome

Outcome for ANOutcome for AN
• High morbidity and mortality (among High morbidity and mortality (among highest of all psychiatric illnesses)highest of all psychiatric illnesses)
• Mortality: 5-20% Mortality: 5-20% – 50% suicide50% suicide– 50% medical complications50% medical complications
Outcome for ANOutcome for AN
• Prognosis in Adolescents:Prognosis in Adolescents:– 50-70% full recovery in 5 years50-70% full recovery in 5 years– 10-20% develop chronic AN10-20% develop chronic AN
• Prognosis in Adults:Prognosis in Adults:– Up to 50% recoverUp to 50% recover– 25% intermediate outcome25% intermediate outcome– 25% poor outcome25% poor outcome

Outcome for B.N.Outcome for B.N.
• Better treatment outcomes Better treatment outcomes compared to A.N.compared to A.N.
• Up to 70% recover with treatmentUp to 70% recover with treatment
• 15-20% intermediate outcome15-20% intermediate outcome
• 10-15% continue to do poorly10-15% continue to do poorly

Outcome cont’d:Outcome cont’d:• Better prognosis associated with:Better prognosis associated with:
– onset (and treatment) before age 15 yrsonset (and treatment) before age 15 yrs– treatment within 3 years of onset of illnesstreatment within 3 years of onset of illness– weight recovery within 2 years of treatmentweight recovery within 2 years of treatment
• Worse Prognosis associated with:Worse Prognosis associated with:– later age of onset, longer duration of illness, later age of onset, longer duration of illness,
previous hospitalizations, greater individual previous hospitalizations, greater individual and family disturbanceand family disturbance

www. nedic.ca

ReferencesReferences• American Psychiatric AssnAmerican Psychiatric Assn. DSM-5. . DSM-5.
Washington, D.C.: American Washington, D.C.: American Psychological Association, 2013.Psychological Association, 2013.
• APA GuidelinesAPA Guidelines, Practice Guideline , Practice Guideline for the Treatment of Patients with for the Treatment of Patients with Eating Disorders, Third Edition, 2006, Eating Disorders, Third Edition, 2006, update 2012update 2012
http://www.psychiatryonline.com/pracGuide/pracGuideTopic_12.aspx
ReferencesReferences
• Le Grange D et al, Academy for Eating Le Grange D et al, Academy for Eating Disorders Position Paper: The Role of the Disorders Position Paper: The Role of the Family in Eating Disorders, Family in Eating Disorders, International International Journal of Eating Disorders, Journal of Eating Disorders, 43:1, p1-5, 43:1, p1-5, 2010. 2010.
• Rosen, David, Identification and Rosen, David, Identification and Management of Eating Disorders in Management of Eating Disorders in Children and Adolescents, Children and Adolescents, PediatricsPediatrics,, Vol. Vol. 126 No. 6 December 2010, pp. 1240-1253 126 No. 6 December 2010, pp. 1240-1253