early pregnancy complications rukset attar, md, phd obstetrics and gynecology department
TRANSCRIPT
EARLY PREGNANCY COMPLICATIONSEARLY PREGNANCY COMPLICATIONS
Rukset Attar, MD, PhDRukset Attar, MD, PhD
Obstetrics and Gynecology Obstetrics and Gynecology DeparDeparttmentment
Nausea, Vomiting & Hyperemesis Gravidarum
70% to 85% of pregnant women often occurs in association with high levels of human
chorionic gonadotropin (hCG), such as with multiple pregnancies, trophoblastic disease
Conditions that Predispose to Excessive Nausea and Vomiting Viral gastroenteritis Gestational trophoblastic disease Hepatitis Urinary tract infection Multifetal gestation Gallbladder disease Migraine
Nausea, Vomiting & Hyperemesis Gravidarum
Treatment Dietary modifications and vitamin B6 therapy Phenothiazines (promethazine (Phenergan) often is
tried first) potential for dystonic effects.
Metoclopramide (Reglan) is the antiemetic drug of choice in pregnancy in several European countries
Ondansetron (Zofran) has been compared with promethazine (Phenergan), and the two drugs are equally effective
Nausea, Vomiting & Hyperemesis Gravidarum
Hyperemesis gravidarum 0.5% to 1% of patients Abnormal electrolytes, dehydration with high urine-
specific gravity, ketosis and acetonuria, and untreated have weight loss >5% of body weight.
Intravenous hydration is the first line of therapy for patients with severe nausea and vomiting
Spontaneous Abortion
Spontaneous abortionSpontaneous abortion is the most common is the most common complication of pregnancycomplication of pregnancy
is defined as the passing of a pregnancy prior to is defined as the passing of a pregnancy prior to completion of the 20th gestational week completion of the 20th gestational week or or delivery of all delivery of all or any part of the products of conception, with or without or any part of the products of conception, with or without a fetus weighing less than 500 g a fetus weighing less than 500 g
Threatened abortionThreatened abortion is bleeding of intrauterine origin is bleeding of intrauterine origin occurring before the 20th completed week, with or occurring before the 20th completed week, with or without uterine contractions, without dilatation of the without uterine contractions, without dilatation of the cervix, and without expulsion of the products of cervix, and without expulsion of the products of conception.conception.
Spontaneous Abortion
Complete abortionComplete abortion is the expulsion of all of the is the expulsion of all of the products of conception before the 20th completed week products of conception before the 20th completed week of gestation of gestation
Blighted ovumBlighted ovum or or anembryonic pregnancyanembryonic pregnancy represents a represents a failed development of the embryo so that only a failed development of the embryo so that only a gestational sac, with or without a yolk sac, is present. An gestational sac, with or without a yolk sac, is present. An alternative hypothesis proposes that the fetal pole has alternative hypothesis proposes that the fetal pole has been resorbed prior to ultrasound diagnosis. been resorbed prior to ultrasound diagnosis.
Spontaneous Abortion
incomplete abortion is the expulsion of some, but not all, of the products of conception
Inevitable abortion refers to bleeding of intrauterine origin before the 20th completed week, with dilatation of the cervix without expulsion of the products of conception
septic abortion, infection of the uterus and sometimes surrounding structures occur.
Spontaneous Abortion
approximately 15% of clinically evident pregnancies and approximately 15% of clinically evident pregnancies and 60% of chemically evident pregnancies end in 60% of chemically evident pregnancies end in spontaneous abortion.spontaneous abortion.
Eighty percent of spontaneous abortions occur prior to Eighty percent of spontaneous abortions occur prior to 12 weeks' gestation. 12 weeks' gestation.
An An abnormal karyotypeabnormal karyotype is present in approximately is present in approximately 50%50% of spontaneous abortions occurring during of spontaneous abortions occurring during the first the first trimester. trimester.
The incidence decreases to The incidence decreases to 20–30% in second-trimester20–30% in second-trimester losses and to losses and to 5–10% in third-trimester5–10% in third-trimester losses losses
Spontaneous Abortion
Etiology the the first-trimester lossesfirst-trimester losses are typically are typically autosomal autosomal
trisomies or monosomy Xtrisomies or monosomy X, whereas , whereas later losseslater losses reflect reflect chromosomal abnormalitieschromosomal abnormalities seen in neonates seen in neonates
infectioninfection,, anatomic defects, anatomic defects, endocrine factors, endocrine factors, immunologic factors, immunologic factors, maternal systemic diseases, maternal systemic diseases, unknownunknown
THROMBOPHILIA IN PREGNANCY
Rukset Attar, MD, PhDRukset Attar, MD, PhD
Obstetrics and Gynecology Obstetrics and Gynecology DeparDeparttmentment
Hypercoagulability in PregnancyHypercoagulability in Pregnancy
During pregnancy, there is a marked increase in the procoagulant activity by elevation of fibrinogen, factors II, V, VII, VIII, IX, X, XII and the von Willebrand factor.
Fibrinogen levels increase up to two fold. It is unclear why factor XI decreases. The physiological anticoagulant system becomes less
efficient because of an increased resistance to activated protein C in the second and third trimester and a reduced protein S activity, due to estrogen induced decreases in total protein S.
higher concentrations of plasminogen activator inhibitors (PAI), and an increased tendency to platelet aggregation
Overall fibrinolytic activity is impaired during pregnancy
Risk factors for thrombotic complications
Pregnancy-related risk factors for VTE include increasing maternal age (35 years), Caesarean section (especially emergency sections), thrombophilia, a family or personal history of thrombosis and obesity The puerperium itself is a risk factor (the most
probable trigger for that is delivery itself, because vessel trauma can cause thrombosis, and systemic coagulation activation in the mother’s circulation can easily occur.
Immobilisation after delivery can substantially add to this risk.
Risk factors for thrombotic complications
An individual assessment of the thrombotic risk should be undertaken, ideally before or in early pregnancy.
There is an increased risk of thrombosis in pregnant patients with thrombophilia depending on the severity of thrombophilia
Thrombophilia in Pregnancy
Inherited thrombophilias Acquired thrombophilias Non-thrombotic pregnancy complications and
thrombophilias
Inherited thrombophilias
genetic conditions with an increased thrombotic risk depending on additional risk factors
frequent causes of inherited thrombophilia are heterozygosity for Factor V Leiden (FVL) and G20210A mutation of the prothrombin gene;
rarer are antithrombin, protein C and S deficiency Hyperhomocysteinemia due to genetic defects
(homozygosity for a thermolabile mutant of methylenetetrahydrofolate reductase MTHFR) is controversially discussed as a cause of hereditary thrombophilia.
Inherited thrombophilias
Rare thrombophilic mutations, such as gene polymorphisms of plasminogen activator inhibitor-1, factor XIII or apolipoprotein B do not generally transfer an independent risk for thrombosis
Acquired thrombophilias
Antiphospholipid antibodies, such as the lupus anticoagulant or anticardiolipin and b-2-glycoprotein I antibodies are directed against glycoproteins in concert with phospholipids and are associated with thromboembolism and/or obstetrical complications.
Antiphospholipid antibodies (aPL) are found in about 5% of the reproductive population and antiphospholipid syndrome (APS) in 15–17% of women with recurrent pregnancy loss
Non-thrombotic pregnancy complications and thrombophilias
Maternal thrombophilias are not associated with pregnancy loss prior to 8–10 weeks of gestation , explained by the embryogenetic development of the vascular system
Before 8 weeks of gestation in the embryo there is only yolk sac vasculature, and thereafter a contact between the maternal and fetal circulation develops.
Therefore, it seems unlikely, that maternal thrombophilia can impair embryonic development at that earliest gestational stage.
Non-thrombotic pregnancy complications and thrombophilias
Women with thrombophilia show an increased risk for pregnancy loss at the end of the first and in the second trimester
those with FVL or prothrombin gene variant show a higher risk of late pregnancy loss (24 weeks)
Recurrent pregnancy loss has been linked to inherited thrombophilia particularly with protein C and S deficiency,FVL and a prothrombin gene variant
A significant association with increased risk for placental abruption was only observed with heterozygous FVL and the prothrombin gene variant
IUGR Pre-eclampsia
Management of thrombotic disorders during pregnancy
Risk-assessment for VTE Major known risk factors for VTE in pregnancy and in the
postpartum period are C-section, obesity, Prolonged bed rest, immobility, pre-eclampsia, Nephrotic syndrome, current infection and recent surgery previous VTE and thrombophilia.
In women at high risk LMWH prophylaxis should be continued for 4–6 weeks postpartum
Management of thrombotic disorders during pregnancy
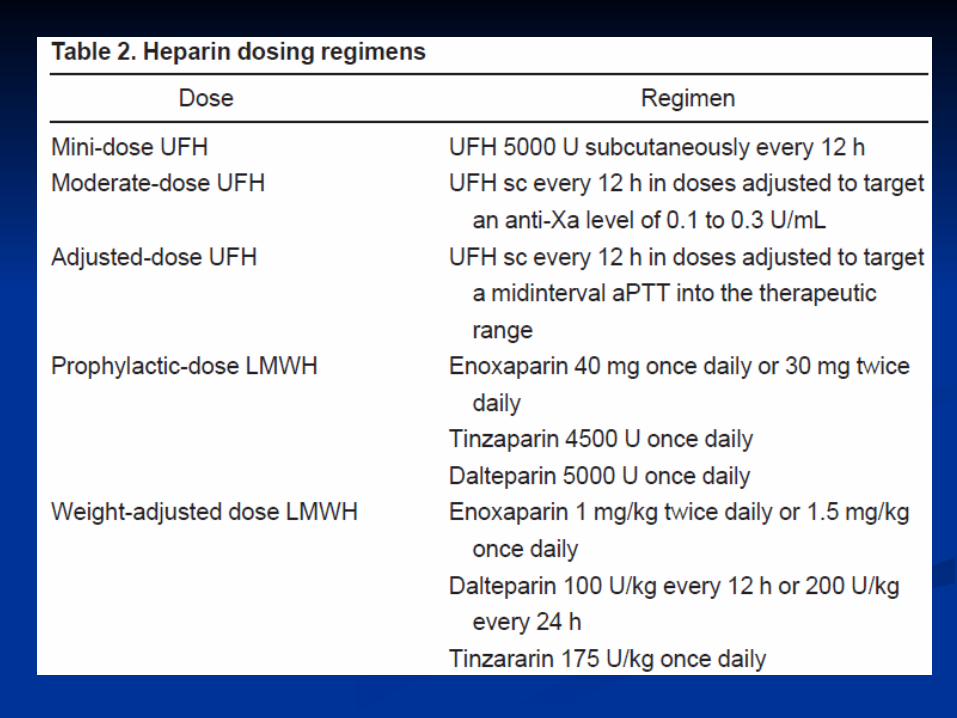
Anticoagulan Therapy coumarin-derivates Unfractionated heparin (UFH) low-molecular-weight heparins (LMWH) and aspirin
The choice of the anticoagulant depends on the maternal or fetal complications.
UFH and LMWH do not cross the placenta and are safe for the fetus.
Maternal bleeding complications appear to be uncommon with LMWH.
Management of thrombotic disorders during pregnancy
Prevention of VTE LMWH is the prophylaxis of choice in pregnancies at
risk for VTE No laboratory monitoring is required. All women with previous VTE or a thrombophilia
should be additionally encouraged to wear elastic compression stockings throughout their pregnancy and for 6–12 weeks after delivery.
Management of thrombotic disorders during pregnancy
Women with prior VTE These women should have a postpartum prophylaxis
for 6 weeks Two options have been proposed:
no routine prophylaxis during pregnancy, but clinical surveillance and immediate investigation in cases with clinical suspicion of VTE- due to transient risk factor
prophylaxis starting during the first trimester (ideally before 10 gestational weeks) in women with an increased risk for VTE (thrombophilia or a history of a severe thrombotic event like PE or extended deep vein thrombosis, VTE during previous pregnancy, or during HRT)-ACCP Guidelines, ACCP Guidelines, Chest 2008Chest 2008
Management of thrombotic disorders during pregnancy
Treatment of VTE Acute DVT or PE during pregnancy should be
managed initially as in non-pregnant women UFH or LMWH have to be given until the diagnosis is
confirmed. The first line treatment remains intravenous UFH (70
IU/kg as bolus, followed by 350 IU/kg/24 h as continuous infusion) to rapidly achieve an aPTT at 1.5–2.5 times the control value.
Therapeutic doses of LMWH may be started once the patient is hemodynamically stable
Management of thrombotic disorders during pregnancy
Weight-adjusted subcutaneous LMWH is to be preferred and administered once daily at a therapeutic dose (200 IU/kg/d) throughout pregnancy.
Twice-daily administration (100 IU/kg q12 h) might be preferable for obese patients to achieve more stable factor Xa-levels in plasma,
Therapeutic anticoagulation should be continued throughout pregnancy and for at least 6 month after thrombosis
• Patients with recurrent trombosis attacks without Patients with recurrent trombosis attacks without trombophilia shoud be on life-long anticoagulan therapytrombophilia shoud be on life-long anticoagulan therapy
• ProProphylaxis with UFH/LMWH during pregnancy and + with UFH/LMWH during pregnancy and + postpartum period is advised for these patients (Grade postpartum period is advised for these patients (Grade 1A)1A)
Management of thrombotic disorders during pregnancy
APS Pregnant women with APS and previous thrombosis
should receive antepartum and postpartum thromboprophylaxis with LMWH in a therapeutic dose
UFH combined with ASS significantly reduced pregnancy loss compared to ASS alone
A typical combined treatment regimen includes A typical combined treatment regimen includes aspirin aspirin (75–85 mg/day), (75–85 mg/day), beginning with attempts at beginning with attempts at conception, and conception, and unfractionated heparin (5,000–unfractionated heparin (5,000–10,000 subcutaneous twice daily), 10,000 subcutaneous twice daily), beginning at first beginning at first indication of pregnancyindication of pregnancy..
• Operations not related to malignancies, lasting Operations not related to malignancies, lasting no longer than 30 minutes don’t require any no longer than 30 minutes don’t require any prophylaxis unless there is another risc factor. prophylaxis unless there is another risc factor. Early mobilisation and IPC is advised for them Early mobilisation and IPC is advised for them (Grade 1A)(Grade 1A)
• No prophylaxis for laparoskopic procedures No prophylaxis for laparoskopic procedures unless there is another risc factor (Grade 1B) unless there is another risc factor (Grade 1B)
• Routin trombosis prophylaxis must be done in Routin trombosis prophylaxis must be done in major gynecologic operations (Grade 1A)major gynecologic operations (Grade 1A)• With no other risc factor and not related to With no other risc factor and not related to
malignancy- malignancy- DMAH (Grade 1A) or DMAH (Grade 1A) or unfractunated heparin (Grade 1A) or IPC unfractunated heparin (Grade 1A) or IPC (Grade 1B) (Grade 1B)
• With another risc factor or operation for With another risc factor or operation for malignancy- malignancy- heparin + IPC (Grade 1C)heparin + IPC (Grade 1C)
SectioSectio
• One risk factor besides pregnancy and sectio - One risk factor besides pregnancy and sectio - heparin prophylaxis or (IPC, GCS) during heparin prophylaxis or (IPC, GCS) during hospital stay (Grade 2C)hospital stay (Grade 2C)
• multipl risk factors- heparin prophylaxis or (IPC, multipl risk factors- heparin prophylaxis or (IPC, GCS) (Grade 2C)GCS) (Grade 2C)
• patients with high risk - prophylaxis for 6 weekspatients with high risk - prophylaxis for 6 weeks
• Routin trombosis prophylaxis should be started Routin trombosis prophylaxis should be started before the major gynecologic operationsbefore the major gynecologic operations
• Should continue during hospital stay (Grade 1A)Should continue during hospital stay (Grade 1A)• İf it was a cancer surgery or if the patient had a İf it was a cancer surgery or if the patient had a
VTE before LMWH should be continued for 28 VTE before LMWH should be continued for 28 days after discharge from the hospital (Grade days after discharge from the hospital (Grade 2C)2C)
Acute trombosis in pregnancyAcute trombosis in pregnancy
• UFH heparin UFH heparin (IV bolus, then infusion, aPTT (IV bolus, then infusion, aPTT measurement every 4 hours) or measurement every 4 hours) or LMWH LMWH ( twice a ( twice a day, s.c.) at least forday, s.c.) at least for 5 days 5 days (Grade 1A) (Grade 1A)
• Then prophylactic dosageThen prophylactic dosage• Should continue thoroughout pregnancy (Grade Should continue thoroughout pregnancy (Grade
1B) and 6 weeks postpartum (Grade 2C)1B) and 6 weeks postpartum (Grade 2C)• Should be stopped 24 hours before delivery Should be stopped 24 hours before delivery
(Grade 1C) if delivered at therapeutic dosage (Grade 1C) if delivered at therapeutic dosage

Unfractunated HeparinUnfractunated Heparin
• 3000- 30.000 Da3000- 30.000 Da• Binds to antitrombin, FIX, FX, FXI ve FXII Binds to antitrombin, FIX, FX, FXI ve FXII • Also binds to beta tromboglobulin, PF4, histidin Also binds to beta tromboglobulin, PF4, histidin
rich protein, vitronektin, platelets, osteoblasts rich protein, vitronektin, platelets, osteoblasts and endothelial cellsand endothelial cells
• IV IV • followed with aPTT measurements x1.5-2.5followed with aPTT measurements x1.5-2.5• neutralised with Protaminneutralised with Protamin
LMWHLMWH
• 2000- 9.000 Da2000- 9.000 Da• Exreacted from UH via chemical and enzimatic Exreacted from UH via chemical and enzimatic
proceduresprocedures• İnhibits Fxaİnhibits Fxa• Low affinity for endothelial cells, osteoblasts and Low affinity for endothelial cells, osteoblasts and
PLTPLT• Sc Sc • monitorised via antiXa- anti-Xa level should be monitorised via antiXa- anti-Xa level should be
0.5-1.2 U/ml0.5-1.2 U/ml• neutralisation with Protamin is lowneutralisation with Protamin is low
Whom should receive prohylaxis with Whom should receive prohylaxis with heparin during pregnancy?heparin during pregnancy?
• Those with valvular dieases or ritm disorders Those with valvular dieases or ritm disorders who are already on anticoagulation therapy who are already on anticoagulation therapy
• Recurrent VTE attacks- who are already on Recurrent VTE attacks- who are already on anticoagulation therapy anticoagulation therapy
• Patients with one VTE + trombophiliaPatients with one VTE + trombophilia• Patients with VTE during previous pregnancy or Patients with VTE during previous pregnancy or
HRTHRT
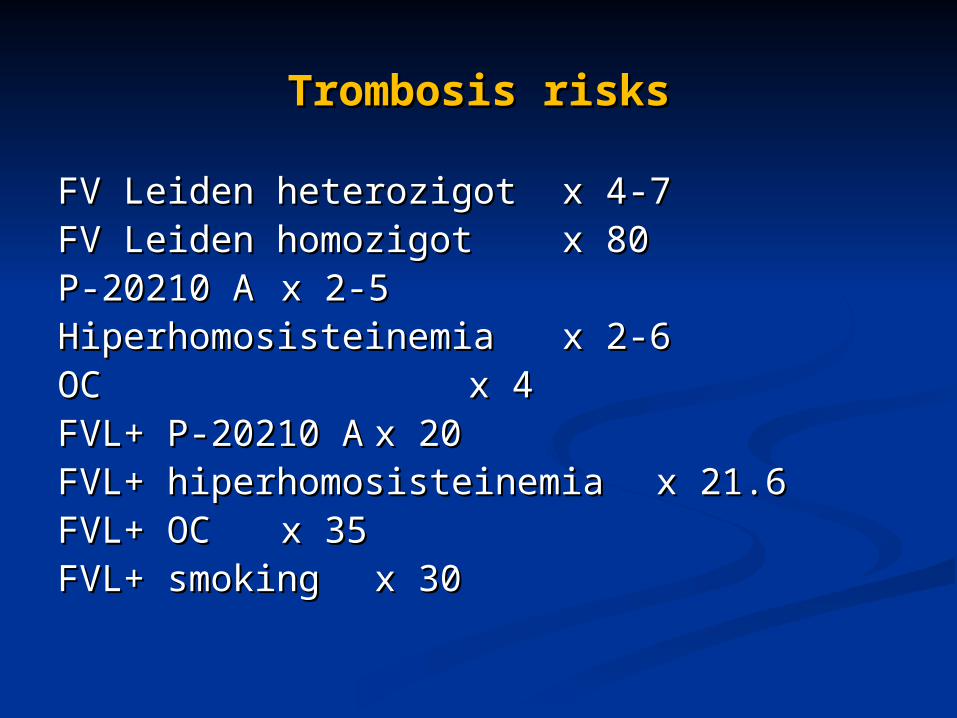
Trombosis risksTrombosis risks
FVFV LLeiden heterozigoteiden heterozigot x 4-7x 4-7FV Leiden homozigotFV Leiden homozigot x 80x 80P-20210 AP-20210 A x 2-5x 2-5HiperhomosisteinemiaHiperhomosisteinemia x 2-6x 2-6OC OC x 4x 4FVL+ P-20210 AFVL+ P-20210 A x 20x 20FVL+ hiperhomosisteinemiaFVL+ hiperhomosisteinemia x 21.6x 21.6FVL+ OCFVL+ OC x 35x 35FVL+ smoking FVL+ smoking x 30x 30
• FV Leiden mutationFV Leiden mutation
• Protrombin G20210AProtrombin G20210A
• Protein C activityProtein C activity
• Protein S activityProtein S activity
• AT activityAT activity
• Fasting homosistein levelFasting homosistein level
• Lupus anticoagulantLupus anticoagulant
• ACA IgG ve IgMACA IgG ve IgM
• Anti-B2 GPI IgG ve IgMAnti-B2 GPI IgG ve IgM
• ANA, anti-DNAANA, anti-DNA