early-life gut microbiota and breast milk oligosaccharides ...211364/fulltext02.pdf1 doctorial...
TRANSCRIPT
1
Doctorial thesis from the Department of Immunology, the Wenner-Gren Institute,
Stockholm University, Stockholm, Sweden
Early-life gut microbiota and breast milk oligosaccharides
in relation to childhood immune maturation and allergy
Ylva Margareta Sjögren
Stockholm 2009
2
Cover illustration: © Taina Litwak
All previously published papers were reproduced with permission from the publishers.
Distributed by Stockholm University Library.
Printed in Sweden by Universitetsservice AB, Stockholm 2009
© Ylva Margareta Sjögren
ISBN 978-91-7155-854-1
3
To all of us who dreamt about owning a pet but never could…

4

5
SUMMARY
Today, atopic allergy is the most common chronic disease among children in the developed world. This high prevalence could be associated with low microbial exposure due to changed lifestyle factors. The neonatal gut is immediately colonised by various bacterial species during and after birth. This gut microbiota is the most numerous bacterial stimuli in infancy and appears to be important for immune maturation. Previous studies also indicate that an altered gut microbiota might be associated with infant allergy development.
Immunomodulatory components in human milk might differ between mothers and could therefore explain the contradictory results seen regarding breastfeeding and allergy development. Oligosaccharides, the third most abundant solid component in human milk, survive the passage through the stomach and can be utilised by the gut microbiota. We analysed nine abundant neutral oligosaccharides in colostrum samples from allergic and non-allergic women and related the consumption of these oligosaccharides to subsequent allergy development in the children. We found a considerable variation in the concentration of neutral oligosaccharides in colostrum, which was not to be explained by the allergic status of the women. Neither was the consumption of neutral colostrum oligosaccharides related to allergy development in the children.
We further studied the early infant gut microbiota in relation to allergy development during the first five years of life, thus with a longer follow up than in previous studies. Also, we investigated gut microbiota at species level rather than genera level. Faecal samples were collected at one week, one month and/or two months after birth and presence and amounts of Clostridium difficile, Bifidobacterium (B.) adolescentis, B. longum, B. bifidum, B. breve, Lactobacilli (L.) group I (comprising L. rhamnosus, L. casei and L. paracasei), Lactobacilli group II (comprising L. gasseri and L. johnsonii) and Bacteroides fragilis were investigated. Infants who harboured Lactobacilli group I and B. adolescentis at one week of age developed allergic disease less frequently, during their first five years, than infants who did not harbour these bacteria at the same time. Further, we investigated whether early colonization with these bacteria was associated with lifestyle factors inversely related to allergy development. Actually, levels of house dust endotoxin and family size were associated with number of Bifidobacterium species in the early faecal samples.
Levels of salivary secretory IgA (SIgA) might be associated with allergy development and SIgA levels as well as the expression of Toll like receptors (TLR) on peripheral blood mononuclear cells (PBMC), could be influenced by microbial exposure. Thus, we investigated if early colonization with the above mentioned bacterial species influences childhood levels of salivary SIgA and spontaneous expression of TLR2 and TLR4 mRNA in PBMC collected twelve months after birth. In addition, we studied whether the early colonization associates with LPS-induced cytokine and chemokine production from the PBMCs. The early Bifidobacterium flora influenced levels of salivary SIgA at six and twelve months. In addition, the intensity of early Bacteroides fragilis colonization was inversely associated with spontaneous TLR4 mRNA expression in the PBMCs and to LPS-induced IL-6 and CCL4 production.
In conclusion, the work presented in this thesis indicates that the early gut microbiota might be altered in infants developing allergic disease. In addition, Bifidobacterium species influence early mucosal immune responses and colonization with these species is associated with house dust endotoxin levels and family size. Thus, the early gut microbiota could, to some extent, explain the inverse relationship between family size/endotoxin exposure and allergy development. However, consumption of colostrum neutral oligosaccharides does not protect against early allergy development.
6
SAMMANFATTNING
Idag är den vanligaste kroniska sjukdomen bland barn i västvärlden atopisk allergi.
En förklaringsmodell är att vi idag utsätts för mikrobiella stimuli i mindre utsträckning än tidigare, vilket troligtvis beror på förändrade livsstilsfaktorer. Spädbarn koloniseras med bakterier under och efter födseln. Det höga antal bakterier som koloniserar tarmen verkar spela roll för immunförsvarets mognad. Tidigare studier har påvisat vissa skillnader i den tidiga tarmfloran mellan barn som utvecklar allergi och barn som inte utvecklar allergi under sina första två år.
I bröstmjölk finns ett flertal komponenter som är viktiga för spädbarns immunförsvar. Dessa ämnen varierar mellan kvinnor och är beroende av såväl miljö- som genetiska faktorer. Några av dessa substanser skiljer sig dessutom åt mellan allergiska och icke-allergiska kvinnor. Denna variation i bröstmjölkens sammansättning skulle kunna förklara varför det är svårt att dra någon slutsats när det gäller amningens effekt på allergiutveckling. Efter fett och laktos förekommer oligosackarider i högst koncentration i bröstmjölk. Dessa bryts inte ned i magsäcken utan når tarmen intakta och kan där användas som näring till tarmbakterier. Vi analyserade nio av de vanligaste oligosackariderna i kolostrum från allergiska och icke-allergiska mammor, samt relaterade denna tidiga oligosackarid-konsumtion till allergiutveckling hos barn som följdes till 18 månader. Det var stor skillnad i oligosackaridkoncentration mellan olika kvinnors kolostrum. Däremot kunde inte kvinnornas allergistatus förklara detta och det var inte heller några skillnader i oligosackaridkoncentration mellan vad de allergiska och icke-allergiska barnen konsumerat under sina första dagar.
Vidare studerade vi tarmfloran under de första två månaderna hos spädbarn som under sina första fem år antingen utvecklade eller inte utvecklade allergi. Uppföljningen var därför längre än i tidigare studier. Förekomst och mängder av Clostridium difficile, Bifidobacterium (B.) adolescentis, B. longum, B. bifidum, B. breve, Lactobacilli (L.) grupp I (bestående av L. rhamnosus, L. casei och L. paracasei), Lactobacilli grupp II (bestående av L. gasseri och L. johnsonii) samt Bacteroides fragilis analyserades i de tidiga fecesproverna. De barn som vid en veckas ålder var koloniserade med Lactobacilli grupp I eller B. adolescentis utvecklade inte allergi i samma utsträckning som de barn som saknade dessa bakterier vid samma ålder. Vi undersökte även om livsstilsfaktorer påverkar koloniseringen av dessa bakterier. Både familjestorlek och endotoxin i damm från barnens hem korrelerade med antalet bifidobakterier i de tidiga fecesproverna.
Koncentrationen av sekretoriskt IgA (SIgA) i saliv kan vara associerat med allergiutveckling. Mikrobiella stimuli antas påverka SIgA nivåer och uttrycket av några av de receptorer som känner igen mikrober (TLR2 och TLR4). Därför undersökte vi hur de ovan nämnda tarmbakterierna påverkar nivåerna av SIgA i saliven under de första fem åren samt uttrycket av TLR2 och TLR4 på perifiera blodceller vid tolv månaders ålder. Den tidiga bifidobakteriefloran hade en tydlig förhöjande effekt på nivåerna av SIgA under det första året. Dessutom korrelerade mängden Bacteroides fragilis negativt med det spontanta uttrycket av TLR4 vid tolv månader. Vidare producerade dessa perifera blodceller lägre IL-6 och CCL4 efter stimuli med TLR4 liganden LPS.
De resultat som sammanfattas i denna avhandling tyder på att den tidiga tarmfloran är annorlunda hos barn som utvecklar allergi. Dessutom påverkar den tidiga bifidobakteriefloran SIgA i saliven under det första året. Bifidobakteriefloran verkar i sin tur vara påverkad av familjestorlek och endotoxin-exponering. Därför skulle tarmfloran till viss del kunna förklara det negativa sambandet mellan familjestorlek/endotoxin-exponering och allergiutveckling. Däremot verkar inte konsumtion av höga nivåer av oligosackarider i kolostrum skydda mot allergiutveckling under de första 18 månaderna.

7
LIST OF PAPERS This thesis is based on the following original articles, referred to in the text by their Roman numerals: I Sjögren Y. M, Duchén K, Lindh F, Björkstén B, Sverremark-Ekström E.
Neutral oligosaccharides in colostrum in relation to maternal allergy and allergy development in children up to 18 months of age. Pediatr Allergy Immunol 2007;18:20-26.
II Sjögren Y. M, Jenmalm M. C, Böttcher MF, Björkstén B, Sverremark-Ekström
E. Altered early infant gut microbiota in children developing allergy up to 5 years of age. Clin Exp Allergy 2009;39:518-526.
III Sjögren Y. M, Tomicic S, Lundberg A, Böttcher M.F, Björkstén B, Sverremark-
Ekström E, Jenmalm M.C. Influence of early gut microbiota on the maturation of childhood mucosal and systemic immune responses. Under revision

8
Om snöret inte håller, utan går av, är det bara att försöka med ett annat snöre
Nalle Puh (A.A Milne)

9
TABLE OF CONTENTS TABLE OF CONTENTS........................................................................................................................................9 ABBREVIATIONS .............................................................................................................................................. 10 INTRODUCTION................................................................................................................................................ 11
INNATE IMMUNITY ...................................................................................................................................... 12 Mononuclear phagocytes and antigen presenting cells................................................................................. 12 Pathogen recognition receptors..................................................................................................................... 13 Chemokines and cytokines in innate responses............................................................................................ 16 Granulocytes and Mast cells ......................................................................................................................... 18 Neutrophils ................................................................................................................................................... 18 Natural Killer cells........................................................................................................................................ 18
ADAPTIVE IMMUNITY ................................................................................................................................. 20 T cells............................................................................................................................................................ 20
CD8+ T cells ........................................................................................................................................... 20 CD4+ T cells ........................................................................................................................................... 20 γδ T cells .................................................................................................................................................. 23
B cells ........................................................................................................................................................... 23 Antibodies ................................................................................................................................................. 24 THE GUT ASSOCIATED IMMUNE SYSTEM ............................................................................................. 26
Antimicrobial peptides.................................................................................................................................. 27 Immunoglobulin A........................................................................................................................................ 28 Oral tolerance................................................................................................................................................ 29
Intestinal T cells and oral tolerance........................................................................................................ 30 Intestinal dendritic cells and oral tolerance............................................................................................ 31 ALLERGY ......................................................................................................................................................... 33
Factors influencing allergy development...................................................................................................... 34 Epidemiology of the hygiene hypothesis.................................................................................................. 36
Neonatal and infant immune responses ........................................................................................................ 37 Neonatal and infant immune responses in relation to subsequent allergy development .............................. 38
THE COMMENSAL GUT MICROBIOTA..................................................................................................... 41 Factors influencing the composition of the gut microbiota .......................................................................... 41 Infant gut microbiota .................................................................................................................................... 43 Fermentation, prebiotics and probiotics ....................................................................................................... 44 Methods for studying the gut microbiota...................................................................................................... 45 Gut microbiota and immune responses......................................................................................................... 46 Gut microbiota and allergy ........................................................................................................................... 48
IMMUNOLOGY OF HUMAN MILK ............................................................................................................. 50 Breast feeding in relation to allergy development ........................................................................................ 51 Human milk oligosaccharides....................................................................................................................... 52
PRESENT STUDY............................................................................................................................................... 54 AIMS ................................................................................................................................................................. 54 MATERIAL AND METHODS ........................................................................................................................ 55
Study population study I ............................................................................................................................... 56 Study population study II and III.................................................................................................................. 57
RESULTS AND DISCUSSION ....................................................................................................................... 59 Human milk oligosaccharides in colostrum of allergic and non-allergic women (I) ................................... 59 Colostrum oligosaccharide concentrations in relation to subsequent allergy development (I) .................... 60 Early infant gut microbiota (II and III) ......................................................................................................... 60 Early infant gut microbiota in relation to allergy development (II) ............................................................. 62 Environmental factors influence the early infant gut microbiota (II) ........................................................... 65 Early infant gut microbiota in relation to maturation of immune responses (III)......................................... 67 Clinical relevance ......................................................................................................................................... 72
CONCLUDING REMARKS ............................................................................................................................ 74 FUTURE PERSPECTIVES ................................................................................................................................ 75 ACKNOWLEDGEMENTS................................................................................................................................. 77 REFERENCES ..................................................................................................................................................... 79

10
ABBREVIATIONS 2´-FL 2´-Fucosyllactose 3-FL 3-Fucosyllactose AB Asthma bronchialis AD Atopic dermatitis AMP Antimicrobial peptide APC Antigen presenting cell APRIL A proliferation-inducing factor ARC Allergic rhinitis/conjunctivitis B. Bifidobacterium BAFF B cell activating factor C. Clostridium CBMC Cord blood mononuclear cell CD Cluster of differentiation CFU Colony forming unit CoNS Coagulase-negative Staphyloccocus CTL Cytotoxic T lymphocyte DC Dendritic cell DC-SIGN Dendritic cell-specific intracellular
adhesion molecule 3-grabbing integrin
DGGE Denaturing gradient gel electrophoreses
DNA Deoxyribonucleic acid E. Escherichia ELISA Enzyme-linked immunosorbent
assay Fel d 1 major allergen of cat (Felis
domesticus) FISH Fluorescent in situ hybridization G- Gram negative bacteria G+ Gram positive bacteria GALT Gut associated lymphoid tissue GF Germ-free HMGB1 High mobility group box protein 1 HMO Human milk oligosaccharides HPLC High performance liquid chromat IEC Intestinal epithelial cell IEL Intraepithelial lymphocyte IFNγ Interferon γ Ig Immunoglobulin IL Interleukin ILF Isolated lymphoid follicle L. Lactobacilli LAL Limulus Amebocyte Lysate LBP LPS binding protein LDFT Lactodifucotetraose LNDFH I Lacto-N-difucohexaose I
LNFP I Lacto-N-fucotetraose I LNFP II Lacto-N-fucotetraose II LNFP III Lacto-N-fucotetraose III LNnT Lacto-N-neotetraose LNT Lacto-N-tetraose LP Lamina propia LPS Lipopolysaccharide MACs Microflora associated
characteristics MALT Mucosa associated lymphoid tissue MAMP Microbial associated molecular
pattern M cell Microfold cell mDC myeloid dendritic cell MHC Major histocompatebility complex MLN Mesenteric lymph node NK cell Natural killer cell NKT cell Natural killer T cell NOD Nucleotide-binding oligomerization
domain OVA Ovalbumin PBMC Peripheral blood mononuclear cell PCR Polymerase chain reaction pDC Plasmacytoid dendritic cell PGN Peptidoglycan pIgR Polymeric immunoglobulin
receptor PP Peyer´s patches PPR Pathogen recognition receptor PSA Polysaccharide A RA Retinoic acid ROS Reactive oxygen species S. Staphylococcus SCFA Short chain fatty acids SIgA Secretory IgA SPT Skin prick test STAT Signal transducer and activator of
transcription TCR T cell receptor TFAN 4-Triflouroacetamidoaniline TGFβ Transforming growth factor β TLR Toll-like receptor Th T helper cell TNF Tumor necrosis factor T reg T regulatory cell TSLP thymic stromal-derived
lymphoprotein
11
INTRODUCTION
The immune system in mammals consists of innate and adaptive branches. An innate immune
response is the first defence against pathogens and involves anatomical and physiological
barriers, i.e. skin and temperature, as well as innate immune cells, like granulocytes,
monocytes and macrophages. These cells respond rapidly by phagocytosing pathogens and by
secreting substances like chemokines and cytokines which attract and activate other cells. The
adaptive branch is slower, but reacts to specific antigens and generates immunological
memory. Adaptive immunity is characterised by lymphocytes, i.e. T and B cells, their
cytokines as well as antibodies (immunoglobulins) produced by the B cells1. T and B cell
clones have receptors which are specific for diverse antigens on e.g. pathogens. On B cells,
these receptors are called antibodies. Secreted antibodies have several different functions i.e.
preventing entry of pathogens, facilitating opsonisation and activating complement. In
addition, antibodies can bind to Fc receptors on other cells than B cells. In allergic
individuals, IgE antibodies, towards innocuous antigens, have bound to e.g. mast cells and the
cross-linking of these antibodies leads to release of mediators causing allergic symptoms.
There is a constant collaboration between the innate and the adaptive immune system.
Antigen presenting cells (APCs), like macrophages and dendritic cells (DCs) recognize
microbial associated molecular patterns (MAMPs) via pathogen recognition receptors
(PRRs)2. The APCs instruct naïve CD4+ T cells to differentiate into either T helper (Th) 1,
Th2, Th17 or T regulatory cells (T regs) which are characterized primarily by their cytokine
profile. The cytokines secreted by Th2 cells facilitate the production of IgE antibodies by B
cells3. However, cytokines secreted by Th1 cells dampen the Th2 responses. The binding of
diverse MAMPs to PRRs on DCs generally favours Th1 differentiation1.
We have studied the most numerous microbial stimuli in infancy, the early infant gut
microbiota, in relation to allergy development. In addition, we investigated how it relates to
the maturation of the immune system and whether it is influenced by environmental factors
inversely related to allergy development. We also studied whether consumption of human
milk oligosaccharides, postulated to support the growth of certain gut microbiota species, is
associated with allergy development.

12
INNATE IMMUNITY
Mononuclear phagocytes and antigen presenting cells
Monocytes develop from the myeloid lineage in the bone marrow and they constitute 5-10
percent of peripheral leukocytes in human adults4. Blood monocytes are precursors for
macrophages and DCs and they also contribute directly to immune responses against
pathogens5 by secreting cytokines and reactive nitrogen and oxygen intermediates. Human
circulating monocytes are divided into two subsets, CD14hiCD16- and CD14loCD16+,
depending on their expression of CD14 and CD165. CD14 is involved in recognition of
lipopolysaccharide (LPS) from Gram negative bacteria (G-) whereas CD16 is an
immunoglobulin G receptor - FcγRIII. The CD14hiCD16-subset represents the majority of
circulating monocytes (80-90%). They are large and highly phagocytic with several granula
and often called classical or inflammatory monocytes, as they migrate to inflamed tissue6. The
CD14loCD16+ population is smaller and often called resident monocytes since they migrate to
non-inflamed tissue under homeostatic conditions. Yet, they are most often called pro-
inflammatory due to their production of high levels of tumour necrosis factor (TNF) after
stimulation with PRR ligands5. The difference in migratory properties depends on the
expression of different chemokine receptors on the two subsets. In example, the CD14hiCD16-
subset expresses high levels of CCR2 and thus responds to monocyte chemoattractant protein
(MCP-1 i.e. CCL2). The expression of the CCR2 receptor is low in CD14loCD16+ monocytes
and these cells rather migrate in the presence of CX3CL1. Furthermore, the subsets express
different immunoglobulin, adhesion and scavenger receptors: CD14loCD16+ expresses higher
levels of major histocompatibility complex (MHC) II and FcγRII and III7. Blood monocytes
can be matured into macrophages and dendritic cells, in vitro, when cultured in the presence
of M-CSF and GM-CSF + interleukin (IL) 4, respectively8. Less is known about this
differentiation in vivo6. Monocytes circulate in blood for approximately 3 days5 and thereafter
migrate to peripheral tissue where they mature into macrophages or DCs6.
Macrophages are a highly heterogeneous population mainly found in peripheral tissue9. They
are phagocytic cells that also release several cytokines and growth factors once they are
activated. Therefore, macrophages are important for clearance of altered cells and tissue
repair in addition to their bactericidal activity6. Macrophage differentiation is influenced by
13
the microenvironment in the actual tissue6. In example, macrophages in the gut meet high
amounts of cytokines with regulatory activity like transforming growth factor (TGF) β and
IL-10. Thus when maturing into intestinal macrophages they lose several receptors and
adhesion molecules. As they express co-stimulatory molecules, e.g. CD40, CD80 and CD86
at low levels, intestinal macrophages are poor APCs6. Also, they lack CD14 expression10 and
are therefore non-responding to inflammatory stimuli like LPS. Still, the intestinal
macrophages are efficient phagocytic cells with bactericidal activity6. There are also resident
macrophages in other tissues, exemplified by Langerhans cells in the skin, Kuppfer cells in
the liver, osteoclasts in bone and microglia cells in the brain7.
Dendritic cells are of major importance for immune responses11. They stem from the myeloid
or plasmacytoid lineage in the bone marrow and are initially divided into myeloid
(conventional) DCs or plasmacytoid DCs, respectively8. They are situated at sites where
pathogens enter, e.g the mucosal tissue. Like monocytes and macrophages, DCs recognize
pathogens via PRRs (see below)11. Furthermore, DCs initiate adaptive immune responses by
activating T cells. The DCs are the most potent APCs, generally assumed as the only cells
able to differentiate naive T cells into Th1, Th2, Th17 or Tregs11. Activated dendritic cells
frequently migrate from peripheral tissue to lymphoid organs in order to interact with T cells4.
Dendritic cells can further be divided into two subtypes depending on their location, blood
DCs and tissue DCs11. In addition, several different subtypes of DCs have been identified in
different tissues and also within different tissues, e.g. within the intestines (see below).
Pathogen recognition receptors
PRRs are essential for innate immunity. They recognize MAMPs that are shared by many
different microorganisms and accordingly PRRs have broad specificity against pathogens1.
Toll-like receptors (TLRs) is the best characterized group of PRRs. They are trans-membrane
receptors that recognize e.g. bacterial cell wall components and viral nucleic acids12. The
human TLRs identified so far (TLR 1-11) and their ligands are summarized in Table 1. For
example, the flagellin of flagellated bacteria is recognized by TLR5 and unmethylated CpG
dinucleotides in bacterial and viral DNA are recognized by TLR9. TLR2 recognizes several
different lipid proteins, e.g. peptidoglycan (PGN) and lipotechoic acid13. These molecules are
abundant in the cell layer of gram positive (G+) bacteria. The cell wall of G- bacteria contains
LPS (also referred to as endotoxin) which is recognized by TLR4. TLR4 also recognizes

14
envelope proteins from viruses and the endogenous heat-shock protein 60 and high mobility
group box 1 protein12, 14. For effective down-stream signaling, LPS binding protein (LBP)
binds to LPS. Thereafter, the LPS-LBP complex is transferred to CD14 which further
transfers LPS to MD-215. Eventually this complex directs TLR4 rearrangement and
recruitment of other adaptor proteins. Finally, intracellular signaling, either MyD88
dependent or independent, occurs. The ligation of most TLRs leads to downstream signaling
via MyD88 and eventually to the activation of transcription factors like NFκB12. This results
in transcription of genes (e.g. cytokines and chemokines) involved in the inflammatory
response.
Not only immune cells express TLRs. They can also be found on/in epithelial cells and
fibroblasts. Importantly, different TLRs are found on different cells. The intracellular TLR7
and TLR9 are expressed by pDCs, while mDC express TLR2, TLR3, TLR4, TLR5, and
TLR816. Monocytes express TLR1, TLR2, TLR4, TLR5, TLR817. Epithelial cells in the gut
appear to have a low expression of TLRs (e.g. TLR 2-5) or only express them on the
basolateral surface (i.e. the surface not facing the lumen containing the microbiota)13. PRRs
on innate cells are not only important for innate immune responses but also for adaptive
immune responses1. DCs recognize microbes and further internalize and present the antigens
of the pathogens to Th cells. Simultaneously the DCs receive signals via its PRRs. The DCs
share these signals with the Th cells via cytokines. Most often MAMPs binding to TLRs lead
to IL-12 production by the DC which directs the naïve T cell to differentiation into a Th1
cell1.
Another group of PRRs is the nucleotide-binding oligomerization domain (NOD) family1. It
consists of two intracellular receptors, NOD1 and NOD2. They recognize different bacterial
PGNs in the cytosol12. As with TLR engagement, NOD engagement leads to the production of
pro-inflammatory cytokines and chemokines resulting in e.g. neutrophil recruitment1.

15
Table. 1. The different human toll like receptors and their common ligands.
TLR receptor Ligand Pathogen containing the ligand
TLR1 Tri-acyl lipopeptides Bacteria and mycobacteria
TLR2 Lipoteichoic acid
Peptidoglycan
Zymosan
Heat shock proteins
G+ bacteria
G+ bacteria (mainly)
Fungi
Host
TLR3 Double stranded RNA Viruses
TLR4 Lipopolysaccharide
Envelope proteins
Heat shock proteins
HMGB1
G- bacteria
Virus
Host
Host
TLR5 Flagellin Flagellated bacteria
TLR6 Di-acyl lipoproteins Mycoplasma
TLR7,8 Single stranded RNA Virus
TLR9 CpG dinucleotides
Hemozoin
Bacteria
Plasmodium
TLR10 Unknown Unknown
TLR11 Unknown Uropathogenic bacteria Constructed from references 12-14. HMGB1= High mobility group box 1 protein, G+= Gram positive bacteria, G-= Gram negative bacteria.
TLR regulation
The expression of TLRs can change following stimulation and is dose and time dependent12,
18. Our group showed that the TLR4 monocyte expression was down regulated shortly after
LPS stimulation while TLR2 expression was up regulated after PGN stimuli in human
peripheral blood cells (PBMCs)19. Pro-inflammatory cytokines e.g. IFNγ can also influence
TLR expression14. It has been shown that high LPS exposure induces endotoxin (LPS)
tolerance18. Thus, endotoxin tolerant mice have decreased splenic TLR2 and TLR4
expression20. Also, these mice do not produce IL-1β when retreated with LPS. In addition,
Nomura et al showed that mouse macrophages produce less IL-6 and IL-12 when pre-
incubated with high doses of LPS18. Intravenous endotoxin administration also influences
16
human CD14+ cells to produce less IL-1β, TNF, IL-6 and CXCL8 (IL-8) after LPS stimuli in
vitro21.
Chemokines and cytokines in innate responses
Chemokines are small proteins that are important for directing immune cells to sites of
inflammation22. In addition, they participate in organ development and angiogenesis.
Chemokines are classified according to the arrangement of cysteine residues in the N-terminal
region of the protein and thus belong to the C, CC, CXC or CX3C subclasses. Chemokines
are produced by different cell types and can either be produced constitutively (homeostatic
chemokines) or in response to inflammatory stimuli (inflammatory chemokines). The
complexity of chemokines is due to their binding to receptors i.e. one chemokine can bind
several different receptors and the receptors can also have several ligands. CXCL8 (IL-8) is a
neutrophil attractant which is released by e.g. monocytes and epithelial cells in response to
bacterial stimuli22, 23. In addition, CXCL8 (IL-8) and CCL2 (MCP-1) are important for
angiogenesis22. Furthermore, CCL2 (MCP-1) is a monocyte, T cell, natural killer (NK) cell
and basophil attractant which also causes smooth muscle cells to proliferate. CCL4 (MIP-1β)
is another inflammatory cytokine released by monocytes in response to microbial stimuli. It
attracts several different leukocytes e.g. monocytes, T cells and DCs.
Cytokines are secreted proteins24 which mainly act locally. That is, they bind to receptors on
nearby cells (paracrine effect) or to receptors on the cell that produced them (autocrine
effect). They are involved in both innate and adaptive immunity and cause for example cells
to grow, differentiate and/or secrete substances like other cytokines or antibodies. Monocytes
can secrete several cytokines, like TNF, IL-1β, IL-6, IL-12, IL-15, IL-18, IL-23 and IL-2724.
IL-15 activates NK cells1 and IL-27 is a pro-inflammatory cytokine which up regulates the
production of interferon (IFN) γ from NK cells and Th1 cells24. The type 1 interferons, IFNα
and IFNβ, are important for protection against viruses1. Some of the mentioned cytokines are
of particular importance for this thesis and thus described below and/or in specific sections.
Tumor necrosis factor
TNF is a pro-inflammatory cytokine which is rapidly produced by macrophages and
monocytes in response to e.g. TLR ligands. TNF exerts its functions by binding to TNF
receptor-1 or TNF receptor-2 and further activates cells like neutrophils, platelets and
macrophages25. It is also important for sleep regulation and embryonic development.

17
Furthermore, TNF could induce apoptotic or necrotic cell death and might thus prevent tumor
growth. However, excess production of TNF is linked to autoimmune diseases and the
wasting syndrome, cachexia.
Interleukin 1β
IL-1β is produced by several cell types e.g. monocytes, macrophages and neutrophils26. The
related IL-1α is also produced by these cells but IL-1α has an autocrine effect and is not
secreted like IL-1β. Interleukin 1β is also a pro-inflammatory cytokine. It is responsible for
fever induction and, together with IL-6, responsible for the acute phase response23.
Interleukin 6
IL-6 is another pro-inflammatory cytokine. It is produced by APCs but can also be produced
by fibroblasts and epithelial cells27. IL-6 binds to the receptor complex of the IL-6 receptor
and gp130. The IL-6 receptor is present on several different leukocytes but also on
hepatocytes. As previously mentioned it induces acute phase responses but IL-6 has several
other functions and is considered as a pleiotropic cytokine28. It is a growth factor for B cells
and important for differentiation and IgA secretion (see below). IL-6 is also important for
macrophage differentiation, especially osteoclast differentiation28. It protects CD4 T cells
from cell death27 but also inhibits the suppressive effect of T regs29. Furthermore, it can
promote Th2 responses in addition to promotion of Th17 differentiation27, 30. Thus, IL-6 has
been linked to autoimmune diseases28.
Interleukin 10
IL-10 is an anti-inflammatory cytokine produced by a variety of cells including macrophages,
DCs, B cells and T regs31. It exerts its anti-inflammatory functions by decreasing cytokine
production and expression of co-stimulatory molecules on macrophages and DCs.
Furthermore, it is important for IgA production by B cells. However, IL-10 can also activate
mast cells, NK cells and CD8+ T cells. IL-10 deficient mice develop colitis and systemically
administrated IL-10 might be beneficial as therapy for psoriasis and Crohn’s disease31.
Interleukin 12
IL-12 is produced by monocytes, macrophages, DCs and neutrophils32. It consists of the two
subunits p35 and p40. The p35 together with p19 also forms the related cytokine IL-23 (see
the section about T cells). IL-12 binds to the receptor complex of IL12-R β1 and IL12Rβ2.
18
This leads to IFNγ production by T and NK cells. Thus IL-12 is important for Th1
differentiation.
Granulocytes and Mast cells
Neutrophils, eosinophils and basophils are all polymorphonuclear leukocytes. Neutrophils are
by far the most abundant of the granulocytes and are described in more detail below.
Eosinophils, basophils and mast cells are especially important for the protection against
parasites1. Mast cells are situated in mucosal and connective tissue whereas eosinophils and
basophils move from blood to the site of infection. A cell wall component of parasites, chitin,
appears to be able to recruit eosinophils. These cells are also involved in the allergic response
and further described in the allergy section.
Neutrophils
Neutrophils are phagocytic cells with antimicrobial activity1. Neutrophils express opsonin
receptors which facilitates the phagocytosis. They constitute approximately 60% of
leukocytes in blood33. Upon infection they are one of the first cells to be recruited. Once a
pathogen is phagocytosed the phagosome fuses with the granules in the neutrophil. These
granules contain different antimicrobial peptides (AMPs), reactive oxygen species (ROS) and
enzymes which kill the pathogen. Thereafter the neutrophil often undergoes apoptosis and is
cleared by macrophages. Neutrophils can also release their antimicrobial substances when
sensing infection34. This destroys surrounding tissue and pus is formed. Apart from being
effective killers, neutrophils are also important for wound healing. This is due to their ability
to sterilize the wound, to abolish the recruitment of additional neutrohils and to attract
macrophages. Furthermore, these macrophages release growth factors for epithelial cells.
Natural Killer cells
NK cells are important for the protection against intracellular pathogens1 and they also kill
transformed malignant cells35. Human blood NK cells can be divided according to their CD56
expression36. CD56dim express lower levels of CD56 and have high cytotoxic activity. In
contrast, CD56bright express higher levels of CD56 and produce more cytokines than CD56dim.
NK cells have activating and inhibitory receptors which recognize ligands on target cells. The
missing self hypothesis suggests that infected cells no longer express MHC class I and thus

19
not the ligand for the inhibitory receptors (e.g. KIR2DL1). If activating receptors (e.g.
NKG2D) simultaneously bind its ligands (e.g. MICA) the target cell will be killed by the NK
cell (for description of the killing see the part about CD8+ T cells). Lately, the importance of
signals from accessory cells for effective NK cell function has been proposed35. These
accessory cells are often antigen presenting cells which produces cytokines or signals via cell-
cell contact.
20
ADAPTIVE IMMUNITY
T cells
T cells originate in the bone marrow but develop in the thymus, hence their name. They
recognize antigens via their CD3-associated receptor37 and they are initially divided according
to the structure of the receptor. The T cell receptor (TCR) is either a complex of αβ subunits
or γδ subunits. The thymus exports six different populations of T cells; γδ T cells, naïve CD4+
αβ T cells, naïve CD8+ αβ T cells, NKT cells, T regulatory cells and intraepithelial
lymphocytes (IELs)38.
During the maturation in the thymus, the loci of the αβ receptor undergo V(D)J
recombination, leading to the specificity of the TCR38. The expression of the β subunit allows
the CD4-CD8- (double negative) T cells to express both the CD4 and the CD8 co-receptors
(double positive)39. These co-receptors recognize MHC class II and I, respectively. After
positive selection via MHC interactions the αβ CD4+ CD8+ T cells are negatively selected to
avoid strong self-reactive T cells. The αβ T cells then become single positive CD4+ or CD8+ T
cells. The single positive αβ T cell leaves the thymus when certain surface molecules, e.g.
S1p1, are up regulated allowing the cell to proliferate when the receptor interacts with its
antigen38.
CD8+ T cells
The CD8+ T cells are also called cytotoxic T lymphocytes (CTL). They are responsible for
killing of virus-infected cells and tumor cells40. When cells are infected, peptide antigens will
be expressed on MHC class I, which are expressed on virtually all nucleated cells, and thus
presented to CTLs. Just like NK cells, the CTLs contain granules. These granules contain
lytic enzymes e.g perforin. Perforin formes pores in the cell membrane of the infected cell.
The granula also contains granzymes which trigger apoptosis of the infected cell.
CD4+ T cells The CD4+ T cells are also called Th cells. APCs, which express MHC II, present antigens to
Th cells. The central role of Th cells is then to coordinate adaptive immune responses by
secreting cytokines and chemokines which attract and activate target cells41. Accordingly,

21
when B cells present antigens to Th cells, the Th cells produce cytokines activating the B cells
which thereby differentiate into antibody secreting plasma cells.
DCs are, in general, the only APC that can direct naïve CD4+ T cells into Th1, Th2, Th17 or T
regs cells11. For a functional differentiation, the TCR needs to encounter its antigen, signals
from co-stimulatory molecules have to occur (see the part about B cells) and cytokines have
to be present. The development of Th1 and Th2 cells appears to be induced mainly by IL-12
and IL-4, respectively41 (see Fig. 1). The transcription factors T-bet and Gata-3 induce
cytokine production in Th1 and Th2 cells, respectively. They also appear to be important for
the differentiation of the two subsets. Another factor that is important for differentiation of
Th1 cells is the IL-12 transducer Stat4. The IL-4 transducer Stat6 and the IL-2 transducer
Stat5 are involved in Th2 differentiation. In mice, is Th17 cell differentiation induced by IL-6
and TGFβ. The cytokines important for human Th17 cell differentiation are more
controversial. A study in 2007 showed that IL-23 and IL-1β but not TGFβ were important for
the differentiation42. However, others postulate that the serum used in this study contained
TGFβ and thus some TGFβ is important for differentiation of human Th17 cells but excess
amounts of this cytokine inhibit Th17 differentiation43. The transcription factor involved in
Th17 differentiation is RORγt and the IL-6, IL-21 and IL-23 signal transducer Stat3 is also of
importance.
The T helper cells are classified primarily according to their cytokine production (Fig. 1). T
helper 1 cells produce high levels of IFNγ and IL-2 after encountering an antigen. IL-2 is
important for formation of CD4+ and CD8+ memory cells41. IFNγ has antiviral activity, up
regulates the production of IL-12 and also activates macrophages41, 44. Th2 cells produce IL-4,
IL-5, IL-9, IL-10, IL-13 and IL-2541. As mentioned above, IL-4 is important for Th2
differentiation. It is also important for IgE class switching in B cells. IL-5 recruits eosinophils
and IL-9 activates mast cells and induces mucin production in epithelial cells. Further, IL-13
is important for IgE class switching and immune responses against helminths. IL-25 (IL-17 E)
induces several genes in Th2 cells leading to increased levels of Th2 cytokines24, 41. Human
Th17 cells secrete IL-17A and F, IL-22, IL-26, IFNγ and CCL2042. IL-17 consists of six
subsets, IL-17 A-F. The A and F subset causes epithelial, endothelial and fibroblasts to
release IL-6 and CXCL8 (IL-8) and thus induces neutrophil migration.

22
The Th1 cells are particularly important for immune responses towards intracellular
pathogens41. For example, their production of IFNγ increases the microbicidal activity by
macrophages. The immune responses mediated by Th2 cells combats parasite infections45
whereas Th17 cells appear to be important for immune responses towards extracellular
pathogens41. However, Th cells also play major roles in autoimmune diseases (Th1 and Th17
cells) and allergic diseases (Th2 cells).
Figure 1. The different subsets of CD4+ T cells. The cytokines and transcription factors important for differentiation are shown as well as the cytokines produced by the diverse subsets. This picture was originally published in Blood. CD4 T cells: fates, functions and faults. Zhu J and Paul WE. Blood 2008;112:1557-69. © the American Society of Hematology.
Regulatory T cells
Several different subsets of T regs exist. The CD4+ T regs can be divided into natural T regs
and induced T regs41, 46. The natural T regs differentiate in the thymus and these cells express
the transcription factor Foxp3 and high levels of the IL-2 receptor, CD2547. As with Th2
differentiation, activation of Stat5 is involved in differentiation of T regs41. The natural T regs
exert their regulatory effect through cell-cell contact but also produce the regulatory cytokines
TGFβ and IL-1041, 46. Induced T regs are Foxp3 positive as well as Foxp3 negative and they
differentiate in the periphery. Human and mice CD25-Foxp3- T cells can become Foxp3+ after
TGFβ stimuli (when pro-inflammatory cytokines are absent)46. In humans, there is no clear
marker that can distinguish T regs from effector T cells let alone natural T regs from induced
T regs46, 48. This is because Foxp3 expression can be up regulated after TGFβ stimuli.

23
However, the Foxp3 loci in natural T regs could be more de-acetylated than the Foxp3 loci in
TGFβ-stimulated T cells, postulating a new approach to identify natural T regs48. Th3 cells
are one example of induced T regs. They exert their regulatory effect by secreting mainly
TGFβ but also IL-10. Th3 cells are important for oral tolerance. T regulatory 1 cells (Tr1)
produce IL-10 and it is debated whether they are a lineage of T regs or merely a state that
each of the other existing lineages can reside in41.
The main function of T regs is to suppress inflammatory responses. Inadequate T regulatory
responses are thus involved in the pathogenesis of autoimmune disorders and allergy
development41. However, T regs might suppress immune responses which are important for
combating human papillomavirus-induced cancer49.
Also T cells express TLRs. TLR5 is strongly expressed on isolated human T cells50.
Activation via the TCR appears to be important for surface expression of some TLRs e.g.
TLR2 and TLR4. However, TCR activation down-regulates TLR5 expression. Interestingly,
the ligation of TLR2 on T regs enhances their suppressive activity50.
γδ T cells
The majority of the γδ T cells that migrate from the thymus reside in epithelial tissue,
including the skin and gut51. The antigens that stimulate epithelial γδ T cells appear to be lipid
antigens and phosphorylated microbial metabolites rather than the protein antigens that αβ T
cells recognize37. Presentation of antigens via MHC I or II is not needed for γδ T cell
activation. γδ T cells can be activated after stress or transformation of surrounding cells51.
Activated γδ T cells play an important role in tissue repair and can release the growth factors,
insulin growth factor-1 and keratinocyte growth factor. They can also lyse infected cells like
macrophages and epithelial cells. In addition, γδ T cells can secrete various cytokines and
chemokines including IFNγ, TNF and IL-437.
B cells
B cells are necessary for the humoral response since they produce antibodies. They develop in
the bone marrow in mammals but actually got their name from the Bursa of Fabricus, where
they develop in birds52. The B cells fully mature in secondary lymphoid organs e.g. lymph

24
nodes or the spleen. In these organs, the germinal center is the follicular environment where
humoral immune responses are initiated53. A B cell that recognizes an antigen internalizes and
presents it, via MCH II, to a CD4+ T cell52. Further CD40 on the B cell interacts with CD40
ligand (CD154) on the T cell. Then other co stimulatory molecules are expressed i.e. B7-1 or
B7-2 (CD80 or CD86) on the B cell which binds CD28 or CTLA-4 on the T cell. If CD28 is
bound there is a positive signal activating the T cell that then produces cytokines52. These
cytokines further support B cell proliferation and its differentiation into plasma or memory
cells, in addition to class switching (see below). Plasma cells secrete antibodies and reside in
organs which are exposed to antigens, e.g. the gut. Memory B cells either remain in their
follicle or circulate. They respond rapidly when encountering its antigen once more. B cells
also express TLRs, however the expression is somewhat altered during differentiation54.
Human memory B cells express TLR1, 5, 6, 7, 9, 10 with a low expression of TLR2. The
TLR ligation can induce polyclonal memory B cell proliferation and thus could TLR ligation
be important for preserving the memory B cell pool. The ligation of TLR 7 and 9 in human B
cells contribute to induction of antibody production. One fundamental difference between
murine and human B cells is the lack of TLR4 on human B cells.
Antibodies
Antibodies recognize antigens, e.g. on pathogens, and can thus facilitate the clearance of
pathogens52. They function as receptors on B cells (when bound to Fc-receptors) and secreted
antibodies can also bind to Fc-receptors on other cells e.g. monocytes, macrophages,
neutrophils and mast cells. When antigen-antibody complexes bind to receptors on
macrophages and neutrophils the complexes are phagocytosed resulting in clearance of the
pathogen. IgG and IgM also activate complement which primarily results in lyses of cells and
pathogens as well as phagocytosis of immune complexes. Secreted antibodies also prevent
pathogens from entering the body (see the part about IgA). An antibody consists of two heavy
chains and two light chains (κ or λ). These chains have constant and variable parts where the
variable part determines the specificity of the binding to a certain antigen. This specificity is
achieved through VDJ recombination which occurs during maturation in the bone marrow52.
The heavy chain determines the class of the antibody i.e. IgM, IgD, IgA, IgG or IgE. Mature
B cells express membrane bound IgM and IgD. IgM is the first antibody produced when the
mature B cell encounters an antigen. Class switching is needed for production of IgG, IgA or
IgE55. It occurs at gene level where the gene for the constant part of the heavy chain, usually
IgM, is replaced by the gene encoding the constant part of IgG isotypes, IgA isotypes or IgE.

25
The DNA in between is deleted. Immunoglobulin G consists of four isotypes, IgG1, IgG2,
IgG3 and IgG4, in humans52. IgA and IgE are abundant in mucosal tissue55 and are further
discussed in the gut immunology and allergy section, respectively.

26
THE GUT ASSOCIATED IMMUNE SYSTEM
The gastrointestinal tract consists of the oesophagus, the stomach, the small intestine and the
large intestine (colon)56. The small intestine can further be divided into duodenum, jejunum
and ileum. The different compartments have different physiological functions important for
food digestion (the stomach and duodenum), absorption of nutrients (small intestine) and
water and electrolytes (small intestine and colon). Mucosal epithelia are primary sites for
antigen entry57. Therefore mucosal associated lymphoid tissue (MALT) is of vast importance
for mounting immune responses towards foreign antigens. There are more lymphocytes in the
gut associated lymphoid tissue (GALT) than in all other secondary lymphoid tissues
combined58. The GALT is an immune privileged organ with the difficult task to mount
immune responses towards pathogens while at the same time being non-responsive to
commensal bacteria and food antigens. The primary barrier of the gut mucosa is the single
layer of epithelium. It consists of 5 types of cells, enterocytes, goblet cells, enteroendocrine
cells, M cells (see below) and Paneth cells17. The enterocytes absorb nutrients in the small
intestine. Paneth cells are only present in the small intestine and produce antimicrobial
peptides (AMPs). The goblet cells produce mucin, containing highly glycosylated proteins,
which protects the epithelium59. Beneath the epithelial cells lies the connective tissue, lamina
propia (LP)60. The GALT has its main site in the LP. The GALT consists of Peyer´s patches
(PP) in the small intestine and of isolated lymphoid follicles (ILF) in the colon (Fig. 2)58. The
most concentrated number of PP is in the terminal ileum11. Both PP and ILF are aggregates of
B-cell follicles with intervening T cells. PPs and ILF are the inductive sites where activation
occurs whereas the diffuse tissues of the lamina propia are effector sites where high amounts
of IgA are produced61.
There are mainly two types of cells in the gut mucosa which are able to transfer luminal
antigens to cells in PP and ILF; DCs and Microfold (M) cells. The M cells are integrated in
the epithelial layer and transport live microbes and microbial material from the lumen. DCs,
present in the LP, are able to open tight junctions in the epithelium making it possible for the
DC to send their dendrites into the gut lumen and sample antigens (Fig. 2)60. The DCs can
then present antigens to lymphocytes in PP and MLNs, but appear to never stray beyond this
lymphoid tissue and thus systemic infection is prevented60.

27
Figure 2. The structure of the gut associated lymphoid tissue (GALT). Adapted from60. © Taina Litwak 2004. Reprinted by permission from Taina Litwak.
Antimicrobial peptides
AMPs are a part of the innate branch and produced by virtually all multi-cellular organisms62.
In mammals, they are produced by leukocytes (especially neutrophils) and epithelium63. One
type of AMPs is enzymes that kill bacteria by disrupting their membrane, e.g. lysozyme59.
Another group is C-type lectins, e.g. RegIIIγ. Both these groups are especially efficient in
killing G+ bacteria. Yet, defensins is the most common group of AMPs in mammals63. Alfa
and β-defensins are the most abundant defensins in humans. The defensins are cationic
peptides which disrupt the membranes of pathogens. They are active against both G+ and G-
bacteria but also against fungi, protozoa and viruses. Alfa-defensins dominate in the small
intestine. They are produced by paneth cells in the crypts of small intestinal villi. Enterocytes

28
in the colon produce mainly β-defensins. Upon infection or inflammation, β-defensin
production is induced63. The fourth type of AMPs, cathelicidins (e.g. LL-37), is produced in
the colon and also kills bacteria by membrane disruption59.
Due to their structure, different AMPs have activity against different pathogens. It has been
postulated that the diverse AMPs produced by an individual can shape the colonizing
intestinal microbiota63. Apart from killing pathogens, regulating the number of bacteria in the
gut and preventing bacteria from entering, AMPs might also protect the stem cells in the
gut63. In addition, LL-37 is chemotactic and might also induce Th1 cytokine secretion by
dendritic cells59. Defensin β1 and Clara cell 16-kD protein also act on DCs and inhibits Th2
differentiation64. Several AMPs are produced constitutively also in germ-free animals59.
However, the ligation of PRRs is important for the production of other AMPs. In example,
production of RegIIIγ is initiated by MyD88 signalling and NOD2 signalling is important for
α-defensin production59. NOD2 mutations have been observed in patients with Crohn’s
disease. Thus, it is postulated that these mutations lead to lower α-defensin production
facilitating the pathogeneses of Crohn’s disease59.
Immunoglobulin A
Secretory IgA (SIgA) is of immense importance for mucosal immunity as it prevents the
invasion of pathogens e.g. Salmonella typimurium65, influenza virus66 and respiratory
syncytial virus67. It binds to adhesins and other receptors of pathogens thus preventing them
from penetrating the mucosal barrier68. In addition, SIgA can also bind to flagella of bacteria
and neutralize toxins. Furthermore, SIgA facilitates antigen sampling by binding to M cells69.
This leads to controlled antigen sampling which is suggested to induce further IgA production
without causing inflammation69. Since IgA does not activate the classical complement
pathway it is considered as an anti-inflammatory antibody70. Antigens that reach the lamina
propia can be bound by IgA and either excreted to the lumen or cleared by binding to FcαRI
on e.g. DCs or neutrophils71.
Humans produce two IgA subclasses; IgA1 and IgA270. Immunoglobulin A1 predominates in
the circulation while both IgA1 and IgA2 are abundant at mucosal surfaces. In the
gastrointestinal tract, IgA1 is more frequently produced in the upper digestive tract while
IgA2 is produced at higher levels in the colon11. The hinge region of IgA is longer in IgA1,

29
than IgA2, which makes IgA1 more susceptible to bacterial proteases70. Immunoglobulin A
mostly occurs as oligomers at mucosal surfaces in humans. The J chain joins the monomers
together and is also important for the transport of IgA across the surface and into the lumen.
The polymeric immunoglobulin receptor (pIgR) at epithelial surfaces interacts with the J
chain and shuttles IgA through the epithelial cell. Eventually pIgR is cleaved leaving IgA
with a secretory component. The seceretory component protects SIgA from proteolytic
degradation72. Large amounts of SIgA, 40-60 mg/kg, are produced in the gut lumen every
day61.
Class switching to IgA is either T cell dependent or T cell independent70. The secretion of IL-
4 and TGFβ1 by antigen-primed CD4+Th2 cells make the B cells undergo µ α switching in
PP73. IgA+ B cells differentiate further in the mesenteric lymph nodes before they enter the
blood stream61. As GALT DCs produce retinoic acid (RA), gut homing receptors (α4β7 and
CCR9) on lymphocytes are up regulated, which facilitates B cell-trafficking to the lamina
propia73. There, the IgA primed B cells finally become IgA secreting plasma cells by the help
of IL-5 and IL-6 produced by CD4+Th2 cells73. In addition the secretion of B cell activating
factor (BAFF) and a proliferation-inducing factor (APRIL) by DCs is important for fully
functional IgA secreting B cells70. Lately a T cell independent pathway for the activation of
IgA producing B cells has been postulated. Work by Mora and colleagues show that the
production of IL-5, IL-6 and RA by DCs in the PP provide a milieu for the B cells to start
producing IgA as well as up regulating gut homing receptors74. Also, others postulate that the
release of APRIL from epithelial cells can cause IgD+ B cells to directly class switch to IgA75
The release of TGFβ1, APRIL and BAFF by DC is probably also needed for this to function
properly70.
Oral tolerance
The intestinal immune system encounters more antigens than any other part of the body76.
Antigens from pathogens should mount a strong immune response but on the other hand food
and commensal antigens should be tolerated. When not tolerated, disorders like inflammatory
bowel disease, coeliac disease and food allergy could occur. Mice undergoing mesenteric
lymphadenectomy cannot induce oral tolerance which postulates a central role for MLNs in
oral tolerance induction58. The predominant site for naive T cell activation takes place in the
MLNs77. It is not known whether tolerance to commensals and food antigens is acquired in

30
the same way78. The commensal microbiota can, in contrast to food antigens, signal through
TLRs which might be important for tolerance induction. Food antigens can also be found in
systemic peripheral lymph organs; however when the MLNs are intact commensals never
stray beyond the MLNs.
Several factors influence the outcome of an immune response towards orally administered
antigens77. The maturation of DCs is influenced by the surrounding cytokine mileu. In
addition, the differentiation of T cells, after antigen presentation, is influenced by the maturity
status of the DC. This and how T cell subsets react to antigens are described below. The
amount of antigen available (see also factors influencing allergy development) and how it is
processed also plays a substantial role for tolerance induction77. The acidic environment and
the proteolytic enzymes in the gut facilitates antigen breakdown. An intact barrier decreases
excess immune responses to the antigen. Inflammation and low secretion of SIgA are two
factors that reduce the integrity of the barrier.
Intestinal T cells and oral tolerance
As mentioned above, lymphocytes that are primed in the PP migrate to the MLN for further
differentiation, then enter the bloodstream and accumulate in the mucosa. As with B
lymphocytes, T lymphocytes up regulate the adhesion molecules CCR9 and α4β7 which
facilitate the migration to the gut mucosa. Lymphocytes located between intestinal epithelial
cells are called intraepithelial lymphocytes (IELs)79. Their primary role is to eliminate
infected and damaged epithelial cells, thus sustaining the integrity of the epithelial barrier.
The IEL population holds NK cells, γδ T cells and CD4+ and CD8+ αβ T cells. The different
compartments of the gut harbour different IELs. In humans, the small intestine IELs are
primarily CD8+ αβ T cells while the colon mainly harbour CD4+ αβ IELs79. The LP is
inhabited by both CD4+ and CD8+ T cells76.
Of importance for oral tolerance are clonal deletion (apoptosis) and clonal anergy of antigen-
specific CD4+ T cells58. This appears to happen after high-dose antigen feeding. An anergic
cell is not activated when its receptor binds the antigen due to lack of costimulation. Immature
DCs express low levels of CD80 and CD8677 and are thus unable to induce signals via CD28
on T cells. CD80 and CD86 can also bind to CTLA-4 on T cells leading to an inhibitory
signal. The molecule CTLA-4 appears to be important for oral tolerance77. Administration of
multiple doses of low concentrations of antigen probably induces active suppression by T

31
regs. Several different subsets of T regs exist in the gut76. When IL-10 and TGFβ were
depleted from LP T cells, they lost their unresponsiveness towards commensal bacteria
indicating that T regs are involved in the tolerance towards commensal antigens. The Th3
cells that produce TGFβ have been isolated from mice MLNs after feeding small doses of
antigen for tolerance induction76. Tr1 cells, which produce IL-10, are induced in PPs and
MLN after feeding77. In addition, mice deficient in IL-10 develop inflammatory bowel
disease, a finding which postulate a role for these cells in controlling immune responses.
Furthermore, CD4+CD25+ T cells could also be important for tolerance induction as children
who outgrow their cow´s milk allergy have allergen-specific CD4+CD25+ T cells in their
blood80. In mice, it has been shown that different compartments of the body harbour different
T regs81. The T regs in spleen and lymph nodes are mainly Foxp3+IL-10- and arise from
thymic precursor cells whereas the most abundant T regs in the small intestine and PPs are
Foxp3-IL-10+ and resemble Tr1 cells81. Also, the large intestine T regs differ from the small
intestinal T regs, as they are merely Foxp3+IL-10+.
Intestinal dendritic cells and oral tolerance
The functional properties of DCs differ due to their different locations10. In presence of TGFβ,
DCs from LP and MLN are better at inducing Foxp3 in naive T cells, than are splenic DCs.
Activated DC subsets from the PP produce higher levels of IL-10 than activated DCs from the
spleen. These PP DCs induce naive T cells to produce higher IL-10 and Th2 cytokines than T
cells activated by splenic DCs. This appears to be especially attributed to the
CD11chiCD11b+CD8α-10. Other subsets in PPs are CD11chiCD11b-CD8α+ and
CD11chiCD11b-CD8α-. These three subtypes of DCs also appear to be present in LP of the
small intestine. Few DCs are present in the LP in the colon. Instead they are mostly located in
the ILFs10. The MLNs contain DCs that have migrated from the LP but also DCs that are
derived from blood-borne precursors. Also, plasmacytoid DC have been identified in the PPs
and MLNs10. Plasmacytoid DCs have been described to be tolerogenic in mice76.
Why do mucosal DCs differ from systemic DCs and preferably secrete anti-inflammatory
cytokines and induce the differentiation of Tregs, Th2 and Th3 cells during homeostasis?
Lately, the intestinal epithelial cells have been shown to play a fundamental role in
conditioning DCs. The thymic stromal-derived lymphoprotein (TLSP) released by epithelial
cells is able to condition DCs into a non-inflammatory state (Fig. 3). Further these DCs
induce naive T cells to differentiate into Th2 cells. In addition, TSLP can convert Foxp3-

32
thymocytes into Foxp3+ thymocytes82. Other factors that are important for conditioning of
DCs, is the presence of IL-10 and TGFβ, either produced by other DCs10 or T cells11. These
GALT DCs also are important for IgA production as previously mentioned.
Figure 3. Proposed mechanism for conditioning of dendritic cells (DCs). Epithelial cells produce retinoic acid (RA) and in response to commensal bacteria; thymic stromal-derived lymphoprotein (TSLP). These substances together with interleukin (IL) 10 and transforming growth factor (TGF) β, influence DCs to mature into conditioning DCs which produce little IL-12. Instead they produce RA, TGFβ and a proliferation inducing factor (APRIL) which are important for IgA production and regulatory responses in the gut. Reprinted by permission from Macmillan Publishers LtD: [Nature Reviews Immunology] 2008;8:435-446.
When pathogens invade the mucosal tissue an inflammatory response needs to be initiated.
This is postulated to occur when pathogens invade mucosal epithelial cells11. Compared to
commensal bacteria, the pathogens produce virulence factors, like toxins and adherence

33
factors, which make it possible to invade the epithelial cell. Once invaded the epithelial cells
produce inflammatory cytokines and chemokines, e.g. CXCL8, which attracts and activates
other cells. Neutrophils, macrophages and monocytes are examples of cells that are activated
by the inflammatory cytokines/chemokines and the pathogens. Possibly DCs from the MLNs
induce Th1 responses when meeting the pathogens10.
ALLERGY
Today, atopic allergy is the most common chronic disease among children in the developed
world. The current prevalence of the allergic symptoms asthma, eczema and allergic rhino-
conjunctivitis has been investigated in the ISAAC studies. Thus, among 6-7 year-old Swedish
children, 10% have asthma, 13% have eczema and 10% have symptoms of allergic rhino-
conjunctivitis83. Exposure to common environmental antigens such as plant pollen, house dust
and animal and food proteins can cause an allergic response. However, it is not known why
some individuals develop allergic disorders. Atopic allergies are IgE-mediated and also called
hypersensitivity type 1 or immediate hypersensitivity reactions. The above prevalence data
only demonstrates symptoms, however it is estimated that approximately 25% of the
population in the developed world have IgE-mediated allergic disease3. The term atopy means
that a person has a hereditary or personal predisposition to produce IgE antibodies towards
allergens and to develop allergic symptoms84. The risk of developing allergic disease is much
higher if both parents are allergic compared to if they are non-allergic85. Since the prevalence
of atopic allergy has increased during the last decades, genetics alone cannot explain the
development of the disorder86. The current view about atopic allergy is that both genetic and
environmental factors seem to interact with each other, leading to the production of IL-477.
IL-4 plays an important role in developing naive T cells into CD4+ Th2 cells (Fig. 4a). The
cytokines produced by Th2 cells induce IgE class switching3. Further allergen encounter
makes the B cells secrete IgE. Mast cells, basophils and eosinophils have receptors for IgE55.
The immediate allergic response occurs when the allergen crosslinks IgE bound to Fcε
receptor 1 on the mast cell3 (Fig. 4b). This leads to mast cell degranulation followed by the
release of histamine, heparin and proteases within minutes, all leading to the clinical
symptoms. The clinical symptoms arise from the contraction of intestinal and bronchial
smooth muscles, increased mucus production, vasodilatation and increased vascular
permeability. The eosinophils and neutrophils are recruited to the inflammatory site by

34
cytokines and chemokines released by e.g. the mast cells55. The allergen-specific T cells as
well as the eosinophils and neutrophils are responsible for the late allergic response (Fig. 4c).
This response occurs hours to days after contact with the allergen and the mediator´s,
leukotrienes and prostaglandines, effects are more pronounced and long-lasting than those of
histamine.
Figure 4. The allergic reaction. The naïve Th cell is presented to an allergen (a). In an IL-4 rich milieu the Th cell develops into a Th2 cell. The B cell encounters the allergen and presents it to the Th2 cell which then produces IL-4, IL-5 and IL-13. IgE class switching is then induced. The IgE antibodies attach to Fcε receptors on mast cells and eosinophils and the individual has become sensitized. Once the individual encounters an allergen again this leads to crosslinking of the Fcε receptors and release of inflammatory mediators causing the allergic response (b and c). The substances released from mast cells cause the immediate reaction (b) while the substances released from eosinophils cause the late reaction (c). Reprinted by permission from Macmillan Publishers LtD: [Nature Reviews Immunology] 2002;2:446-453
Factors influencing allergy development
Parental allergy is a strong risk factor for allergy development87. Both complete chromosome
regions and gene polymorphisms have been linked to allergic disease64. The linkage region in

35
chromosome 5q31-33 includes 14 genes associated with asthma and atopy e.g the genes for
IL-4, IL-13 and CD14. Polymorphisms in genes involved in microbial recognition and innate
immune responses as well as Th2 differentiation are also linked to allergic disease, as are
polymorphisms in genes for epithelial-produced chemokines, i.e. the eosinophilic attractants
CCL11, CCL24 and CCL26. Interestingly, phenotypes might respond differently depending
on their environmental exposure postulating that gene-environment interactions are of
importance. It has been shown that the CC allele, of CD14 C-260, protects against high
specific IgE when children are exposed to high levels of endotoxin or stable animals88.
Children bearing the TT allele rather have high total IgE levels when exposed to high
endotoxin levels and stable animals but low IgE levels when living with a dog or a cat.
The dose, timing and route of allergen exposure seem to influence allergy development. The
foetus can be exposed to allergens already in utero89. Allergens cross the placenta90 and
consumption of food allergens correlate with the levels in cord blood91. However, the IgE
levels in cord blood do not correlate with the IgE levels at six month92 indicating that allergen
exposure in utero does not lead to any persistent IgE-sensitization. The exposure to high birch
pollen in utero is not significantly associated with sensitisation later in life93. However, the
exposure during the first months of life significantly increases the risk for allergic asthma and
positive skin prick test (SPT)94, postulating that the exposure in infancy might be of
importance. Yet, exposure to pets during the first year of life has, in contrast, been shown to
be associated with lower frequency of allergic rhinitis and asthma later in life95. Previously,
the American Academy of Pediatrics recommended pregnant and lactating women to avoid
peanuts. In addition, they also recommended a delayed introduction of dairy products, egg,
fish and nuts to the infants. However, these recommendations were not enough evidence
based and today no organisation recommends food avoidance due to its allergenicity96. Others
have instead suggested the opposite i.e. that earlier introduction of complementary foods
(with continued breastfeeding) increases tolerance induction97. This is due to the postulated
time window of opportunity for tolerance induction97. Theoretically, the fetus can be exposed
to allergen-specific IgE antibodies from its mother, but it is controversial whether IgE crosses
the placenta98. IgE antibodies are readily detected on fetal cells in the placenta, regardless of
maternal allergy99 and it is likely that this IgE actually originates from the mother100.

36
Figure 5. Allergic heredity is associated with allergic disease and also the timing and dose of allergen exposure appear to influence allergy development. Environmental factors increase or decrease the risk of developing allergic disease. Importantly, the interaction between heredity, allergen and environmental exposure contribute to the development of allergic disease.
Epidemiology of the hygiene hypothesis
In 1989 David Strachan described that children with older siblings developed allergy to a
lower extent101. It was postulated that the lower incidence of atopic disease among these
children was due to higher microbial exposure of these children, the so called hygiene
hypothesis. Since then, several epidemiologic studies have confirmed the inverse relationship
between number of siblings and allergy development102. Also, certain infections are
associated with less allergic disease. Matricardi et al showed that seropositivity to several
food and orofecal pathogens was associated with 60% lower incidence of allergic disease than
seronegativity to these pathogens103. Another recent study showed that seropositivity, against
different infectious pathogens, decreased the incidence of different atopic disorders104.
Supporting this, seropositivity towards the herpesvirus Epstain Barr Virus (EBV) was
negatively associated with IgE sensitization and this was further strengthened if the subjects
also were seropositive for cytomegalovirus85. The same study could not show any association
between seropositivity against respiratory viruses and IgE sensitization, however85. Actually,
severe infections with respiratory syncytial virus might instead be associated with increased
risk of asthma development105. So far it cannot be concluded that childhood infections protect
from atopic disease106.

37
There is a lower prevalence of atopic allergy among children growing up on farm107. Children
growing up in this environment are exposed to high levels of microbial products, i.e.
endotoxin and bacterial DNA108. Furthermore, children exposed to higher levels of endotoxin
are less frequently allergic109. In addition, prenatal exposure to farming environment might be
particularly protective110. Consequently, it might be the microbial products and not the
infections per se that prevent allergic disease.
Neonatal and infant immune responses
The immune system of the newborn is immature111. The structure of the lymph nodes and
spleen is underdeveloped. In addition, the number of B and T cells is low. Infant and neonatal
B cells rather differentiate into memory B cells than plasma B cells, due to low expression of
CD21 on naïve B cells112. Class switching is also incomplete113 and neonates respond poorly
to thymus independent antigens like polysaccharides on encapsulated bacteria112. Actually,
IgG antibody responses to polysaccharides are limited during the first 18-24 months whereas
antibody responses to protein antigens are limited during the first twelve months112.
Fortunately, maternal IgG is actively transferred across the placenta during pregnancy to
compensate for the impaired production of Ig isotypes at birth114. However, these antibodies
are catabolised during the first two to six months after birth112, 113. As shown in formula-fed
infants, the infants own production of intestinal SIgA is rare during the first ten days after
birth115. Actually, the isolated lymphoid follicles in the colon do not develop during fetal
life116. Instead they develop when the gut is colonized. It takes up to five years before the
levels of salivary SIgA reach adult levels (Tomicic et al unpublished). Also, the transport of
IgA appears to be immature in infants. That is, the levels of salivary SIgA are low in infancy
whereas the levels of total IgA are higher117. This immaturity seems to be more pronounced in
Swedish compared to Estonian infants (Tomicic et al unpublished).
With a rather immature adaptive immune system the innate branch is of increased importance.
However, also the innate part is somewhat immature in neonates. There are fewer DCs in
newborns and they express lower levels of co-stimulatory molecules111. Possibly, the
production of Th1 associated cytokines is suppressed23. Actually, cord blood mononuclear
cells (CBMCs) produce less IFNγ, IL-12 and probably also less IL-1β after TLR ligation than
adult PBMC23, 118. The neonatal production of IL-6, IL-10 and IL-23 is possibly higher, after
38
TLR ligation in monocytes and APCs, compared to adult levels23, 118. This does not appear to
be attributed to the level of TLR expression, however, as neonatal and adult PBMC have
similar basal expression of TLRs19, 118. Neither does the type of delivery influence the
cytokine production by CBMC after TLR ligation118. The IL-6/TNF ratio produced by CMBC
is higher, after TLR ligation, than from PBMC119. This appears to be especially attributed to
factors in the serum of cord blood i.e. adenosine. It is not known for how long the circulating
levels of adenosine persist, but blood cells from 2 month- and 12 month-old infants produce
much lower levels of IL-6, IL-10 and TNF, after TLR ligation, compared to the cord blood
levels118. The high production of IL-6 at birth could be important for increasing acute phase
proteins23. This, together with the role of IL-6 in preventing neutrophil recruitment could
prevent too much inflammation when the neonate is exposed to colonizing microbes.
At birth, infants are coated with a waxy coating, the vernix caseosa23. As this waxy layer
contains several AMPs it is thought to be the first protection against colonizing microbes. A
majority of infants are colonized with coagulase-negative Staphyloccocus (CoNS) one day
after birth120. Not surprisingly, approximately half of all infants respond immunologically to
the colonization of their skin23. The benign rashes they develop are probably caused by the
CoNS, which penetrate the hair follicles, and the macrophages, eosinphils, neutrophils and
mast cells that then are recruited120. Macrophages produce IL-6 which further leads to the
production of acute phase proteins23. In all, this response is believed to be beneficial for the
maturation of the neonatal immune system.
Neonatal and infant immune responses in relation to subsequent allergy development
It is believed that a somewhat Th2 skewed immune system predisposes allergy
development121. Th1 cells secrete IFNγ which is able to counter-regulate Th2 responses. A
lower amount of Th1 cytokines therefore creates a milieu for allergic sensitisation. As the
neonatal immune system appears to be somewhat Th2 skewed (see above) the exposure to
microbial products early in life is central since it leads to activation of TLRs on e.g. innate
cells and subsequently to the development of Th1 cells1. The receptor Notch is expressed on
naïve T cells. When DCs encounter TLR ligands, they express Delta which binds to Notch
leading to Th1 differentiation122. It is assumed that more immature dendritic cells instead
express Jagged, leading to Th2 differentiation. It has been shown that substances mimicking
microbial products switch the allergen-specific response from Th2 to Th1 by increasing the

39
production of Th1 cytokines123. Also, mice with a deficient TLR4 receptor responded with
high IgE responses and anaphylactic shock when a food allergen coupled to an adjuvant was
administered 124. However, if the mice simultaneously were given CpG oligodeoxynucleotides
(mimicking bacterial DNA) no anaphylactic reactions were seen. T regulatory cells dampen
both Th1 and Th2 responses121. CD4+CD25+ T cells suppress proliferation of CD4+ and CD8+
T cells probably via cell-cell contact77. Tr1 cells also suppress T cell proliferation and appear
to switch antibody production away from IgE towards IgG4121. In addition, TGFβ inhibits
proliferation and differentiation of naive T cells77. Insufficient microbial stimulation can also
lead to poorer development of T regs. Ligation of TLR2 on T regs enhances their suppressive
activity50.
There might be a time window of opportunity when the exposure to microbes is essential for a
proper down regulation of Th2 responses125. Results from animal experiments support this
theory. In a murine model, Bifidobacterium (B.) infantis could restore oral tolerance in
neonatal ex-germ-free mice but not in adult mice126. Also, sensitisation at 2 years has been
shown to correlate with high amounts of Th2 cytokines produced by PBMC from 6 month-old
infants after allergen stimulation127. Although the above mentioned study could not show it,
there might also be an imbalance in cytokine and chemokine production in children
developing allergic disease already prenatally. One study showed a significantly lower
proportion of IL-12 producing CBMCs following allergen stimulation in children who
became IgE-sensitized at two years of age when compared to CMBC from non-sensitized
children128. Also, the ratio of CCL22 (a Th2 associated chemokine) to the Th1 associated
cytokines CXCL10 and CXCL11, is higher in cord blood of children who develop allergy at
two years of age129. Furthermore, the phytohemaglutamin (PHA)-induced expression of the
transcription factor GATA3 is higher in CBMC from infants who develop IgE-associated
allergic disease compared to CBMC from infants who remain non-allergic130. Studies from
our group also indicate an early immaturity of anti-microbial immune responses by
monocytes in children with allergic mothers, an impairment which seems to persist during the
first 2 years of life19, 131. Yet, it is rather the allergic status of the child, that influences
antimicrobial immune responses in monocytes at five years of age132. Others have shown that
exposure to house dust endotoxin and pets are associated with higher IFNγ production by
CMBC and infant PBMC after phorbol 12-myristate 13-acetate and Concavilin A stimuli133.
Probably are both the in utero environment and early repeated microbial stimuli important for
priming of immune responses.

40
Sensitized infants who develop allergic symptoms have lower levels of salivary SIgA
compared to sensitized infants who do not develop allergic symptoms (117, Tomicic et al
unpublished). Also, infants with IgA deficiency might be at increased risk for developing
allergic disease134. Furthermore, the allergen-specific IgA levels in feces are lower in a mouse
model with food allergy compared to tolerant mice135.

41
THE COMMENSAL GUT MICROBIOTA
It is estimated that the gut harbours 500-1000 different species of bacteria136. These species
belong to nine different phyla of bacteria with Firmicutes and Bacteroides being the most
predominant137. The total amount of gut bacteria is estimated to weigh approximately one kg
and outnumbers the number of cells in the human body by a factor of ten138, 139. The bacteria
are differently distributed along the gastrointestinal tract (Fig. 6), with few species in the
acidic stomach. The bacterial density increases in the small intestine and the colon harbours
the highest number of bacteria, 1012 colony forming units (CFU)/ml137. The gut harbours both
anaerobic and facultative anaerobic genera of bacteria but the anaerobes constitute the largest
proportion, approximately 99% in adults140. Bifidobacterium, Clostridium (C.), Bacteroides,
Lactobacilli (L.) and Eubacterium are common anaerobic genera of gut bacteria141.
Streptococcus, Enterococcus, Staphylococcus (S.) and Escherichia (E.), together with other
Enterobacteriaceae, are facultative anaerobic genera of gut bacteria.
A polysaccharide rich mucus gel layer is overlying the gut epithelium. This mucus layer
provides carbohydrate motifs that enable microbes to attach to the mucus and form
biofilms136. The biofilm promotes several of the functions exerted by the microbiota136. It also
makes the microbes resist the forces of gut peristalsis58. The gut microbiota has several
functions. It ferments non-digestible carbohydrates (see below) and synthesizes vitamins, e.g.
vitamin K and biotin. Apart from being important for immune system development (see
below), the commensal microbiota also protects the host from pathogens in additional ways.
Lactic acid producing bacteria, e.g. lactobacilli and bifidobacteria, lower the pH in the gut and
create a milieu less friendly for pathogens. The commensal microbiota also competes with
pathogens for nutrients and receptors.
Factors influencing the composition of the gut microbiota
The composition of the intestinal microbiota is rather stable in healthy individuals144. Thus,
adults are colonization resistant meaning that it is difficult for new strains to establish. This is
probably due to the vast amount of obligate anaerobes in the adult intestine140. However, the
gut microbiota can be altered by several factors like drugs, diet, stress, disease and aging.
Compared to the adult flora, the infant gut microbiota is less diverse. Mitsouka has studied the
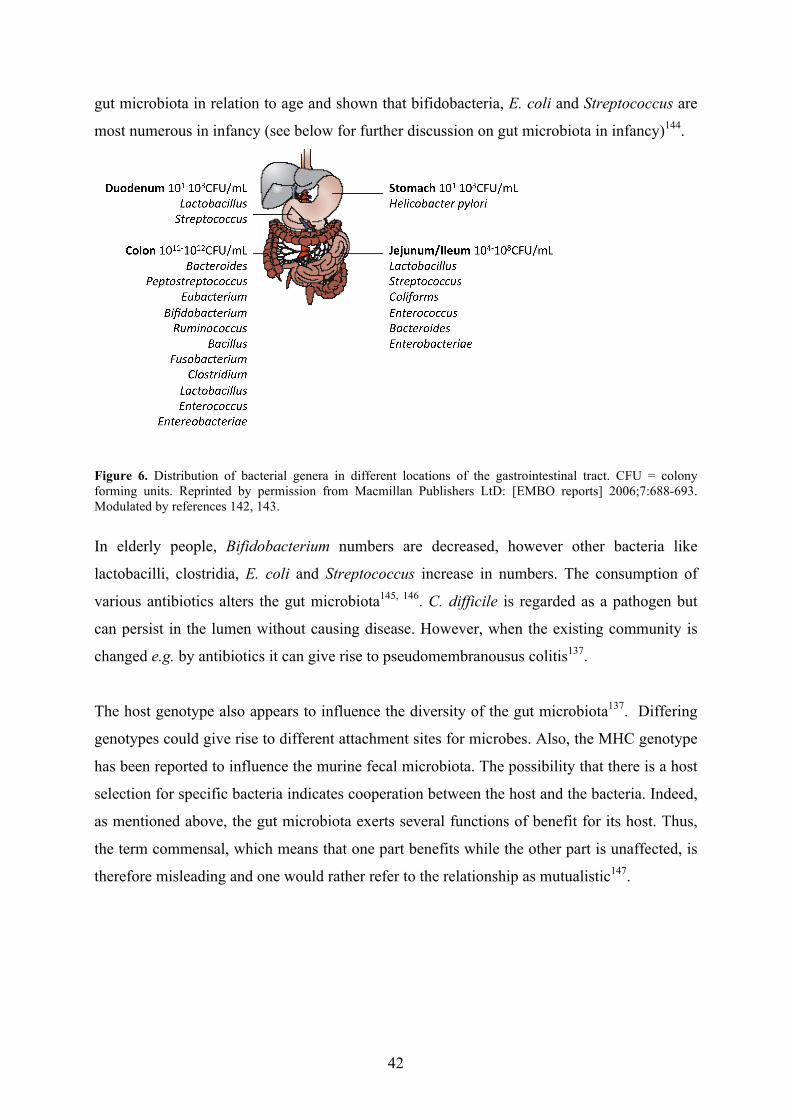
42
gut microbiota in relation to age and shown that bifidobacteria, E. coli and Streptococcus are
most numerous in infancy (see below for further discussion on gut microbiota in infancy)144.
Figure 6. Distribution of bacterial genera in different locations of the gastrointestinal tract. CFU = colony forming units. Reprinted by permission from Macmillan Publishers LtD: [EMBO reports] 2006;7:688-693. Modulated by references 142, 143.
In elderly people, Bifidobacterium numbers are decreased, however other bacteria like
lactobacilli, clostridia, E. coli and Streptococcus increase in numbers. The consumption of
various antibiotics alters the gut microbiota145, 146. C. difficile is regarded as a pathogen but
can persist in the lumen without causing disease. However, when the existing community is
changed e.g. by antibiotics it can give rise to pseudomembranousus colitis137.
The host genotype also appears to influence the diversity of the gut microbiota137. Differing
genotypes could give rise to different attachment sites for microbes. Also, the MHC genotype
has been reported to influence the murine fecal microbiota. The possibility that there is a host
selection for specific bacteria indicates cooperation between the host and the bacteria. Indeed,
as mentioned above, the gut microbiota exerts several functions of benefit for its host. Thus,
the term commensal, which means that one part benefits while the other part is unaffected, is
therefore misleading and one would rather refer to the relationship as mutualistic147.

43
Infant gut microbiota
The foetus is sterile in utero but the colonisation starts immediately after birth148. The first
colonizers are facultative anaerobes, e.g. E. coli and staphylococci, which consume oxygen140.
Anaerobes colonize the gut a few days after birth. These are e.g. Bifidobacterium,
Bacteroides, Clostridium and Lactobacillus species.
It has been shown that type of delivery influences the gut microbiota. Vaginally delivered
infants are exposed to the faecal, peritoneal and vaginal flora of the mother. Neonates born
with caesarean section are initially mainly exposed to bacteria in the hospital environment and
of nursing staff. Indeed, neonates born with caesarean section often harbour less
bifidobacteria and bacteroides145 and are colonised later with E. coli, lactobacilli, Bacteroides
and Bifidobacterium species149, 150. It can take up to over one month before infants born with
caesarean section have similar levels of these bacteria compared to those of vaginally
delivered infants150. A long-lasting vaginal delivery appears to increase the chance of finding
live bacteria in the mouth and stomach of newborn infants148. Infants raised in developed
compared to developing countries appear to have a different microbiota. A higher prevalence
of Ethiopian and Estonian infants, compared to Swedish infants, harbour lactobacilli151, 152.
Adlerbeth et al showed that Pakistani infants were colonised earlier than Swedish infants and
also harboured a more diverse enterobacterial microbiota153. The hygienic procedures in
developed countries might be responsible for these differences which also might have
unfavourable consequences (see below).
Bifidobacteria constitute a large proportion of the gut microbiota in infants154. Once fully
weaned, infants harbour a lower proportion of bifidobacteria. Studies investigating differences
in gut microbiota between breastfed and formula fed infants indicate that breastfed infants
harbour higher numbers of bifidobacteria155. However, there are less clear differences
between studies today compared to studies performed decades ago, suggesting that the
composition of formula has improved140. Clostridia have been found in higher numbers in
formula-fed infants. Streptococcus, Bacteroides and Enterobacteriaceae might also be higher
in formula-fed infants140, 148. In addition, microbiota associated characteristics appear to differ
between breast-fed and formula-fed infants156.

44
Fermentation, prebiotics and probiotics
Several attempts have been made to change the composition of the gut microbiota. As
mentioned above the diet could influence the gut microbiota. Non-digested carbohydrates like
dietary fibres, resistant starch and oligosaccharides reach the colon and are fermented by the
gut microbiota157. The end products produced following this fermentation are mainly short
chained fatty acids (SCFA) and gases (e.g. methane and CO2)158. The different degradation
enzymes and adhesion factors in various bacterial species determine their ability to ferment
different substrates. Lactobacilli, which occur in higher numbers in the small intestine,
preferentially ferment mono-, di- and tri-saccharides159. Bacteroides and bifidobacteria, which
are more abundant in the colon, are efficient at degrading complex carbohydrates. Genes
involved in poly/oligosaccharide metabolism have been shown to account for 8% of the
genome of B. longum while an even larger part of the genome of Bacteroides
thetaiotaomicron contains genes responsible for polysaccharide breakdown160. Bifidobacteria
and lactobacilli are producers of lactate and therefore often called lactic acid producing
bacteria144. Bifidobacteria also produce acetate. About 90% of the SCFAs in faeces of infants
below three months are acetic acid156.
Prebiotics are defined as “non-digestible food ingredients that beneficially affect the host by
selectively stimulating one or a limited number of bacterial species already resident in the
human colon”161. Prebiotics such as inulin and fructo-oligosaccharides have been shown to
function as substrates for bifidobacteria and lactobacilli and thereby increasing their growth,
but investigations on how the whole gut microbiota is affected by prebiotics are lacking. In
addition, much is still unknown about the substrate preferences by many bacterial species162.
Thus, prebiotics are probably not only degraded by the target bacteria but also by other
species. Furthermore, some species are unable to degrade complex carbohydrates and can
instead ferment the products produced by other species. This is termed cross-feeding. Also,
factors in the gut environment, e.g. pH, influence the metabolism of different bacteria.
Nevertheless, prebiotics have been shown to improve gut health by increasing faecal weight
and thereby increase gut peristalsis counteracting constipation163.
Probiotic bacteria are live orally administered bacteria with potential health benefits164.
Mainly species of bifidobacteria and lactobacilli have been used as probiotics. Probiotics have
been postulated to have many effects but are so far only concluded to have effects on lactose

45
intolerance (since they increase the concentration of lactase) and some types of diarrhoea.
However, there is no conclusive evidence that probiotics actually colonise the gut154.
Methods for studying the gut microbiota
Culture-dependent methods have been extensively used for analyses of the gut microbiota.
However, these methods are time-consuming and, importantly, not all species in the gut can
be cultivated159. In addition, it might be difficult to analyse different species, within a genus,
by cultivation. Sequencing of bacterial genomes made the use of molecular methods feasible.
It was shown that the genes for 16SrRNA contained conserved and variable regions. The
conserved regions have made it possible to design probes or primers to study domains of
bacteria while the variable regions made it possible to investigate different genus or species of
bacteria159. Several different techniques use the 16SrRNA genes. These include terminal
restriction fragment length polymorphism (TRFLP) and denaturing gradient gel
electrophoreses (DGGE). These techniques are useful for analysis of known species of
bacteria but also for analysis of diversity as they provide molecular fingerprints of the gut
microbiota. However, they have a rather low sensitivity and do not quantify bacterial
numbers165. Fluorescent in situ hybridisation (FISH) and Quantitative (Real-time) PCR uses
probes and primers to detect and quantify known species, groups or genus of bacteria.
Quantitative PCR can detect and quantify bacteria present in low numbers165. Yet, one
disadvantage with molecular methods is that they also detect dead bacteria.
Faecal samples are most widely used when studying the gut microbiota. However, different
bacteria adhere at various sites within the diverse compartments of the gut. Faecal samples
might thus not reflect the ecology in different parts of the gut165. Also, aerobe bacteria might
appear to exist in higher numbers when faeces are studied instead of biopsies from the more
anaerobe gut166. Another useful tool, for studying differences in the gut microbiota between
two populations, is to use microbiota-associated characteristics (MACs). This method
measures the function of the microbes since metabolic products, like short chained fatty acids,
are studied. Still, this method does not provide information of the presence and numbers of
certain bacteria.

46
Gut microbiota and immune responses
Germ-free (GF) animals have been used to investigate the role of the commensal microbiota.
These animals have alterations in their intestinal morphology and thicker muscle cell wall
compared to animals reared conventionally139,167. The large intestine of GF animals
accumulates mucus due to the lack of mucus-degrading enzymes and they therefore have a
larger caecum. Importantly, the immune system in these animals is altered compared to
conventionally colonized animals. Especially the GALT is less developed in GF animals with
few IgA producing B cells, less T cells and smaller, underdeveloped PPs and MLN´s61, 168. In
addition, CD4+CD25+ T cells from the GALT of GF mice elicits lower suppressor activity
than CD4+CD25+ T cells from conventional mice169. Other secondary lymphoid organs are
also affected. For example, the spleen of GF mice has been shown to contain fewer numbers
of CD4+ T cells170. In fact, the systemic immunity is affected i.e. with lower immunoglobulin
levels and GF animals are thus more susceptible to infections168.
Gnotobiotic animals are GF animals selectively colonized with one or more known bacterial
species168. The use of these animals makes it possible to study the effect of the commensal
microbiota or certain gut microbes on the immune system. After colonisation with commensal
bacteria, increased populations of IgA+ B cells can be detected and thus also increased
production of IgA167, 168.Germ-free mice appear to be somewhat Th2 skewed. They produce
low amounts of IFNγ and IgG2a but high amounts of IgE, IgG1 and IL-4 after tolerogenic
doses of ovalbumin (OVA) followed by a systemic challenge with OVA126. After introduction
with B. infantis, the IFNγ and IgG2a response is restored in neonatal mice but not in adult
mice126. This postulates a role for the commensal microbiota in early tolerance induction.
Interestingly, a polysaccharide from Bacteroides fragilis restores the proportion of CD4+ T
cells in the spleen of GF mice and drives the T cell development towards a Th1 phenotype170.
The commensal microbiota also appears to be important for intestinal homeostatsis171.
Following gut injury, mice with a disturbed gut microbiota produce less cytokines compared
to mice with a normal gut microbiota171. Also, in the same study it was shown that mice
deficient in MyD88 produce significantly less cytokines than wild type mice after gut injury.
Thus the activation of TLRs is central in the recognition of the commensal microbiota and
important for gut homestasis.
The immune modulatory capacity of probiotics has been studied in both mice and humans.
Yet, it is important to remember that humans and conventional mice are not gnotobiotic and it

47
can not be concluded whether the probiotic bacterium exerts the immune effects or whether it
alters the existing microbiota which in turn is responsible for the effects. As this thesis
focuses on how the very early gut microbiota influences immunity and allergy development, I
only discuss studies that have given the probiotic bacterium early. Mice given L. rhamnosus
GG or B. lactis directly from birth had higher numbers of TGFβ-secreting CD4+ cells in their
MLN´s and more Foxp3-expressing cells in their peribronchial lymph nodes compared to
untreated mice172. These mice also produced less total IgE and less OVA-specific IgE och
IgG2a. They also responded with lower production of IL-4, IL-5, IFNα and IL-10 to OVA.
Infants who received pro- and prebiotics showed higher regulatory responses, measured as
plasma IL-10, compared to placebo-treated infants. In addition, the pro- and prebiotic-treated
infants had higher plasma concentrations of C-reactive protein, total IgA and total IgE at six
months compared to the placebo group173. However, PBMC from six month old infants
receiving L. acidophilus since birth did not respond differently to allergens than PBMC from
placebo-treated infants174. Conflicting results could be due to the studies being performed in
mice versus humans. In addition, different stimuli and bacterial strains have been used. Also,
most studies have not investigated if the probiotic bacterium actually colonizes the infant gut.
It might thus be more relevant to investigate some of the gut bacteria species actually
colonizing the gut in relation to immune responses. Actually, early S. aureus colonization has
been shown to increase the plasma levels of sCD14175. Low levels of sCD14 have been shown
to be associated with allergic disease175.
Both in vivo and in vitro studies are necessary to study effects on the immune system
mediated by probiotics. However, when performing in vitro studies one might avoid the
confounding factors associated with in vivo studies. Commensal G+ and G- bacteria induce
different amounts of pro-inflammatory cytokines from human monocytes176. G+ bacteria
induce higher amounts of TNF whereas G- bacteria are better at inducing IL-6 and IL-8. In
comparison to monocytes, dendritic cells respond less to G+ bacteria177. Importantly, the
commensal bacteria are in contact with dendritic cells rather than monocytes. A study on
CBMCs reveals that both G+ and G- commensal bacteria are efficient in inducing sCD14 and
sCD83 production from dendritic cells175. Several studies show that certain strains of
lactobacilli (L. casei and L. rhamnosus) are less efficient in inducing activation markers on
dendritic cells compared to E. coli178 and Klebsiella pneumoniae179. Yet, within the genera of
lactobacilli strain-specific responses might occur as L. casei and L. reuteri, but not L.
plantarum, bind to the PRR DC-SIGN (dendritic cell-specific intercellular adhesion molecule

48
3-grabbing nonintegrin) and induce the maturation of T regulatory cells180. Also, several
strains of lactic acid bacteria, but not all, induce IL-10 production from PBMC and down-
regulate Th2 cytokine production after PHA stimulation181. Diverse Bifidobacterium species
have also been shown to induce activation markers (CD83, CD86) on DCs generated from
PBMCs182. Also, B. bifidum, B. longum and B. pseudocatenulatum induce IL-10
production182.
Gut microbiota and allergy
The gut microbiota could have changed according to increased hygienic conditions. There
appears to be an early colonisation with “skin bacteria” like Staphyloccous today compared to
decades ago183. Also, differences in gut microbiota between children from affluent countries
compared to children from developing countries postulates a role for increased hygiene as a
modulator of the gut microbiota151-153. Differences in gut microbiota have also been shown
between children raised with an antroposofic lifestyle with more fermented food and less use
of antibiotics146. Antroposophic children less often develop allergies compared to children
raised during conventional conditions184.
In the late 1990´s studies postulated a role for the gut microbiota in relation to allergic
disease. Children who were allergic at two years of age were less often colonised with
bifidobacteria and lactobacilli whereas they had higher counts of coliforms and S. aureus185.
Another study found that colonisation with B. adolescentis, was more common in children
with atopic allergies as compared to non-allergic children who were colonised with B.
infantis, B. bifidum and B. breve to a higher extent186. However, Murray et al did not see any
differences, regarding species of bifidobacteria, when they compared the faecal microbiota
between sensitized wheezy and non-sensitised non-wheezy children187. Yet, they found that
children with eczema had lower counts of bifidobacteria. Thus, there might be a difference in
the gut microbiota between allergic and non-allergic children.
Nevertheless, these studies do not address whether it is potential differences in the infant gut
microbiota that drives development of allergic disease or if allergic disease might influence
the gut microbiota. Therefore it is relevant to study the infant gut microbiota in relation to
subsequent allergy development. Such prospective studies have mainly focused on genera of
bacteria and show interesting but not quite concurrent results. One study showed that children

49
who had become allergic at the age of two years were less often colonised with enterococci
and bifidobacteria but more frequently colonised with S. aureus and had higher counts of
clostridia already as infants138. Kalliomäki et al also showed that children who had become
allergic at 12 months of age had higher counts of clostridia at three weeks of age188. No other
genera of bacteria appeared to differ but the fatty acid profile of bacteria were different
between the two groups suggesting that children who develop allergic disease have a different
gut microbiota composition. A large study by Adlerbeth et al showed that increased total IgE
in serum at 18 months correlated with later colonisation by lactobacilli species149. However,
no other bacteria were associated with allergy development or total IgE. Lately, the KOALA
study showed alterations in C. difficle and E. coli colonisation at 1 month in children who
developed allergy during their first 2 years189. However, no alterations in total
bifidobacteria189 or at Bifidobacterium species level190 were seen between infants who
developed allergy compared to infants who did not. Evaluation of allergic outcome was
performed early in all of these studies (at 12, 18 or 24 months). During this time allergic
disease is mainly manisfested in the skin and gut and later allergic disease, i.e. respiratory
allergy, was not considered in these studies.

50
IMMUNOLOGY OF HUMAN MILK
Human milk is the ideal nutrition for infants. It contains optimal proportions of the
macronutrients; carbohydrates, lipids and proteins, as well as micronutrients such as vitamins
and minerals. Apart from containing nutrients important for the growth of the infant, human
milk also contains several immunomodulatory components191. As the immune system of the
infant is far from developed at birth (see above), human milk IgA, lactoferrin,
oligosaccharides, leukocytes, cytokines and lysozyme play a substantial role in protecting the
infant from pathogens192. Since the lactating mammary glands belong to the mucosal immune
system, the human milk antibodies reflect maternal MALT-encountered antigens193.
Therefore, the SIgA in human milk protects the infant from the antigens the mother has been
exposed to.
Several different leukocytes are present in human milk192. They are most predominant in
colostrum and decrease during the course of lactation. Macrophages and neutrophils are most
common but also lymphocytes, mainly T cells, are present. The human milk macrophages
express activation markers and could thus theoretically activate the infant’s lymphocytes,
while the role of the neutrophils in human milk is not known.
Both anti-inflammatory (e.g. IL-10, TGFβ) and pro-inflammatory (e.g. IL-1β, IL-6, IL-8,
TNF) cytokines are present in human milk191, 192. They mainly arise from production in the
mammary gland, although the leukocytes in human milk contribute to the production of
cytokines192. The physiological role of these cytokines is not completely understood since it is
not known to which extent the cytokines survive the passage through the stomach. Still the
cytokines in human milk could be of importance for the development of the immune system
in infants (see below).
Lactoferrin is a major protein in human milk194. It chelates free iron leading to increased
absorption of iron for the infant as well as making this nutrient unavailable for bacteria.
Another AMP in human milk is lysozyme which is able to break bonds in peptidoglycan.
51
Exosomes have also been found in human milk195. These human milk exosomes have been
found to increase the development of Foxp3+CD4+CD25+ T regulatory cells from PBMCs and
also to regulate the production of several pro-inflammatory cytokines.
Breast feeding in relation to allergy development
It has been estimated that 13% of the world deaths of children below five could be prevented
if the World Health Organisation’s breast-feeding guidelines (exclusive breastfeeding during
the first 6 months) were followed191. However, the role of breastfeeding in allergy prevention
is controversial. One meta-analysis, regarding exclusive breastfeeding for the first 3 months,
pointed at a decreased risk of breastfeeding on development of allergic rhinitis196. The effect
was however not that pronounced for children with atopic heredity. Kull et al showed that
exclusive breastfeeding for 4 months or more decreased the risk of developing eczema and
asthma197, 198. However, another large Swedish study demonstrated that breastfeeding did not
protect children from atopic dermatitis during their first year199. Therefore, it is debated
whether the different immunomodulatory components in human milk differ between mothers.
Indeed, some studies show that low levels of SIgA are associated with increased risk of cow’s
milk allergy in infants, however not all studies confirm this200. The composition of
polyunsaturated fatty acids in milk might differ between allergic and non-allergic mothers and
could also be related to allergy outcome in children201. The levels of cytokines might vary
between allergic and non-allergic mothers with significantly higher IL-4 concentrations in the
milk from allergic mothers202. A recent study from our group indicates that mothers with
higher exposure to infections, before the age of ten, have increased levels of TGFβ1, IL-6 and
IL-8 in their breast milk203.
Ovalbumin allergen has been found in the milk of lactating mice exposed to OVA204.
Interestingly, the mice fed by OVA exposed mothers were protected against asthma as shown
by e.g. decreased airway hyperreactivity, lower number of eosinophils in the broncoalveolar
lavage and less IL-4 producing CD4+ T cells. Both the presence of TGFβ in the milk and the
TGFβ signalling by T cells appeared to be responsible for the tolerance induction. Levels of
allergens like casein, egg proteins and peanut proteins have also been detected in human milk.
However whether they cause tolerance induction in humans is not known200.

52
Human milk oligosaccharides
Human milk oligosaccharides (HMOs) are the third most abundant solid component in human
milk after lactose and lipids205. Colostrum contains roughly 20g HMOs/L while the
concentration in mature milk is lower, 12-14g/L206. HMOs are complex carbohydrate
structures (3-10 monosaccharide units) that are synthesised in the mammary gland by
glycosyl- and fucosyltransferases207. HMOs contain lactose in the reducing end206, 208. Lactose
consists of the two monomers D-glucose and D-galactose. Other monomers of HMOs are N-
acetylglucosamine, L-fucose and sialic acid. Different enzymes combine these monomers into
manifold structures. Approximately 130 different HMOs have been characterised so far209. Of
these are roughly 90 % neutral and the rest acidic. It is the secretor status and the Lewis blood
group of the mother that determines the pattern of oligosaccharides in the breast milk and at
least four different HMO patterns exist209. Approximately 77% of Caucasians are secretors
meaning they have the enzyme α1-2 fucosyltransferase208. This enzyme is needed for the
formation of 2-fucosyllatose (2-FL) and lacto-N-fucopentaose I (LNFP I). Non-secretors
therefore lack these HMOs. Other common HMOs are Lacto-N-tetraose (LNT) and Lacto-N-
neo-tetraose (LNnT) which form core structures important for longer HMOs like LNFP I, II,
III and Lacto-N-difuco-hexaose I (LNDFH I). 2-FL together with 3-Fucosyllactose (3-FL)
and Lactodifucotetraose (LDFT) are shorter oligosaccharides.
The HMOs have been shown to be resistant towards digestive enzymes and therefore reaches
the intestines intact210. The high concentrations of HMOs combined with the fact that they are
resistant to digestion have raised the question of the function of these glycans. Several studies
postulate two important functions of these oligosaccharides194, 209. The HMOs are assumed to
be the major components responsible for the differences seen between breastfed and formula
fed infants (see above)209. HMOs function as the first prebiotics since they are fermented by
bacteria like B. infantis211. The N-acetyl-glucosamine containing oligosaccharides have been
shown to be essential for the growth of a subspecies of B. bifidum212. Also Coppa and
collegues have shown that high concentrations of oligosaccharides in milk correlate with a
higher diversity of Bifidobacterium species207.
Interestingly, HMOs also appear to act as anti-adhesion agents inhibiting pathogens from
binding to gut epithelial surfaces123, 205. The glycosyl- and fucosyltranferases that synthesise
HMOs are also responsible for the formation of the glycans present on different cell types.
Therefore HMOs resemble glycans on human cells. Pathogens use these glycans to adhere to

53
epithelial cells. When free HMOs are present in the gut lumen the pathogens bind to these and
therefore HMOs decrease the infection load of orofeacal pathogens. Indeed, HMOs have been
shown to protect infants from infectious diarrhoea213. High concentrations of α1,2-linked
HMOs have been shown to be most protective.

54
PRESENT STUDY
AIMS
Previous studies suggest that the infant gut microbiota is important for maturation of the
immune system and subsequent allergy development. The overall aim of this thesis was
therefore to further investigate how the infant gut microbiota influences childhood immune
responses and allergy development. In addition, the role of breast feeding in allergy
prevention is debated. As human milk oligosaccharides might stimulate the growth of certain
species of the gut microbiota, the consumption of these was investigated for their role in
allergy development. Furthermore, other factors, negatively associated with allergy
development, were investigated for their influence on certain species of the early infant gut
microbiota.
The specific aims of each study were to:
Study I:
• Investigate whether the colostrum from allergic and non-allergic mothers differ in
composition regarding neutral oligosaccharides.
• Study if there is a difference in the consumption of colostrum oligosaccharides
between neonates who at the age of 18 months had developed allergic disease
compared to neonates who had not developed allergy at 18 months.
Study II:
• Examine the presence and amounts of four Bifidobacterium species, 2 groups of
Lactobacilli, C. difficile and Bacteroides fragilis in infant faecal samples collected at
one week, one month and two months of age and relate to the development of allergic
disease in these children up to five years of age.
• Investigate whether these early infant gut microbiota species are influenced by the
exposure to environmental factors i.e. endotoxin, Fel d 1 and family size.
Study III:
• Examine whether early colonization with the above mentioned species of bacteria
influences childhood mucosal immune responses i.e. salivary SIgA.
• Investigate whether early colonization with these bacteria influence systemic immune
responses in terms of spontaneous TLR2 and TLR4 mRNA expression and LPS-
induced cytokine production by PBMC collected 12 months after birth.

55
MATERIAL AND METHODS
The methods used are listed below and further discussed in each paper:
Study I:
• Gel permeation chromatography for separation of colostrum carbohydrates according
to size.
• High performance liquid chromatography (HPLC) for analysis of neutral HMOs (tri-
to hexasaccharides).
Study II and III:
• Extraction of nucleic acids from faecal samples collected one week, one month and
two months after birth.
• Real-time PCR for analysis of C. difficile, B. adolescentis, B. longum, B. bifidum, B.
breve, lactobacilli group I (comprising L. rhamnosus, L. casei and L. paracasei),
lactobacilli group II (comprising L. gasseri and L. johnsonii) and Bacteroides fragilis.
Study II:
• Limulus Amebocyte Lysate (LAL) assay for quantification of house dust endotoxin.
The house dust was collected from carpets once when the children were between 3-12
months old.
• Enzyme-linked immune sorbent assay (ELISA) for quantification of house dust Fel d
1.
Study III:
• ELISA for quantification of salivary SIgA. The saliva was collected at age six and
twelve months and two and five years.
• Real-time PCR for quantification of TLR2 and TLR4 mRNA expression in PBMC
collected 12 months after birth.
• Luminex for analysis of LPS-induced cytokine and chemokine production (IL-6,
CXCL8 (IL-8), IL-10, IL12p70, IL-17, IL-1β, CCL2 (MCP-1), CCL4 (MIP-1β), TNF)
from the above mentioned PBMC.
The statistical analyses are described in each paper.
56
The different study populations are described below. The studies were approved by the
Regional Ethics Committee for Human Research at Linköping University.
Study population study I
Mothers attending the Antenatal Health Care Centres in Linköping August 1993 to March
1996 and in the beginning of 2004 were invited to participate in a prospective study of the
development of atopic symptoms in relation to environmental factors and maternal immunity.
The children were born between January 1994 to July 1997 and June to October 2004. All the
children were delivered at term and they had an uncomplicated perinatal period. Mothers who
breastfed their babies for less than 3 months were excluded.
Clinical examinations and SPT against fresh hen’s egg, milk and extracts from cat and peanut
(ALK, Denmark) were carried out at 6, 12 and 18 months of age, and whenever allergic
symptoms were suspected. At these appointments the parents also completed a questionnaire
regarding e.g. clinical symptoms. In all studies, SPT was considered to be positive if the mean
diameter of the wheal reaction was ≥3 mm. Atopic eczema was defined as pruritic chronic or
chronically relapsing dermatitis with typical morphology and distribution214. Food allergy was
defined as a positive skin prick test, combined with a positive clinical history of immediate
skin and/or gastrointestinal reactions or atopic symptoms upon exposure to a certain food and
clinical remission of atopic symptoms on an exclusion diet. Breast-feeding was defined as
exclusive when all cow’s milk formula, except for extensively hydrolysed formula (i.e.
Nutramigen™, Bristol Meyers), were avoided.
The diagnosis of atopy in the parents was based on a convincing clinical history of bronchial
asthma, allergic rhinoconjunctivitis, atopic eczema and/or food allergy. The mothers were
classified as allergic if they showed clinical symptoms of allergic disease and had circulating
IgE antibodies against a panel of common allergens, measured with allergy screen test (Magic
Lite™, ALK, Hørsholm, Denmark) or Phadiatop (Pharmacia CAP System RAST FEIA,
Pharmacia Diagnostics AB, Uppsala, Sweden). Mothers not reporting clinical symptoms of
allergy and having a negative allergy screen test or Phadiatop were classified as non-allergic.
Children were classified as non-allergic when they did not show any symptoms of allergy and
had a negative SPT. Children were classified as allergic if they showed clinical symptoms of
allergic disease.
57
From the original study population, we randomly selected 20 women (11 allergic and 9 non-
allergic) and 20 children. Eleven of these children were non-allergic and nine showed
symptoms of atopic eczema, food allergy or both (see paper I).
Study population study II and III
The study population, including 123 Swedish children, has been described in detail by Voor et
al215. The children were born between March 1996 and October 1999 in Linköping, Sweden.
All were born at term and they had an uncomplicated perinatal period.
A clinical examination of the babies was made at three, six and twelve months and at two and
five years. At these occasions, skin prick tests were performed, and questionnaires were
completed regarding e.g. symptoms of allergy, use of antibiotics and family size. Atopic
dermatitis was defined as in study I. Asthma was defined as three or more episodes of
bronchial obstruction during the last 12-month period, of which at least one should be verified
by a physician. Allergic rhinitis/conjunctivitis was defined as rhinitis and/or conjunctivitis
following at least twice in one hour after allergen exposure and not in relation to an obvious
infection e.g. fever or a cold. SPTs, with fresh skimmed cow’s milk and thawed egg white,
were performed at all follow ups. From 12 months, the children were tested with cat allergen
extract and at two and five years also with birch- and timothy extracts (ALK, Hørsholm,
Denmark).
Inclusion in study II was based on availability of faecal samples at one week, one month
and/or at two months of age and known allergy status up to the age of five. The children were
classified as allergic and non-allergic based on symptoms and SPT. Thus, the allergic children
had shown symptoms of allergic disease and at least one positive SPT during their first five
years of life, while the non-allergic children had not shown symptoms of allergic disease, nor
had a positive SPT. Therefore, 47 infants were included. Sixteen children were classified as
allergic and 31 as non-allergic. For demographic data of these children see table 1 in paper II.
The demographic data did not differ between the allergic and non-allergic group.
Inclusion in study III was based on availability of faecal samples at one week, one month
and/or at two months of age as well as blood samples collected at twelve months, and/or

58
salivary samples, collected at six months, twelve months, two years and/or five years. As
known allergic status during the first five years was not an inclusion criterion, additional
children, compared to study II, could be included. In all, 64 infants were included; this group
included all 47 subjects in study II. The demographic data of all 64 children is shown in table
2.
Table 2. Demographic data of the subjects.
AD= Atopic dermatitis, AB= Asthma bronchialis, ARC= Allergic rhinitis/conjunctivitis, SPT= Skin prick test a = missing data for one subject regarding exclusive breastfeeding. b = missing data for three subjects regarding number of family members and thus household area/individual. c= six children had left the study at five years of age.
A majority of the children had a history of atopic disease in the immediate family (78%,
Table 2). In total, three children were delivered with caesarean section. Most infants were
exclusively breastfed during their first three months (83%) and only two infants received oral
antibiotics during this time. Seventeen children (27%) were sensitized during their first five
years of life. A majority of these children showed SPT reactivity to food allergens before five
years (12 children). Also, at five years of age, ten of the sensitized infants were SPT positive
to inhalant allergens. Twenty-one children had atopic dermatitis during their first five years of
life. At age five, seven children had allergic rhinitis/conjunctivitis either in combination with
asthma (four) or without (three). Two children had asthma in combination with atopic
dermatitis and four children had asthma alone.
Subjects n=64
%
Female subjects 32 (50%) Born with caesarean section 3 (5%) Any atopic heredity 50 (78%) Exclusively breastfed ≥ 3 months 53 (83%)a Oral antibiotics ≤ 3 months 2 (3%) Pets 11 (17%) Number of family members 3 (3-8)b Household area/individual (m2) 29 (18-75)b AD cumulative five years 21 (33%)c AB cumulative five years 10 (16%)c ARC cumulative five years 7 (13%)c SPT cumulative five years 17 (27%)c

59
RESULTS AND DISCUSSION
Human milk oligosaccharides in colostrum of allergic and non-allergic women (I)
Some components in human milk might differ between allergic and non-allergic mothers201,
202. Oligosaccharides are the third most abundant solid component in human milk205 and
appear to be resistant towards digestive enzymes210. Thus, they reach the intestines intact
which postulate a significant role for the HMOs in the intestine. In order to investigate
whether maternal allergy influences the content of these, the concentration of the neutral
oligosaccharides LNDFH I, LNFP I, LNFP II, LNFP III, LNT, LNnT, 3-FL, 2´-FL and LDFT
were analysed in colostrum samples from allergic (n=11) and non-allergic (n=9) women. The
colostrum samples were collected at the same time of the day and at the same time in the
lactation period; 2-4 days post partum. In accordance with previous studies213, 216, 217, 2´-FL
and LNFP I were the most abundant neutral oligosaccharides. There was no difference in the
amount of neutral oligosaccharides in the colostrum from allergic compared to non-allergic
mothers (see table 2 in study I). This suggests that the amount of neutral oligosaccharides in
human milk is not influenced by the allergy status of the mother.
Although there was no difference in HMO concentration between colostrum of allergic and
non-allergic women, the variation in oligosaccharide concentration in milk from different
women was immense. This variation is in accordance with previous studies and partly
depends on the secretor status, the ABO- and Lewis blood group types218. Actually, the
production of HMOs is catalyzed by the same enzymes, glycosyltransferases including
fucosyltransferases, which are involved in the production of cell surface glycoconjugates. On
erythrocytes these conjugates determine blood group type218 and on other cell types they
function as receptors for particles and pathogens. Due to their structural resemblance with
these cell surface glycoconjugates, the HMOs might prevent the binding of certain pathogens
to the mucosa, thus lowering the infection rate by these pathogens205, 210. Indeed, high
amounts of α1,2-linked fucosylated oligosaccharides appears to protect the infant from
several types of diarrhoea213. Therefore, variation in HMO concentrations might be of
importance for other diseases.

60
Colostrum oligosaccharide concentrations in relation to subsequent allergy development
(I)
The HMOs might function as the first prebiotics by increasing the growth of certain
commensal gut bacteria209, 211. Furthermore, the gut microbiota might be altered in children
developing allergic disease138, 188, 189. Thus, we studied the concentrations of the above
mentioned oligosaccharides in colostrum samples and related these data to allergy
development at 18 months. Our results indicate that children who had developed allergic
symptoms at the age of 18 months tended to have consumed colostrum with higher
concentrations of neutral oligosaccharides in total, although the difference did not reach
statistical significance (p=0.12). This tendency could however not be attributed to any specific
neutral oligosaccharide. The fact that oligosaccharides in human milk act as receptor
homologues213, 218 and thus prevent pathogens from binding to the cells in the mucosa implies
that a high amount of neutral oligosaccharides protects against orofecal pathogens.
Interestingly, it has been shown that infections with food and orofecal pathogens were able to
reduce the risk of atopy with 60%103. Accordingly, the ability of human milk oligosaccharides
to bind pathogens and serve as anti-infective agents might influence allergy development
more than their ability to stimulate gut microbiota-immune interactions. Still, others have
shown that infants who received formula supplemented with prebiotic galacto- and fructo-
oligosaccharides had less atopic dermatitis during their first six months compared to infants
who received standard formula219. In addition, the prebiotic group had more bifidobacteria in
their faeces. Probably, additional studies are of importance for investiging the role of HMOs
and prebiotics on allergy development.
Early infant gut microbiota (II and III)
The commensal gut microbiota appears to be important for oral tolerance induction and gut
homeostasis126, 171. Previous studies have shown differences in the infant gut microbiota
between children who develop allergic disease compared to children who do not138, 188, 189.
However, this has not been confirmed by others149. In order to investigate whether early infant
gut microbiota is related to allergy development and immune maturation, faecal samples were
collected from infants (n=64) at one week, one month and two months after birth. Real-time
PCR was employed for analysis of the following bacterial species; C. difficile, B. bifidum, B.
longum, B. adolescentis, B. breve, Bacteroides fragilis, Lactobacilli group I (L. rhamnosus, L.
paracasei, L. casei) and Lactobacilli group II (L. gasseri, L. johnsonii). The Lactobacilli and

61
Bifidobacterium species were chosen due to their abundance in early faecal samples from
infants220, 221 and their postulated role in allergy development222. Also, C. difficile has been
associated with allergy development189. Furthermore, a component from Bacteroides fragilis
has recently been shown to be a potent immunomodulator170 and thus this bacteria was also
included.
Table 3. Proportion of infants (%) colonized with Bifidobacterium (B.), Lactobacillus, Clostridium (C.) difficile and Bacteroides fragilis during the first two months of life. The numbers in the headers show the number of infants with available faecal samples at the different time points. The figures, after the different bacteria, show the percent of infants who were colonized with the bacteria. Bacteria
1 week n=52
1 month n=56
2 months n=56
B. longum 88 91 91 B. adolescentis 71 66 75 B. bifidum 56 63 63 B. breve 40 43 50 Lactobacilli group I 31 57 57 Lactobacilli group II 33 43 54 C. difficile 6 11 21 Bacteroides fragilis 60 55 55
Bifidobacteria were detected in all infants in at least one of the three samples collected during
the first two months of life (Table 3). Compared to studies using cultivation to detect bacteria
this prevalence of bifidobacteria is high138. However, other studies using molecular methods
find bifidobacteria in most faecal samples from one- month old infants189, 223. Bifidobacterium
longum, which includes B. infantis, was the most prevalent Bifidobacterium species in the
infant faecal samples, which is in accordance with previous findings221, 224. Also B.
adolescentis was common, which is in agreement with some 223, 225 but not other previous
studies221, 224. Bifidobacterium breve was the least common of the Bifidobacterium species.
Both Lactobacilli group I and Lactobacilli group II were present in the early faecal samples.
Others have shown that Swedish infants harbour lactobacilli species, belonging to these
groups, during their first two months220. Few infants were colonised with C. difficile. Yet, C.
difficile appears to be more common in later infancy as 59% of 12 month- old infants harbour
this bacterium (Johansson et al unpublished). The two infants who received antibiotics (Table
2) harboured few Bifidobacterium species. However, DNA from Bacteroides fragilis
constituted a major fraction of the nucleic acids purified from the faecal samples of these
children (close to one percent). Actually, strains of Bacteroides fragilis are resistant to several

62
different antibiotics226. Two of the three children who were born with caesarean section
harboured C. difficile. Others have reported that infants born with caesarean section harbour
C. difficile more often than vaginally delivered infants227. The samples from the children who
were not exclusively breastfed did not appear to differ from the samples from exclusively
breastfed children.
Early infant gut microbiota in relation to allergy development (II)
Infants who developed allergic disease were, as one-week old infants, less often colonized
with Lactobacilli gr. I and B. adolescentis compared to infants who remained non-allergic
(p=0.02 and p=0.03, Fig. 7).
Figure 7. Proportion of infants (%) colonized with Lactobacilli gr. I and Bifidobacterium (B.) adolescentis during the first two months of life. Allergic infants developed allergy during their first five years while non-allergic infants did not.
Also, B. adolescentis, Lactobacilli group I, and C. difficile were less often detected in the
three samples, obtained during the first two months of life, from allergic infants than in the
samples from non-allergic infants (p=0.045, p=0.02 and p=0.03 respectively, Fig. 8). This
suggests that persistent colonisation with these species are of importance. The colonization
pattern of the other bacteria was similar in infants who did and did not develop allergy (see
Table 3 in study II).

63
Figure 8. Number of occasions with detectable Bifidobacterium (B.) adolescentis, Lactobacilli group I and Clostridium (C.) difficile during the first two months of life in relation to allergy development up to age five. The y-axis shows the percentage of infants who did (A, n=11) or did not develop allergy (NA, n=21) during their first five years of life. The bacteria were studied on three occasions during the first two months and the x-axis illustrates the number of occasions with detectable bacteria. As calculated with Mann-Whitney U test, the non-allergic children harboured B. adolescentis, Lactobacilli gr. I and C. difficile on more occasions than the allergic group (p=0.045, p=0.02 and p=0.03 respectively). None of the other investigated bacteria occurred at different occasions between the allergic and the non-allergic group. Children are only included if faecal samples from all occasions were available.
The early infant gut microbiota has been related to allergy development during the first two
years of life, in most previous studies138, 149, 189. At this age, allergic manifestations are mostly
limited to the skin and gut. The children in our study were followed to the age of five, i.e. to
an age when respiratory allergy and sensitization to inhaled allergens have become the major
clinical manifestation of allergy. We further subdivided the allergic children (who were all
SPT+ as previously mentioned) according to their clinical symptoms. Nine children were
included in the atopic dermatitis only group (AD only) and seven children in the allergic
rhinitis/conjunctivitis and/or asthma ever group (ARC/AB ever). As shown for the total
allergic group, the AD only group were less frequently colonized with Lactobacilli group I
one week after birth compared with the non-allergic group (p=0.03). This should be
considered in the context of clinical studies, in which different strains of probiotic lactobacilli
reduced the incidence of infant eczema228 and IgE-associated eczema229, 230. Importantly,
preliminary data from a cohort from Sachs’ Children’s hospital also indicate that children

64
who are sensitized and develop allergic symptoms before the age of five are less frequently
colonized with Lactobacilli gr. I during their first two months, compared to non-allergic
children (p=0.06-0.13) (Johansson et al unpublished). In addition, infants to allergic mothers
have a delayed colonization with Lactobacilli gr. I (Johansson et al unpublished). The primer
Lactobacilli gr. I detects L. rhamnosus, L. casei and L. paracasei. Interestingly, Lactobacillus
rhamnosus stimulated DCs have been shown to induce hyporesponsive T cells231. Also, L.
reuteri and L. casei bind to the PRR DC-SIGN (dendritic cell-specific intercellular adhesion
molecule 3-grabbing nonintegrin) on DCs leading to priming of IL-10 producing T regs180.
These studies thus provide mechanisms supporting our findings. Yet, bacterial colonization in
the seven children with respiratory allergy did not differ from bacterial colonization in the
non-allergic children. It is difficult to interpret the role of Lactobacilli group I on respiratory
allergies as only one child developed respiratory allergy without previous atopic dermatitis.
Furthermore, only seven children had developed allergic asthma and rhinitis/conjunctivitis at
age five. Children belonging to the AD only group, at age five, might develop respiratory
allergy later as a substantial proportion of sensitized children with atopic eczema develop
respiratory allergy before age seven232.
Bifidobacterium adolescentis was more commonly detected in infants not developing allergic
disease. In addition, the AD only group tended to be less frequently colonized with B.
adolescentis one week after birth compared with the non-allergic group (p=0.06). This is in
contrast to findings by others where no difference was observed regarding early B.
adolescentis colonization between the infants who did or did not develop allergic disease190,
225. Colonization with B. catenulatum (at one month) and B. bifidum (at three and six months)
was however more common among the infants who developed allergic disease225. However,
in these reports, allergy development was investigated early, at six225 and twelve months190,
and a follow up of the children in these studies might show different results. Others have
shown differences in Bifidobacterium composition between allergic and non-allergic
infants186, 233 and children234, where B. adolescentis186, 234 and B. pseudocatenulatum233 were
more frequently detected in the allergic individuals. However, these are all investigations of
the gut microbiota in children with an already manifested allergic disease in contrast to our
prospective study. Different Bifidobacterium species elicit distinct immune responses from
diverse immune cells182, 235. Hence, the early Bifidobacterium colonization could thus have
the potential to influence immune responses during the postulated short period early in life
when the immune system might be matured in order to prevent allergy development125.

65
Studies investigating gut microbiota composition when the disease is already established
might primarily indicate that individuals with allergic disease provide a different
gastrointestinal milieu, favouring growth and attachment of certain species of bacteria.
Certain bacterial species appear to be associated with allergic disease when the gut microbiota
is less diverse, exemplified by C. difficile. Previous studies suggest that colonization early in
life with C. difficile is more common among infants who develop allergic disease than among
infants who do not189. We could not confirm this, as infants who developed allergy were less
likely to be colonized with C. difficile during their first two months. The low rate of C.
difficile colonization combined with the relatively few number of allergic children may
explain the lack of a reverse association in our study. Nevertheless, several studies, in which
clostridia is more abundant in allergic infants, also indicate low prevalence of some other
commensal bacteria in children developing or suffering from allergy138, 188, 236. Prevalence of
non-toxigenic and toxigenic C. difficile colonization at one month is associated with eczema
and wheeze, respectively227. Interestingly, both non-toxigenic and toxigenic C. difficile
colonization is associated with formula feeding and caesarean section, early factors which are
associated with a less diverse microbiota. Therefore, it might rather be a gut microbiota with
lower diversity that is associated with allergy development. Interestingly, a large recent study
did not find any relationship between the presence of different bacteria and allergy
development up to 18 months of age149, but indeed showed that infants who developed allergy
had a lower diversity in their gut microbiota237. Additional prospective studies investigating
the microbiota before the onset of allergic disease in combination with mechanistic studies are
important for understanding the role of the gut microbiota, or certain gut microbiota species,
on allergy development.
Environmental factors influence the early infant gut microbiota (II)
Type of delivery, diet and country of birth influence the infant gut microbiota145, 149, 151-153.
Yet, other factors might also contribute to the colonization of the infant gut. We investigated
whether lifestyle factors, inversely related to allergy development, influence the early
colonization of the above mentioned species. Information about number of family members
was collected through questioners. Dust samples were collected from the infant’s homes and
analysed for endotoxin and Fel d 1 with LAL and ELISA, respectively. Number of
Bifidobacterium species at one week and two months correlated significantly with number of

66
family members (Fig. 9). Considering that higher counts of bifidobacteria145 and later
acquisition of Clostridium species in infants with siblings149 have been reported, family
members and siblings may rapidly contaminate the infant with a commensal microbiota.
Figure 9. Larger household size was associated with additional number of Bifidobacterium species in the faecal samples collected one week and two months after birth (a and b). Although displaying the same trend, no significance was seen in the one month samples (see study II). The x-axis shows number of family members and the y-axis the number of Bifidobacterium species in the infant faecal samples. The p-values indicate the trend after Cuzick´s non-parametric test for trend.
Colonization with several (3-4) Bifidobacterium species, at one week and two months of age
tended to be associated with exposure to higher levels of endotoxin than colonization with
low numbers (0-2) of Bifidobacterium species (Fig. 10). This was particularly obvious during
the first week of life (Fig. 10b). There was no similar correlation with the Fel d 1 levels in
house dust. Endotoxin is a component in G- bacteria and should probably be viewed as a
marker of total bacterial exposure in the homes and not as a factor directly related to the G+
bifidobacterial microbiota. However, postnatal colonization with the G- and facultative
aerobic enterobacterial microbiota, is important to establish an appropriate environment for
anaerobic bacteria, such as bifidobacteria and bacteroides140. Today, staphylococci are
acquired the first days after birth among Swedish infants, while it takes up to two months
before most infants have achieved an enterobacterial microbiota183. Speculatively, high
bacterial exposure may lead to early colonization with appropriate facultative aerobic
bacteria, which in turn would facilitate colonization of commensal anaerobic bacteria.
Thus, lifestyle factors might influence the colonization in infants. In addition, our group has
shown that the maternal faecal flora influences the colonization of some species of bacteria,
i.e. B. bifidum (Johansson et al unpublished).

67
Figure 10. Number of faecal Bifidobacterium species (B. sp.) in relation to endotoxin levels in house dust (EU/mg dust). The white boxes symbolize samples with two or less B. sp. and the grey boxes those with three or more. In figure a and b, the number of B. sp. is measured in faecal samples collected at one week after birth. In figure c and d, the faecal samples were collected at one month and two months, respectively.
Early infant gut microbiota in relation to maturation of immune responses (III)
In study II, we showed that children who developed allergic disease were less often colonized
with Lactobacilli gr. I, B. adolescentis and C. difficile. To explore potential mechanisms
behind this association we investigated whether early colonization with the gut microbiota
species, analyzed in study II, associates with childhood immune maturation, specifically
salivary SIgA and the spontaneous TLR2 and TLR4 mRNA expression in PBMC collected 12
months after birth. The possible allergy-protective effects from the increased pre- and
postnatal microbial exposure in farming environments might increase the expression of
several PRRs e.g. TLR2 and TLR4110, 238. Thus, we hypothesized that early exposure to
certain intestinal microbes modulates TLR expression and LPS responsiveness at twelve
months.
The spontaneous expression of TLR4 mRNA, which is important for responses to G- bacteria,
correlated inversely to the intensity (i.e. the relative amounts) of one week/one month
colonization with the G- bacteria Bacteroides fragilis (r=-0.47, p=0.02 and Figure 11a). The
expression of TLR2, which is important for responses to G+ bacteria was not affected,

68
however, nor were the G+ bifidobacteria, lactobacilli and C. difficile associated with TLR2 or
TLR4 mRNA expression.
Fig 11. The spontaneous expression of TLR4 mRNA (a) at twelve months and the LPS-induced production of CCL4 (MIP-1β) (b) and IL-6 (c) are inversely correlated to the intensity of Bacteroides fragilis colonization at one month after birth. The y-axis shows in figure 11a, the relative TLR4 mRNA expression/rRNA in PBMC collected twelve months after birth. In figure 11b and c, the y-axis shows the concentration of CCL4 (b) and IL-6 (c) in supernatants from the PBMCs stimulated with LPS for 24 hours. The x-axis shows the relative amount of Bacteroides fragilis at one month expressed as percent Bacteroides fragilis DNA of total amount nucleic acids.. The dotted line shows the detection limit at 5*10-6 % Bacteroides fragilis DNA of total amount nucleic acids. n.d. = not detectable.
Following this observation we wanted to investigate whether the intensity of Bacteroides
fragilis colonization influences LPS responsiveness. In concordance with the TLR4 mRNA
findings, the intensity of Bacteroides fragilis colonization at one week, one month and two
month were all inversely related to the LPS-induced production of IL-6 and CCL4 (MIP-1β)
(r=-0.62 to -0.79, p=0.002 to 0.04 and r=-0.75 to -0.86, p=0.001 to 0.005; Fig. 11b and c
exemplifies one month colonization). Also, LPS-induced CXCL8 (IL-8) and IL-17 were
inversely related to the intensity of Bacteroides fragilis colonization at one week after birth
(r=-0.75, p=0.008 and r=-0.68, p=0.02). In contrast, the intensity of B. adolescentis
colonization at one/two month correlated or tended to correlate to TNF, IL-10 and IL-12p70
(see study III). Partially supporting our findings, it has been observed that increased exposure
to muramic acid from G+ bacteria in house dust, correlated with IL-6 and TNF production in
mitogen-stimulated PBMC239. Conversely, the same study also showed that house dust levels

69
of 3-hydroxy fatty acids, from G- bacteria, were inversely associated with the production of
IL-6 and TNF after mitogen stimulation239. High LPS exposure induces endotoxin (LPS)
tolerance18 and endotoxin tolerant mice have decreased splenic TLR2 and TLR4 expression20.
Speculatively, the observed decreased LPS responsiveness in infants colonized with high
levels of Bacteroides fragilis could thus be due to endotoxin tolerance caused by the high
exposure to the G- Bacteroides fragilis. Also, PSA, which is another component from
Bacteroides fragilis has immunomodulatory properties240. Apart from restoring the proportion
of CD4+ T cells in the spleen of ex-GF mice, this component is also able to balance the
production of inflammatory cytokines, e.g. TNF and IL-17, in mice with induced colitis241.
Hypothetically, exposure to increased levels of gut Bacteroides fragilis PSA might regulate
the production of inflammatory cytokines systemically. Interestingly, Round and collegues
have shown that administration of PSA to GF mice prevents induced systemic septic shock
(Personal communication with June L Round at Keystone symposia A6 2009). In addition,
IL-6 and TNF production is lower in PSA treated mice. This fits well with our results that
early colonization with high numbers of Bacteroides fragilis reduces spontaneous TLR4
expression. The levels of salivary SIgA is higher in sensitized infants who show no symptoms of allergic
disease compared to the SIgA levels in infants with allergic disease117 (Tomicic et al
unpublished). Further, the salivary SIgA levels reflect the antigen-specific SIgA levels in the
gut (after low antigen administration)242 and thus we hypothesized that early colonization with
certain gut microbes influences SIgA levels in the gut and in additional compartments of the
MALT (salivary glands). The number of Bifidobacterium species in faeces collected one
week, one month and two months after birth correlated with salivary SIgA at six months
(r=0.51 to 0.58, p=0.02 to 0.045; Fig. 12a exemplifies the one month colonization).
Furthermore, the intensity of one/two month B. adolescentis colonization were associated
with higher SIgA at six months (Fig. 12b and r=0.55, p=0.03, respectively). The intensity of
B. bifidum colonization at one week, one month and two months after birth were correlated
with the SIgA production at twelve months (r=0.41 to 0.47, p=0.01 to 0.04, figure 12c
exemplifies one month colonization). In addition, early colonization with B. adolescentis, B.
breve and B. bifidum tended to be associated with higher levels of SIgA at six and twelve
months (study III). Thus, Bifidobacterium colonization appears to influence salivary SIgA
levels up to twelve months, but not later in infancy nor at five years of age. The later SIgA
formation might be influenced by other factors i.e. infections (Sandin et al unpublished). In

70
addition, the levels of SIgA at six months and five years were significantly associated with the
colonisation with lactobacilli group I at one month after birth (see Figure 2 a and d in study
III). Gut microbes appear to induce APRIL and TSLP production from IEC75. These factors
are involved in IgA2 class switching by B cells. Possibly could our results indicate that early
Bifidobacterium colonization influences APRIL and TSLP production leading to increased
SIgA production. Yet, others did not show that microbial colonization during the first two
months was associated with plasma levels of APRIL at four months243. The gut microbiota
might be more efficient in inducing APRIL production locally, however. Since the GALT and
the salivary glands are part of the common mucosal immune system244 the IgA production by
gut B cells might be reflected in saliva.
Figure 12. Total salivary secretory IgA (SIgA) at six months is associated with a more diverse Bifidobacterium (B.) flora (a) and the intensity of B. adolescentis colonization (b) at one month. Total SIgA at twelve months is associated with the intensity of B. bifidum colonization at one month (c). The y-axis shows total salivary secretory IgA (SIgA) (µg/ml) at six and twelve months and the x-axis shows the number of Bifidobacterium species (a) and the intensity of B. adolescentis (b) and B. bifidum (c) colonization. The intensity is expressed as percent B. adolescentis or B. bifidum DNA of total amount nucleic acids. The dotted line shows the detection limit at 5*10-6 % B. adolescentis or B. bifidum DNA of total amount nucleic acids. n.d. = not detectable.
As higher levels of SIgA might protect sensitized infants from allergy development117, it is
tempting to speculate that a more diverse Bifidobacterium flora could prevent allergy
development partially by stimulating salivary SIgA. I have summarized findings from us and
others regarding environmental factors associated with allergy development in figure 13.

71
There is a strong negative association between family size/endotoxin exposure and allergy
development102, 109. The other associations in this figure are weaker. However, what we and
others have shown is that these factors associate with each other. Family size and endotoxin
exposure appear to influence the diversity of the early Bifidobacterium flora (II). Others have
shown that a less diverse early gut microbiota is associated with allergy development237. In
addition, we showed that infants who developed allergic disease were less often colonized
with Lactobacilli gr. I, B. adolescentis and C. difficile during their first two months. Thus, a
more diverse gut microbiota might explain the inverse relationship between family
size/endotoxin exposure and allergy development. Children with older siblings have higher
SIgA (Sandin et al unpublished). Although endotoxin exposure was not associated with SIgA
levels (Tomicic et al unpublished), Estonian infants, who are exposed to higher levels of
endotoxin, have higher levels of SIgA than Swedish infants117, (Tomicic et al unpublished).
These results fit with the speculation above that a more diverse Bifidobacterium flora could
prevent allergy development partially by stimulating salivary SIgA. Conversely could the
observed association between the early Bifidobacterium flora and SIgA levels during the first
year indicate that an overall more diverse gut microbiota, in general, increases salivary SIgA.
Actually, also colonization with lactobacilli gr. I, at one month, was associated with higher
levels of salivary SIgA at six months and five years (see study III). Interestingly, Estonian
infants, who are more commonly colonized with lactobacilli152, have higher levels of SIgA,
compared to Swedish infants (Tomicic et al unpublished). Further studies are needed to
demonstrate if my speculations are true.
Figure 13. Associations between environmental factors, SIgA and allergy development. The green arrows indicate positive associations whereas the black arrows indicate negative associations. References to different studies are shown.

72
Clinical relevance
By studying the infant gut microbiota in relation to allergy development we might understand
which bacteria that could be of importance in allergy prevention and thus appropriate
probiotic candidates. Studies have investigated how very early administration of probiotics
(from birth or prenataly to pregnant mothers) associates with subsequent allergy development.
Interestingly a strain of L. rhamnosus, given to pregnant and breastfeeding mothers and to
their infants reduced the frequency of eczema in the children up to age seven indicating that
this species might be important in eczema prevention228, 245. However, SPT positivity did not
differ between the two groups. Another double-blind randomised placebo-controlled trial
investigated the role of L. reuteri administration to mothers prenatally and to their infants for
their first 12 months229. The prevalence of eczema outcome and asthma did not differ between
the two groups, however the probiotic group had significantly lower proportion of IgE-
associated eczema at two years. Recently, L. rhamnosus administration but not B. lactis
administration was shown to decrease the incidence of IgE-associated eczema230. Trials
showing no association between probiotic administration and allergy development have also
been completed246. Importantly, administration of L. acidophilus during the first six months
and an increased risk for sensitization has also been reported247. The different strains, when
they are administered (prenatally and/or from birth), number of participants and the follow up
period are all factors which could influence the outcome. The largest study performed, which
used several probiotic strains (2 strains of L. rhamnosus, B. breve and Propionibacterium
freudenreichii) and prebiotic galacto-oligosaccharides, showed promising results regarding
eczema and atopic eczema outcome at two years of age 248. Yet, the five-year follow up could
not find any difference in allergic disease between the probiotic- or placebo-treated group249.
This somewhat fit with our results where early Lactobacilli gr. I colonization and B.
adolescentis colonization was associated with decreased development of atopic eczema but
not later allergy development.
Importantly, much is still unknown about the gut microbiota. The solution might not be to
administer some strains of probiotic bacteria but rather to increase the diversity of the gut
microbiota as a whole. In paper II we showed that lifestyle factors appear to influence the
Bifidobacterium flora. Promoting vaginal delivery could be another approach. Caesarean-
delivered infants appear to have a delayed colonization with several different species of
bacteria150. In addition these infants are at higher risk for developing allergic disease250.

73
Probiotic therapy might be beneficial when vaginal delivery is not an option. Actually, the
five-year follow up mentioned above showed that infants delivered with ceaserean section
were at decreased risk of developing atopic disease if they were given probiotics from birth
compared to if they received placebo249.
Our study regarding consumption of colostrum oligosaccharides did not show any significant
association with allergy development at 18 months of age. Yet, additional substances in
human milk might also stimulate species of the gut microbiota206. Also, human milk contains
Bifidobacterium species223 and has been shown to modulate TLR responses251. Thus, it might
be of relevance to promote breastfeeding also for its ability to contribute to infant colonization
and stimulation of gut microbiota-immune interactions.

74
CONCLUDING REMARKS
• The content of neutral oligosaccharides in colostrum did not depend on maternal
allergy, nor was consumption of colostrum with high amounts of oligosaccharides
associated with less allergy development up to 18 months.
• Infants who harboured Lactobacilli group I (L. rhamnosus, L. paracasei, L. casei) and
B. adolescentis at one week of age less frequently developed allergic disease
compared to infants who did not harbour these bacteria at the same time. This might
imply the importance of a diverse gut microbiota early in life for the development of a
fully functional immune system.
• Family size and endotoxin exposure influenced the early Bifidobacterium flora. Thus,
a more diverse gut microbiota might possibly explain the inverse relationship between
family size/endotoxin exposure and allergy development.
• The early Bifidobacterium flora influenced levels of salivary SIgA at six and twelve
months. Speculatively, this provides a potential mechanism to why early B.
adolescentis colonization could be associated with less allergy development.
• The intensity of early Bacteroides fragilis colonization influenced LPS responsiveness
of PBMCs collected at 12 month. Thus, this bacterium might influence systemic
immune responses.

75
FUTURE PERSPECTIVES
In our second study we investigated the early infant gut microbiota in relation to allergy
development up to five years of age and found differences at species level. Since human milk
is the only food during the first months (in our study population) it might influence the early
gut microbiota. Although we could not show that consumption of colostrum oligosaccharides
influences allergy development (study I) the later milk oligosaccharides might be of
importance. As breast milk consumed by the children in study II has been collected we can
relate the neutral oligosaccharide composition in these samples to the presence of amounts of
the bacterial species investigated in paper II and probably understand more about the prebiotic
function of HMOs.
In our third study we showed that infants who harbour a more diverse Bifidobacterium flora
during their first two months have increased levels of salivary SIgA at six months. After
encountering bacterial components, the intestinal epithelial cells (IECs) appear to be able to
produce cytokines important for IgA class switching e.g. APRIL75. How certain gut
microbiota species influences the production of these cytokines and thus IgA class switching
in the gut needs to be further investigated. In addition, IECs produce other cytokines which
are important for conditioning of DCs and further for differentiation of regulatory T cells as
described previously10. Thus, it would be interesting to study whether lactic acid bacteria
induce production of regulatory and conditioning cytokines e.g. TGFβ and TSLP from IECs.
These cytokines also influence IgA production. To further understand the role of IgA in
development of allergic disease it would be interesting to measure fecal levels of SIgA and
relate to later allergy development. Actually, high levels of SIgA in faeces are associated with
tolerance in mice135. However, this would have to be performed in age-matched infants not
receiving breast milk.
Although IECs appear to be somewhat non-responding towards lactic acid bacteria, regarding
IL-8 production252, pre-incubation with lactic acid bacteria reduces the pro-inflammatory
responses mediated by Salmonella typhimurium or flagellin and abolishes DC maturation
induced by G- bacteria252, 253. In study II we showed that infants who developed allergy were
less often colonized with C. difficile during their first two months. In contrast others show that
early C. difficile colonization is more common in infants who develop allergic disease
compared to infants who remain non-allergic138, 189 We speculate that it is not C. difficile

76
colonization per se that is associated with allergy development. However, C. difficile induces
unfavorable immune responses when the gut microbiota is less diverse. A diverse lactic acid
flora might decrease these responses and it would be of interest to study if pre-incubation with
lactic acid bacteria influences IL-8 production of IEC after C. difficile stimulation. We have
also shown that IECs are rather non-responsive to stimulation with breast milk or LPS alone
(Holmlund et al unpublished). However, simultaneous stimulation with LPS and breast milk
induces high IL-8 production. Speculatively, these responses could cause too much
inflammation and it would thus be interesting to study whether pre-incubation with lactic acid
bacteria decreases these responses.
We have investigated the gut microbiota in relation to allergy development. In addition, we
show that certain gut microbiota species appear to influence systemic and mucosal immunity
(III). Consequently, the observed associations could also be attributable to other disorders.
Increased infant SIgA in saliva and feces would prevent both allergens and pathogens from
entering the mucosa thus increasing the integrity of the barrier. The gut microbiota has also
been linked to inflammatory bowel disease, obesity and type 1 diabetes254-256 The gut
microbiota could probably influence these diseases by modulating immunological factors.
However, other physiological factors could also be influenced by the gut microbiota257. Future
studies will have to reveal how the vast amounts of genes present among the bacterial strains
in the gut, the gut microbiome147, relates to the physiology and health of the host.

77
ACKNOWLEDGEMENTS
I am most grateful to my supervisor Eva Sverremark Ekström for giving me the opportunity to do a PhD. You have been an excellent supervisor and given me a lot of support during these past four years. You have always listened to my ideas and then pushed me in the right direction for them to succeed. Your belief in me has made me believe more in myself. I am very thankful to my co-author Maria Jenmalm at Linköping University for all your great ideas and help with the manuscripts. You always take your time and it is wonderful to work with people who are so dedicated to their work. I would also especially like to thank professor Bengt “Muck” Björkstén for all your help and your enthusiasm. Your previous work has been such an inspiration and I have learnt a lot working with you. I am also grateful to you for introducing us to the Linköping staff. Another person without whom this work would not have been possible is Frank “Zeke” Lindh. Thank you for bringing me to Uppsala and Isosep and for teaching me the procedure of HMO analysis! Thanks also for the fun we had there and for keeping the “godisskål” filled! I am also very grateful to my other co-authors from Linköping: Karel Duchén, Malin Böttcher, Sara Tomicic and Anna Lundberg for all your help. Your previous work has been an inspiration. I would also like to thank you all (and Maria Je) for being excellent soccer supporters. I appreciate all the effort Lena Lindell and Ann-Marie Fornander at Linköping Universty hospital have put into collecting and keeping track of samples. Other persons who have helped me in my work by simply being there and eager to discuss are my previous and present roommates and group members: Yvonne Sundström, Nora Bachmayer, Petra Amoudruz, Ulrika Holmlund, Maria Johansson, Ebba Sohlberg, Shanie Hedengren and Elin Hultgren. I have so enjoyed sharing room and laughs with you. Thank you for letting me ask “stupid” questions and for being great friends! I am also grateful for all the fun we have had during conferences. We have seen too much (Yvonne and me on the built island in Vienna). We have danced in Bangkok (Petra and Shanie) and Taos (Maria) and enjoyed sunbathing and skiing. Many thanks to Nora for your cute notes, for teaching me the importance of a plan and for enjoying a glass of wine! I am grateful for the help I have got from my “slaves” that is my 10- and 20-points project workers: Caroline “Carro” Nissan, Karin Sundström and Maria Johansson. Thanks for sharing the interest of my work with me but also for sharing other important things in life like chocolate (Karin), gossip (Caroline) and exercise (Maria)! Thank you, Gelana Yadeta, Margareta “Maggan” Hagstedt, Ann Sjölund and Anna-Lena Jarva for your help with everyday issues like keeping track of my LADOK points and answering my stupid questions about where the different chemicals are! Thanks to all the seniors at the department, professors Carmen Fernandez, Klavs Berzins, Marita Troye-Blomberg and Eva Severinsson, for interesting discussions!

78
I would like to thank all present and former students at the Immunology department for making the department a nice place to come in to. John Arko-Mensah, Nancy Away, Halima Balogun, Jubayer Rahman, Amre Nasr, Salah Farouk, Nnaemeka Iriemenam, Anna Tjärnlund, Camilla Rydström, Jacob Minang, Khosro Masjedi, Manijeh Vafa Homann, Fernando Sosa, Olivia Simone, Stefania Verani, Jacqueline Calla, Geshanti Arambepola, Nicky Thrupp, Susanna Kearsly, Charles Arama, Lucia Liszka, Russel Al-Balaghi, Stephanie Boström and Olga Daniela Chuquima. I would especially like to thank Lisa Israelsson and Pablo Giusti for keeping the spirit up with your laughs and crazy ideas and Anna-Karin Sigfrinius for teaching me how the QPCR works. Thank you, Anette, Thomas, Ulrika, Björn, Pär and Håkan at Isosep for nice lunches, fun parties and all the gossip! Mina underbara vänner, tack! För att ni aldrig tröttnar på att prata. För allt galet och alla skratt. Särskilt tack till: Carro! Vi har kämpat oss igenom gymnasiet, ett flertal universitetskurser och kan (förhoppningsvis) båda två kalla oss doktorer när 2010 nalkas. Du är en underbar vän som har gett mig en massa stöd! Vi har delat skrattanfall, en minisäng och mer eller mindre lyckade nyårsaftnar och jag hoppas vi får dela så mycket mer i framtiden. Kia! För att du alltid finns där när jag behöver och för att man aldrig vet var man kan hamna när man är med dig. Kanske i ett hustält i Venedig eller på kändisspan i Halmstad. Tack också för att du lät mig hänga i korridoren! Jossan, Saad och Isak! För att ni är så gulliga, för mysiga middagar och alla gånger jag fått skjuts. Och Jossan, visst kan man ha väldigt kul i krogkön? Marie! För att du gjorde studierna så mycket roligare och var en superb labbpartner. Min andra familj som jag har fått under dessa fyra år; Ingvar, Monica, Robin och Karin. Tack för alla härliga skiddagar och middagar vi delat! Jag är så väldigt tacksam för de möjligheter min underbara familj har gett mig. Tack mamma och pappa för att ni alltid funnits där och tragglat glosor, fysik, matte och kemi med mig! Se nu var det har lett… Tack moster Maggan för att du som familjens första doktor har gett mig fotspår att vandra i! Tack Sven och Hanna för allt kul vi hade under barndomen och nu fortsätter ha när vi blivit vuxna! Även om vi alltid kommer vara barnen... Jacob, du har skänkt mig så mycket glädje, stöd och kärlek under dessa år. Jag är väldigt lycklig över att du finns i mitt liv och alltid får mig att le. Det värmer så att du försöker förstå ”de där bakterierna” och tack vare din smittsamma entusiasm har du fått mig att kämpa på när det har varit som tyngst. Jag älskar dig! This work was supported by: The Ekhaga foundation, the Cancer and Allergy foundation, Mjölkdroppen, the Magnus Bergvall foundation, the Konsul Th C Berghs foundation, the Swedish Research Council (57X-15160-05-2 and 74X-20146-01-2), the National Swedish Association against Allergic Diseases, the National Heart and Lung Association and the Swedish Foundation for Health Care Sciences and Allergy Research.

79
REFERENCES 1. Medzhitov R. Recognition of microorganisms and activation of the immune response. Nature. 2007;
449(7164):819-826.
2. Kaisho T, Akira S. Toll-like receptor function and signaling. J Allergy Clin Immunol. 2006; 117(5):979-87.
3. Valenta R. The future of antigen-specific immunotherapy of allergy. Nat Rev Immunol. 2002; 2(6):446-453.
4. Tacke F, Randolph GJ. Migratory fate and differentiation of blood monocyte subsets. Immunobiology. 2006; 211(6-8):609-618.
5. Serbina NV, Jia T, Hohl TM, Pamer EG. Monocyte-mediated defense against microbial pathogens. Annu Rev Immunol. 2008; 26:421-452.
6. Schenk M, Mueller C. Adaptations of intestinal macrophages to an antigen-rich environment. Semin Immunol. 2007; 19(2):84-93.
7. Gordon S, Taylor PR. Monocyte and macrophage heterogeneity. Nat Rev Immunol. 2005; 5(12):953-964.
8. Wu L, Dakic A. Development of dendritic cell system. Cell Mol Immunol. 2004; 1(2):112-118.
9. Hume DA. Macrophages as APC and the dendritic cell myth. J Immunol. 2008; 181(9):5829-5835.
10. Coombes JL, Powrie F. Dendritic cells in intestinal immune regulation. Nat Rev Immunol. 2008;8:435-446.
11. Iwasaki A. Mucosal dendritic cells. Annu Rev Immunol. 2007; 25:381-418.
12. Akira S, Uematsu S, Takeuchi O. Pathogen recognition and innate immunity. Cell. 2006; 124(4):783-801.
13. Harris G, KuoLee R, Chen W. Role of toll-like receptors in health and diseases of gastrointestinal tract. World J Gastroenterol. 2006; 12(14):2149-2160.
14. Tsujimoto H, Ono S, Efron PA, Scumpia PO, Moldawer LL, Mochizuki H. Role of toll-like receptors in the development of sepsis. Shock. 2008; 29(3):315-321.
15. Jerala R. Structural biology of the LPS recognition. Int J Med Microbiol. 2007; 297(5):353-363.
16. Kapsenberg ML. Dendritic-cell control of pathogen-driven T-cell polarization. Nat Rev Immunol. 2003; 3(12):984-993.
17. Winkler P, Ghadimi D, Schrezenmeir J, Kraehenbuhl JP. Molecular and cellular basis of microflora-host interactions. J Nutr. 2007; 137(3 Suppl 2):756S-72S.
18. Nomura F, Akashi S, Sakao Y, et al. Cutting edge: Endotoxin tolerance in mouse peritoneal macrophages correlates with down-regulation of surface toll-like receptor 4 expression. J Immunol. 2000; 164(7):3476-3479.
19. Amoudruz P, Holmlund U, Malmström V, et al. Neonatal immune responses to microbial stimuli: Is there an influence of maternal allergy? J Allergy Clin Immunol. 2005; 115(6):1304-1310.
20. Zhong B, Ma HY, Yang Q, Gu FR, Yin GQ, Xia CM. Decrease in toll-like receptors 2 and 4 in the spleen of mouse with endotoxic tolerance. Inflamm Res. 2008; 57(6):252-259.
21. Granowitz EV, Porat R, Mier JW, et al. Intravenous endotoxin suppresses the cytokine response of peripheral blood mononuclear cells of healthy humans. J Immunol. 1993; 151(3):1637-1645.

80
22. Le Y, Zhou Y, Iribarren P, Wang J. Chemokines and chemokine receptors: Their manifold roles in homeostasis and disease. Cell Mol Immunol. 2004; 1(2):95-104.
23. Levy O. Innate immunity of the newborn: Basic mechanisms and clinical correlates. Nat Rev Immunol. 2007; 7(5):379-390.
24. Steinke JW, Borish L. 3. cytokines and chemokines. J Allergy Clin Immunol. 2006; 117:S441-5.
25. Idriss HT, Naismith JH. TNF alpha and the TNF receptor superfamily: Structure-function relationship(s). Microsc Res Tech. 2000; 50(3):184-195.
26. Arend WP, Palmer G, Gabay C. IL-1, IL-18, and IL-33 families of cytokines. Immunol Rev. 2008; 223:20-38.
27. Dienz O, Rincon M. The effects of IL-6 on CD4 T cell responses. Clin Immunol. 2009; 130(1):27-33.
28. Kishimoto T. Interleukin-6: Discovery of a pleiotropic cytokine. Arthritis Res Ther. 2006; 8 Suppl 2:S2.
29. Pasare C, Medzhitov R. Toll pathway-dependent blockade of CD4+CD25+ T cell-mediated suppression by dendritic cells. Science. 2003; 299(5609):1033-1036.
30. Kimura A, Naka T, Kishimoto T. IL-6-dependent and -independent pathways in the development of interleukin 17-producing T helper cells. Proc Natl Acad Sci U S A. 2007; 104(29):12099-12104.
31. O'Garra A, Barrat FJ, Castro AG, Vicari A, Hawrylowicz C. Strategies for use of IL-10 or its antagonists in human disease. Immunol Rev. 2008; 223:114-131.
32. Trinchieri G, Pflanz S, Kastelein RA. The IL-12 family of heterodimeric cytokines: New players in the regulation of T cell responses. Immunity. 2003; 19(5):641-644.
33. Brinkmann V, Zychlinsky A. Beneficial suicide: Why neutrophils die to make NETs. Nat Rev Microbiol. 2007; 5(8):577-582.
34. Nathan C. Neutrophils and immunity: Challenges and opportunities. Nat Rev Immunol. 2006; 6(3):173-182.
35. Newman KC, Riley EM. Whatever turns you on: Accessory-cell-dependent activation of NK cells by pathogens. Nat Rev Immunol. 2007; 7(4):279-291.
36. Yokoyama WM, Riley JK. NK cells and their receptors. Reprod Biomed Online. 2008; 16(2):173-191.
37. Beetz S, Wesch D, Marischen L, Welte S, Oberg HH, Kabelitz D. Innate immune functions of human gammadelta T cells. Immunobiology. 2008; 213(3-4):173-182.
38. Weinreich MA, Hogquist KA. Thymic emigration: When and how T cells leave home. J Immunol. 2008; 181(4):2265-2270.
39. Hayday A, Gibbons D. Brokering the peace: The origin of intestinal T cells. Mucosal Immunol. 2008; 1(3):172-174.
40. Trambas CM, Griffiths GM. Delivering the kiss of death. Nat Immunol. 2003; 4(5):399-403.
41. Zhu J, Paul WE. CD4 T cells: Fates, functions, and faults. Blood. 2008; 112(5):1557-1569.
42. Wilson NJ, Boniface K, Chan JR, et al. Development, cytokine profile and function of human interleukin 17-producing helper T cells. Nat Immunol. 2007; 8(9):950-957.
43. Korn T, Bettelli E, Oukka M, Kuchroo VK. IL-17 and Th17 cells. Annu Rev Immunol. 2009 Epub ahead of print.

81
44. Vuillermin PJ, Ponsonby AL, Saffery R, et al. Microbial exposure, interferon gamma gene demethylation in naive T-cells, and the risk of allergic disease. Allergy. 2009 Epub ahead of print.
45. Yazdanbakhsh M, van den Biggelaar A, Maizels RM. Th2 responses without atopy: Immunoregulation in chronic helminth infections and reduced allergic disease. Trends Immunol. 2001; 22(7):372-377.
46. Pillai V, Karandikar NJ. Human regulatory T cells: A unique, stable thymic subset or a reversible peripheral state of differentiation? Immunol Lett. 2007; 114(1):9-15.
47. Hori S, Nomura T, Sakaguchi S. Control of regulatory T cell development by the transcription factor Foxp3. Science. 2003; 299(5609):1057-1061.
48. Buckner JH, Ziegler SF. Functional analysis of FOXP3. Ann N Y Acad Sci. 2008; 1143:151-169.
49. Visser J, Nijman HW, Hoogenboom BN, et al. Frequencies and role of regulatory T cells in patients with (pre)malignant cervical neoplasia. Clin Exp Immunol. 2007; 150(2):199-209.
50. Kabelitz D. Expression and function of toll-like receptors in T lymphocytes. Curr Opin Immunol. 2007; 19(1):39-45.
51. Komori HK, Meehan TF, Havran WL. Epithelial and mucosal gamma delta T cells. Curr Opin Immunol. 2006; 18(5):534-538.
52. Moura R, Agua-Doce A, Weinmann P, Graca L, Fonseca JE. B cells from the bench to the clinical practice. Acta Reumatol Port. 2008; 33(2):137-154.
53. Batista FD, Harwood NE. The who, how and where of antigen presentation to B cells. Nat Rev Immunol. 2009; 9(1):15-27.
54. Chiron D, Bekeredjian-Ding I, Pellat-Deceunynck C, Bataille R, Jego G. Toll-like receptors: Lessons to learn from normal and malignant human B cells. Blood. 2008; 112(6):2205-2213.
55. Gould HJ, Sutton BJ. IgE in allergy and asthma today. Nat Rev Immunol. 2008; 8(3):205-217.
56. Fukata M, Abreu MT. Role of toll-like receptors in gastrointestinal malignancies. Oncogene. 2008; 27(2):234-243.
57. Nagler-Anderson C. Man the barrier! strategic defences in the intestinal mucosa. Nat Rev Immunol. 2001; 1(1):59-67.
58. Iweala OI, Nagler CR. Immune privilege in the gut: The establishment and maintenance of non-responsiveness to dietary antigens and commensal flora. Immunol Rev. 2006; 213:82-100.
59. Mukherjee S, Vaishnava S, Hooper LV. Multi-layered regulation of intestinal antimicrobial defense. Cell Mol Life Sci. 2008; 65(19):3019-3027.
60. Kraehenbuhl JP, Corbett M. Immunology. keeping the gut microflora at bay. Science. 2004; 303(5664):1624-1625.
61. Suzuki K, Ha SA, Tsuji M, Fagarasan S. Intestinal IgA synthesis: A primitive form of adaptive immunity that regulates microbial communities in the gut. Semin Immunol. 2007; 19(2):127-135.
62. Zasloff M. Antimicrobial peptides of multicellular organisms. Nature. 2002; 415(6870):389-395.
63. Salzman NH, Underwood MA, Bevins CL. Paneth cells, defensins, and the commensal microbiota: A hypothesis on intimate interplay at the intestinal mucosa. Semin Immunol. 2007; 19(2):70-83.
64. Vercelli D. Discovering susceptibility genes for asthma and allergy. Nat Rev Immunol. 2008; 8(3):169-182.

82
65. Michetti P, Mahan MJ, Slauch JM, Mekalanos JJ, Neutra MR. Monoclonal secretory immunoglobulin A protects mice against oral challenge with the invasive pathogen Salmonella typhimurium. Infect Immun. 1992; 60(5):1786-1792.
66. Renegar KB, Small PA,Jr. Passive transfer of local immunity to influenza virus infection by IgA antibody. J Immunol. 1991; 146(6):1972-1978.
67. Ruggeri FM, Johansen K, Basile G, Kraehenbuhl JP, Svensson L. Antirotavirus immunoglobulin A neutralizes virus in vitro after transcytosis through epithelial cells and protects infant mice from diarrhea. J Virol. 1998; 72(4):2708-2714.
68. Lamm ME. Interaction of antigens and antibodies at mucosal surfaces. Annu Rev Microbiol. 1997; 51:311-340.
69. Corthesy B. Roundtrip ticket for secretory IgA: Role in mucosal homeostasis? J Immunol. 2007;178:27-32.
70. Cerutti A. The regulation of IgA class switching. Nat Rev Immunol. 2008; 8(6):421-434.
71. Cerutti A, Rescigno M. The biology of intestinal immunoglobulin A responses. Immunity. 2008; 28(6):740-750.
72. Brandtzaeg P. Do salivary antibodies reliably reflect both mucosal and systemic immunity? Ann N Y Acad Sci. 2007; 1098:288-311.
73. McGhee JR, Kunisawa J, Kiyono H. Gut lymphocyte migration: We are halfway 'home'. Trends Immunol. 2007; 28(4):150-153.
74. Mora JR, Iwata M, Eksteen B, et al. Generation of gut-homing IgA-secreting B cells by intestinal dendritic cells. Science. 2006; 314(5802):1157-1160.
75. He B, Xu W, Santini PA, et al. Intestinal bacteria trigger T cell-independent immunoglobulin A(2) class switching by inducing epithelial-cell secretion of the cytokine APRIL. Immunity. 2007; 26(6):812-826.
76. Mowat AM. Anatomical basis of tolerance and immunity to intestinal antigens. Nat Rev Immunol. 2003; 3(4):331-341.
77. van Wijk F, Knippels L. Initiating mechanisms of food allergy: Oral tolerance versus allergic sensitization. Biomed Pharmacother. 2007; 61(1):8-20.
78. Smith DW, Nagler-Anderson C. Preventing intolerance: The induction of nonresponsiveness to dietary and microbial antigens in the intestinal mucosa. J Immunol. 2005; 174(7):3851-3857.
79. Jabri B, Ebert E. Human CD8+ intraepithelial lymphocytes: A unique model to study the regulation of effector cytotoxic T lymphocytes in tissue. Immunol Rev. 2007; 215:202-214.
80. Karlsson MR, Rugtveit J, Brandtzaeg P. Allergen-responsive CD4+CD25+ regulatory T cells in children who have outgrown cow's milk allergy. J Exp Med. 2004; 199(12):1679-1688.
81. Maynard CL, Harrington LE, Janowski KM, et al. Regulatory T cells expressing interleukin 10 develop from Foxp3+ and Foxp3- precursor cells in the absence of interleukin 10. Nat Immunol. 2007; 8(9):931-941.
82. Watanabe N, Wang YH, Lee HK, et al. Hassall's corpuscles instruct dendritic cells to induce CD4+CD25+ regulatory T cells in human thymus. Nature. 2005; 436(7054):1181-1185.
83. Asher MI, Montefort S, Björkstén B, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet. 2006; 368(9537):733-743.
83
84. Johansson SG, Hourihane JO, Bousquet J, et al. A revised nomenclature for allergy. an EAACI position statement from the EAACI nomenclature task force. Allergy. 2001; 56(9):813-824.
85. Nilsson C, Linde A, Montgomery SM, et al. Does early EBV infection protect against IgE sensitization? J Allergy Clin Immunol. 2005; 116(2):438-444.
86. Björkstén B. Effects of intestinal microflora and the environment on the development of asthma and allergy. Springer Semin Immunopathol. 2004; 25(3-4):257-270.
87. Bergmann RL, Edenharter G, Bergmann KE, et al. Predictability of early atopy by cord blood-IgE and parental history. Clin Exp Allergy. 1997; 27(7):752-760.
88. Eder W, Klimecki W, Yu L, et al. Opposite effects of CD 14/-260 on serum IgE levels in children raised in different environments. J Allergy Clin Immunol. 2005; 116(3):601-607.
89. Salvatore S, Keymolen K, Hauser B, Vandenplas Y. Intervention during pregnancy and allergic disease in the offspring. Pediatr Allergy Immunol. 2005; 16(7):558-566.
90. Loibichler C, Pichler J, Gerstmayr M, et al. Materno-fetal passage of nutritive and inhalant allergens across placentas of term and pre-term deliveries perfused in vitro. Clin Exp Allergy. 2002; 32(11):1546-1551.
91. Edelbauer M, Loibichler C, Nentwich I, Gerstmayr M, Urbanek R, Szepfalusi Z. Maternally delivered nutritive allergens in cord blood and in placental tissue of term and preterm neonates. Clin Exp Allergy. 2004; 34(2):189-193.
92. Bonnelykke K, Pipper CB, Bisgaard H. Sensitization does not develop in utero. J Allergy Clin Immunol. 2008; 121(3):646-651.
93. Kihlström A, Lilja G, Pershagen G, Hedlin G. Exposure to high doses of birch pollen during pregnancy, and risk of sensitization and atopic disease in the child. Allergy. 2003; 58(9):871-877.
94. Kihlström A, Lilja G, Pershagen G, Hedlin G. Exposure to birch pollen in infancy and development of atopic disease in childhood. J Allergy Clin Immunol. 2002; 110(1):78-84.
95. Hesselmar B, Åberg N, Åberg B, Eriksson B, Björkstén B. Does early exposure to cat or dog protect against later allergy development? Clin Exp Allergy. 1999; 29(5):611-617.
96. Sicherer SH, Burks AW. Maternal and infant diets for prevention of allergic diseases: Understanding menu changes in 2008. J Allergy Clin Immunol. 2008; 122(1):29-33.
97. Prescott SL, Smith P, Tang M, et al. The importance of early complementary feeding in the development of oral tolerance: Concerns and controversies. Pediatr Allergy Immunol. 2008; 19(5):375-380.
98. Holt PG. Prenatal versus postnatal priming of allergen specific immunologic memory: The debate continues. J Allergy Clin Immunol. 2008; 122(4):717-718.
99. Sverremark Ekström E, Nilsson C, Holmlund U, et al. IgE is expressed on, but not produced by, fetal cells in the human placenta irrespective of maternal atopy. Clin Exp Immunol. 2002; 127(2):274-282.
100. Joerink M, Rindsjö E, Stenius F, et al. Evidence for allergen-specific IgE of maternal origin in human placenta. Allergy. 2009 Epub ahead of print.
101. Strachan DP. Hay fever, hygiene, and household size. BMJ. 1989; 299(6710):1259-1260.
102. Karmaus W, Botezan C. Does a higher number of siblings protect against the development of allergy and asthma? A review. J Epidemiol Community Health. 2002; 56(3):209-217.
103. Matricardi PM, Rosmini F, Riondino S, et al. Exposure to foodborne and orofecal microbes versus airborne viruses in relation to atopy and allergic asthma: Epidemiological study. BMJ. 2000; 320(7232):412-417.

84
104. Janson C, Asbjornsdottir H, Birgisdottir A, et al. The effect of infectious burden on the prevalence of atopy and respiratory allergies in Iceland, Estonia, and Sweden. J Allergy Clin Immunol. 2007;120:673-679.
105. Stensballe LG, Simonsen JB, Thomsen SF, et al. The causal direction in the association between respiratory syncytial virus hospitalization and asthma. J Allergy Clin Immunol. 2009; 123(1):131-137.e1.
106. Strachan DP. Family size, infection and atopy: The first decade of the "hygiene hypothesis". Thorax. 2000; 55 Suppl 1:S2-10.
107. Kilpelainen M, Terho EO, Helenius H, Koskenvuo M. Farm environment in childhood prevents the development of allergies. Clin Exp Allergy. 2000; 30(2):201-208.
108. Roy SR, Schiltz AM, Marotta A, Shen Y, Liu AH. Bacterial DNA in house and farm barn dust. J Allergy Clin Immunol. 2003; 112(3):571-578.
109. Braun-Fahrländer C, Riedler J, Herz U, et al. Environmental exposure to endotoxin and its relation to asthma in school-age children. N Engl J Med. 2002; 347(12):869-877.
110. Ege MJ, Bieli C, Frei R, et al. Prenatal farm exposure is related to the expression of receptors of the innate immunity and to atopic sensitization in school-age children. J Allergy Clin Immunol. 2006; 117(4):817-823.
111. Willems F, Vollstedt S, Suter M. Phenotype and function of neonatal DC. Eur J Immunol. 2009; 39(1):26-35.
112. Siegrist CA, Aspinall R. B-cell responses to vaccination at the extremes of age. Nat Rev Immunol. 2009; 9(3):185-194.
113. Landers CD, Chelvarajan RL, Bondada S. The role of B cells and accessory cells in the neonatal response to TI-2 antigens. Immunol Res. 2005; 31(1):25-36.
114. Holt PG, Jones CA. The development of the immune system during pregnancy and early life. Allergy. 2000; 55(8):688-697.
115. Bakker-Zierikzee AM, Tol EA, Kroes H, Alles MS, Kok FJ, Bindels JG. Faecal SIgA secretion in infants fed on pre- or probiotic infant formula. Pediatr Allergy Immunol. 2006; 17(2):134-140.
116. Blumer N, Pfefferle PI, Renz H. Development of mucosal immune function in the intrauterine and early postnatal environment. Curr Opin Gastroenterol. 2007; 23(6):655-660.
117. Böttcher MF, Häggström P, Björkstén B, Jenmalm MC. Total and allergen-specific immunoglobulin A levels in saliva in relation to the development of allergy in infants up to 2 years of age. Clin Exp Allergy. 2002; 32(9):1293-1298.
118. Yerkovich ST, Wikström ME, Suriyaarachchi D, Prescott SL, Upham JW, Holt PG. Postnatal development of monocyte cytokine responses to bacterial lipopolysaccharide. Pediatr Res. 2007; 62(5):547-552.
119. Levy O, Coughlin M, Cronstein BN, Roy RM, Desai A, Wessels MR. The adenosine system selectively inhibits TLR-mediated TNF-alpha production in the human newborn. J Immunol. 2006; 177(3):1956-1966.
120. Marchini G, Nelson A, Edner J, Lonne-Rahm S, Stavreus-Evers A, Hultenby K. Erythema toxicum neonatorum is an innate immune response to commensal microbes penetrated into the skin of the newborn infant. Pediatr Res. 2005; 58(3):613-616.
121. Romagnani S. The increased prevalence of allergy and the hygiene hypothesis: Missing immune deviation, reduced immune suppression, or both? Immunology. 2004; 112(3):352-363.
122. Romagnani S. Coming back to a missing immune deviation as the main explanatory mechanism for the hygiene hypothesis. J Allergy Clin Immunol. 2007; 119(6):1511-1513.

85
123. Bohle B, Jahn-Schmid B, Maurer D, Kraft D, Ebner C. Oligodeoxynucleotides containing CpG motifs induce IL-12, IL-18 and IFN-gamma production in cells from allergic individuals and inhibit IgE synthesis in vitro. Eur J Immunol. 1999; 29(7):2344-2353.
124. Bashir ME, Louie S, Shi HN, Nagler-Anderson C. Toll-like receptor 4 signaling by intestinal microbes influences susceptibility to food allergy. J Immunol. 2004; 172(11):6978-6987.
125. Garn H, Renz H. Epidemiological and immunological evidence for the hygiene hypothesis. Immunobiology. 2007; 212(6):441-452.
126. Sudo N, Sawamura S, Tanaka K, Aiba Y, Kubo C, Koga Y. The requirement of intestinal bacterial flora for the development of an IgE production system fully susceptible to oral tolerance induction. J Immunol. 1997; 159(4):1739-1745.
127. Rowe J, Kusel M, Holt BJ, et al. Prenatal versus postnatal sensitization to environmental allergens in a high-risk birth cohort. J Allergy Clin Immunol. 2007; 119(5):1164-1173.
128. Nilsson C, Larsson AK, Höglind A, Gabrielsson S, Troye Blomberg M, Lilja G. Low numbers of interleukin-12-producing cord blood mononuclear cells and immunoglobulin E sensitization in early childhood. Clin Exp Allergy. 2004; 34(3):373-380.
129. Sandberg M, Frykman A, Ernerudh J, et al. Cord blood cytokines and chemokines and development of allergic disease. Pediatr Allergy Immunol. 2008 Epub ahead of print.
130. Marschan E, Honkanen J, Kukkonen K, Kuitunen M, Savilahti E, Vaarala O. Increased activation of GATA-3, IL-2 and IL-5 of cord blood mononuclear cells in infants with IgE sensitization. Pediatr Allergy Immunol. 2008; 19(2):132-139.
131. Saghafian-Hedengren S, Holmlund U, Amoudruz P, Nilsson C, Sverremark-Ekström E. Maternal allergy influences p38-mitogen-activated protein kinase activity upon microbial challenge in CD14+ monocytes from 2-year-old children. Clin Exp Allergy. 2008; 38(3):449-457.
132. Amoudruz P, Holmlund U, Saghafian-Hedengren S, Nilsson C, Sverremark-Ekström E. Impaired toll-like receptor 2 signalling in monocytes from 5-year-old allergic children. Clin Exp Immunol. 2009; 155(3):387-394.
133. Roponen M, Hyvärinen A, Hirvonen MR, Keski-Nisula L, Pekkanen J. Change in IFN-gamma-producing capacity in early life and exposure to environmental microbes. J Allergy Clin Immunol. 2005; 116(5):1048-1052.
134. Ballow M. Primary immunodeficiency disorders: Antibody deficiency. J Allergy Clin Immunol. 2002; 109(4):581-591.
135. Frossard CP, Hauser C, Eigenmann PA. Antigen-specific secretory IgA antibodies in the gut are decreased in a mouse model of food allergy. J Allergy Clin Immunol. 2004; 114(2):377-382.
136. Sonnenburg JL, Angenent LT, Gordon JI. Getting a grip on things: How do communities of bacterial symbionts become established in our intestine? Nat Immunol. 2004; 5(6):569-573.
137. Dethlefsen L, Eckburg PB, Bik EM, Relman DA. Assembly of the human intestinal microbiota. Trends Ecol Evol. 2006; 21(9):517-523.
138. Björkstén B, Sepp E, Julge K, Voor T, Mikelsaar M. Allergy development and the intestinal microflora during the first year of life. J Allergy Clin Immunol. 2001; 108(4):516-520.
139. O'Hara AM, Shanahan F. The gut flora as a forgotten organ. EMBO Rep. 2006; 7(7):688-693.
140. Adlerberth I, Wold AE. Establishment of the gut microbiota in western infants. Acta Paediatr. 2009; 98(2):229-238.

86
141. Noverr MC, Huffnagle GB. Does the microbiota regulate immune responses outside the gut? Trends Microbiol. 2004; 12(12):562-568.
142. Berg RD. The indigenous gastrointestinal microflora. Trends Microbiol. 1996; 4(11):430-435.
143. Hayashi H, Takahashi R, Nishi T, Sakamoto M, Benno Y. Molecular analysis of jejunal, ileal, caecal and recto-sigmoidal human colonic microbiota using 16S rRNA gene libraries and terminal restriction fragment length polymorphism. J Med Microbiol. 2005; 54(Pt 11):1093-1101.
144. Mitsuoka T. Intestinal flora and aging. Nutr Rev. 1992; 50(12):438-446.
145. Penders J, Thijs C, Vink C, et al. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics. 2006; 118(2):511-521.
146. Dicksved J, Floistrup H, Bergstrom A, et al. Molecular fingerprinting of the fecal microbiota of children raised according to different lifestyles. Appl Environ Microbiol. 2007; 73(7):2284-2289.
147. Bäckhed F, Ley RE, Sonnenburg JL, Peterson DA, Gordon JI. Host-bacterial mutualism in the human intestine. Science. 2005; 307(5717):1915-1920.
148. Mackie RI, Sghir A, Gaskins HR. Developmental microbial ecology of the neonatal gastrointestinal tract. Am J Clin Nutr. 1999; 69(5):1035S-1045S.
149. Adlerberth I, Strachan DP, Matricardi PM, et al. Gut microbiota and development of atopic eczema in 3 european birth cohorts. J Allergy Clin Immunol. 2007; 120(2):343-350.
150. Grönlund MM, Lehtonen OP, Eerola E, Kero P. Fecal microflora in healthy infants born by different methods of delivery: Permanent changes in intestinal flora after cesarean delivery. J Pediatr Gastroenterol Nutr. 1999; 28(1):19-25.
151. Bennet R, Eriksson M, Tafari N, Nord CE. Intestinal bacteria of newborn ethiopian infants in relation to antibiotic treatment and colonisation by potentially pathogenic gram-negative bacteria. Scand J Infect Dis. 1991; 23(1):63-69.
152. Sepp E, Julge K, Vasar M, Naaber P, Björkstén B, Mikelsaar M. Intestinal microflora of estonian and swedish infants. Acta Paediatr. 1997; 86(9):956-961.
153. Adlerberth I, Carlsson B, de Man P, et al. Intestinal colonization with enterobacteriaceae in pakistani and swedish hospital-delivered infants. Acta Paediatr Scand. 1991; 80(6-7):602-610.
154. Tannock GW. What immunologists should know about bacterial communities of the human bowel. Semin Immunol. 2007; 19(2):94-105.
155. Yoshioka H, Iseki K, Fujita K. Development and differences of intestinal flora in the neonatal period in breast-fed and bottle-fed infants. Pediatrics. 1983; 72(3):317-321.
156. Midtvedt AC, Midtvedt T. Production of short chain fatty acids by the intestinal microflora during the first 2 years of human life. J Pediatr Gastroenterol Nutr. 1992; 15(4):395-403.
157. Flint HJ, Bayer EA, Rincon MT, Lamed R, White BA. Polysaccharide utilization by gut bacteria: Potential for new insights from genomic analysis. Nat Rev Microbiol. 2008; 6(2):121-131.
158. Mountzouris KC, McCartney AL, Gibson GR. Intestinal microflora of human infants and current trends for its nutritional modulation. Br J Nutr. 2002; 87(5):405-420.
159. Klijn A, Mercenier A, Arigoni F. Lessons from the genomes of bifidobacteria. FEMS Microbiol Rev. 2005; 29(3):491-509.

87
160. Flint HJ. Polysaccharide breakdown by anaerobic microorganisms inhabiting the mammalian gut. Adv Appl Microbiol. 2004; 56:89-120.
161. Collins MD, Gibson GR. Probiotics, prebiotics, and synbiotics: Approaches for modulating the microbial ecology of the gut. Am J Clin Nutr. 1999; 69(5):1052S-1057S.
162. Flint HJ, Duncan SH, Scott KP, Louis P. Interactions and competition within the microbial community of the human colon: Links between diet and health. Environ Microbiol. 2007; 9(5):1101-1111.
163. Andersson H, Asp NG, Bruce Å, Roos S, Wadström T, Wold AE. Health effects of probiotics and prebiotics. A litterature review on human studies. Scand J Nutr. 2001; 45:57-75.
164. Parracho H, McCartney AL, Gibson GR. Probiotics and prebiotics in infant nutrition. Proc Nutr Soc. 2007; 66(3):405-411.
165. Zoetendal EG, Collier CT, Koike S, Mackie RI, Gaskins HR. Molecular ecological analysis of the gastrointestinal microbiota: A review. J Nutr. 2004; 134(2):465-472.
166. Eckburg PB, Bik EM, Bernstein CN, et al. Diversity of the human intestinal microbial flora. Science. 2005; 308(5728):1635-1638.
167. Tlaskalova-Hogenova H, Stepankova R, Hudcovic T, et al. Commensal bacteria (normal microflora), mucosal immunity and chronic inflammatory and autoimmune diseases. Immunol Lett. 2004; 93(2-3):97-108.
168. Smith K, McCoy KD, Macpherson AJ. Use of axenic animals in studying the adaptation of mammals to their commensal intestinal microbiota. Semin Immunol. 2007; 19(2):59-69.
169. Ostman S, Rask C, Wold AE, Hultkrantz S, Telemo E. Impaired regulatory T cell function in germ-free mice. Eur J Immunol. 2006; 36(9):2336-2346.
170. Mazmanian SK, Liu CH, Tzianabos AO, Kasper DL. An immunomodulatory molecule of symbiotic bacteria directs maturation of the host immune system. Cell. 2005; 122(1):107-118.
171. Rakoff-Nahoum S, Paglino J, Eslami-Varzaneh F, Edberg S, Medzhitov R. Recognition of commensal microflora by toll-like receptors is required for intestinal homeostasis. Cell. 2004; 118(2):229-241.
172. Feleszko W, Jaworska J, Rha RD, et al. Probiotic-induced suppression of allergic sensitization and airway inflammation is associated with an increase of T regulatory-dependent mechanisms in a murine model of asthma. Clin Exp Allergy. 2007; 37(4):498-505.
173. Marschan E, Kuitunen M, Kukkonen K, et al. Probiotics in infancy induce protective immune profiles that are characteristic for chronic low-grade inflammation. Clin Exp Allergy. 2008; 38(4):611-618.
174. Taylor AL, Hale J, Wiltschut J, Lehmann H, Dunstan JA, Prescott SL. Effects of probiotic supplementation for the first 6 months of life on allergen- and vaccine-specific immune responses. Clin Exp Allergy. 2006; 36(10):1227-1235.
175. Lundell AC, Adlerberth I, Lindberg E, et al. Increased levels of circulating soluble CD14 but not CD83 in infants are associated with early intestinal colonization with Staphylococcus aureus. Clin Exp Allergy. 2007; 37(1):62-71.
176. Hessle CC, Andersson B, Wold AE. Gram-positive and gram-negative bacteria elicit different patterns of pro-inflammatory cytokines in human monocytes. Cytokine. 2005; 30(6):311-318.
177. Karlsson H, Larsson P, Wold AE, Rudin A. Pattern of cytokine responses to gram-positive and gram-negative commensal bacteria is profoundly changed when monocytes differentiate into dendritic cells. Infect Immun. 2004; 72(5):2671-2678.
88
178. Drakes M, Blanchard T, Czinn S. Bacterial probiotic modulation of dendritic cells. Infect Immun. 2004; 72(6):3299-3309.
179. Braat H, de Jong EC, van den Brande JM, et al. Dichotomy between Lactobacillus rhamnosus and Klebsiella pneumoniae on dendritic cell phenotype and function. J Mol Med. 2004; 82(3):197-205.
180. Smits HH, Engering A, van der Kleij D, et al. Selective probiotic bacteria induce IL-10-producing regulatory T cells in vitro by modulating dendritic cell function through dendritic cell-specific intercellular adhesion molecule 3-grabbing nonintegrin. J Allergy Clin Immunol. 2005; 115(6):1260-1267.
181. Niers LE, Timmerman HM, Rijkers GT, et al. Identification of strong interleukin-10 inducing lactic acid bacteria which down-regulate T helper type 2 cytokines. Clin Exp Allergy. 2005; 35(11):1481-1489.
182. Young SL, Simon MA, Baird MA, et al. Bifidobacterial species differentially affect expression of cell surface markers and cytokines of dendritic cells harvested from cord blood. Clin Diagn Lab Immunol. 2004; 11(4):686-690.
183. Adlerberth I, Lindberg E, Åberg N, et al. Reduced enterobacterial and increased staphylococcal colonization of the infantile bowel: An effect of hygienic lifestyle? Pediatr Res. 2006; 59(1):96-101.
184. Alm JS, Swartz J, Lilja G, Scheynius A, Pershagen G. Atopy in children of families with an anthroposophic lifestyle. Lancet. 1999; 353(9163):1485-1488.
185. Björkstén B, Naaber P, Sepp E, Mikelsaar M. The intestinal microflora in allergic Estonian and Swedish 2-year-old children. Clin Exp Allergy. 1999; 29(3):342-346.
186. He F, Ouwehand AC, Isolauri E, Hashimoto H, Benno Y, Salminen S. Comparison of mucosal adhesion and species identification of bifidobacteria isolated from healthy and allergic infants. FEMS Immunol Med Microbiol. 2001; 30(1):43-47.
187. Murray CS, Tannock GW, Simon MA, et al. Fecal microbiota in sensitized wheezy and non-sensitized non-wheezy children: A nested case-control study. Clin Exp Allergy. 2005; 35(6):741-745.
188. Kalliomäki M, Kirjavainen P, Eerola E, Kero P, Salminen S, Isolauri E. Distinct patterns of neonatal gut microflora in infants in whom atopy was and was not developing. J Allergy Clin Immunol. 2001; 107(1):129-134.
189. Penders J, Thijs C, van den Brandt PA, et al. Gut microbiota composition and development of atopic manifestations in infancy: The KOALA birth cohort study. Gut. 2007; 56(5):661-667.
190. Penders J, Stobberingh EE, Thijs C, et al. Molecular fingerprinting of the intestinal microbiota of infants in whom atopic eczema was or was not developing. Clin Exp Allergy. 2006; 36(12):1602-1608.
191. Labbok MH, Clark D, Goldman AS. Breastfeeding: Maintaining an irreplaceable immunological resource. Nat Rev Immunol. 2004; 4(7):565-572.
192. Field CJ. The immunological components of human milk and their effect on immune development in infants. J Nutr. 2005; 135(1):1-4.
193. Brandtzaeg P. Mucosal immunity: Integration between mother and the breast-fed infant. Vaccine. 2003; 21(24):3382-3388.
194. Newburg DS, Walker WA. Protection of the neonate by the innate immune system of developing gut and of human milk. Pediatr Res. 2007; 61(1):2-8.
195. Admyre C, Johansson SM, Qazi KR, et al. Exosomes with immune modulatory features are present in human breast milk. J Immunol. 2007; 179(3):1969-1978.
89
196. Mimouni Bloch A, Mimouni D, Mimouni M, Gdalevich M. Does breastfeeding protect against allergic rhinitis during childhood? A meta-analysis of prospective studies. Acta Paediatr. 2002; 91(3):275-279.
197. Kull I, Almqvist C, Lilja G, Pershagen G, Wickman M. Breast-feeding reduces the risk of asthma during the first 4 years of life. J Allergy Clin Immunol. 2004; 114(4):755-760.
198. Kull I, Bohme M, Wahlgren CF, Nordvall L, Pershagen G, Wickman M. Breast-feeding reduces the risk for childhood eczema. J Allergy Clin Immunol. 2005; 116(3):657-661.
199. Ludvigsson JF, Moström M, Ludvigsson J, Duchén K. Exclusive breastfeeding and risk of atopic dermatitis in some 8300 infants. Pediatr Allergy Immunol. 2005; 16(3):201-208.
200. Friedman NJ, Zeiger RS. The role of breast-feeding in the development of allergies and asthma. J Allergy Clin Immunol. 2005; 115(6):1238-1248.
201. Duchén K, Björkstén B. Polyunsaturated n-3 fatty acids and the development of atopic disease. Lipids. 2001; 36(9):1033-1042.
202. Böttcher MF, Jenmalm MC, Garofalo RP, Björkstén B. Cytokines in breast milk from allergic and nonallergic mothers. Pediatr Res. 2000; 47(1):157-162.
203. Amoudruz P, Holmlund U, Schollin J, Sverremark-Ekström E, Montgomery SM. Maternal country of birth and previous pregnancies are associated with breast milk characteristics. Pediatr Allergy Immunol. 2009; 20(1):19-29.
204. Verhasselt V, Milcent V, Cazareth J, et al. Breast milk-mediated transfer of an antigen induces tolerance and protection from allergic asthma. Nat Med. 2008; 14(2):170-175.
205. Newburg DS, Ruiz-Palacios GM, Morrow AL. Human milk glycans protect infants against enteric pathogens. Annu Rev Nutr. 2005; 25:37-58.
206. Coppa GV, Zampini L, Galeazzi T, Gabrielli O. Prebiotics in human milk: A review. Dig Liver Dis. 2006; 38 Suppl 2:S291-4.
207. Coppa GV, Bruni S, Morelli L, Soldi S, Gabrielli O. The first prebiotics in humans: Human milk oligosaccharides. J Clin Gastroenterol. 2004; 38(6 Suppl):S80-3.
208. Kunz C, Rudloff S, Baier W, Klein N, Strobel S. Oligosaccharides in human milk: Structural, functional, and metabolic aspects. Annu Rev Nutr. 2000; 20:699-722.
209. Boehm G, Stahl B. Oligosaccharides from milk. J Nutr. 2007; 137:847S-9S.
210. Bode L. Recent advances on structure, metabolism, and function of human milk oligosaccharides. J Nutr. 2006; 136(8):2127-2130.
211. Ward RE, Ninonuevo M, Mills DA, Lebrilla CB, German JB. In vitro fermentation of breast milk oligosaccharides by Bifidobacterium infantis and Lactobacillus gasseri. Appl Environ Microbiol. 2006; 72(6):4497-4499.
212. Bezkorovainy A. Probiotics: Determinants of survival and growth in the gut. Am J Clin Nutr. 2001; 73:399S-405S.
213. Morrow AL, Ruiz-Palacios GM, Jiang X, Newburg DS. Human-milk glycans that inhibit pathogen binding protect breast-feeding infants against infectious diarrhea. J Nutr. 2005; 135(5):1304-1307.
214. Hanifin J.M., Rajka G. Diagnostic features of atopic dermatitis. Acta Dermatol Venerol. 1980; 92:44-47.
215. Voor T, Julge K, Böttcher MF, Jenmalm MC, Duchen K, Björkstén B. Atopic sensitization and atopic dermatitis in Estonian and Swedish infants. Clin Exp Allergy. 2005; 35(2):153-159.

90
216. Erney RM, Malone WT, Skelding MB, et al. Variability of human milk neutral oligosaccharides in a diverse population. J Pediatr Gastroenterol Nutr. 2000; 30(2):181-192.
217. Sumiyoshi W, Urashima T, Nakamura T, et al. Determination of each neutral oligosaccharide in the milk of Japanese women during the course of lactation. Br J Nutr. 2003; 89(1):61-69.
218. Newburg DS. Are all human milks created equal? variation in human milk oligosaccharides. J Pediatr Gastroenterol Nutr. 2000; 30(2):131-133.
219. Moro G, Arslanoglu S, Stahl B, Jelinek J, Wahn U, Boehm G. A mixture of prebiotic oligosaccharides reduces the incidence of atopic dermatitis during the first six months of age. Arch Dis Child. 2006; 91(10):814-819.
220. Ahrné S, Lönnermark E, Wold AE, et al. Lactobacilli in the intestinal microbiota of Swedish infants. Microbes Infect. 2005; 7(11-12):1256-1262.
221. Sakata S, Tonooka T, Ishizeki S, et al. Culture-independent analysis of fecal microbiota in infants, with special reference to Bifidobacterium species. FEMS Microbiol Lett. 2005; 243(2):417-423.
222. He F, Morita H, Hashimoto H, et al. Intestinal bifidobacterium species induce varying cytokine production. J Allergy Clin Immunol. 2002; 109(6):1035-1036.
223. Martin R, Jimenez E, Heilig H, et al. Isolation of bifidobacteria from breast milk and assessment of the bifidobacterial population by PCR-denaturing gradient gel electrophoresis and quantitative real-time PCR. Appl Environ Microbiol. 2009; 75(4):965-969.
224. Grönlund MM, Gueimonde M, Laitinen K, et al. Maternal breast-milk and intestinal bifidobacteria guide the compositional development of the Bifidobacterium microbiota in infants at risk of allergic disease. Clin Exp Allergy. 2007; 37(12):1764-1772.
225. Suzuki S, Shimojo N, Tajiri Y, Kumemura M, Kohno Y. Differences in the composition of intestinal Bifidobacterium species and the development of allergic diseases in infants in rural Japan. Clin Exp Allergy. 2007; 37(4):506-511.
226. Wexler HM. Bacteroides: The good, the bad, and the nitty-gritty. Clin Microbiol Rev. 2007; 20(4):593-621.
227. Penders J, Stobberingh EE, van den Brandt PA, van Ree R, Thijs C. Toxigenic and non-toxigenic Clostridium difficile: Determinants of intestinal colonisation and role in childhood atopic manifestations. Gut. 2008; 57(7):1025-1026.
228. Kalliomäki M, Salminen S, Arvilommi H, Kero P, Koskinen P, Isolauri E. Probiotics in primary prevention of atopic disease: A randomised placebo-controlled trial. Lancet. 2001; 357(9262):1076-1079.
229. Abrahamsson TR, Jakobsson T, Böttcher MF, et al. Probiotics in prevention of IgE-associated eczema: A double-blind, randomized, placebo-controlled trial. J Allergy Clin Immunol. 2007; 119(5):1174-1180.
230. Wickens K, Black PN, Stanley TV, et al. A differential effect of 2 probiotics in the prevention of eczema and atopy: A double-blind, randomized, placebo-controlled trial. J Allergy Clin Immunol. 2008; 122(4):788-794.
231. Braat H, van den Brande J, van Tol E, Hommes D, Peppelenbosch M, van Deventer S. Lactobacillus rhamnosus induces peripheral hyporesponsiveness in stimulated CD4+ T cells via modulation of dendritic cell function. Am J Clin Nutr. 2004; 80(6):1618-1625.
232. Lowe AJ, Hosking CS, Bennett CM, et al. Skin prick test can identify eczematous infants at risk of asthma and allergic rhinitis. Clin Exp Allergy. 2007; 37(11):1624-1631.

91
233. Gore C, Munro K, Lay C, et al. Bifidobacterium pseudocatenulatum is associated with atopic eczema: A nested case-control study investigating the fecal microbiota of infants. J Allergy Clin Immunol. 2008; 121(1):135-140.
234. Stsepetova J, Sepp E, Julge K, Vaughan E, Mikelsaar M, de Vos WM. Molecularly assessed shifts of Bifidobacterium ssp. and less diverse microbial communities are characteristic of 5-year-old allergic children. FEMS Immunol Med Microbiol. 2007; 51(2):260-269.
235. He F, Morita H, Ouwehand AC, et al. Stimulation of the secretion of pro-inflammatory cytokines by Bifidobacterium strains. Microbiol Immunol. 2002; 46(11):781-785.
236. Böttcher MF, Nordin EK, Sandin A, Midtvedt T, Björkstén B. Microflora-associated characteristics in faeces from allergic and nonallergic infants. Clin Exp Allergy. 2000; 30(11):1590-1596.
237. Wang M, Karlsson C, Olsson C, et al. Reduced diversity in the early fecal microbiota of infants with atopic eczema. J Allergy Clin Immunol. 2008; 121(1):129-134.
238. Lauener RP, Birchler T, Adamski J, et al. Expression of CD14 and toll-like receptor 2 in farmers' and non-farmers' children. Lancet. 2002; 360(9331):465-466.
239. Lappalainen MH, Roponen M, Hyvarinen A, et al. Exposure to environmental bacteria may have differing effects on tumour necrosis factor-alpha and interleukin-6-producing capacity in infancy. Clin Exp Allergy. 2008; 38(9):1483-1492.
240. Mazmanian SK, Kasper DL. The love-hate relationship between bacterial polysaccharides and the host immune system. Nat Rev Immunol. 2006; 6(11):849-858.
241. Mazmanian SK, Round JL, Kasper DL. A microbial symbiosis factor prevents intestinal inflammatory disease. Nature. 2008; 453(7195):620-625.
242. Externest D, Meckelein B, Schmidt MA, Frey A. Correlations between antibody immune responses at different mucosal effector sites are controlled by antigen type and dosage. Infect Immun. 2000;68:3830-39.
243. Lundell AC, Hesselmar B, Nordström I, et al. High circulating immunoglobulin A levels in infants are associated with intestinal toxigenic Staphylococcus aureus and a lower frequency of eczema. Clin Exp Allergy. 2009 Epub ahead of print.
244. Kang W, Kudsk KA. Is there evidence that the gut contributes to mucosal immunity in humans? JPEN J Parenter Enteral Nutr. 2007; 31(3):246-258.
245. Kalliomäki M, Salminen S, Poussa T, Isolauri E. Probiotics during the first 7 years of life: A cumulative risk reduction of eczema in a randomized, placebo-controlled trial. J Allergy Clin Immunol. 2007; 119(4):1019-1021.
246. Kopp MV, Hennemuth I, Heinzmann A, Urbanek R. Randomized, double-blind, placebo-controlled trial of probiotics for primary prevention: No clinical effects of Lactobacillus GG supplementation. Pediatrics. 2008; 121(4):e850-6.
247. Taylor AL, Dunstan JA, Prescott SL. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: A randomized controlled trial. J Allergy Clin Immunol. 2007; 119(1):184-191.
248. Kukkonen K, Savilahti E, Haahtela T, et al. Probiotics and prebiotic galacto-oligosaccharides in the prevention of allergic diseases: A randomized, double-blind, placebo-controlled trial. J Allergy Clin Immunol. 2007; 119(1):192-198.
249. Kuitunen M, Kukkonen K, Juntunen-Backman K, et al. Probiotics prevent IgE-associated allergy until age 5 years in cesarean-delivered children but not in the total cohort. J Allergy Clin Immunol. 2009; 123(2):335-341.
92
250. Koplin J, Allen K, Gurrin L, Osborne N, Tang ML, Dharmage S. Is caesarean delivery associated with
sensitization to food allergens and IgE-mediated food allergy: A systematic review. Pediatr Allergy Immunol. 2008; 19(8):682-687.
251. LeBouder E, Rey-Nores JE, Raby AC, et al. Modulation of neonatal microbial recognition: TLR-mediated innate immune responses are specifically and differentially modulated by human milk. J Immunol. 2006; 176(6):3742-3752.
252. Zeuthen LH, Fink LN, Frokiaer H. Epithelial cells prime the immune response to an array of gut-derived commensals towards a tolerogenic phenotype through distinct actions of thymic stromal lymphopoietin and transforming growth factor-beta. Immunology. 2008; 123(2):197-208.
253. O'Hara AM, O'Regan P, Fanning A, et al. Functional modulation of human intestinal epithelial cell responses by Bifidobacterium infantis and Lactobacillus salivarius. Immunology. 2006; 118(2):202-215.
254. Willing B, Halfvarson J, Dicksved J, et al. Twin studies reveal specific imbalances in the mucosa-associated microbiota of patients with ileal crohn's disease. Inflamm Bowel Dis. 2008;15:653-660 .
255. Ley RE, Turnbaugh PJ, Klein S, Gordon JI. Microbial ecology: Human gut microbes associated with obesity. Nature. 2006; 444(7122):1022-1023.
256. Wen L, Ley RE, Volchkov PY, et al. Innate immunity and intestinal microbiota in the development of type 1 diabetes. Nature. 2008; 455(7216):1109-1113.
257. Bäckhed F, Ding H, Wang T, et al. The gut microbiota as an environmental factor that regulates fat storage. Proc Natl Acad Sci U S A. 2004; 101(44):15718-15723.