early breast cancer therapy
DESCRIPTION
Early breast cancer is nowadays seen often and is the major cause of morbidity to general population.TRANSCRIPT

SURGICAL TREATMENT OPTIONS IN MANAGEMENT
OF BREAST CANCER
CHAIRPERSONS – PROF. N. C. NATH DR. A. MAJI
PRESENTED BY – DR. IPSEET MISHRA

HISTORICAL ASPECT
o EGYPTIANS – COULD NOT BELIEVE BREAST CANCER COULD BE CURED
o GALEN & ALUBUCASIS – STARTED REMOVING BREAST TUMOURS
o AMBROISE PARE – FIRST TO RECOGNIZE ROLE OF AXILLARY LYMPH NODES IN BREAST CANCER
o W H HALSTEAD – FIRST TO PERFORM RADICAL MASTECTOMY – EN BLOC REMOVAL OF BREAST WITH LYMPHATICS AND BOTH PECTORALIS MUSCLES IN 1882
o D H PATEY – PECTORALIS MAJOR MUSCLE WAS NOT REMOVED D/T EXCESS BLOOD LOSS AND COSMETIC DEFORMITY. REMOVAL OF PECTORALIS MINOR WAS DONE FOR AXILLARY CLEARANCE –PATEY MODIFICATION
o R NOER & B FISHER – INITIATED NSABP TRIAL AND SUPPORTED USE OF SEGMENTECTOMY

EXCISIONAL BIOPSY WITH NEEDLE LOCALIZATION
Complete removal of breast lesion with a margin of normal appearing breast tissue
Reserved for cases where needle core biopsy results are discordant with imaging findings or needle localization.
Requires a pre-operative visit to mammography suite for placement of localization wire or radiolabelled seed that can be detected intra-operatively with handheld probe or can be targeted by sonography in imaging suite or operating room.
Specimen radiography is always performed after excision of suspicious lesion to confirm complete excision with appropriate margins.
Impalpable lesions localized prior to surgery using Skin marking, Injection of Blue dye, Carbon or Radioisotope, insertion of a Hook wire with postlocalization mammograms , or by intraoperative ultrasound.
If the lesion localized by ultrasound, the skin directly over the cancer is marked along with the depth of the cancer below the skin by the radiologist.
If the lesion is only visible on the mammograms, it is usually possible for the surgeon to locate the skin directly over the lesion. If dissection continues toward the wire in place, it can be located above where it enters the lesion.
Radio-guided occult lesion localization is a newer technique. Under mammogram or ultrasound control technetium-labelled human serum albumin or sulfur colloid is injected into the tumor. The surgeon then uses a handheld gamma-detecting probe intraoperatively to locate the lesion to guide excision.

Diagrammatic representation of mammograms illustratingthe position of a hook wire in relation to the area ofmicro calcification. A: Lateral view. B: Craniocaudal view.
Planned incision over area of microcalcification.

BREAST CONSERVING SURGERY
- Lumpectomy / Segmentectomy / Partial mastectomy / Wide local excision - Aim – Achieving long term local disease control with minimum local morbidity
- Defined as complete surgical resection of a primary tumour with wide negative margins ideally 1cm. - INDICATIONS – T1, T2 (<4CM), N0 , N1, M0 - T2 > 4CM
- SINGLE CLINICAL AND MAMMOGRAPHIC LESION
- ADVANTAGES : Survival outcomes are same for BCS or mastectomy whichever is performed. Aesthetic outcome more with preservation of Breast shape, skin or sensation. Lesser psychological morbidity of patients than those with mastectomy.

- INCISIONS FOR BCS – Periareolar incision for centrally placed lesion , - Curvilinear incision for peripherally located lesion, - Radial incision for lower quadrants.
- In general, scars that are parallel both to the lines of maximum resting skin tension and to the orientation of collagen fibers produce the best cosmetic incisions with least hypertrophy and keloid formation. - The cosmetic result after BCT is influenced by the amount of skin excised and length of incision.
The direction of Langer's lines (A) and the lines of maximum resting skin tension in the breast (the so called dynamic lines of Kraissl)

When elevating skin, it is important not to disrupt the subcutaneous fat as thin skin flaps has a poor cosmetic result.
The skin flaps should be elevated 1 to 2 cm beyond the edge of the cancer. The line of incision should be 1 cm beyond the limit of the palpable mass.
It is usually but not always necessary to remove full thickness of breast tissue. To ensure that there is an adequate margin deep to the cancer for the majority of patients, dissection through the breast tissue is continued down to the pectoral fascia and the breast tissue containing the cancer is lifted off the pectoral fascia.
It is not necessary to excise pectoral fascia unless it is tethered to the tumor. A portion of the affected muscle should be removed beneath the tumor if a carcinoma is infiltrating one of the chest wall muscles.
The specimen is immediately orientated prior to submission to the pathologist with sutures, ligacllps, or metal markers. Metal markers or ligaclips allows anteroposterior orientation for intraoperative specimen radiography that helps the surgeon to assess the completeness of excision at all margins. If the specimen radiograph shows that the cancer or any associated microcalcification is close to a radial margin, then the surgeon can remove further tissue from the margin.
Having excised the cancer from the breast suturing the defect in the breast without mobilization of the breast tissue usually results in distortion of the breast contour.
Small defects ( <5% breast volume) can be left open and can produce a good final cosmetic result.
Large defects in the breast should be closed by mobilizing the surrounding breast tissue from both the overlying skin and subcutaneous tissue and the underlying chest wall.

Large defects(> 10% breast volume) can be filled by using a LD muscle, TRAM flaps, or more major breast reshaping as part of a unilateral or bilateral therapeutic mammoplasty.
Drains are not necessary following wide local excision and should not be used routinely. They do not protect against hematoma formation and increase infection rates.
Breast skin wounds should be closed in layers with absorbable sutures. finishing with a subcuticular suture.
Staples and interrupted sutures are not an acceptable method of wound closure in the breast.
- CONTRADICTIONS – Absolute – T4, N2, M1 - clinically evident multifocal or multicentric
disease - h/o previous irradiation or inability to
undergo radiation - 1st or 2nd trimester of pregnancy - persistent positive margins after previous BCS - patients who prefer mastectomy - Relative – small breast size - large or central tumours in small breasts - collagen vascular diseases - strong family h/o breast cancer or BRCA 1/2 mutation carriers
Radiation therapy ± systemic therapy are must after BCS. SLN is performed before removal of primary tumour for axillary staging. The use of Oncoplastic techniques can be performed at the time of BCS or at a later time to
improve aesthetic outcome.

FACTORS RESULTING IN POOR SURGICAL OUTCOME IN BCS - Large breast size - Increasing tumour size - Large volume of breast tissue removed - Central tumour size - Re-excision procedure - Increasing scar length - Post-operative complications - Associated axillary dissection - Increasing dose of radiotherapy - Chemotherapy

TOTAL MASTECTOMY - complete removal of all breast tissue from subclavius superiorly, sternal border medially, inferiorly 3-4cm down the infra-mammary fold, laterally anterior margin of latissimus dorsi with en-bloc resection of pectoralis major fascia - Indications – Risk reducing mastectomy - Local recurrence in previously treated breast cancer - Palliative treatment in metastatic breast cancer - Malignant phylloides tumour
RADICAL MASTECTOMY - Total mastectomy plus en bloc resection of the pectoralis muscles and ALND ( complete level I-III axillary LN dissection)
EXTENDED RADICAL MASTECTOMY - Radical mastectomy with resection of internal mammary lymph nodes

MODIFIED RADICAL MASTECTOMY - Total mastectomy with axillary lymph node dissection
VARIOUS MODIFICATIONS OF MODIFIED RADICAL MASTECTOMY
- PATEY MODIFICATION : pectoralis minor is divided to allow axillary clearance
- SCANLON MODIFICATION : pectoralis minor is divided but not removed that allows level III dissection
- AUCHINCLOSS MODIFICATION : pectoralis minor is retracted that allows only level I & II dissection
OTHER VARIATIONS OF MASTECTOMY :
- SKIN SPARING TOTAL MASTECTOMY (SSM) AND NIPPLE SPARING TOTAL MASTECTOMY (NSM)
- Minimally invasive surgical approaches that are technically more difficult and thus more time consuming than traditional method.
- Gives same extent of resection with preservation of skin envelope and position of infra-mammary fold.
- Preferred for Early stage breast cancer patients who elect to have immediate reconstruction.
- Not appropriate for - cancers near skin or nipple - locally advanced or inflammatory breast carcinoma.
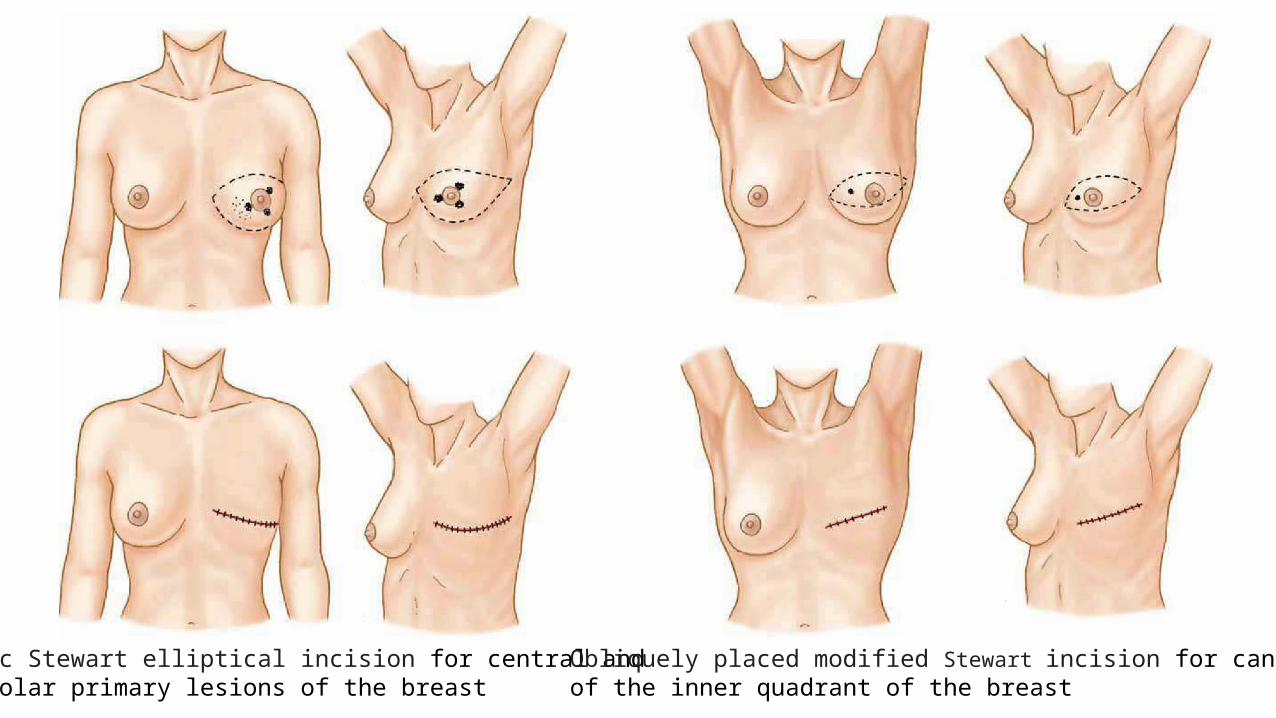
Classic Stewart elliptical incision for central and subareolar primary lesions of the breast
Obliquely placed modified Stewart incision for cancer of the inner quadrant of the breast
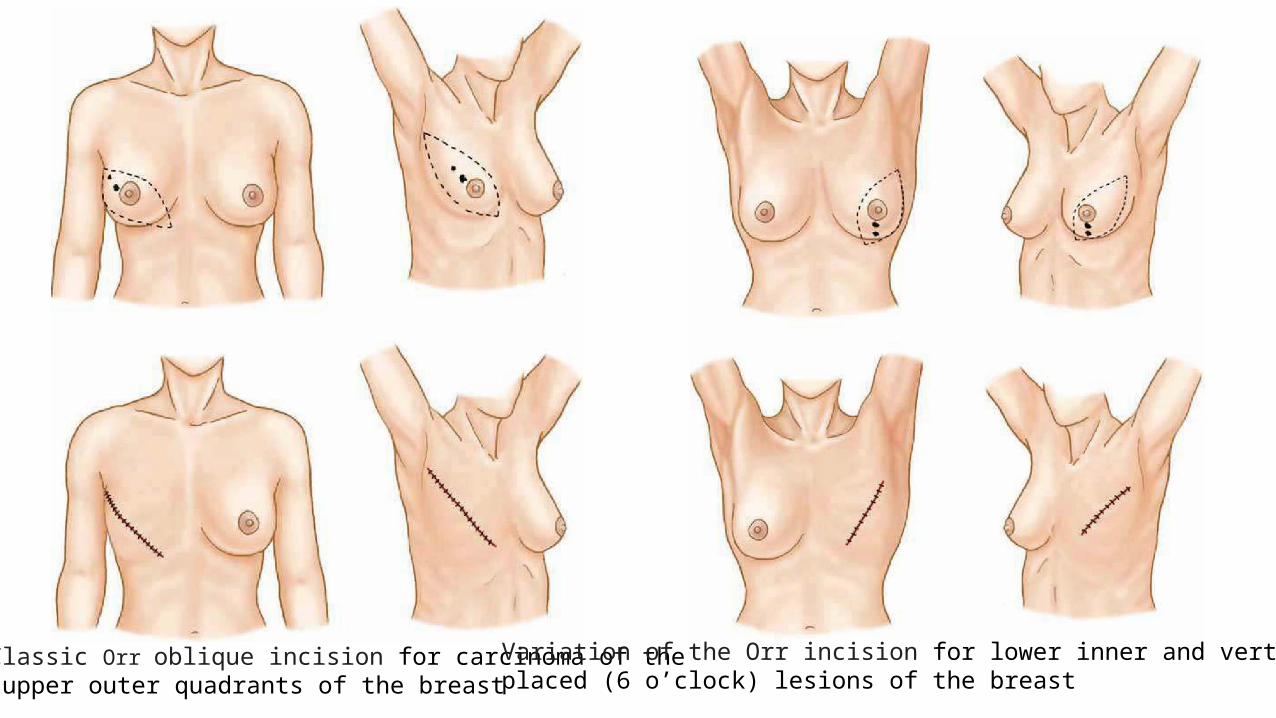
Classic Orr oblique incision for carcinoma of the upper outer quadrants of the breast
Variation of the Orr incision for lower inner and vertically placed (6 o’clock) lesions of the breast

Flaps are developed at boundaries of dissection for MRM with electocautery or scalpel – 1. anterior margin of LD laterally
2. Midline of sternum medially 3. subclavius superiorly and 4. 3-4 cm inferior to infra-mammary fold inferiorly.
Skin flaps include skin and tela subcutanea and the appropriate dissection plane is deep to subcutaneous vasculature and superficial to vessels of breast parenchyma.
Skin flap is raised with consistent thickness to avoid creation of devascularized subcutaneous tissues that can contribute to wound seroma, skin necrosis and flap retraction.
Perforators from lateral thoracic arteries or anterior intercostal arteries supplying pectoralis muscles should be identified and ligated.
Lateral neurovascular bundle containing medial pectoral nerve should be preserved to prevent atrophy of pectoralis muscle.

COMPLICATIONS OF MASTECTOMY : Seromas beneath skin flaps or in the axilla – Reduced by use of closed system suction drain.
Wound infections – infrequent, majority after skin flap necrosis – managed with C/S of specimen, debridement and effective antibiotic therapy.
Haemorrhage – managed with early wound exploration and re-establishment of closed system suction drain.
Lymphedema – incidence 20% but can be 50-60% after post-operative radiation – early PMR referral and use of individually fitted compressive sleeves.
Local – regional recurrence of breast cancer –
1. Women treated with BCS before should undergo mastectomy and appropriate reconstruction alongwith chemotherapy ± antiestrogen therapy.
2. Women treated with mastectomy previously should undergo resection of recurrence and appropriate reconstruction alongwith chemotherapy ± antiestrogen therapy. Radiation therapy to be given if chest wall has not been previously radiated or by opinion of radiation oncologist.
