adjuvant endocrine therapy for postmenopausal breast cancer
TRANSCRIPT

Adjuvant Endocrine Therapy For Hormone Positive Breast Cancer
Postmenopausal WomenEmad Shash MBBCh., MSc., MD.
Medical Oncology Department
National Cancer Institute, Cairo University

Female Menstrual & Reproductive Period Definitions
Menarche Menopause
Premenopausal Period Postmenopausal PeriodPerimenopausal Period
Menopause is diagnosed after 12 months of
amenorrhea 1, 2
NCCN Definition (Aimed to standardize definition across Clinical trials initially) 3: • Prior bilateral oophorectomy.• 60 or older.• If Age < 60 years, the female should be:
• Amenorrhea for 12 or more months in the absence of: • chemotherapy• tamoxifen, toremifene, or ovarian suppression
• If receiving cancer directed therapy: follicle-stimulating hormone (FSH) and plasma estradiol in the postmenopausal range.
• It is not possible to assign menopausal status to women who are receiving LHRH agonist or antagonist.
• In women premenopausal at the time of adjuvant chemotherapy, amenorrhea is not a reliable indicator of menopausal status.
1 Butler L, Santoro N. Steroids 20112 Santoro N, Randolph JF Jr. Obstet Gynecol Clin North Am 2011
3 NCCN Guidelines version 1.2017 [accessed April 2017]
A female Life Time Story

Breast Cancer Snapshot
SEER 18 2009-2013, All Races, Females
Median Age at Diagnosis
62 years old
Age at Diagnosis by Menopausal Status
Premenopausal
Perimenopausal
Postmenopausal
More than 90% of patients are either postmenopausal or will
get menopausal
seer.cancer.gov [accessed April 2017]

Breast Cancer & Hormonal Status
• Around 60-70% patients diagnosed to have breast cancer are Estrogen receptor-positive
(65% of these are also positive for Progesterone receptors)
• Patients with (ER+) tumours have a better survival than (ER-) tumours
• Patients with ER + tumours are candidates for hormonal therapy

1896 19751896 1904 1912 1920 1928 1936 1944 1952 1960 1970
First Use of Hormonal Therapy in Cancer Treatment
Tamoxifen (ICI-46474) First Development
1st Clinical Study of Tamoxifen in Advanced Breast Cancer
Tamoxifien Dose Optimization
1st Work done on AI in Breast Cancer
Surgical Oopherectomy for Advanced Breast Cancer
1896 – Dr George Beaston• Significant tumor regression• Sense of well being• Reduction in cutaneous metastases• No effect on osseous metastases• Best above age of 40 years
1941 – Dr Charles Higgins
1966 – Dr Arthur L Walpole/Dr Dora Richardson
Developed Tamoxifen (ICI-46474) as a Contraceptive “Morning After Pill”Never proved useful in human contraception
History & Evolution

Endocrine Therapies Development for Breast Cancer
Lim E, et al. Oncology (Williston Park) 2012. Croxtall JD, et al. Drugs. 2011.

Rationale for Endocrine Therapy
• Estrogen: • Steroid hormone
• Profound proliferative effect on normal human mammary epithelium through its activation of ER-alpha, a classic nuclear hormone receptor
• Estrogen promotes the growth of breast cancer by binding to and activating the Estrogen Receptor (ER)

3 possible ways to interrupt this process
Reduce estrogen production
Down regulate receptor
Interfere with
receptor binding
Tamoxifen & SERMs
Fulvestrant
Premenopausal (LHRH)Postmenopausal (AI)
But we need to understand how to use them wisely!!
Case Presentation: Postmenopausal Patient
• 62 year old female with suspicious micro calcifications on screening mammography
• Biopsy: • IDC grade 2, hormone +with high grade DCIS. • Patient underwent lumpectomy with SLN
• Final pathology: • 1.2 cm grade 2 IDC with high grade DCIS. • SLN 0/1 T1cN0 Stage IA
• Oncotype Dx Recurrence Score – low risk

Considerations in Postmenopausal Patients(What will be discussed today?)
• Peripheral conversion of androgen to estrogen by aromatase - main source of estrogen and primary target of therapy
• Questions:• Should she receive an AI or Tamoxifen?
• Should she receive monotherapy (AI or Tamoxifen alone) or sequential therapy using both?
• 5 vs 10 years of therapy?
• If More than 5 years of endocrine therapy, which class to be used?

Tamoxifen for 1, 2 or 5 years!What the Historical Data tells us? “Recurrence”
Early Breast Cancer Trialists' Collaborative Group. Lancet 2011
∆ 8 % ∆ 8.8 % ∆ 14.2 %

Tamoxifen for 1, 2 or 5 years!What the Historical Data tells us? “Mortality”
Early Breast Cancer Trialists' Collaborative Group. Lancet 2011
∆ 5.8 % ∆ 6.1 % ∆ 7.2 %

Tamoxifen “5years” Long Term Effect: Perimenopausal & Postmenopausal
Early Breast Cancer Trialists' Collaborative Group. Lancet 2011

Can we do better than TAM For 5 years?
Quantity of life
Quality of life

0 2 3 5 10
RTAM
AI
UpfrontATACBIG 1-98ABCSG 12TEAM
Questions addressed in Randomized Clinical Trials (Can we do better than TAM X 5 years)?
A Breast Cancer female Life Time Story
# 1st Question

ATAC Trial (AI Superiority over Tamoxifen in postmenopausal females)
Ran
do
miz
e Tamoxifen 20 mg X 5 Years (N: 3116)
Anastrazole 1 mg X 5 Years (N: 3125)
Tamoxifen + Anastrazole X 5 Years (N: 3125)
Postmenopausal women with
histologically proven operable invasive breast cancer who
had completed primary surgery and
chemotherapy (where given), and were candidates to receive hormonal adjuvant therapy*
(N = 9366)
Baum M, et al. Lancet 2002Cuzick et al. Lancet Oncol 2010
* At the time the ATAC trial was started, patients with negative or unknown hormone-receptor status were included because hormone-receptor-negative patients were thought to derive benefit from adjuvant therapy with a hormonal agent.
time to recurrence in hormone-receptor-positive patientsFirst reported results
time to recurrence in hormone-receptor-positive patientsUpdated 10 years results

BIG 1-98 Study Design
Thurlimann B et al. N Eng J Med 2005
0 2 3 51 4
Tamoxifen Letrazole
TamoxifenLetrazole
Letrazole
Tamoxifen
4 arm option (1999-2003)
A
B
C
D
Letrazole
Tamoxifen
2 arm option (1998-2000)
A
B
N= 911
N= 917
N= 1548
N= 1546
N= 1548
N= 1546
• 1ry endpoint: disease-free survival (DFS) • 2ry endpoints: overall survival (OS),
invasive breast cancer-free interval (BCFI), and distant recurrence-free interval (DRFI)
Randomized, phase III, double-blind trial that recruited 8010 postmenopausal Hormone positive women early breast cancer.

AI Superiority Confirmed with BIG 1-98 (Long Term Benefit)
Thurlimann B et al. N Eng J Med 2005 Thurlimann B et al. SABCS 2016
Confirmed Benefit at 10 years updated analysis!

5 Years AI Vs. TamoxifenMeta-analysis Conclude & Consolidate Evidence
Early Breast Cancer Trialists' Collaborative Group. Lancet 2015

0 2 3 5 10
RTAM
AI
TAM RTAM
AITAM
UpfrontATACBIG 1-98ABCSG 12TEAM
SequentialBIG 1-98IESITANSAS BC-03ARNO 95ABCSG 8
Questions addressed in Randomized Clinical Trials (Can we do better than TAM X 5 years)?
A Breast Cancer female Life Time Story
# 1st Question
# 2nd Question

Switching to AI (Anastrazole) after 2-3 years of TAM better than 5 years Tamoxifen
Jonat W et al. Lancet Oncol 2006
These findings gives a clear message to clinicians “consider switching postmenopausal women who have taken adjuvant tamoxifen for 2–3 years
to anastrozole”

BIG 1-98: Sequential Strategy is not bad VS Letrazole Monotherapy!
There were no statistically significant differences in OS, DRFI, or BCFI for either sequence compared with letrozole monotherapy
Regan MM et al. Lancet Oncol 2011

Switching strategy: starting with Tamoxifen is equal to an upfront AI
No significant difference in DFS between the arms
Tamoxifen Exemestane
TEAM trial
Tamoxifen Exemestane Adjuvant Multinational Trial
Van de Velde et al. Lancet 2011
9775 postmenopausal hormone positive patients randomized to Aromasin vssequential TAM/Aromasin
Exemestane
0 2 3 51 4

0 2 3 5 10
RAI
AI
RTAM
AI
TAM RTAM
AITAM
UpfrontATACBIG 1-98ABCSG 12TEAM
SequentialBIG 1-98IESITANSAS BC-03ARNO 95ABCSG 8
AI CompMA27FACE
Questions addressed in Randomized Clinical Trials (Can we do better than TAM X 5 years)?
A Breast Cancer female Life Time Story
# 1st Question
# 2nd Question
# 3rd Question

Which AI should be used upfront?With All the Respect to both Trade Name Companies & Lovers

NCIC CTG MA.27 Phase III Trial
Post-menopausal women HR +VE
Underwent adequate Surgery.
Adjuvant chemotherapy and radiation are allowable.
– Chemotherapy must be completed before randomization.
(N = 7,576 women median age, 64.1 years)
Follow-up
Follow-up
Exemestane 25 mgX 5 years
Anastrazole 1 mgX 5 years
1. Lymph node status at diagnosis (negative, positive or unknown)2. Prior adjuvant chemotherapy (yes, no)
3. Current low dose prophylactic aspirin use, < 81 mg/day (yes, no)
R ± celecoxib 200 mgX 3 years
Goss PE et al. JCO 2013
• 1ry Endpoint: event free survival (EFS)• 2ry Endpoints: overall survival, time to distant recurrence, incidence
of contralateral breast cancer, long-term clinical and laboratory safety
• Exemestane & Anastrazole have equivalent efficacy.
• Different Side effect profile.

FACE Phase IIIb Trial
Postmenopausal women with HR + ve & node-positive eBC (stage IIA to IIIC invasive cancer) who were within 12 weeks after breast surgery or completion of adjuvant chemotherapy.
Patients who received neoadjuvant chemotherapy or adjuvant treatment with trastuzumab were also eligible
(N = 4,136 women)
Letrazole 2.5 mgX 5 years
Anastrazole 1 mgX 5 years
1. Number of lymph nodes (one to three or four or more2. Human epidermal growth factor receptor 2 (HER2)
R
Smith I et al. JCO 2017
• 1ry Endpoint: disease free survival (DFS)• 2ry Endpoints: overall survival, time to development of distant
metastases, distant disease-free survival and safety
• Letrozole did not provide statistically superior efficacy over anastrozole for both the 1ry & 2ry
endpoints • Different Side effect profile.
Which AI should be used? What we have learned?
• The benefits of AI therapy appears to be a “class effect”
• The different AIs appear to have equivalent efficacy (MA-27 & FACE)
• How to choose: Safety profile & Patients preference??

0 2 3 5 10
RAI
AI
RTAM
AI
TAM RTAM
AITAM
UpfrontATACBIG 1-98ABCSG 12TEAM
SequentialBIG 1-98IESITANSAS BC-03ARNO 95ABCSG 8
AI CompMA27FACE
Questions addressed in Randomized Clinical Trials (Can we do better than TAM X 5 years)?
A Breast Cancer female Life Time Story
# 1st Question
# 2nd Question
# 3rd Question
# 4th Question Do we have a benefit from Extended Hormonal Therapy?

Are we happy with the 5 years of adjuvant endocrine therapy?If not:
• why???
• How shall we proceed?
• For how long?
Optimal duration of therapy in Postmenopausal Patients

Predictors of recurrence during years 5-14 in 46,138 women with ER+ breast cancer allocated 5 years only of endocrine therapy (ET)
Pan et al. ASCO 2016
Other Predictors?
• High Ki 67• Higher Tumor Grade• Non Luminal A subtypes• Age???• Risk Recurrence Scoring
(need to be further validated)

Are we happy with the 5 years of adjuvant endocrine therapy?If not:
• why???
• How shall we proceed?
• For how long?
Optimal duration of therapy in Postmenopausal Patients

Proposed Strategies
0 2 3 5 10
Tamoxifen AI
Aromatase Inhibitor (AI)
Tamoxifen
Aromatase Inhibitor (AI)
Tamoxifen
Aromatase Inhibitor (AI)
Aromatase Inhibitor (AI)
ATLASaTTom
MA 17
MA 17RIDEALDATA
NSAPB B-42

ATLAS Trial Adjuvant Tamoxifen Longer Against Shorter
Davies C et al. Lancet 2013
Ran
do
miz
e
Discontinue tamoxifen
(5 years total therapy)
Continue tamoxifen for
10 years total therapy
6846 patient
After Completion of 5 Years of
Adjuvant Tamoxifen

ATLAS Results: Recurrence and breast cancer mortality
3.7% reduction in recurrence2.8% reduction in breast cancer mortality

MA-17**
**883 (out ~ 5000 enrolled) were premenopausal at diagnosis and became postmenopausal (oophorectomy or secondary to chemotherapy) after 5 years of tamoxifen
• Significantly improved DFS with Letrazole vs Placebo
• But wasn’t reflected on OS
• QoL???
Goss PE et al. N Eng J Med 2003
Postmenopausal women with
primary breast cancer who had
completed approximately 5
years (4.5 to 6) of adjuvant tamoxifen
therapy
Letrazole 2.5 mg
For 5 years
Placebo
For 5 Years

Extended duration with AI (>5 years)
AI > 5 Years?
MA 17R
DATA
NSAPB B-42
IDEAL

MA.17R: Study Design
• Primary endpoint: DFS (from randomization)
• Secondary endpoints: OS, CBC, safety, QoL
Postmenopausal pts with ER+ and/or PgR+ breast cancer who completed
4.5-6 yrs of letrozole2.5 mg PO QD ± prior
tamoxifen (N = 1918)
Goss PE, et al. ASCO 2016. Abstract LBA1.
Stratification by lymph node status at diagnosis, prior adjuvant chemotherapy,
interval between last AI dose and randomization, duration of prior tamoxifen
Ran
do
miz
e
Letrazole 2.5 mg PO QD
for 5 years
(n = 959)
Placebo
for 5 years
(n = 959)
Follow-up
Follow-up
Median follow-up: 6.3 yrs

MA.17R: DFS and OS After Median Follow-up of 6.3 Yrs
• MA.17R first study to demonstrate benefit of extending AI treatment beyond 5 years• Letrazole treatment for 10 years decreased risk of disease recurrence by 34%
• Majority of benefit in reduction of contralateral breast cancer
• OS not improved by extending Letrazole beyond 5 years
DFS Outcomes Letrozole Placebo HR (95% CI) P Value
Overall 5-yr DFS, % 95 910.66
(0.48-0.91).01
Events, n (%) 67 (7.0) 98 (10.2)
New contralateral breast cancers, n (%)
13 (1.4) 31 (3.2) .007
Locoregional recurrences, n 19 30
Distant recurrences, n 42 53
Bone recurrences, n 28 37
Goss PE, et al. ASCO 2016. Abstract LBA1.

NSAPB B-42: Study Design
0 2 3 5 10
Tamoxifen AI
Aromatase Inhibitor (AI)
R
Letrazole 2.5 mg
Placebo
Mamounas EP P et al. SABCS 2016
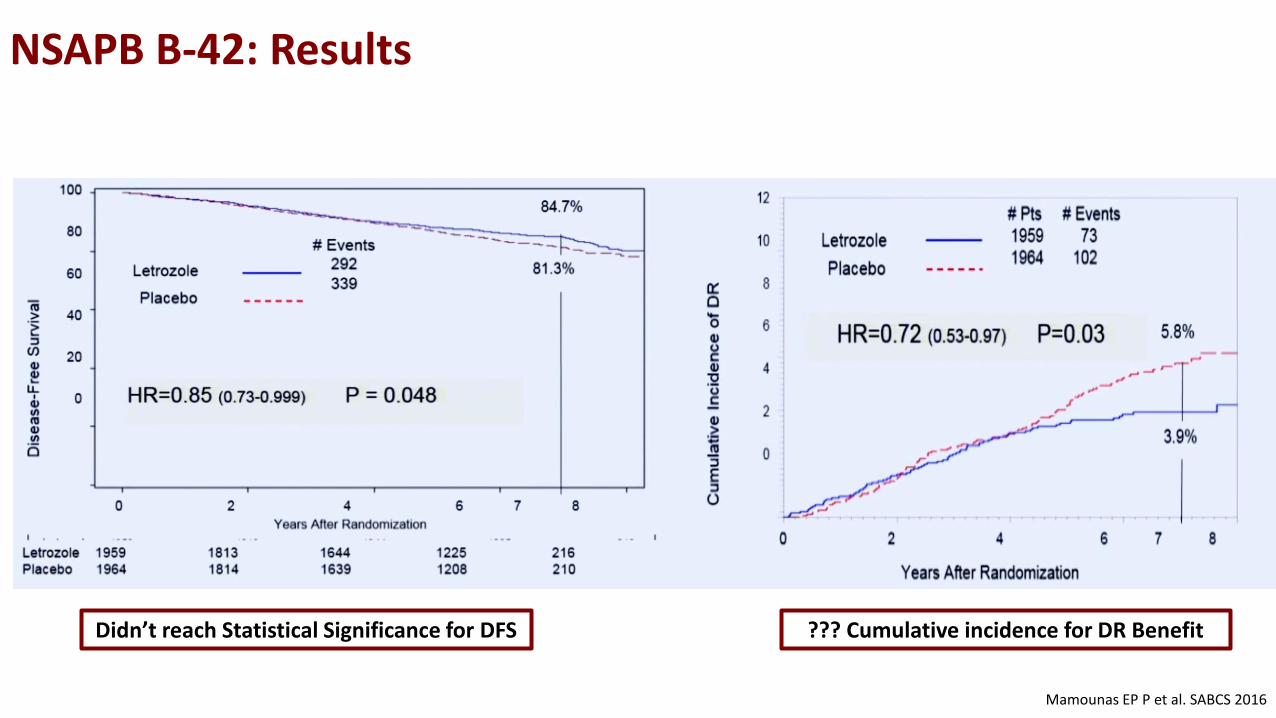
NSAPB B-42: Results
Mamounas EP P et al. SABCS 2016
Didn’t reach Statistical Significance for DFS ??? Cumulative incidence for DR Benefit

IDEAL* & DATA**
0 2 3 5 10
Tamoxifen AI
Aromatase Inhibitor (AI)
Tamoxifen
R
Letrazole 2.5 mg
Letrazole 2.5 mg
*Blok EJ J et al. SABCS 2016**Tjan-Heijnen VC C et al. SABCS 2016
0 2 3 5 10
Tamoxifen
R
Anastrazole 1 mg
Anastrazole 1 mg
IDEAL* DATA**
These findings do not yet support the use of extended adjuvant AI prescription after 5 years of sequential endocrine therapy for postmenopausal patients with hormone receptor-positive breast
cancer
0 2 3 5 10
RAI
AI
RTAM
AI
TAM RTAM
AITAM
UpfrontATACBIG 1-98ABCSG 12TEAM
SequentialBIG 1-98IESITANSAS BC-03ARNO 95ABCSG 8
AI CompMA27FACE
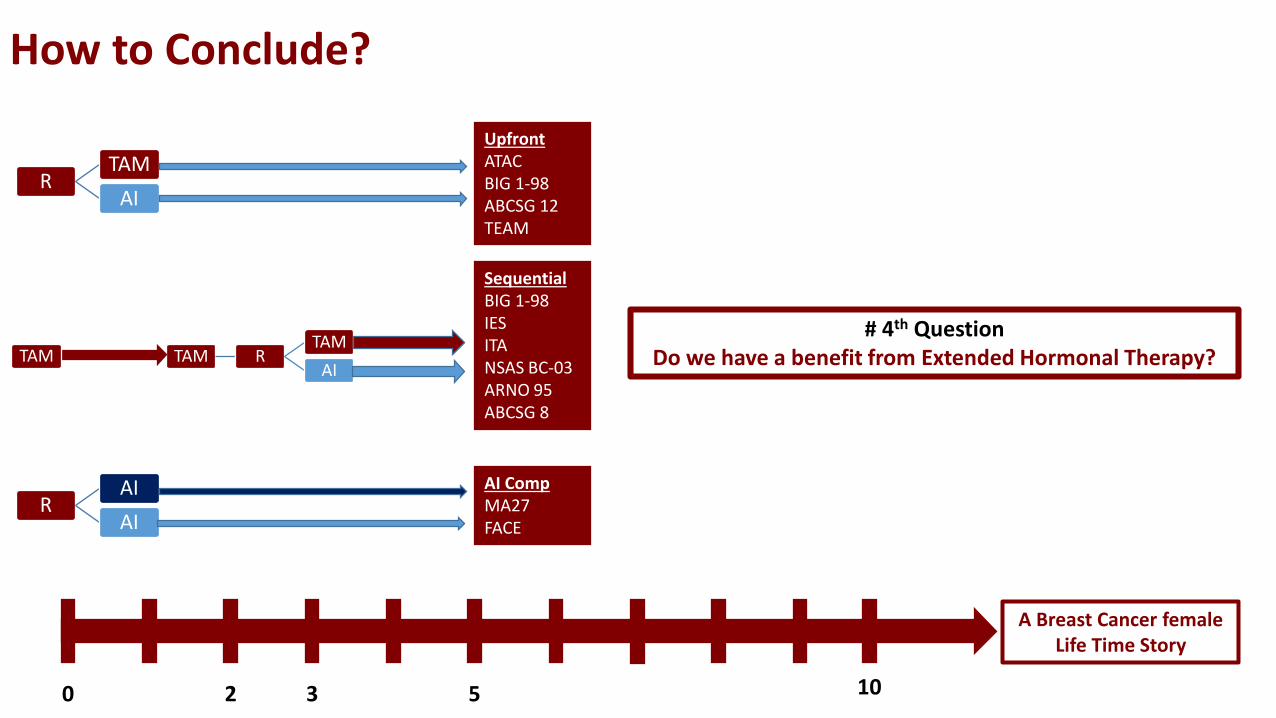
How to Conclude?
A Breast Cancer female Life Time Story
# 4th Question Do we have a benefit from Extended Hormonal Therapy?
Postmenopausal Take Home Message“5 years of Endocrine Therapy”
• 5 years of adjuvant AI better than 5 years of TAM (ATAC, BIG 1-98 monotherapy arm)
• Switching to AI after 2-3 years of TAM is better than 5 years of Tam (ARNO, IES, ABCSG 8)
• Switching to AI after 2-3 years of TAM is equivalent to 5 years of AI (TEAM, BIG 1-98)
• Switching to an AI after 5 years of TAM is better than placebo (MA 17)
• Endocrine therapy should include AI but sequencing with tamoxifen is acceptable

Postmenopausal Take Home Message“Extended Endocrine Therapy Beyond 5 years”
• Late Recurrences are real accounting for > 50% of events• Baseline Stage, grade, and other prognostic markers……….
• Treatment Pros/Cons• Benefits include: lower distant recurrences & secondary prophylaxis• Side Effects include: ongoing familiar side effects & bone health risks
• When to consider Extended adjuvant endocrine therapy?• Women with Stage 3 • Women with stage 2 at higher risks especial node positive• Women with stage 1 (still need to be more personally individualized)
• Women who had tolerated and willing to continue!• Women had started with Tamoxifen!!• Duration not to exceed 10 years (lesser attempts: data are not mature to give a definitive answer)