dry bed: a rapid method of eliminating bedwetting (enuresis) of the retarded
TRANSCRIPT

Behav. Res. & Therapy, 1973, Vol. 11, pp. 427 to 434. Pergamon Press. Printed in Eng!and
DRY BED: A RAPID METHOD OF ELIMINATING BEDWETTING (ENURESIS) OF THE RETARDED*
N. H. AZRIN, T. J. SNEED and R. M. Foxx
Anna State Hospital, Anna, Illinois, U.S.A. and Rehabilitation Institute, Southern Illinois University, Carbondale, Illinois, U.S.A.
(Received 7 December 1972)
Summary-Bedwetting has been a major and unsolved problem for the severely retarded. To solve this problem, an intensive training program was designed similar to a recently developed program for daytime toilet training of the retarded. Some distinctive features of the new procedure were frequent positive rein- forcement for correct toileting, a negative reinforcer for accidents, positive practice in night time toilet& increased level of urination by forcing drinking, immediate detection of correct and incorrect toileting, and Positive Practice for accidents. Of twelve retarded adult bedwetters, the average bedwetter required only one night of intensive training. Several days of apparatus monitoring were used following the training but proved unnecessary for two-thirds of the trainees. Accidents were reduced by about 85% during the first week after training, and almost entirely (95 Y<) during the fifth week with no relapse during a 3 month follow-up. No reduction of accidents resulted when the same bedwetters were given a control procedure that provided no positive or negative reactions other than the sounding of an alarm upon bedwetting. The Dry-Bed procedure appears to be a very rapid solution to the problem of enuresis among the retarded and may be applicable to other difficult populations and also to normals.
ENUFEZ~ is a common problem for which the Mowrer and Mowrer (1938) urine-sensing alarm has provided an acceptable solution. The procedure has been shown to be effective for about 9076 of enuretics and to allow few relapses (see review by Lovibond, 1964). The generally accepted conceptualization regarding this procedure has been that some type of Pavlovian associational learning occurs with respect to bladder pressure, the bladder muscles and bladder sphincter, and the alarm which sounds immediately upon bedwetting (Mowrer and Mowrer, 1938; Lovibond, 1964; Jones, 1960). Recently, an operant conceptualization of the bed-alarm procedure has been offered (Lovibond, 1964; Turner, Young and Rachman, 1970). Surprisingly, no reports have been published demonstrating the effectiveness of this procedure with the severely retarded in spite of their generally high incidence of enuresis. About 70 per cent or more of the institutionalized severely retarded are enuretic (Sugaya, 1967), a frequency that has been confirmed by our own survey. The absence of reports of effective extension of the urine-alarm procedure to the retarded seems to be more than simple omission as was indicated by the failure of the technique in our early (unpublished) efforts to cure retarded enuretics. Recently, procedures have been devel- oped for eliminating the daytime incontinence of the severely retarded (Azrin and Foxx, 1971; Foxx and Azrin, 1973a). These procedures have viewed toileting as an operant process in which social and motivational factors play as great a role as does sensitivity to bladder and bowel stimuli. This same general rationale was used here to develop a method of treating
* This investigation is based in part on a thesis submitted by T. J. Sneed to Southern Illinois University in partial fulfilment of the requirements for the M.S. degree. The research was supported by the State of Illinois Department of Mental Health and Grant No. 17981 from the National Institute of Mental Health. Grateful acknowledgement is given to G. Bible, R. Clutts, J. Kelly, and R. Travis for their assistance. Reprints may be obtained from N. H. Azrin, Behavior Research Laboratory, Anna State Hospital, 1000 North Main Street, Anna, Iliinois 62906, U.S.A.
427

428 N. r-r. AZRIN, -r. J. SNEED and R. M. Foxx
enuresis based also on this social-motivational model. The present study evaluated the effectiveness of this new procedure and compared it with a simple associational procedure that had no operant or social consequences for bedwetting.
Enuresis was viewed here as a socially unacceptable response that persists because the social reinforcement and social inhibitory influences are not acting at an optimal level. The greater prevalence of enuresis (night time incontinence) than daytime incontinence is considered to be caused by the greater delay in social reactions to an accident at night, the greater difficulty in toileting correctly at night because of interference with sleep, and the reduced state of alertness. Enuresis among the retarded is viewed as requiring especially intensive social learning since the retarded person’s learning capacity is more limited.
Some of the distinctive features of the new training program were positive reinforcement for having a dry bed, positive reinforcement for night time urination in the toilet, practice in arising to urinate in the toilet, an artificially increased need to urinate, immediate detection of correct toiletings as well as bedwetting, and negative reinforcers for accidents. The objec- tive was to devise a very intensive learning experience that would eliminate enuresis among the severely retarded within one day of training.
Subjects METHOD
Twelve residents of a state hospital ward for the profoundly retarded were selected as subjects after a survey of bedwetting of all ward residents. The criterion for selection was that the resident had wet his bed at least four out of 12 nights, was accident-free during the day, that he was ambulatory, had vision, and had no medical pathology related to bladder control. The mean recorded IQ for the 12 residents was 12. The Vineland Social Maturity Test yielded a mean Social Age of 2.3 years and a mean Social Quotient of 6.3. Most of the residents had major medical and physical problems such as paralysis of one arm for two of the residents. Speech was absent for five of them, and minimal for the others. None of the residents normally engaged in positive social interaction with each other and only infrequently in even negative aggressive interaction, Seven were male and five were female. The mean age was 37 of which a mean of 28 years had been spent institutionalized. One additional subject was 72 years old and walked only with great effort. His participation will be considered separately.
Urine-alarm apparatus
The apparatus used for detecting bed-wetting was a commercially available device (Lite Alert, Sears Co., Chicago, Illinois). The detection component of the apparatus consisted of two aluminium foil pads, one of which was perforated to allow urine to be absorbed by a cloth separating the pads. The urine-soaked cloth caused a small electrical current to flow between the metal pads thereby causing a buzzer to sound in the nearby circuit box which constituted the second component of the apparatus and was connected to the pads by a wire.
Detection of urination in the ward toilet bowl was assisted by a second type of apparatus. This ‘Potty-Alert’ apparatus had as its detection component a bowl that was inserted in the ward toilet bowl. The apparatus has been described in previous reports (Azrin and Foxx, 1971) and is also commercially available (Potty Alert, Lehigh Valley Electronics, Box 125, Fogelsville, Pennsylvania 18051 U.S.A.).

DRY BED: A RAPID METHOD OF ELIMINATING B~DWE~ING 429
Experimental design
The 12 subjects were divided randomly into two groups. The sequence of conditions for the two groups was
Group 1: Baseline + Urine-Alarm -+ Dry-Bed Training
Group 2: Baseline + Dry-Bed Training + Dry-Bed Training.
The Baseline condition lasted for three weeks as did also the Urine-Alarm procedure. The Dry-Bed procedure remained in effect once it was introduced. To allow the night staff sufficient time to attend properly to the procedure, the residents were introduced into the control and training procedure in pairs; one from Group I and one from Group 2. The Group 1 resident entered the control procedure at the same time that the Group 2 resident entered the training procedure. The next pair was introduced after the first pair no longer required excessive staff attention, usually after a day or two.
Baseline
The 3-week baseline condition consisted of the usual ward routine. The residents were encouraged to toilet themselves at bed time. The ward staff did not inspect the beds at night. The principal change in the usual ward routine was to have a check made of each resident’s bed immediately prior to the required time of arising.
arable-alarm procedure (contru!)
During the 3-week Urine-Alarm condition, the urine-sensing device was placed on the resident’s bed each night. When the resident wet his bed, a loud alarm sounded and was allowed tocontinue for 5 min before the staff member disconnected it. The staff member did not awaken the resident, nor reprimand him. The buzzer sound usually awakened the bed- wetter at least briefly. This procedure was designed to associate the buzzer with urination but with no programmed social consequences of the act. The procedure was not intended to duplicate the “usual” use of the urine-alarm since such usual use involves some degree of social consequences such as requiring the bedwetter to awaken and to toilet himself.
~r~-~ed procedure
Table 1 shows the procedural outline and sequence of the steps that were followed in the dry-bed procedure.
Intensive training. About one-half hour before bedtime the resident was given two cups of a preferred drink (usually a flavored punch), the urine-alarm was put in place on his bed, and the potty-signal apparatus was placed in a toilet bowl in the ward toilet area shortly after he retired. Every hour, the staff member awakened the resident by using the minimal prompt needed for the awakening. Sometimes the resident could only be awakened by manually guiding him to a raised position; this guidance was gradually faded out to a mere touch. The staff member then directed the resident to the toilet usually using only instructions but occasionally gentle manual guidance. The resident was allowed to sit on the toilet for 5 min. If urination did not occur within that period, the resident was returned to his bed where he was given two more cups of fluid and verbal praise for having arisen and walked to the toilet. If the resident did urinate within the 5 min period, the trainer allowed the urination to be completed and then immediately praised the resident and gave him the two cups of fluid as well as a large candied snack as a reinforcer and then returned him to his

430 br. H. AZRIN, T. J. SNEED and R. M. Foxx
TABLE 1. DRY-BED PROCEDURE
X. Intensive Training A. Before bedtime
1. Bedwetter drinks fluids 2. Urine alarm placed on the bed 3. Potty-alert placed in toilet bowl
B. Hourly awakenings 1. Minimal prompt given for awakening the resident 2. Resident instructed or guided to the toilet 3. Resident seated on toilet bowl
a. If urination does not occur within 5 minutes (i) return resident to bed
(ii) at bedside give resident fluids and praise as reinforcers b. If urination does occur within 5 min.
(i) give resident praise, snacks and fluids as reinforcers (ii) return resident to bed
4. Praise resident for having dry bed (require resident to touch the dry sheets) 5. Resident returns to sleep
C. When accident occurs45 Min of Cleanliness Training and Positive Practice 1. Disconnect the sound of the urine-alarm 2. Awaken resident 3. Reprimand resident for wetting and direct him to the toilet to finish urination 4. Cleanliness Training
a. Bedwetter changes wet linen b. Attendant reactivates urine-alarm
5. Positive Practice in toiieting a. Bedwetter lies down in bed for 3 minutes b. Bedwetter awakened with minimal prompt after 3 minutes c. Bedwetter directed to toilet d. Repeat steps a, b, c about 9 times
6. Bedwetter returns to sleep when 45 minutes have elapsed since accident was detected
II. Monitored post-training phase A. Initiation of monitored post-training
1. When resident has no more than 1 accident during a training night 2. When the resident correctly toilets on at least 50% of all opportunities during a training night.
B. Procedure 1. Urine-alarm on bed 2. Whenever accident occurs, reprimand, Cleanliness Training and Positive Practice follow for 45
minutes 3. No fluids, no hourly awakenings, no reinforcers
C. Termination of monitored post-training 1. Terminated 7 nights after last accident
III. Norma/procedure A. Initiated after resident goes I nights without accident B. No urine-alarm, no reinforcers, no Positive Practice, etc. C. Bed inspected each morning
1. If bed wet, resident remakes and cleans bed (Cleanliness Training) 2. If 2 accidents occur within a given week, the Monitored phase is reinstated

DRY BED: A RAPID METHOD OF ELIMINATING BEDWETTING 431
bed. Whether or not the resident had urinated in the toilet, once at bedside, the resident was directed to touch the dry sheets on his bed and was verbally praised for having dry sheets. The resident then returned to sleep until the next hourly toileting was scheduled. Training was terminated (1) when no more than one accident occurred during the entire evening and (2) when the resident correctly toileted in the toilet bowl on at least half of the opportunities presented by the scheduled hourly toiletings. Unscheduled urinations in the toilet were also included in this calculation.
Accidents during training
When the bed became wet between the hourly toiletings, the wetting was signalled by the sounding of the urine-alarm. The attendant immediately disconnected the sounding of the alarm so as not to disturb the other residents. The bed wetter was then awakened and occupied for a period of 45 min. First, the attendant verbally reprimanded the bed wetter for having wet and then sent him to the toilet. While the resident was occupied in the toilet, the attendant removed the urine-alarm apparatus and replaced the wet cloth material, thereby preparing the apparatus for its next usage. When the bed wetter returned to the dormitory, he was given Cleanliness Training which required him to remove the wet linen, wipe off the mattress, bring the wet linens to the nearby laundry room, obtain fresh linen from another room, and remake the bed. After the bed linen was changed, the resident was given Positive Practice in arising from a drowsy state in order to toilet. He was directed to lie down in the bed for 3 min after which he was awakened using the minimal prompt necessary. He was then directed to the toilet where he sat on the toilet bowl for no more than 30 set after which he was directed back to his bed. No reinforcement was given even if urination did occur within the 30 set period. After returning to his bed for 3 min, he was again awakened and directed to the toilet. These toilet-approach trials were repeated until a total of 45 min had elapsed since the initial detection of the accident thereby allowing about S-10 trials for most residents.
Monitored post-training
After the intensive training, the urine-alarm was placed on the bed as usual prior to bed time. If the resident had an accident, he was given the same procedure described above, namely, awakened, given the reprimand, required to clean and change his bed and given Positive Practice for toileting. The fluids, the tasty edible reinforcers, the praise, approval, and hourly awakenings that were used in the intensive training phase all were discontinued in this phase. The monitored phase terminated seven days after the last accident had occurred, which meant that if no accidents occurred after the intensive training phase, the monitored phase lasted for exactly seven days.
Normal ward procedure
After the monitored phase, no urine-alarm was used, nor were verbal, edible, or fluid reinforcers or Positive Practice as had been used in the monitored phase. The only pro- cedure that the staff followed in this phase was to inspect each bed in the morning and, if the bed was wet, to require the resident to remake the bed himself. If bed wetting was detected on two days within a given week, the normal ward procedure was terminated and the monitored phase reinstated.
Details, and the rationale, of the specific procedures such as fading the prompts, the

432 N. H. AZRIN, T. J. SNEED and R. ht. Foxx
types of fluids used, the Graduated manual guidance procedure, the Cleanliness Training procedure, Positive Practice, etc., have been described in the previous reports of the daytime toilet training (Azrin and Foxx, 1971; Foxx and Azrin, 1973a). Additiona details and discussion of the Positive Practice and Graduated Guidance procedures are provided in Foxx and Azrin, 1972; 1973b; 1973c; Azrin, Kaplan and FOXX, 1973.
Bed-rest alarm apparatus
An unexpected discovery during the toilet training procedure was that some of the residents were arising from their bed at night and urinating on the floor. These inappropriate urinations could not, of course, be detected by the urine-alarm apparatus, nor could the staff usually discover which resident had urinated. The problem was solved by using a ‘Bed-Rest Alarm’ apparatus which had been used and described in a previous report (Webster and Azrin, in press). The apparatus consists of a metal cylinder that attaches to a leg of the resident’s bed and contains a switch which is closed when the weight of a person Iying on the bed is added to the normal weight of the bed. The switch opens when the person leaves the bed. This switch action was used to sound a signal to the staff indicating that a resident had arisen from his bed. The apparatus was used only for four residents who were known or suspected to have arisen from their bed and urinated on the floor. When the ward staff heard the signal from the Bed-Rest Alarm apparatus, they required the resident to return to his bed unless he was proceeding to the toilet.
DRY-BED TRAINING
BASELINE URINE- ALARM
7 / , I 2 3
t 4
t POST-TRAINING
N:12 RETARDATES
r,
/ I 2 3 4 5 6 7 8 12
WEEKS
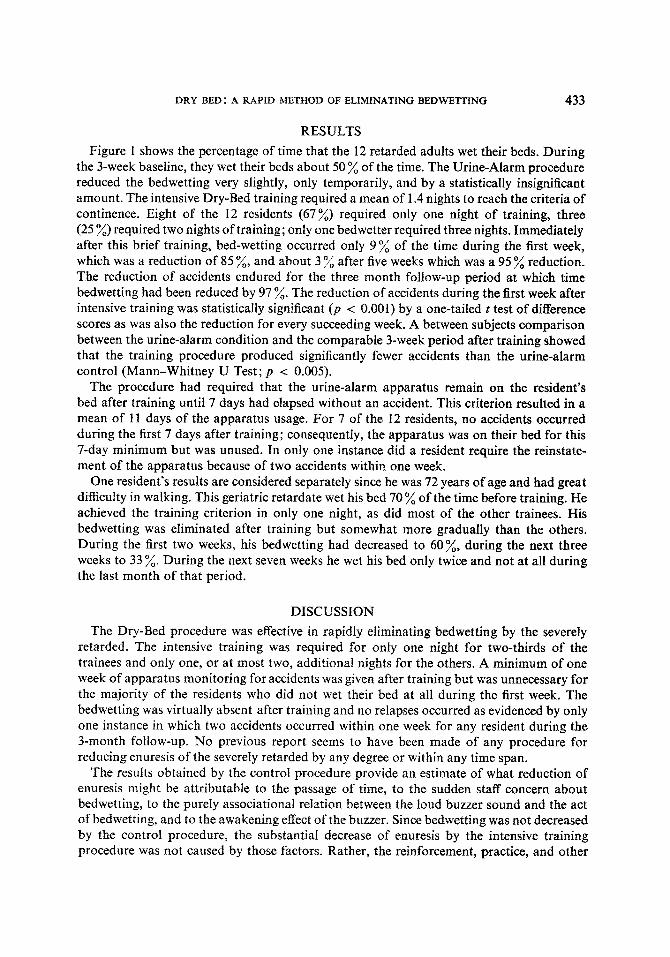
FIG. 1. The effect of the Dry Bed procedure on the nighttime bedwetting of profoundly retarded adults. During the baseline period, no contingencies were in effect for bed wetting. In the Urine-Alarm condition, urine-sensing apparatuses sounded an alarm upon bedwetting. The dry-bed training arranged an intensive reinforcement experience and required an average of 1.4 nights. Each data point designates the mean percentage of nights in which bedwetting occurred per resident. Also, each data point is the average for a one-week period for the 12 trainees, except for the final data point which is the average for a four-week period, and
except for the Urine-Alarm condition which is for 6 trainees.
DRY BED: A RAPID METHOD OF ELIMINATING BEDWETTING 433
RESULTS
Figure 1 shows the percentage of time that the 12 retarded adults wet their beds. During the 3-week baseline, they wet their beds about 50 % of the time. The Urine-Alarm procedure reduced the bedwetting very slightly, only temporarily, and by a statistically insignificant amount. The intensive Dry-Bed training required a mean of 1.4 nights to reach the criteria of continence. Eight of the 12 residents (67%) required only one night of training, three (25 %) required two nights of training; only one bedwetter required three nights. Immediately after this brief training, bed-wetting occurred only 9% of the time during the first week, which was a reduction of 85 ‘A, and about 3 ‘A after five weeks which was a 95 % reduction. The reduction of accidents endured for the three month follow-up period at which time bedwetting had been reduced by 97 %. The reduction of accidents during the first week after intensive training was statistically significant (p < 0.001) by a one-tailed t test of difference scores as was also the reduction for every succeeding week. A between subjects comparison between the urine-alarm condition and the comparable 3-week period after training showed that the training procedure produced significantly fewer accidents than the urine-alarm control (Mann-Whitney U Test; p < 0.005).
The procedure had required that the urine-alarm apparatus remain on the resident’s bed after training until 7 days had elapsed without an accident. This criterion resulted in a mean of 11 days of the apparatus usage. For 7 of the 12 residents, no accidents occurred during the first 7 days after training; consequently, the apparatus was on their bed for this 7-day minimum but was unused. In only one instance did a resident require the reinstate- ment of the apparatus because of two accidents within one week.
One resident’s results are considered separately since he was 72 years of age and had great difficulty in walking. This geriatric retardate wet his bed 70 % of the time before training. He achieved the training criterion in only one night, as did most of the other trainees. His bedwetting was eliminated after training but somewhat more gradually than the others. During the first two weeks, his bedwetting had decreased to 60%, during the next three weeks to 33 ‘A. During the next seven weeks he wet his bed only twice and not at all during the last month of that period.
DISCUSSION
The Dry-Bed procedure was effective in rapidly eIiminat~ng ~dwetting by the severely retarded. The intensive training was required for only one night for two-thirds of the trainees and only one, or at most two, additional nights for the others. A minimum of one week of apparatus monitoring for accidents was given after training but was unnecessary for the majority of the residents who did not wet their bed at all during the first week. The bedwetting was virtually absent after training and no relapses occurred as evidenced by only one instance in which two accidents occurred within one week for any resident during the 3-month follow-up. No previous report seems to have been made of any procedure for reducing enuresis of the severely retarded by any degree or within any time span.
The results obtained by the control procedure provide an estimate of what reduction of enuresis might be attributable to the passage of time, to the sudden staff concern about bedwetting, to the purely associational relation between the loud buzzer sound and the act of bedwetting, and to the awakening effect of the buzzer. Since bedwetting was not decreased by the control procedure, the substantial decrease of enuresis by the intensive training procedure was not caused by those factors. Rather, the reinforcement, practice, and other

434 N. H. AZRIN, T. J. SNEED and R. M. FOXX
features of the intensive training program seem to have been responsible. How much of a role each of the component procedures played is unknown. The poor results obtained by the simple use of the urine-alarm apparatus supports the conception of night time continence as an operant reinforcement process, rather than as an associational process (Lovibond, 1964; Turner et al. 1970).
The speed and completeness of the present method suggests its possible use with popu- lations other than the one used here. The present sample of retarded individuals had as low a level of functioning as one is likely to encounter. The higher level retardate might be expected to be trained even more quickly. The nonretarded enuretic would seem to be even more influenced by this procedure since verbal instructions and explanations could be used and learning ability is intact. Conversely, the procedure may offer hope for enuresis produced by other types of disability, such as geriatric incontinence. This conjecture is supported by the elimination of enuresis by the 72 year old trainee in the present study who suffered the three-way disability of geriatric infirmity, profound retardation and enuresis.
REFERENCES
AZRIN N. H. and Foxx R. M. (1971) Autism reversal: eliminating stereotyped self-stimulation of the retarded. J. appl. Behav. Anal. 4, 89-99.
AZRIN N. H., KAPLAN S. J. and Foxx R. M. (1973) Autism reversal : eliminating stereotyped self-stimulation of the retarded. Am. J. Men. Def. To be published.
Foxx R. M. and AZRIN N. H. (1972) Restitution: A method of eliminating aggressive-disruptive behavior of retarded and brain damaged patients. Behav. Res. & Therapy 10, 15-27.
Foxx R. M. and AZRIN N. H. (1973a) Toilet Training the Retarded: a Rapid Program for Day and Night- rime Independent Toileting. Research Press, Champaign, Illinois.
Foxx R. M. and AZRIN N. H. (1973b) The elimination of autistic, self-stimulatory behavior by overcorrection. J. appl. Behav. Anal. To be published.
Foxx R. M. and AZRIN N. H. (1973~) Dry pants: A rapid method of toilet training children. Behav. Res. & Therapy. To be published.
JONES G. H. (1960) The behavioral treatment of enuresis nocturna. In Behavior Therapy and the Neuroses (Ed. EYSENCK H. J.), pp. 377-403. Pergamon Press, New York.
LOVIBOND S. H. (1964) Conditioning and Enuresis. The Macmillan Company, New York. MOWRER 0. H. and MOWRER W. M. (1938) Enuresis-a method for its study and treatment. Am. J. Ortho.
Psychiat. 8, 436447. SUGAYA K. (1967) Survey of the enureses problem in an institution for the mentally retarded with emphasis
on the clinical psychological aspects. Japanese J. of Child Psychiat. 8 (2), 142-l 50. T~~RNER R. K., YOUNG G. C. and RACHMAN S. (1970) The treatment of nocturnal enuresis by conditioning
techniques. Behav. Res. & Therapy 8, 367-381. WEBSTER D. R. and AZRIN N. H. (1972) Required relaxation: A method of inhibiting agitative-disruptive
behavior of retardates. Behav. Res. & Therapy. 11, 67-78.