dr keith giles laboratory for cancer medicine, western australian institute for medical research,...
TRANSCRIPT

Dr Keith Giles
Laboratory for Cancer Medicine, Western Australian Institute for Medical Research, School of Medicine and Pharmacology,University of Western Australia
Genetics of brain tumours

Overview
1. Glioblastoma - the most common & lethal form of adult primary brain tumour
2. What we know about the molecular biology of glioblastoma
3. Targeted therapy of glioblastoma
4. New advances in understanding glioblastoma genetics
5. Research into microRNAs and glioblastoma

Glioblastoma
• Most common & lethal primary brain tumour in adults
• Highly resistant to therapy (surgery, radiation therapy & chemotherapy)
• Disease recurrence is common following surgery
• Life expectancy of glioblastoma multiforme patients (GBM; Grade IV) is ~14 months
• Urgent need for new treatment options

organism organ cell
Molecular biology
molecules:DNA, RNA, proteins

What cells make up a tumour?

DNA(genes)
RNA Protein
Structure & function of cells
Disease
How genes cause disease

Genetic basis of cancer
Cancers originate as the result of hereditary or accumulated changes (mutations) in genes that control critical processes in cells
DNAsequence
G A C T A A T C G G Normal gene
G A C T A G T C G G Single base change
G A C T A A C C A T C G G Insertion
G A C T C G G Deletion

Genetic basis of cancer
Mutations can activate oncogenes or silence tumour suppressor genes
oncogenes(bad)
tumour suppressor genes (good)

Genetic basis of cancer
There is increased or decreased expression of specific genes in cancer
Normal cell Cancer cell
Gene A
Gene B
Gene A
Gene B

Genetic basis of cancer
These changes (mutations) can be studied in the laboratory using sophisticated genetic analysis methods
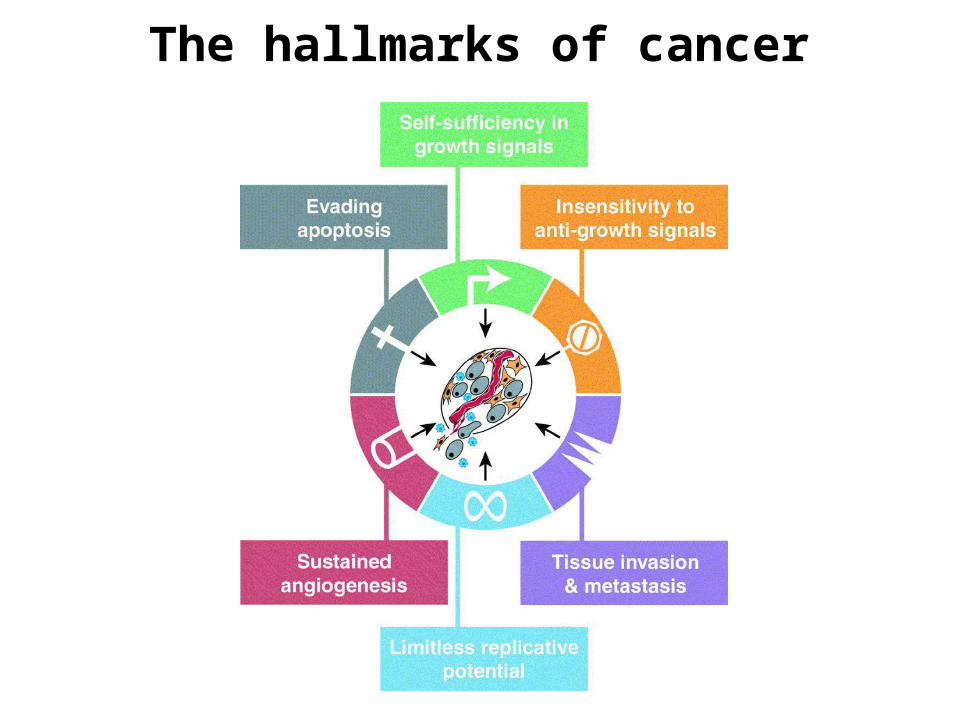
The hallmarks of cancer
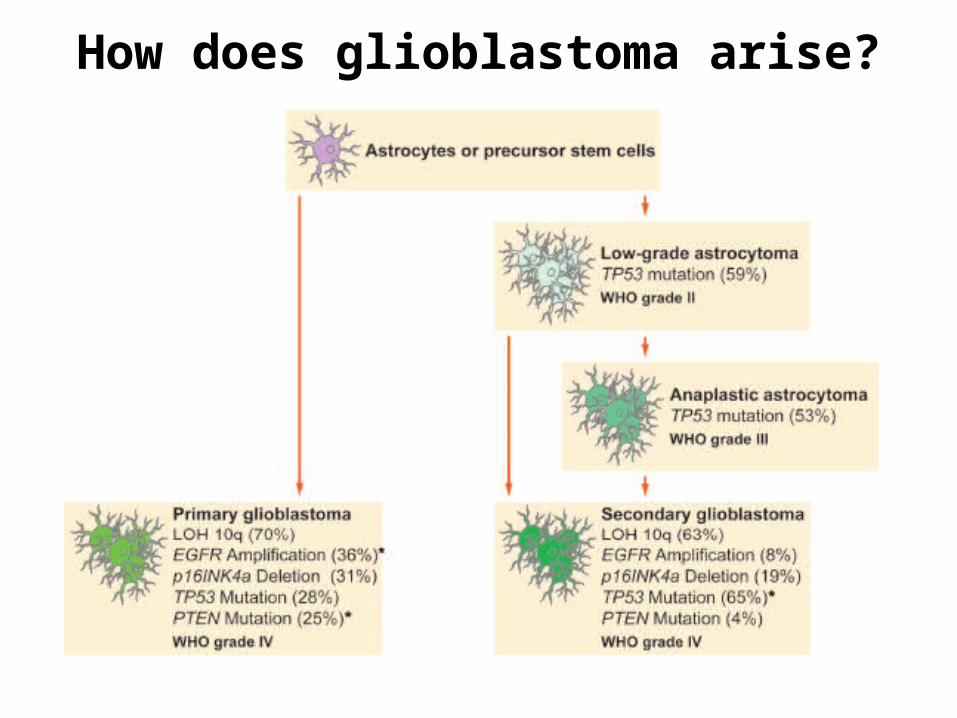
How does glioblastoma arise?

1. Two main pathways by which glioblastomas develop (primary vs secondary)
2. Primary and secondary glioblastomas can arise via different mutations
3. Mutations between primary or secondary glioblastomas can differ
Molecular development of glioblastoma

Increased EGFR expression and signaling in glioblastoma
normalcell
growth
glioblastomacell
growth

How can understanding the genetics of cancer cells (glioblastoma)
help us to develop new treatments for the disease?

Understand what has “gone wrong” in glioblastoma cells
Design a drug to correct what has “gone wrong”

Targeted cancer therapy
Find & understand mutation/alteration that drives cancer cell growth (choosing the ‘right’ target)
Design & develop drug that specifically targets this mutation/alteration
Normal cells lack the mutation & should be relatively unaffected; side effects should be
minimised

Gleevec & chronic myelogenous leukaemia (CML)
(TIME magazine,May 2001)

(Tyrosinekinase
Inhibitor)
Is there a ‘gleevec’ for glioblastoma?

Not yet
There may never be one drug that works on
all glioblastomas

Why?
Heterogeneity(no single mutation causes all
glioblastomas)

Redundancy(a glioblastoma is not dependent on one mutation; other mutations can
compensate)
growth

Resistance(by targeting one mutation, new mutations can arise that allow
glioblastoma cells to escape this targeting)

Case study of a targeted glioblastoma drug
Erlotinib (Tarceva)
(A small molecule tyrosine kinase inhibitor of the epidermal growth factor
receptor [EGFR])

Epidermal growth factor receptor (EGFR) as a therapeutic target in glioblastoma
ERK1/2PI3K/Akt
Tyrosine kinase inhibitor (erlotinib)

The rationale for using erlotinib to treat glioblastoma
• About half of glioblastomas have high expression of EGFR
• Blocking EGFR should block glioblastoma growth & invasion
• Promising results in other cancer with high expression of EGFR (eg. lung)
• Small molecule tyrosine kinase inhibitor (TKI) - crosses blood-brain barrier

Erlotinib and glioblastoma
• Unfortunately, few patients (~10-20%) respond to erlotinib and survival benefit is small
• Need to identify what determines whether a patient will respond/not respond to erlotinib
• Combine erlotinib with other treatments (chemotherapy, other targeted agents, radiation therapy) to improve responses and increase patient survival
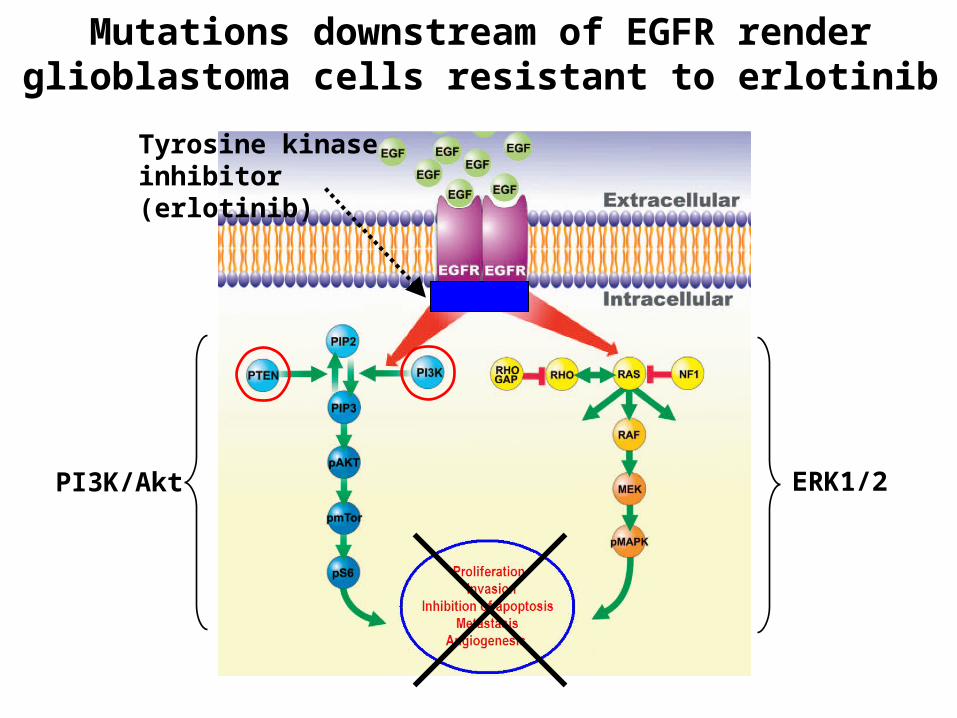
Mutations downstream of EGFR render glioblastoma cells resistant to erlotinib
ERK1/2PI3K/Akt
Tyrosine kinase inhibitor (erlotinib)

New advances in understanding of
glioblastoma

Brain tumour stem cells
• Cancer stem cell hypothesis: tumours are dependent on a small population of cancer stem cells that are distinct from the more abundant tumour cells.
• Cancer stem cells are highly resistant to conventional cancer therapies
• Express specific cell surface markers (eg. CD133).
• Molecular characterisation has identified possible drug targets for brain tumour stem cells.

Targeting brain tumour stem cells

The Cancer Genome Project
• Human Genome Project: database of a complete genome of a normal human
• Cancer Genome Project: established in 2006; to characterise >10,000 tumours at a molecular level from at least 20 tumour types (incl. glioblastoma) by 2015.
• Will identify many more mutations responsible for glioblastomas - new treatment targets?
• Made possible by rapid development of high throughput techniques - researchers can screen millions of DNA bases quickly and cheaply. This has only been feasible in the last few years.

The Cancer Genome Project
• Some achievements to date in understanding glioblastoma:
(1) Discovery that patients with an unmethylated version ofMGMT gene respond better to temozolomide. Patient selection?
(2) Discovery that a subset of glioblastoma patients that live anaverage of three years have different gene mutations to regularglioblastoma patients. What do these do?
(3) Identification of at least four glioblastoma subtypes, based ontheir DNA signatures. Survival, response to aggressivechemotherapy & radiotherapy differed according to subtype.

microRNAs and glioblastoma
microRNAs (miRNAs)
• miRNAs are short, endogenous, non-coding RNAs- >900 miRNAs, many are conserved, cell & tissue-specific expression
• miRNAs negatively-regulate gene expression- bind to specific target mRNAs, predicted to regulate 1/3 of all genes
• miRNAs have important functions in normal cells- development, differentiation, angiogenesis, proliferation, apoptosis
• miRNA expression is altered in disease states- cancer - oncogenes & tumour suppressor genes

microRNAs block expression of specific target genes
DNA
RNA
protein
microRNA

microRNA expression is altered in cancer cells vs normal cells
• Cancer miRNA “signature” - classify tumours
• Biomarkers?
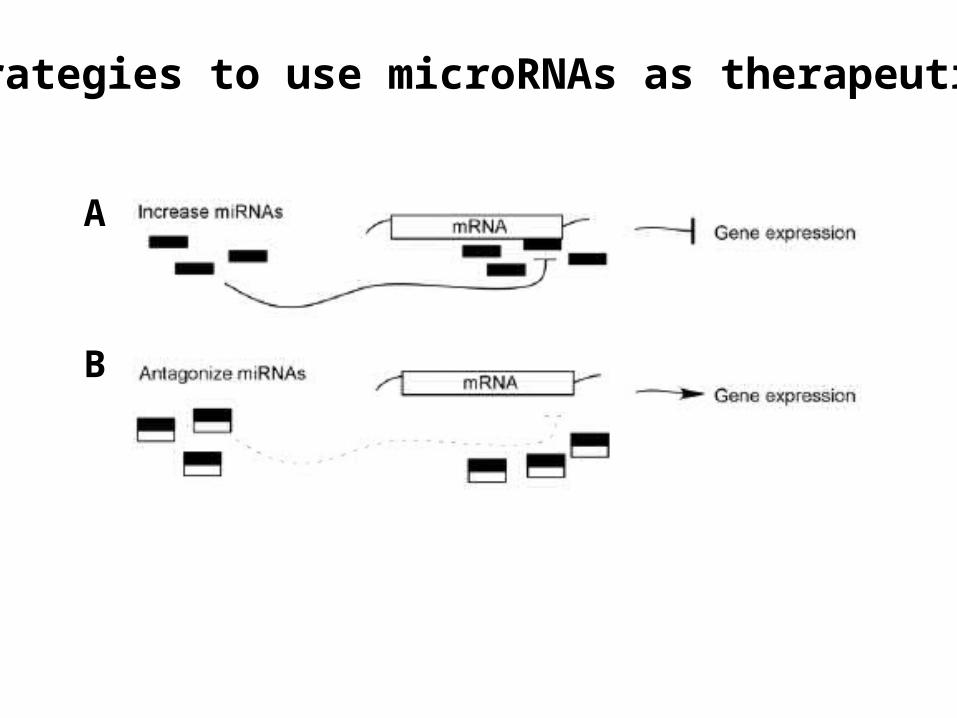
Strategies to use microRNAs as therapeutics
A
B
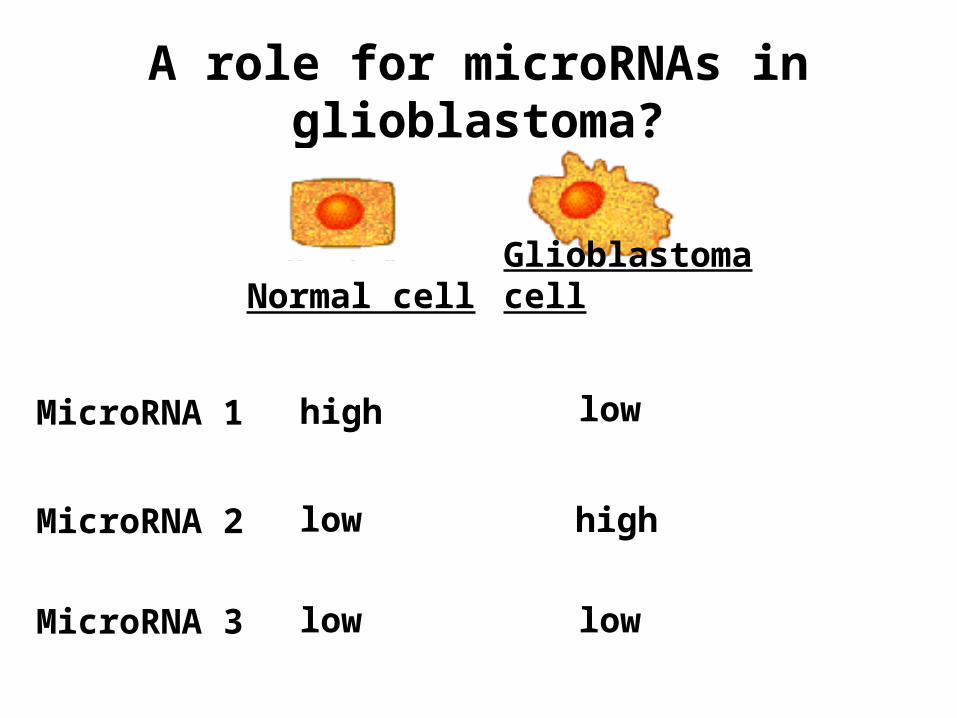
A role for microRNAs in glioblastoma?
Normal cell Glioblastoma cell
MicroRNA 1
MicroRNA 2
MicroRNA 3
high low
low
low low
high

Levels of miR-7 microRNA are significantly reduced in glioblastoma patient tissues vs
normal brain

Culture of glioblastoma cell lines in the laboratory
glioblastoma cell line
glioblastoma tumour
• Study gene mutations/alterations• Study new treatments

Levels of miR-7 microRNA are significantly reduced in glioblastoma tumour cell lines vs
normal brain

Glioblastoma cell lines can be transfected with microRNA
glioblastoma cell line
microRNA (eg. miR-7)
• Determine effects on other genes involved in glioblastoma (eg. EGFR)• Measure effects on glioblastoma cell growth
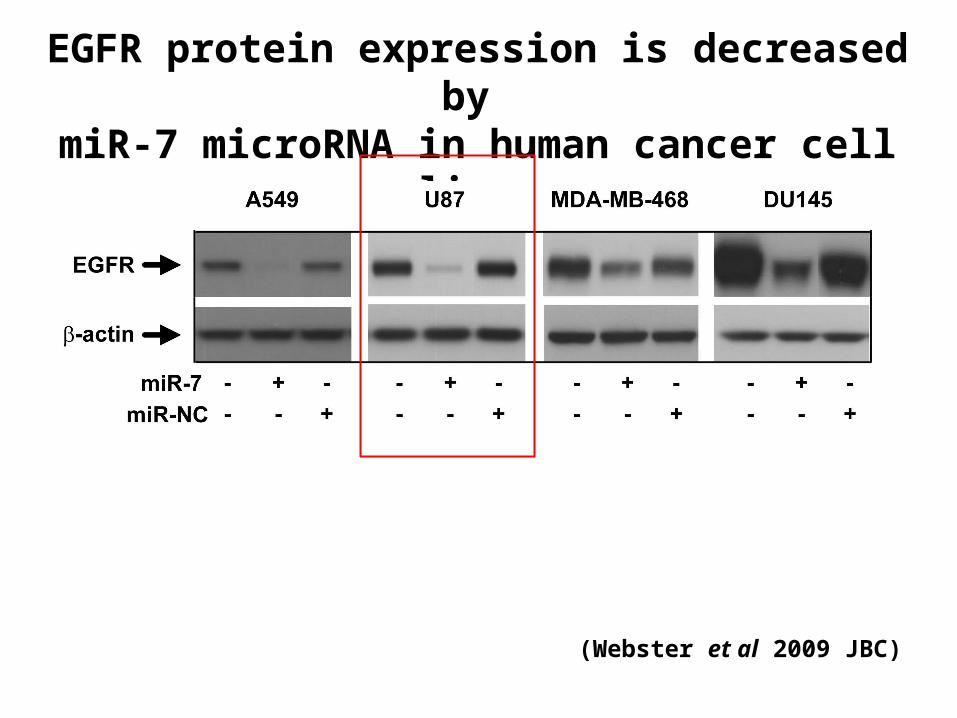
EGFR protein expression is decreased by miR-7 microRNA in human cancer cell lines
(Webster et al 2009 JBC)

miR-7 microRNA reduces glioblastoma cell growth

Summary• Glioblastomas are different & often arise via different
mutations. This might explain why they can respond differently to treatment.
• First generation of targeted agents have yielded disappointing results, but research can explain why this has been the case and improvements made to future drug design.
• Understanding all of the important mutations in glioblastoma (eg. via large scale research efforts such as the Cancer Genome Project) should allow the development of new drugs that are effective in patients with the correct mutation.

More work is needed but progress is being made…
“I’ve been treating glioblastoma for about 22 years. I’vetaken care of more than 20,000 patients. The kinds ofthings we’ve seen in the clinic in the last four yearsblows away anything I saw in the previous 18 years ofmy career.”
Howard Fine, MD - Chief, Neuro-oncology, Centre for CancerResearch, National National Cancer Institute, commenting in Jan 2010 on a report estimating that the percentage ofglioblastoma patients who survive two years from diagnosis hasmore than tripled in the last five years as a result of newtreatment regimens.

AcknowledgementsRebecca Webster, Priscilla Zhang, Karina Price, Michael Epis, Andrew Barker, Felicity Kalinowski
The Leedman Lab
Western Australian Institute for Medical Research
Terry Johns (Monash), Kerrie McDonald (Lowy), Greg Goodall (Hanson), John Mattick (UQ)
Cancer Council WA & Pearl Bethel Allan Research Grant Endowment
National Health and Medical Research Council
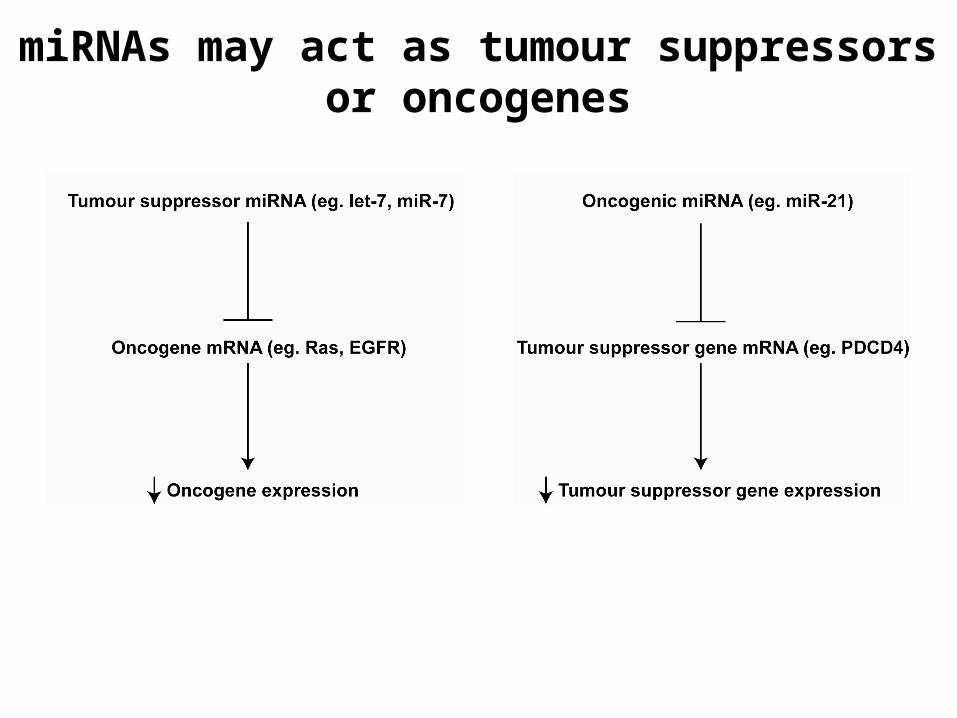
miRNAs may act as tumour suppressors or oncogenes

• miRNAs bind to specific target mRNAs, regulate 1/3 of all genes
• One miRNA can have 100’s of mRNA targets
microRNAs block expression of target genes

Glioblastomas arise from glial cells
• Glioblastomas are a group of low-grade and high-grade brain tumours that originate from glia (Greek for ‘glue’)
• Normally, glial cells (eg. astrocytes) provide support to neurons (nerve cells): nutrients, mechanical support, development, immune function
• Genetic alterations occur in glial cells glioblastoma