dr karen murphy,sir charles gairdner & osborne park health care group - the ‘spice’ of life
DESCRIPTION
Dr Karen Murphy delivered the presentation at the 2014 Emergency Department Management Conference. The 2014 Emergency Department Management Conference explored areas such as how to improve access to care, clinical redesign, NEAT compliance, patient flow, point of care testing, geriatric care, and enhance the performance of Emergency Department. For more information about the event, please visit: http://bit.ly/edmanagement14TRANSCRIPT

SCGH Four Hour Rule Program
The SPICe of Life…
Dr Karen Murphy
A/Executive Director Medical Services
Sir Charles Gairdner & Osborne Park Health Care Group
Perth, Western Australia
July 2014

Sir Charles Gairdner Hospital

QEII Medical Centre - SCGH

Sir Charles Gairdner Osborne Park
Health Care Group

The problem ………In the Beginning

And then… The Four Hour Rule Program

SCGH Four Hour Rule Program
Process solutions – 5 key areas
Pat
ient
S
uppo
rtN
ursi
ngC
leric
alM
edic
al
Admissions
Stream
Discharge Stream
Patient to Emergency Decisions Unit
Patients should be transferred to EDU as
soon as it becomes clinically indicated. If no
plan identified at 3 hours post triage
(patients name on EDIS turns black), ED
Liaison Officer is responsible for informing
Senior Doctor
ED Senior Registrar
or Consultant
authorises a decision
to admit patient to
Emergency
Decisions Unit
ED Nursing Coordinator completes
details clinical & safety details on
booking slip & hands to ED Liaison
Officer
ED Medical Officer
documents plan in notes
(including DECT phone
number)
ED Liaison Officer
inputs information
into EDIS.
(patient is
transferred to SSU
location on EDIS)
OBS Coordinator sends OBS HSA to
collect patient. If unavailable organises
other HSA to transport. Upon collecting
patient HSA informs ACO or Resus
Coordinator
Emergency Decisions Unit
Admission Procedure
ED Clerk collects
booking slip,
admits to
TOPAS.
Completes
registration &
Financial
Election
HSA informs Obs
coordinator of patient
arrival
BOOKING SLIP
ED Medical Officer completes booking slip
and hands to Nursing Coordinator of Area
Or
CLINICAL HANDOVER
ED Medical Officer provides handover and
plan to Obs Coordinator (x6713) ONLY if
clinically indicated
EDU Pull
Obs Coordinator notices on EDIS that
patient is for EDU and pulls patient
across
Medical Team responsible
for patient from Triage
continues Medical
Management
ED Clerk informs
Obs Liaison
Officer of
admission details.
LO ensures
patient in correct
location on EDIS
Bed Realignment
Discharge ED Process - EDU
Ward Leadership Process

Four Hour Rule Program - Challenges
Not just about the Emergency Department
Front door to back door solutions
Engagement – some thought it would „go
away‟
Full implementation of solutions not
realised – poor compliance (& success)
Ownership & accountability

SCGH Four Hour Rule Program
Results - context
ED presentations / Access Block

SCGH Four Hour Rule Program
Performance against 4/24 target
2008 Jan 46% 2009 Jan
39%
2010 Jan 46%
2010 Aug 50%
2011 Jan 68%
2012 Jan 71%
2012 Aug 52%
2013 Jan 62%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
2008 2009 2010 2011 2012 2013
Four Hour
Rule Program
commenced
Solution
implementation
commenced
Perfromance-
56% - Solution
Review &
Actions
Stokes Review Winter demand

SCGH Four Hour Rule Program
NEAT in 2013… what was going wrong?
The FHRP resulted in performance
against 4 hour time frame by ~ 25%
Access block from 60% to 12%
Reached target in Oct 2011
Performance not sustained and declined in
2012
SCGH did not achieve target of 76%

NEAT in 2013…. Adding to the challenge
Change fatigue and effects on staff
engagement
Competing reform – NEAT vs NEST
Efficiency – ABM/ABF
Winter stress, high bed occupancy
Downstream care – inpatient, ambulatory,
community
Mental Health in ED

Re-igniting the flame… mid 2013
MfH – huge interest in NEAT
MfH – UK visit - Prof Derek Bell et al
invited to Perth
Team of auditors – clinical & statistical
analysts visited Perth July 2013
Reviewing Emergency Flow processes at 3
Tertiary sites in WA
Involving pre-visit departmental self-
assessment, professional workshop and
on-site visit / „Day of Care‟ audit.

SCGH Four Hour Rule Program
The Bell audit (1) - Aug 2013
Audit components:
1. Pre visit departmental self assessment
against „Adult Emergency Service
Standards for ACUTE admission‟ (UK)
2. Key Stakeholder Workshop
3. „Day of Care‟ survey & walkabout Audit task carried out on ALL patients in SCGH beds
at 0700 on Monday 5th August
Audit tool provided by UK team to review local
practice against adapted UK standards
Involving majority of wards, AAU, ED, Radiology,
Pathology, Pharmacy & Allied Health

SCGH Four Hour Rule Program
The Bell Report
Preliminary results presented to
DG Health and Area Health
Service CEs 8th Aug 2013
Final Report to sites Sept 2013

SCGH Four Hour Rule Program
Bell Recommendations for SCGH
1. Improve patient flow
2. Reduce complexity of internal ED systems
3. Reduce the complexity of the admission
interface between ED and AAU/SAU
4. Optimise the admission flow between ED and
specialist wards; and between AAU/SAU and
sub-specialty inpatient wards
5. Provide continuity of care
6. Optimise physical and staff capacity – Doing
today’s work today and making Monday’s
better

SCGH Four Hour Rule Program
The Birth of SPICe!
Governance Governance Governance!
Strategic Patient Flow Implementation
Committee (SPICe)
Provide executive oversight of
organisational strategies aimed at
improving patient flow at SCGOPHCG
Broad, multidisciplinary & executive
representation
Meets weekly
ACE and SCG OPHCG ED attend

SCGH Four Hour Rule Program
The SPICe Action Plan
Developed by SPICe – based on the Bell
recommendations
Dynamic document – forms basis of
agenda/minutes weekly
RAG status used to monitor achievement /
progress / barriers / risk
Action driven!

SCGH Four Hour Rule Program
SPICe in action….. examples
1. Improving Patient Flow – front door to
back door and beyond
Consultant-led care - ensure daily consultant-
led care across all specialties
Discharge planning - Focus on the EDD –
whiteboards, patient room boards, health
record & TELL THE PATIENT! Monthly audits –
significant improvement with compliance across
all areas

SCGH Four Hour Rule Program
SPICe in action….. examples
1. Improving Patient Flow, cont‟d
Discharge Ward Utilisation – the „norm‟ rather
than the exception… recent improvement
Discharge „Rounding‟ – senior staff incl Exec on
the floor…
Review bed stock allocation to align with
demand – increase MAU capacity

SCGH Four Hour Rule Program
SPICe in action….. examples
2. Reduce complexity of internal ED systems
RAT (Rapid Assessment Treatment) consultant
in ED to ensure early senior input
Admission of Emergency Patients Policy –
rights for ED drs

SCGH Four Hour Rule Program
SPICe in action….. examples
2. Reduce complexity of internal ED systems
Daily NEAT Breach Report - identification of
contributing factors and actions to improve
SCGH Four Hour Rule Program
3. Reduce the Complexity of Admission
interface between ED and AAU/SAU
Development of single admission proforma –
enhance continuity; reduce duplication
SPICe in action….. examples

SCGH Four Hour Rule Program
4. Optimise the admission flow between ED and
specialist wards
MHOA (Mental Health Observation Area) established
within SCGH to enable ED direct admission of
mental health patients. Managed/governed by
NMMHS - 4/24 performance & approp location for
patients
Alternate strategy for escort of MH patients –
deputising security staff (NMMHS-NMHS) - LOS
for MH pts on forms in ED
SPICe in action….. examples
SCGH Four Hour Rule Program
NEAT after Bell (1) …..
Significant improvements
ED KPIs
Pre 1000 discharges
Target (81%) met 13/51 days
(mid Oct – early Dec)

SCGH Four Hour Rule Program
NEAT after Bell (1) ….
2008 Jan 46% 2009 Jan
39%
2010 Jan 46%
2010 Aug 50%
2011 Jan 68%
2012 Jan 71%
2012 Aug 52%
2013 Jan 62%
2013 Aug 62%
2013 Oct 77%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
2008 2009 2010 2011 2012 2013
Four Hour
Rule Program
commenced
Solution
implementation
commenced Stokes Review
Aug 2013 -
Bell Audit
Sept 2013 -
Establish SPICe &
Action Plan

SCGH Four Hour Rule Program
Keeping the SPICe going … change in
action..key factors
Leadership
Clear goals & expectations
Improved leadership of actions
Involvement of snr staff – audit / rounding
Accountability
Data data data
SPICe Action Plan – action driven (RAG
status)
Managing performance < expected

SCGH Four Hour Rule Program
Keeping the SPICe going … change in
action..key factors
Communications / Involvement
Getting the message to everyone
Involving staff - all levels, all disciplines
Patient focus vs target focus
Looking for quick wins
Getting back to basics
SCGH Four Hour Rule Program
Bell Audit (2) – March 2014
Follow-up audit – similar audit team led by
Prof Derek Bell
Same method as previous
Outcomes
Team acknowledged that much hard work
had taken place in the last few months
Staff expressed “ED a safer department
now”
Day of Care Survey 16% patients did not
meet criteria vs 27% (August)
Additional recommendations to build on
previous
SCGH Four Hour Rule Program
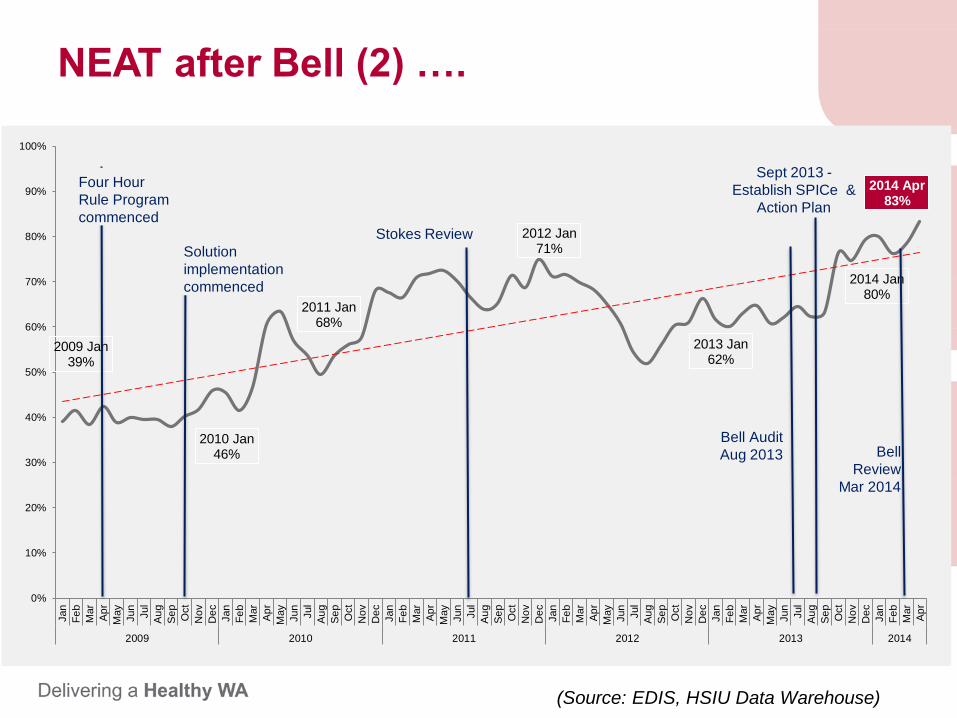
NEAT after Bell (2) ….
2009 Jan 39%
2010 Jan 46%
2011 Jan 68%
2012 Jan 71%
2013 Jan 62%
2014 Jan 80%
2014 Apr 83%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
May
Jun
Jul
Au
g
Se
p
Oct
No
v
De
c
Jan
Fe
b
Mar
Ap
r
2009 2010 2011 2012 2013 2014
Four Hour
Rule Program
commenced
Solution
implementation
commenced
Stokes Review
Bell Audit
Aug 2013
Sept 2013 -
Establish SPICe &
Action Plan
Bell
Review
Mar 2014
(Source: EDIS, HSIU Data Warehouse)
SCGH Four Hour Rule Program
And now…..
Acknowledge the dynamic state
Focus on breaches within 4 – 4.30
Monitoring ward consultant led care
Monthly EDD audit & actions
Ward based Discharge Planning process
Bed meeting – revision and new model
Bed turnaround times – ward
Ability to „view‟ ED on MAU & SAU
SCG – OPH transfer / using capacity

SCGH Four Hour Rule Program
NEAT % - current

SCGH Four Hour Rule Program
Sustaining our achievements…
Support leadership
Maintain accountability – use data
Consistent, clear, frequent, RELEVANT messages

SCGH Four Hour Rule Program
Dr Karen Murphy
Sustaining our achievements…
Embed the good – acknowledge reward
celebrate (at all levels / disciplines)
Manage the bad – performance
management, JDF, set expectations
Modify the ugly – continuous improvement
