dph annual report 2013 dr carol davidson, director of public health nhs ayrshire and arran dph...
TRANSCRIPT

DPH Annual Report 2013
Dr Carol Davidson, Director of Public HealthNHS Ayrshire and Arran
DPH Annual Report 2013/14
Dr Carol Davidson, Director of Public HealthNHS Ayrshire & Arran
Public Health Seminar11 November 2014

Director of Public Health Annual Report 2013/14
• Introduction• Population Profile• Deprivation and Health Inequalities• Public Health Priorities – ATOM+• Public Health Screening Programmes
Director of Public Health Report 2013/14

Director of Public Health Report 2013/14
Percentage change in population by age group, East, North and South Ayrshire compared to Scotland, 2001 to 2011
Source: www.scotlandscensus.gov.uk/en/censusresults/downloadablefiles.html
Population change between 2001 and 2011 Census
aged under 15 aged 15 to 64 aged 65 and over-15
-10
-5
0
5
10
15
20
25Scotland
East Ayrshire
North Ayrshire
South Ayrshire
Perc
enta
ge

Projected population of Ayrshire & Arran by age group, 2010 - 2035
2010 2015 2020 2025 2030 20350
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
90,000
100,000
110,000
0-15 16-29 30-49 50-64 65-79 80+
Popu
latio
n
Director of Public Health Report 2013/14
Year

Director of Public Health Report 2013/14
• Mid year population 2012 = 373,189• Live births 2012 = 3,807• Deaths in 2012 = 4,231
Make up of population at 2010 and projected to 20350 -15 year old group 17% 16%16-64 year old group 64% 54%65 + group 19%
30%
Population Profile

Director of Public Health Report 2013/14
• Dialogue on sustaining wellbeing and equity in the long-term
• Shifting funding towards prevention to lower the burden of disease
• Co-production will be an important approach to building assets of individuals and communities
• Shifting care closer to home• Caring for the carers
Key messages and recommendationsdemography
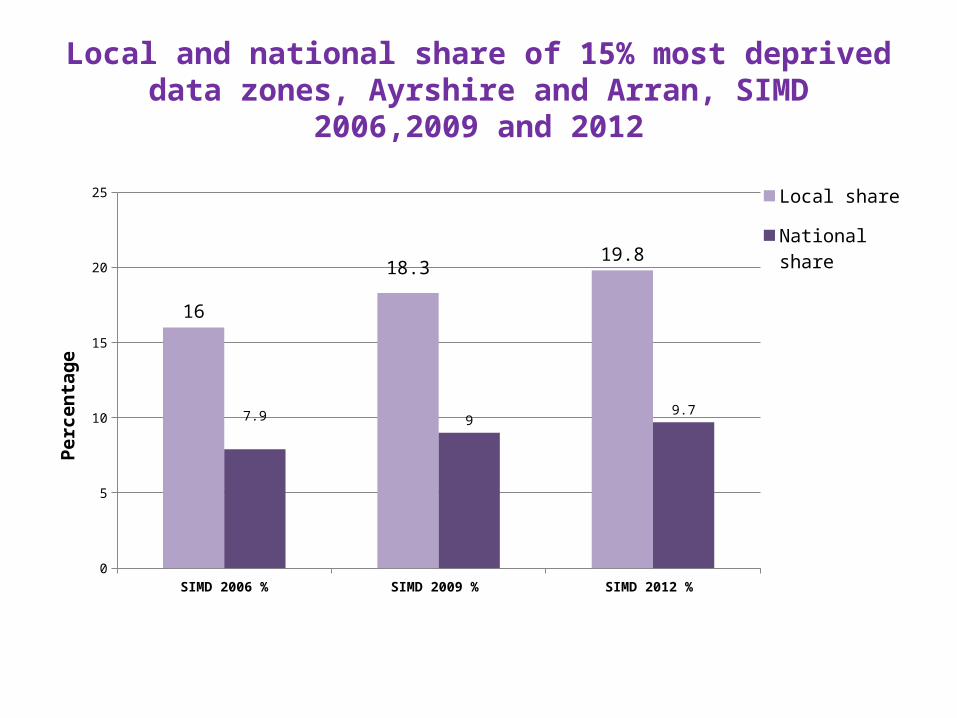
Local and national share of 15% most deprived data zones, Ayrshire and Arran, SIMD 2006,2009 and 2012
SIMD 2006 % SIMD 2009 % SIMD 2012 % 0
5
10
15
20
25
16
18.319.8
7.9 99.7
Local share
National share
Perc
enta
ge

% babies underweight by deprivation, Ayrshire & Arran, 2012
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 50
1
2
3
4
5
6
7
8
9
10
1500-2499g
<1500g
Perc
ent U
nder
wei
ght
Director of Public Health Report 2013/14

% of all women with a known smoking status at first antenatal booking appointment by deprivation,
(2008,2009,2010 combined)
Director of Public Health Report 2013/14
Quintile 1 most deprived
Quintile 2 Quintile 3 Quintile 4 Quintile 5 least deprived
0
5
10
15
20
25
30
35
40
45
40
29
18
119
35
25
18
12
7
Ayrshire & Arran percentage
Scotland average per-centage
Perc
enta
ge (f
rom
3-y
ear c
ombi
ned
tota
ls)

% of women smoking at first antenatal appointment, 2001 - 2012
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012p10
13
16
19
22
25
28
31
34
Ayrshire & Arran
Scotland
Perc
enta
ge o
f wom
en
Director of Public Health Report 2013/14

% smoking quit rate at one month follow-up by deprivation, Ayrshire and Arran and Scotland, 2012
Quintile 1 - most deprived
Quintile 2 Quintile 3 Quintile 4 Quintile 5 - least deprived
0
2
4
6
8
10
12
14
16
13.712.9
9.7
6.6
4.4
12.8
9.8
7.4
5.4
3.5
Ayrshire and Arran per-centage
Scotland average percentage
Quit rate at one month follow-up
Perc
enta
ge

Main causes of death, males and females, all ages for Ayrshire and Arran, 2012
29%
31%
14%
5%
6%
5%
11%
Cancer
Circulatory diseases
Respiratory diseases
Digestive diseases
External causes
Mental & Behavioural
Other
Males
25%
30%16%
6%
3%8%
11%
Females
Director of Public Health Report 2013/14

Main causes of death in under 75 year olds, 2006 – 2012, Ayrshire and Arran
2006 2007 2008 2009 2010 2011 20120
50
100
150
200
250
300
Cancer
Circulatory diseases
Respiratory diseases
EASR
rate
per
100
,000
pop
ulati
on
Director of Public Health Report 2013/14

Director of Public Health Report 2013/14
• Socioeconomic deprivation continues to be a major public health issue in Ayrshire and Arran
• Health inequalities result in a significant loss of years and quality of life for most of society.
• Health inequalities are not inevitable but with tightening public sector budgets, welfare reforms hitting the poorest hardest, the challenge is huge and requires a massive collective effort.
• Circulatory disease, cancer, respiratory disease, digestive disease and intentional/unintentional injury are significant current contributors to inequalities in life expectancy.
Key messagesDeprivation and Health inequalities

Director of Public Health Report 2013/14
• Alcohol-related deaths East, North and South Ayrshire, 1979-83 to 2008-12
• Reducing alcohol availability is associated with a reduction in alcohol-related harm, including medical harms, intentional and unintentional injury and crime. Local Licensing Boards have a key role in the reduction of harm associated with alcohol. All Community Planning Partners must prioritise work to support the Licensing Boards and Licensing Fora in this role.
• Alcohol consumption has also been shown repeatedly to be price sensitive and the
introduction of minimum pricing for alcohol is a landmark policy widely supported by the public health community.
Public Health Prioritiesalcohol
1979
-83
1980
-84
1981
-85
1982
-86
1983
-87
1984
-88
1985
-89
1986
-90
1987
-91
1988
-92
1989
-93
1990
-94
1991
-95
1992
-96
1993
-97
1994
-98
1995
-99
1996
-00
1997
-01
1998
-02
1999
-03
2000
-04
2001
-05
2002
-06
2003
-07
2004
-08
2005
-09
2006
-10
2007
-11
2008
-12
- 5
10 15 20 25 30 35 40 45 50
East Ayrshire North Ayrshire South Ayrshire
Num
ber o
f alco
hol r
elat
ed d
eath
s (5
-yea
r mov
ing
annu
al a
vera
ge)

Alcohol-related hospital discharge rates, Ayrshire and Arran and Scotland, 1997 - 2012
19971998
19992000
20012002
20032004
20052006
20072008
20092010
20112012
0
200
400
600
800
1000
1200
Ayrshire Scotland
EASR
rate
per
100
,000
pop
ulati
on
Director of Public Health Report 2013/14

Public Health Prioritiestobacco
29%
14%
14%
13%
7%
5%
18%
Male cancer deaths, 2012Trachea, bronchus and lung
Bowel (colon, rectum and anus)
Oesophagus and stomach
Prostate
Malignant neoplasm of lymphoid, haematopoietic and related tissue
Pancreas
Other
31%
10%
7%16%
9%
9%
18%
Female cancer deaths, 2012Trachea, bronchus and lung
Bowel (colon, rectum and anus)
Oesophagus and stomach
Breast
Malignant neoplasm of lymphoid, haematopoietic and related tissue
Pancreas
Other
• Tackling tobacco control, and the associated socio-economic and health inequalities, needs to be taken forward in partnership. Health services are best placed to deal with cessation, but collaboration is required with other agencies such as Trading Standards and Education to address the issues of prevention and protection.
• It is vital in moving forward with this agenda that the Pan-Ayrshire Tobacco Control Steering
Group acts as an alliance in sharing information and best practice and lobbying government with regards to future policy and legislation.
• Concerted effort is required by all agencies to help Scotland meet their endgame target of a
smoking prevalence of 5% of the population by 2034. Director of Public Health Report 2013/14
Director of Public Health Report 2013/14
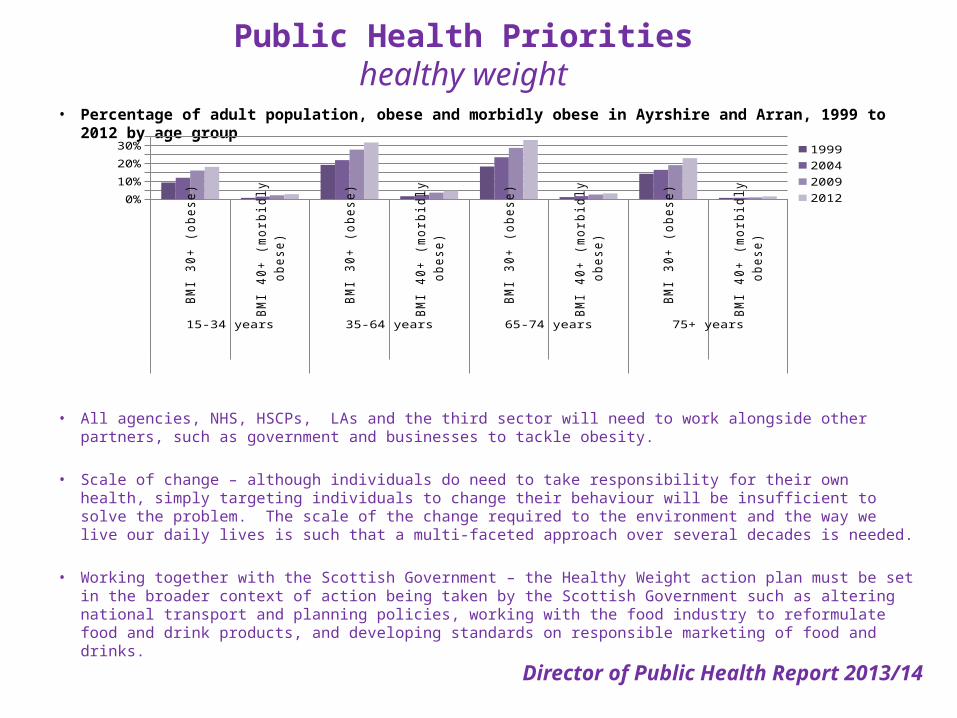
• Percentage of adult population, obese and morbidly obese in Ayrshire and Arran, 1999 to 2012 by age group
• All agencies, NHS, HSCPs, LAs and the third sector will need to work alongside other partners, such as government and businesses to tackle obesity.
• Scale of change – although individuals do need to take responsibility for their own health, simply targeting individuals
to change their behaviour will be insufficient to solve the problem. The scale of the change required to the environment and the way we live our daily lives is such that a multi-faceted approach over several decades is needed.
• Working together with the Scottish Government – the Healthy Weight action plan must be set in the broader context
of action being taken by the Scottish Government such as altering national transport and planning policies, working with the food industry to reformulate food and drink products, and developing standards on responsible marketing of food and drinks.
Public Health Prioritieshealthy weight
BMI 30+ (obese)
BMI 40+ (morbidly
obese)
BMI 30+ (obese)
BMI 40+ (morbidly
obese)
BMI 30+ (obese)
BMI 40+ (morbidly
obese)
BMI 30+ (obese)
BMI 40+ (morbidly
obese)15-34 years 35-64 years 65-74 years 75+ years
0%
5%
10%
15%
20%
25%
30%
35%1999200420092012

Director of Public Health Report 2013/14
Children and young people's mental wellbeing using WEMWBS by deprivation quintile, Ayrshire and Arran compared to Scotland, 2010
• Mental health is a public health priority and it is often said that there is no health without mental health. • The Mental Health and Wellbeing strategy should inform the plans of all agencies • From conception onwards, children’s early life circumstances and experiences shape their physical, social, mental,
emotional and cognitive development and provide a foundation for their future attainment and health. • Positive mental health and wellbeing provides individuals with the resources to enjoy life and with the resilience to
manage life’s challenges. It is a protective factor against mental health problems and is associated with better physical health and the adoption of associated positive lifestyle choices.
Public Health Prioritiesmental health and wellbeing
Quintile 1 - most deprived
2 3 4 Qintile 5 - least deprived
46
47
48
49
50
51
52
53Scotland
Ayrshire and Arran
Mea
n W
EMW
BS sc
ore
(min
=
14, m
ax =
70)

Director of Public Health Report 2013/14
• The wellbeing of children and young people must remain a priority for NHS Ayrshire & Arran and our planning partners. The scale of the challenge is significant as the overall health and wellbeing of the population needs to improve and we also need to reduce health inequalities.
• Tackling threats to wellbeing and inequalities requires a sustained focus on behaviour change. Perinatal smoking cessation, promoting a positive message around abstinence from alcohol in pregnancy, promoting breastfeeding, a healthy diet and physical activity and acting to improve maternal and child mental health remain the central issues.
• To reflect the changing partnership arrangements, we will refresh our shared vision for protecting and improving the health and wellbeing of children and young people. This vision will link together all planning partners across Ayrshire and Arran.
Key messages and recommendationschildren and young people

Key messages and recommendationschildren and young people
• In tandem, we will develop a framework for measuring the health and wellbeing of children and young people across the population in Ayrshire and Arran.
• We recommend that a holistic approach to child health and wellbeing is adopted, underpinned by the National Practice Model. This model and the new Children and Young People (Scotland) Act should be implemented consistently across the acute sector and the three health and social care partnerships in order to move services to a progressive universalism. This approach should include early, systematic identification of needs and early, proportionate intervention in order to improve the outcomes for children.
• In order to achieve cultural change, we recommend that all partners agree a common approach to staff training which equips them to support children’s rights across the public sector and wider society.
Director of Public Health Report 2013/14
The UK National Screening Committee defines screening as:“…a process of identifying apparently healthy people who may be at increased risk of a
disease or condition. They can then be offered information, further tests and appropriate treatment to reduce their risk and/or any complications arising from the disease or condition.”
Detect Cancer Early• Cancer survival in Scotland is poor compared to the rest of the UK and Europe. In
Scotland poor survival is mainly due to cancers being detected at a later stage. • Bowel screening uptake is low among men living in the most deprived areas
(particularly working age men).• Women living in deprived areas are less likely to respond to an invitation for breast
screening and more likely to have breast cancer detected later.
Public health screening programmesCervical – bowel – breast – diabetic retinopathy and abdominal aortic aneurysm
Public health screening programmes

Screening Programmes
Screening programme
Target population
Time frame Uptake outcomes
cervical Eligible Women 20-60 years
2011-12 81.1% 21 – invasive ca576 referrals colposcopy
bowel Adults 50 – 70 years
Nov 2010 to Oct 2012
54.8% 2.8% positivity rate ; 0.2% ca
breast Eligible Women 50 – 70 years
2011 74% 123 ca detected (1.0%)
Diabetic retinopathy
People over 12 years with diabetes
April 2012 to March 2013
80.1% 3.4% positivity rate
Abdominal Aortic Aneurysm
Men in 65th year
June 2013 to Dec 2013
78.4% 31 under surveillance
Director of Public Health Report 2013/14
• Babies and infants are routinely immunised against a range of diseases including diphtheria, tetanus, polio, pertussis and Haemophilus influenzae type b, pneumococcal infection and later against Meningitis C, measles, mumps and rubella. Where appropriate, they may also be immunised against hepatitis B and tuberculosis.
• Uptake of childhood immunisation at 24 months in Ayrshire and Arran remains at a consistently high level of 98% and continues to exceed national targets.
• The past variation in immunisation uptake between East, North and South Ayrshire Council areas has reduced and the rates continue to be higher than the Scottish average.
• Uptake of MMR 1 at age 24 months has reached the target of 95% for the first time and is above the national average of 95%.
Childhood Immunisation in Ayrshire and Arran

Summing up• This report provides a broad picture of the health and wellbeing of the population
in Ayrshire and Arran, with a substantial focus on inequality.
• As we consider how we sustain public services we need to be mindful of the impact of population change on demand for services.
• Government legislation is resulting in unprecedented change in the way health and social care services are organised in Ayrshire and Arran, providing opportunities for change.
• A key element is the importance of community engagement so that services are delivered with communities rather than to them.
• The population is growing older with people living longer, often with multiple health and social care needs. Changes in the population are therefore everyone’s business.
• The changes are also a chance to focus organisations and the communities which they represent to work towards the common goal of living healthier, happier lives.Director of Public Health Report 2013/14