
www.england.nhs.uk
Improving Inhaler Technique through Community Pharmacy Service
Greater Manchester Area TeamAutumn 2014

www.england.nhs.uk
Service Specification
www.england.nhs.uk
• Built upon the MUR/Prescription Intervention advance service
• Any patient eligible for a Prescription Intervention can be invited to join the scheme
• Patients newly prescribed an inhaler should receive inhaler technique training via NMS- outside of this project
• Patients entitled to one PI; one brief intervention; and one MUR in a 12 month period
Service Details
www.england.nhs.uk
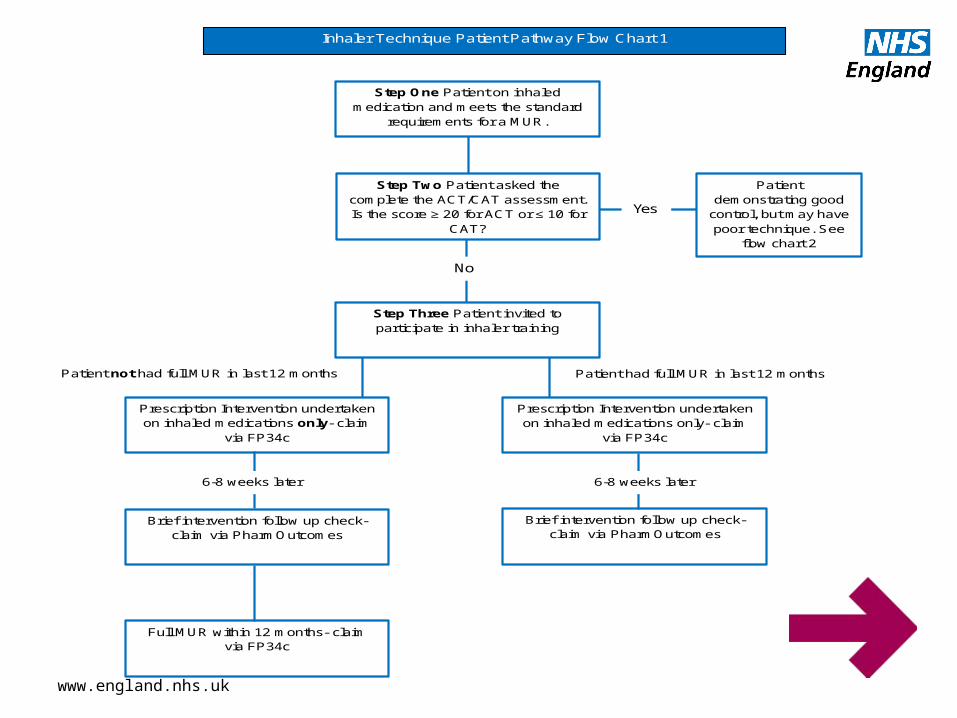
Step One Patient on inhaled medication and meets the standard
requirements for a MUR.
Step Two Patient asked the complete the ACT/CAT assessment. Is the score ≥ 20 for ACT or ≤ 10 for
CAT?
Step Three Patient invited to participate in inhaler training
Patient demonstrating good
control, but may have poor technique. See
flow chart 2
Prescription Intervention undertaken on inhaled medications only- claim
via FP34c
Prescription Intervention undertaken on inhaled medications only- claim
via FP34c
Brief intervention follow up check- claim via PharmOutcomes
Brief intervention follow up check- claim via PharmOutcomes
Full MUR within 12 months- claim via FP34c
Inhaler Technique Patient Pathway Flow Chart 1
Yes
No
Patient had full MUR in last 12 months Patient not had full MUR in last 12 months
6-8 weeks later 6-8 weeks later

www.england.nhs.uk
Patient has an ACT/CAT score ≥ 20 for ACT or ≤ 10 for CAT?
Inspiration rate checked using In-Check® device
Follow Flow Chart 1 from Step Three
Does the patient meet the standard
requirements for an MUR?
Perform MUR- claim via FP34c
Patient to be invited back for an MUR when meets national eligibility criteria
In-correct inspiration rate demonstrated
Correct inspiration rate demonstrated
Yes No
Inhaler Technique Patient Pathway Flow Chart 2
www.england.nhs.uk
• Required data and patient consent to be captured on consultation form(s)
• Information to be entered on to PharmOutcomes• Consultation form(s) to be retained in the pharmacy;
copy to be sent to patients GP• Payment for PI to be claimed via FP34c (£28)• Payment for brief intervention generated via
PharmOutcomes (£10)• Expressions of Interest to provide the scheme to be
circulated to contractors shortly
Service Details
www.england.nhs.uk
• PREM1 to be submitted to AT (if not previously done)• Intervention to take place in the consultation room• Telephone interventions are not allowed• Offsite consultations are permitted, apply to the AT via
the standard NHS England procedure http://www.england.nhs.uk/pharm-adv-serv/
• Signed SLA submitted to AT
Premises Requirements
www.england.nhs.uk
Pharmacist Accreditation

www.england.nhs.uk
• Accredited to undertake MURs• Undergone face to face inhaler technique training
since 2011• Completed the Declaration of Competence for
Improving Inhaler Technique through Community Pharmacy
Pharmacist requirements
www.england.nhs.uk
• Soon to be launched• Pharmacists that have undergone face to face inhaler
technique training are able to start and accredit retrospectively
• Contractors to be informed when DoC available, pharmacists providing the service will have 2 months after launch to complete
• Copy of DoC to be kept in the pharmacy
Declaration of Competence

www.england.nhs.uk
Top Tips
www.england.nhs.uk
1. Check the patient’s PMR for frequency of ordering of medication before starting the review.
For patients with asthma• Ordering more than twelve short-acting reliever inhalers
over the last year may indicate poor control and that preventative treatments need to be stepped up.
• Generally patients with asthma should require thirteen inhaled corticosteroid (ICS) preventer inhalers per year (might be less for 200 dose metered dose inhalers).
• Is the patient prescribed a long-acting beta 2 agonist (LABA) without an ICS? This requires a review of the regimen.
Top Tips for Respiratory MURs

www.england.nhs.uk
2. What does the patient know about their condition and its treatment?
3. Has the patient had a review before? Who did the review? Does the patient see anyone else for their condition? Explain that the reviews are being done with the knowledge of GP practices in the area and that the aim is to improve medicines use for respiratory conditions.
4. Check adherence with the information from the PMR and document any reasons for non-adherence e.g. difficulty in using device, side-effects, perception of ineffectiveness, lack of knowledge of indications for different inhalers. Does the patient experience any problems taking / using their medicines?
Top Tips for Respiratory MURs

www.england.nhs.uk
5. Assess inhaler technique - use In-check device. Would the patient benefit from a device switch, adding a spacer? Does the patient have the same devices i.e. MDI or Turbohaler?
6. Does the patient know how to take other medicines prescribed for their respiratory condition e.g. rescue packs of corticosteroids / antibiotics, mucolytics or theophylline for COPD.
7. Give smoking cessation advice if appropriate.
8. Does the patient need flu or Pneumococcal vaccination?
Top Tips for Respiratory MURs
www.england.nhs.uk
9. Does the patient have any questions / need more information about their medicines?
10.Refer patients if they report:• An increase in exacerbations• Their symptoms are not controlled• Side-effects of medicines
• Severe or life-threatening asthma exacerbation• Haemoptysis- spitting or coughing up blood
Top Tips for Respiratory MURs








