Download - Worldwide 5%-10% of population 121 million affected ½ depressed adults get treatment WHO, 2009

Worldwide5%-10% of population 121 million affected½ depressed adults get treatment
WHO, 2009

NationallyLife-time prevalence 15.3% -
16.9%
University Student Higher prevalence 8.7% - 43.4%
Andrade et al., 2003; CDC, n.d.; Kessler, 2003; Ohayon, 2007; ACHA, 2009; Steptoe, Tsuda, Tanaka, & Wardle, 2007; Wardle et al., 2004; Vasquez & Blanco, 2008; Wong, Cheung, Chan, Ma & Tang, 2006; Stecker, 2004; Dahlin, Joneborg & Runeson, 2005, WHO, 2009

ACHA NCHA II22.7% felt very sad in the past 12 months
20% felt hopeless in the past 12 months
13.7% felt so depressed it was difficult to function

ACHA NCHA II11.1% of students felt depression affected their academic performance
9.2% of students were diagnosed or treated by a professional for depression
3.8% seriously considered suicide0.8% attempted suicide

SuicideReduced quality of lifeReduced social functioningRole impairmentExcess disability
WHO, 2009; CDC, n.d.; Kessler, 2003; Kessler & Walters, 2003

Occurs with anxietyMore likely to have CVD, DM, asthma, and obesity
More likely to smoke, be physically inactive, and drink alcohol
Andrade et al., 2003; CDC, n.d., Kessler, 2003; Ohayon, 2007

Insufficient30% properly diagnosed and treated
Chizobam et al., 2009; WHO, 2009; Wittchen, 2009

USPSTF (2002) recommends screening for depression in clinical practices that have systems in place that assure accurate diagnosis, effective treatment, and adequate follow-up

Healthy Campus 2010 goal: “improve mental health and ensure access to appropriate, quality mental health services”
ACHA, 2002 p. 66
Unipolar depression:◦Major depressive disorder (MDD)◦Dysthymic disorder◦Depressive disorder not otherwise specified (NOS)
APA, 1994

1. Depressed mood 2. Diminished interest (anhedonia)
APA, 1994

1. Significant weight loss or gain or decreased or increase in appetite
2. Insomnia or hypersomnia 3. Psychomotor agitation or retardation4. Fatigue or loss of energy 5. Feelings of worthlessness or excessive or
inappropriate guilt6. Diminished ability to think or concentrate or
indecisiveness7. Recurrent thoughts of death, recurrent suicidal
ideation without a specified plan or a suicide attempt, or a specific plan for committing suicide
A depressive disorder that is characterized by at least two years of depressed mood for more days than not
Accompanied by two of the following:1. Poor appetite or overeating2. Insomnia or hypersomnia3. Low energy or fatigue4. Low self-esteem5. Poor concentration or difficulty making
decisions6. Feelings of hopelessness
Included for diagnostic coding of depression that has features that do not meet criteria for the other depressive disorder

Improve depression careSample of 50 students18% were diagnosed with depression
24% had a history of depression
What are the effects of using the Chronic Care Model (CCM) on depression outcomes with a group of students compared with a group using current practice at a Midwestern university health and wellness center?

Outcomes measured• Detection of depression• Depression improvement• Patient compliance with medication
• Patient satisfaction

Databases Searched ◦Cochrane◦Academic Search Premier ◦CINAHL◦Health Source: Nursing/Academic◦MEDLINE◦PsycArticles◦ERIC

Key Terms Used◦Depression and multifaceted interventions
◦Depression and collaborative care◦Depression and chronic care model◦Depression and disease management

Inclusion CriteriaInclusion Criteria◦ January 1, 1999 to January, 31
2010◦ English◦ Age 18 to 64◦ More than one intervention ◦ Primary care

Exclusion CriteriaExclusion Criteria◦Patients with pre- or postnatal depression
◦Care specific to one gender

Abstracts identified using search terms
N = 939
Articles met criteria for review
N = 38
ExcludedN = 901
Articles met criteria for review
from hand searchesN = 63
Articles met inclusion criteriaN = 14
Articles valid and reliable
N = 9
ExcludedN = 87
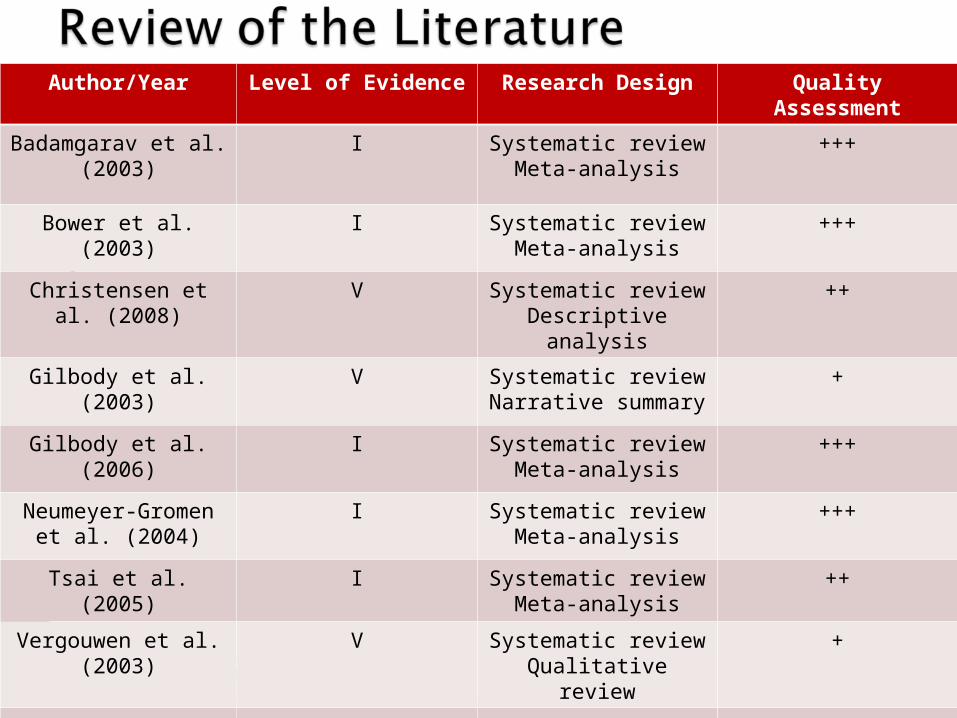
Author/Year Level of Evidence Research Design Quality Assessment
Badamgarav et al. (2003)
I Systematic reviewMeta-analysis
+++
Bower et al. (2003) I Systematic reviewMeta-analysis
+++
Christensen et al. (2008)
V Systematic reviewDescriptive analysis
++
Gilbody et al. (2003)
V Systematic review Narrative summary
+
Gilbody et al. (2006)
I Systematic review Meta-analysis
+++
Neumeyer-Gromen et al. (2004)
I Systematic review Meta-analysis
+++
Tsai et al. (2005) I Systematic review Meta-analysis
++
Vergouwen et al. (2003)
V Systematic review Qualitative review
+
Williams et al. (2007)
V Systematic reviewDescriptive analysis
+

• Sample sizes: 10 – 55 articles• Patients described as depressed• 5-18 multifaceted interventions
used

Models that guided the literature search and interventions:
Chronic Care Model (3 reviews) Collaborative Care (3 reviews) Disease Management Program (2
reviews) 1 looked at multifaceted
interventions

Interventions:1.Delivery system design:
◦ Case management◦ Regular follow-up◦ Culturally appropriate care ◦ Defining each provider’s roles and
tasks
ICSI, 2009; Wagner et al., 1999

2. Self-Management Support: Educating patients about their disease
Providing emotional support Helping set priorities and goal setting Developing strategies for living withchronic illness
ICSI, 2009; Wagner et al., 1999

3. Clinical Information Systems Electronic health records Paper registry systems
ICSI, 2009; Wagner et al., 1999
4. Decision Support Provider education to stay up to date Evidence based guidelines in daily
practice Sharing of evidence based guidelines
and information with patients to encourage their participation
ICSI, 2009; Wagner et al., 1999

5. Community Resources Encouraging patients to participate in
effective community programs Forming partnerships with community
organizations to support patient interventions
Advocating for policies to improve patient care
ICSI, 2009; Wagner et al., 1999

6. Health System Leadership that visibly supports
improvements at all levels Leadership that provides incentives based
on quality of care Leadership that encourages open and
systematic handling of quality problems to improve care
ICSI, 2009; Wagner et al., 1999

Outcomes from implementing multifaceted interventions caused improvement in:1. Depression (all 9 articles)2. Medication adherence (6 out of 6
articles)3. Patient satisfaction (2 out of 2
articles)4. Depression detection through
screening (1 out of 1 article)

• Less likely to cause depression improvement: Provider education and feedback
• More likely to cause depression improvement: Case management and patient preference

• Systematic reviews• Provider preference• CCM• PHQ-9 depression screening tool• Institute for Clinical Systems
Improvement (ICSI; 2009) practice guideline

RN Discuss the Project with Patient
2 simple questions
PHQ-9 screening tool
Randomly draw envelope
DeclinesUsual Care
UnexposedUsual Care
No Usual Care
Score 0-4Usual Care

PHQ-9 screening tool
InterviewAssess
comorbiditesTreat
Assess response
Good: Continuation or Maintenance
Phase
No: Reevaluate

• Ace Star Model• Quasi experimental design• Convenience sample • University students • Age 18 and older • Midwestern university health and
wellness center • Randomly assigned • Consented
Interventions based on the CCM:
1. Delivery system2. Patient self-management3. Clinical information system4. Decision support5. Community resources6. Health care system

Sample Size91 (65%) agreed to participate and 49 (35%) declined
Eight patients withdrew (8.8%) Total of 83 patients, 47 (57%) exposed, 36 (43%) unexposed

Sample Characteristics for Entire Group
22 males (26.5%) and 61 females (73.5%)
Age range between 19-53 years, mean age 27
15 patients diagnosed with depression (18%)

Demographic Data for Entire Patient Population in Study
Demographi
csExposed Unexposed Test
Resultp
Female % (n=83)
70 (n=47) 78 (n=36) X²(1) = .599 0.439
Age, mean (sd) (n=81)
28.70 (8.87)(n=46)
25.89 (7.19)(n=35)
t(79) = 1.53 0.130

Demographic Data for Depressed Population
Demographics
Exposed (n = 10)
Unexposed (n = 5)
Test Result
p
Female % 55.6 44.4 X²(1) =1.25 0.264
Age, mean (sd)
31.50 (12.42) 22.40 (1.14) t(9.30) = 2.30 0.046

Demographic Information for Depressed Patients (n = 10)

(n = 10)
10% declined medication/counseling 70% used antidepressant medication 90% used on-campus counseling 30% referred to psychiatrist

21.3% detected in the exposed 13.9% detected in the unexposed
X²(df) = .751(1) p = .386
No statistically significant difference

N Initial Mean PHQ-9 Score (sd)
Final Mean PHQ-9 Score
(sd)
t test
6 16.67 (7.12) 9.00 (5.37) t(5) = 2.15,p > .05
10 17.80 (6.01) 9.20 (4.26) t(9) = 3.63 p = .005
Outcome 2: Changes in PHQ-9 Scores

Outcome n Exposed (%) Unexposed (%)
X²(df) p
Improved depression
13 75 (n = 9) 25 (n = 3) 4.88(2) 0.087
Medication compliance
14 83.3 (n = 10) 16.7 (n = 2) 3.97(2) 0.141
Outcome 3 and 4:

Patient Satisfaction with the Care Received◦ Of the questionnaires sent out◦ 4 (11%) completed with 2 (50%) in the exposed
and 2 (50%) in the unexposed group
◦ 5 (14%) returned with no forwarding address◦ 6 (16%) completed without a name

Patient Satisfaction (continued)◦ Mean PHQ-9 score: 91.75◦ No significant difference between the 2 groups
Patient Group
N Mean Score
Minimum
Score
Maximum
Score
sd
Total 4 91.75 81 99 7.63
Exposed 2 90.00 81 99 12.73
Unexposed
2 93.50 93 94 0.70

Strengths of the project◦PHQ-9 scores improved◦Current staff ◦No increase in budget◦NP feedback positive◦PHQ-9 screening tool improved
communication

Recommendations about implementation◦Increase sample size◦Implement multi-center design◦Utilize different patient satisfaction survey◦Change the location of the educational
brochures◦Ensure consistency in demographic data
collection and PHQ-9 screening◦Longer than 12 weeks
Implications for nursing◦Multidisciplinary approach◦Campus resources linked◦APN education of chronic illness

Implications for nursing◦Further research needs to be completed Larger sample size NP vs. MD Interventions with the greatest impact Use with other chronic conditions

“Depression is the inability to construct a future.”Rollo May







