Download - The$PerfectStorm$ - nebula.wsimg.com

The Perfect Storm Claudia Tessier RHIA MEd
ICD-‐10 and Medical
Transcrip4on
Copyright, C. Tessier, 2013

Some relevant informaEon about me • I co-‐developed Coding for Healthcare Professionals, an online program for learning medical coding.
• I am a consultant with an internaEonal firm (ID InformaEon and DocumentaEon in Healthcare) that designs coding soMware and is introducing its ICD-‐10 soMware into the US.
• Thus, much of my ICD-‐10 knowledge comes from them – BUT I learned and taught ICD-‐9 coding years ago.
• I was CEO of the American AssociaEon for Medical TranscripEon for 18 years
• I authored The AAMT Book of Style for Medical Transcrip;on (1st ediEon)

The Perfect Storm of Opportunity
• “Evolving” medical transcripEon pracEce and business models
• Increasing adopEon of technologies: EMR, SR, CAC, NLP...
• Impending transiEon to ICD-‐10 • Need for qualified coders
Integrate Medical Coding with Transcrip4on
The Strategic View of Medical TranscripEon

Just what is ICD-‐10? • ICD: InternaEonal ClassificaEon of Diseases
– Standard classificaEon: general epidemiological reporEng, also health management and clinical purposes
– Started in 1850s, 1st ediEon 1893: InternaEonal List of Causes of Death – WHO became responsible in 1948 with 6th revision -‐ first ediEon to
include morbidity causes in addiEon to mortality • ICD-‐9 – adopted in 1977 • ICD-‐10
– Endorsed by 43rd World Health Assembly in 1990 – Adopted by WHO member states in 1994 – US is among last few countries to adopt ICD-‐10
• IniEal adopEon date: October 1, 2013 • HHS has proposed delay to October 1, 2014

Why not stay with ICD-‐9? Because it’s outdated!
• Designed for reporEng morbidity and mortality
• Lacks structure and granularity for clinical decision making and research
• Matches imperfectly in more than 95% of cases
• Can’t keep up with advances in medicine and healthcare
• Can’t be relied on to support conEnuity of care and management

The ICD-‐10 Challenge
• Increase from 17,000 to 155,000 codes • 25% to 50% decrease in coder producEvity • Increase in 3 % error rate to 6% to 10% • Denial rate increase 10% to 25%2
• 10%+ charts will not have documentaEon specific enough for coding2
Huge changes and demands

Increased specificity in ICD-‐10-‐CM: Knowledge that MTs already have or know how to find.
• Laterality • Episode of care – iniEal subsequent, sequelae • CC/MCC (complicaEons and co-‐morbidiEes/master complicaEons and
co-‐morbidiEes • Acuity • Anatomic detail • SupporEng lab values • Qualifiers: severity, chronic/acute, accompanying condiEons, eEology, fracture
type, etc. • CausaEve agents, drugs, diseases, geneEcs • Disease processes connected to common manifestaEons • Alcohol, tobacco, and drugs • Expanded codes for injury, diabetes, alcohol/substance abuse, postoperaEve
complicaEons • Updated clinical terminology (e.g. diabetes mellitus, malignant/benign
hypertension -‐ e.g., 6 diabetes mellitus categories • Changes in Eme frames specified in certain codes, e.g., trimesters • Lack of specificity more physician queries

Benefits of ICD-‐10 • That increased specificity will
– Improve cost analyses and resource uElizaEon – Enhance comparability for volume, cost, morbidity and mortality
– Facilitate opportuniEes for quality improvement – Improved revenue stream resulEng from documentaEon improvement
– Enhance disease management and protocol development – Support meaningful use – Facilitate strategic posiEoning – Facilitate epidemiological and bio-‐surveillance acEviEes
Source: Rose Dunn “Bemer Late than Never: How to Catch up with ICD-‐10-‐CM/CPS in 2012,” AHIMA ICD-‐10 Summit, April 2012
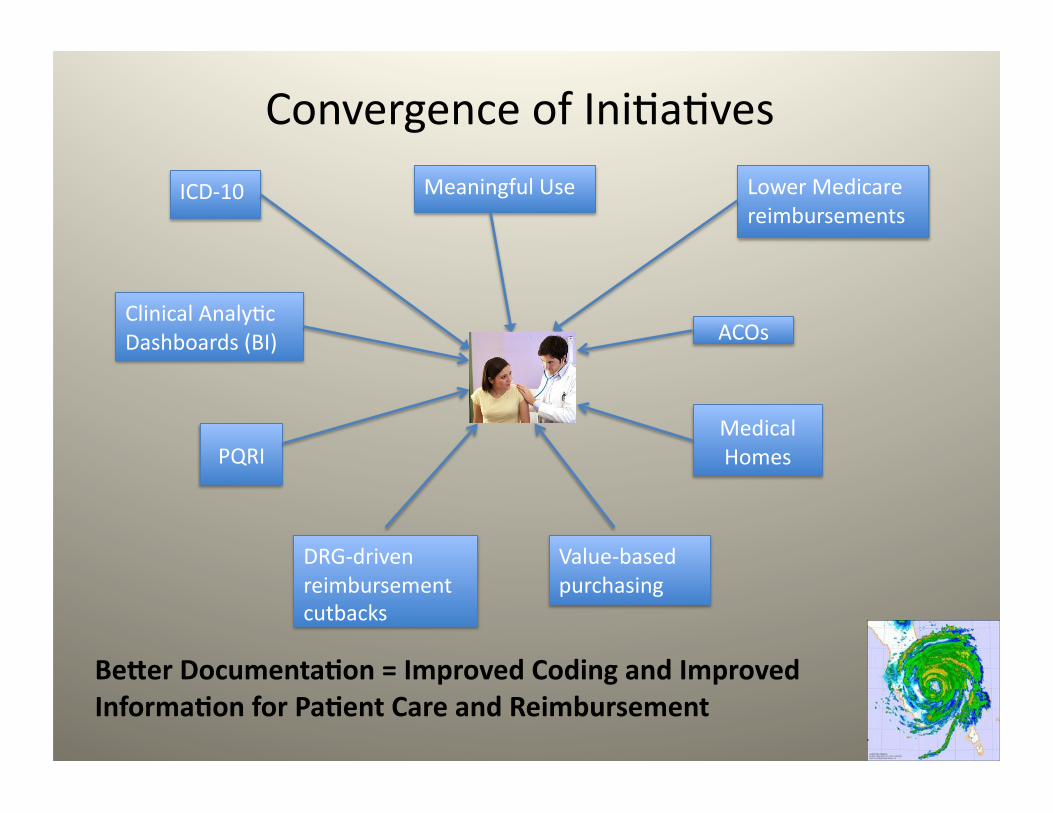
ICD-‐10 Meaningful Use Lower Medicare reimbursements
ACOs
Value-‐based purchasing
Medical Homes
DRG-‐driven reimbursement cutbacks
PQRI
Clinical AnalyEc Dashboards (BI)
Be>er Documenta4on = Improved Coding and Improved Informa4on for Pa4ent Care and Reimbursement
Convergence of IniEaEves

Changing Regulatory Environment
• Federal/state payment iniEaEves and reforms impact documentaEon and coding
• ICD-‐10 will bring greater demands – Clinical documentaEon must be more specific – Coder producEvity will drop – Training will take coders and CDI specialists away from daily workflow
Opportunity!

RelaEonship between EHRs and ICD-‐10
• Some EHRs are successful without structured documentaEon BUT
• Specific structured clinical data are needed to achieve meaningful use AND
• ICD-‐10 clinical documentaEon must be highly structured
• Therefore, the documents you transcribe will become increasingly structured

ICD-‐9 to ICD-‐10 TransiEon Impacts Coders
• Coders need expanded clinical, medical language, anatomy and physiology, pharma, lab data knowledge.
• Intelligent coding is the key to accuracy
OPPORTUNITY!

ICD-‐10 and Clinical DocumentaEon
• Data integrity is the Issue – Must capture specificity in documentaEon
– So, how to improve documentaEon accuracy
• Predicted 10% to 20% increase in documentaEon in response to ICD-‐10
• Denials will increase iniEally

Medical TranscripEonists as Coders • Both require knowledge of
• medical language • anatomy and physiology • clinical assessments • diagnoses, • treatments • procedures • pharmacology • pathophysiology • laboratory pracEce
• Both must be able to – Read and understand paEent medical records – Abstract paEent informaEon quickly and accurately – Research clinical informaEon effecEvely

Impact of ConnecEng Coding with TranscripEon
• Expanded pool of qualified coders • Delayed or incomplete coding instances reduced • Diagnoses and procedures supplemented by MTs’ knowledge of and
access to content • Coding process facilitated and streamlined • Improved clinical documentaEon • Reimbursement based on more accurate, complete, and Emely
coding • Delayed reimbursement due to requests for supporEng
documentaEon to support diagnoses diminished • Clients potenEal for revenue increased • More accurate, complete, and Emely coding • Clinical documentaEon services will provide valued service to clients potenEal for increased revenue
ENHANCES MT VALUE

Coding Resources
• The usual – medical dicEonaries, word books, pharma and lab resources, etc.
• Plus – CAC – computer assisted coding – NLP – natural language processing – Remote coding – EHR-‐supported coding – Automated feedback – CDI efforts -‐ clinical documentaEon improvement

Use of PaEent Documents
Coders
• History and physicals • Discharge summaries • ConsultaEons • Progress notes • OperaEve and procedure
reports
• Radiology reports • Pathology reports
Medical Transcrip4onists

Coding with ICD-‐10

Crosswalk: ICD-‐9 to ICD-‐10

Clinical DocumentaEon Improvement • MigraEng paper records to electronic via hybrids
• Deliberately discourages – Copy and paste – HandwriEng – Free text narraEves
• ParEal soluEons – Templates – Speech recogniEon – Direct entry via pick lists, pull-‐down menus…

Clinical DocumentaEon Improvement • Physician clinical documentaEon goals – Standardized content and streamlined workflow
– Address quality and regulatory consideraEons – Avoid financial penalEes for poor documentaEon – Enhance clinical value
• Technology advancements
• Workflow changes

Workflow Changes • DocumentaEon in mulEple locaEons vs centralized records
• Automated feedback to clinicians as they document • CDI (clinical documentaEon improvement) programs • TranscripEon-‐supported coding • Concurrent coding via EMR • Electronic queries generated within EMR • Remote coding, chart reviews/audits • Include query response TAT within suspension process • Final coding

Concurrent CDI and Coding
• The route toward data improvement and integrity
• DocumentaEon leads to coding
• Ergo…
Opportunity!

Technology Changes Impact Coding • Increased use of technology improves producEvity, compliance, consistency of documentaEon and therefore of coding – CAC, NLP – ICD-‐10 crosswalks and mapping – DRG Grouper – OpEmizaEon of EHR-‐supported coding – Electronic queries and templates
What is Computer-‐assisted Coding?
• “…the use of computer soMware that automaEcally generates a set of medical codes for review, validaEon, and use based upon clinical documentaEon provided by healthcare pracEEoners.”
– Delving into Computer-‐assisted Coding
(AHIMA PracEce Brief, 2004)

Impact of CAC on Coding
• First 9 months, expected 50% decrease in efficiency
• CAC can offer gains up to 30%, reducing impact to 20%
• Staff augmentaEon necessary • Increase coder efficiency – PotenEal code alerts – Reports/results accessible online – Reduce paper shuffling – Automated workflow

CAC Goals • Solid foundaEon for ICD-‐10 readiness • Seamless integraEon • Improved documentaEon • Improved quality • Greater producEvity • Greater consistency • Real-‐Eme coding • AutomaEon/integraEon of criEcal documentaEon data, e.g., POA, ROM, SOI • Reduce labor and outsourcing costs • Generate correct, compliant billing • ReducEon in denials • Reduce A/R days and DNFB • Improves capture of paEent severity • Facilitates idenEficaEon of PSI/HAC • Integrates with CDI and improves DRG accuracy and potenEal queries to physicians • Improves coder and CDI staff saEsfacEon • Facilitate communicaEon between coders, CDIS, clinicians, MTS
MulEple goals of significant benefit to paEent care and reimbursement
NLP and CAC
• CAC with natural language processing as single platorm is best soluEon
• Improves workflow and producEon
• Facilitates achieving CAC goals

What is NLP? • A form of arEficial intelligence • Reads text and understands meaning from standard dictaEon/
transcripEon, SR, and templates with free-‐text fields – Most cannot read images of text or handwrimen documents
• Word-‐search funcEons for terms to support clinical findings • Compares new and old documents • IdenEfy query opportuniEes improve producEvity and accuracy • Auto-‐suggest codes • Crosswalk ICD-‐10 and guidelines to alert for addiEonal specificity
needed • Different types
– Rules-‐based – StaEsEcs-‐based – CombinaEon
• May give overwhelming feedback – need to discriminate

NLP: Stage 1 – Documents Uploaded

NLP Stage 2: Analysis and AcEon Begin

Major Concern re TransiEon to ICD-‐10
• Coder shortage and producEvity • ReacEons/soluEons – Training
• Advance • At implementaEon • Ongoing • SomeEmes funded
– RetenEon bonuses – Sign-‐on bonuses
Opportunity!

What is Needed for MTs?
• Training for coding • Understanding of computer-‐assisted coding tools
• Understanding how NLP can be integrated • MarkeEng of new value to transcripEon and to its users
What about ICD-‐9-‐CM?
• Learning ICD-‐9-‐CM is a bonus • Dual coding (ICD-‐9 and ICD-‐10) will be done for months prior to the implementaEon date for ICD-‐10 and for some Eme aMer
• Dual coding will allow comparisons of case mix, revenue, documentaEon, etc.
• Knowing both ICD-‐9-‐CM and ICD-‐10-‐CM/PCS will enhance qualificaEons
MTs have a Key Advantage
They already know so much about disease processes, medical terminology, patho-‐physiology, laboratory data, pharmacology, etc.

Training Requirements • Variable depending on clinical knowledge and knowledge of coding systems
• Medical transcripEonists • Already have clinical knowledge • Need to gain in-‐depth knowledge of coding systems
• Need course work plus lab Eme

Training OpEons • Internal resources • Colleges/community colleges/technical schools
• ApprenEce programs
• Online programs
• Websites
• YouTube • Professional associaEons • MT resources, e.g. MT Tools Online

Coding Training
• AHIMA – approved coding cerEficate program directory – Find sites athmp://www.ahima.org/careers/college_search/search.aspx
– Search by state and by whether onsite or distance learning

Coding CredenEals for Hospitals or Physician’s Offices – AHIMA*
• CCA – cerEfied coding associate – first-‐level • CCS: cerEfied coding specialist – mastery-‐level • CCS-‐P: cerEfied coding specialist-‐-‐physician-‐based
Note: The U.S. Department of Labor's Bureau of Labor Sta;s;cs projects a 20% increase in employment before 2018 for the Medical Coding and Billing field, which includes medical coding and billing professionals. This represents more than 37,000 new jobs.
• AHIMA coding creden;als are the only ones currently accredited by the Na;onal Commission of Cer;fying Agencies

Coding CredenEals for Physician Offices and OutpaEent Hospitals – AAPC*
• CPC: cerEfied professional coder – physician’s office
• CPC-‐H: cerEfied professional coder – outpaEent hospital
• CPC-‐P: cerEfied professional coder – payer • CIRCC: cerEfied intervenEonal radiology cardiovascular coder
• MulEple specialty coding credenEals *American Academy of Professional Coders

2008 AHIMA Salary Survey for Coders
Coders working in consulEng services • average salary of $57,700.
Otherwise, averages range from • $36,502 for coders in home health or hospice to • $48,115 for those in non-‐provider sezngs.

Medical Coder Salaries: 2011 AAPC survey
•
Average for CPC was $46,900 (up $1400 from previous year). Over half the respondents reported earning more than $40,000.

Recent PosEngs: Medical Coder Salaries
• InpaEent/DRG Coder $38-‐$59K • Remote coder $43-‐$75K • Coding Supervisor $50-‐$60K • Traveling IP Coders, Full travel $50-‐$60K • Home-‐based Lead Coder Up to $60K • InpaEent Coder $56-‐$78K • Corporate Coder $65-‐$75K • Senior IP/DRG Coder $68K
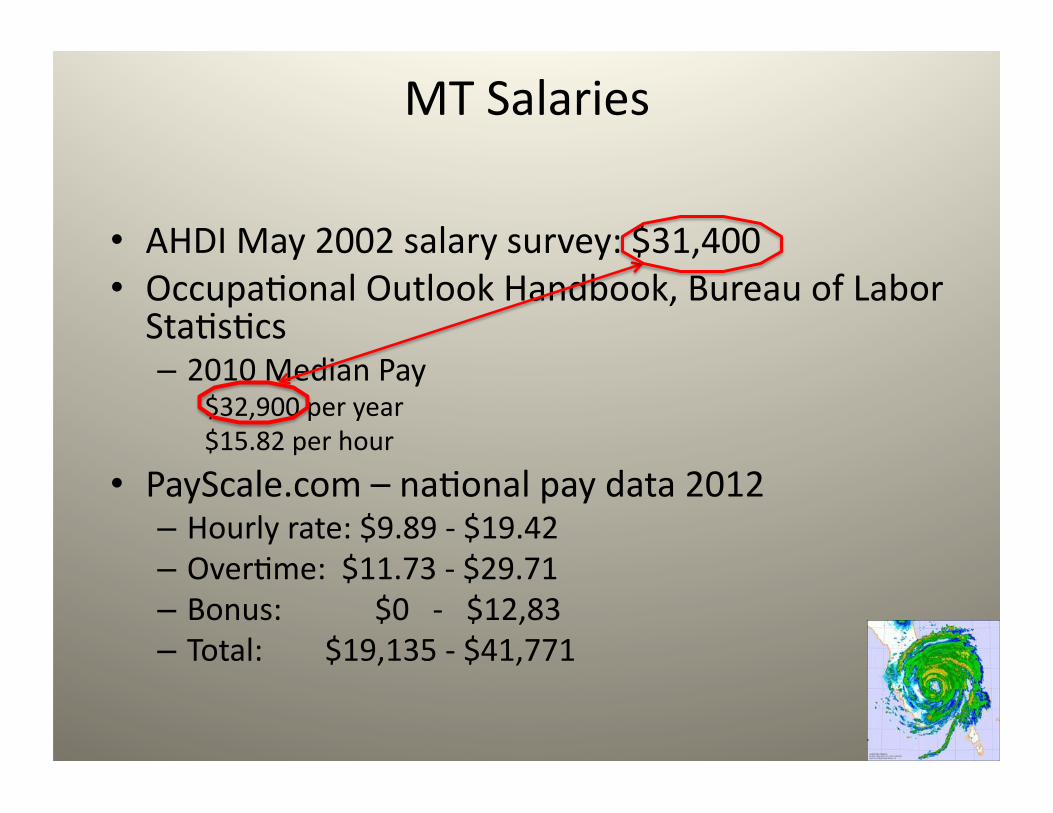
MT Salaries
• AHDI May 2002 salary survey: $31,400 • OccupaEonal Outlook Handbook, Bureau of Labor StaEsEcs – 2010 Median Pay
$32,900 per year $15.82 per hour
• PayScale.com – naEonal pay data 2012 – Hourly rate: $9.89 -‐ $19.42 – OverEme: $11.73 -‐ $29.71 – Bonus: $0 -‐ $12,83 – Total: $19,135 -‐ $41,771

Remember?
• Three levels of medical transcripEonists (per 1999 Hay Study)
• With integrated coding skills, medical transcripEonists can create and enter the
Fourth Level
New career opportunity
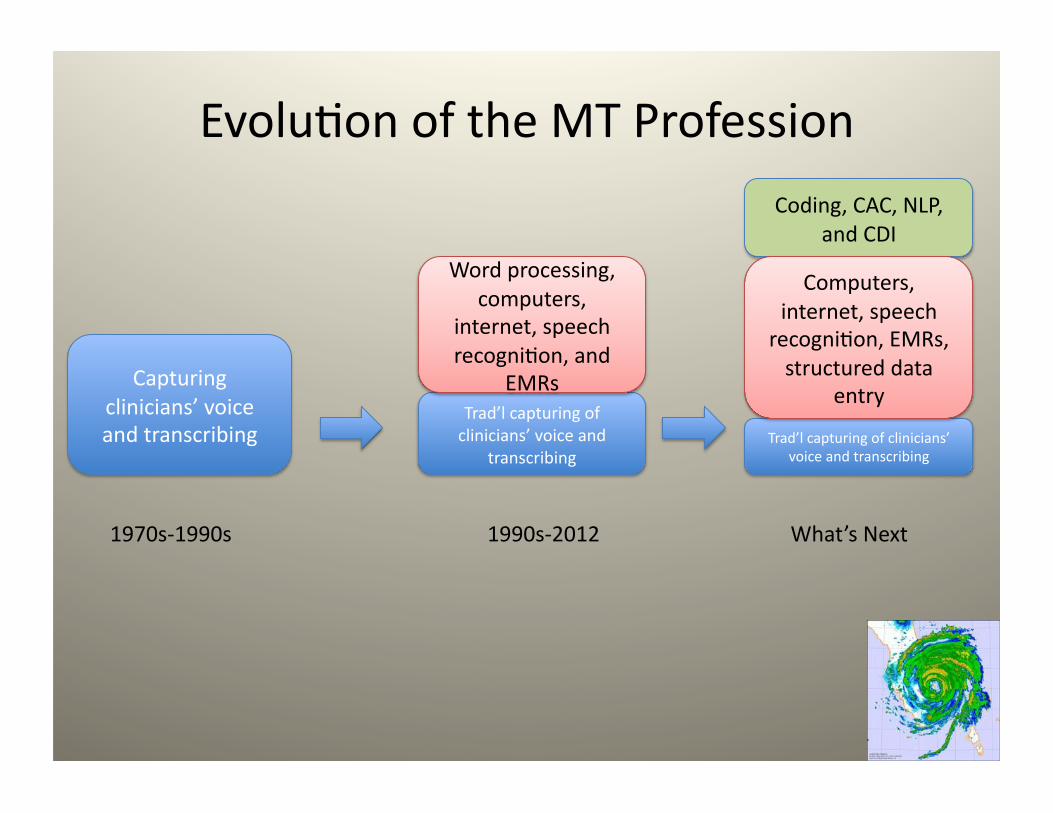
EvoluEon of the MT Profession
Capturing clinicians’ voice and transcribing
1970s-‐1990s
Trad’l capturing of clinicians’ voice and
transcribing
Word processing, computers,
internet, speech recogniEon, and
EMRs
1990s-‐2012
Trad’l capturing of clinicians’ voice and transcribing
Coding, CAC, NLP, and CDI
What’s Next
Computers, internet, speech recogniEon, EMRs, structured data
entry

What do we need?
• A project that addresses both training and integraEon of coding with transcripEon to address – Coding educaEon requirements for MTs
– Process and flow requirements for integraEng coding into medical documentaEon/transcripEon
– Business models
• Rebranding!

QuesEons • How much do we have to invest in training? • How much of transcripEon producEvity will be lost due to coding?
• How much coding producEvity and value will be gained?
• How much can be charged for the integrated process? • How much can MT/coders expect to be paid? • What will it affect status and value of MT? Of coding? • How will it affect paEent care, reimbursement, CDI, etc.?
• How will it affect our future?

So… who will benefit from this perfect storm?
Those with Blue Sky Thinking!

Thank you! – Claudia Tessier RHIA MEd
– [email protected] – www.codingforhcp.com – www.ctessier.com
– +1 617-‐816-‐7513







