
MycobacteriaNocardia
Actinomyces
Prof. Károly NAGY
Institute of Medical Microbiology Semmelweis University
NAGY KÁROLY

� aerobic, rod shape(0.4x3 µm), no spores or cilias
� Can not be stained by Gram , once stained, reisist decoloration by acid or alcohol
Acid-fast bacteria
�
� high level resistance towards chemicals
MYCOBACTERIA (> 50 species, saprophitic)
Pathogenicity Species Reservoire Disease
Pathogenic M.tuberculosis human tbc
M.leprae human lepra
M.bovis bovine, human intestinal-,miliary tb c
Potentially M.avium- soil, birds, water disseminated and lung tbc
Pathogenic intracellulare bovine (frequent in AIDS )
M.kansasii water, bovine lung tbc
M.marinum fish, water sc.nodules, skin ulcers
M.scrofulaceum soil, water granuloma, cervical ly.ad
M.ulcerans human, environment sc.nodules, skin ulcers
M.fortuitum-chelonei soil, water, animals sc.abscess,disseminated
Stained by Ziehl-Neelsen acid-fast dye

lipid bilayerplasma memrane
peptidoglycan
Lipid+LPS
Mycolic acid(mycolyltrehalose:„cord-factor”)
porins
D-arabinoseD-galactose
acyl lipids
Gram negatíve Gram positive Complex (acid-fast )
Ziehl-Neelsen stain
„Cord-formation”
M. tbc

Mycobacterium tuberculosis
Culture: aerobic, slow growth : cell division 18 h
� Solid mediumLöwenstein-Jensen (egg,potato extract
Malachit-green, antibiotics)3-8 weeks
� Broth media
Sula (semisynthetic, Malachit-green)
Growth: clamps, bigger volumes

Mycobacterium tuberculosisPathogenesis
alveolsgranulomalympnodescaverna
Source of infection:Sick humananimal
InfectionAerosol dropletsdustper os (milk)contacts
Tbc develops in < 5% of those infected
Lung granuloma

Mycobacterium tuberculosisPathogenesis
2-4 weeks post infection:�CD4 T-cell cytokins activate macrophages
����Granuloma and caverna formation:cytokine toxycity, complement activation,ischemia, macrophag enzym activity,etc.
High number of bacteria in sputum:primer and secunder infection,high resistance towards drying and chemicals !
Surviving in phagolysosomes
alveolar macrophag

Mycobacterium tuberculosis: Pathogenesis
Focal,cheesy necrosis:Caverna formation

Mycobacterium tuberculosis (tbc): Clinical picture
Pulmonal: lung (middle/lower lobes), lymphnodes, pleura
tünetek: weakness, fatigue,weight loss, caughing, spitting: yellow/green mucus, blood in the sputum, short breath, night sweating, pain in chest, back
• clinical diagnosis• x - ray• microscopy• culture
In those infected disease develops <2years: 5%, > 2 years : additional 5-10%

Extrapulmonal : haematogen or urogen dissemination, contact infectio
• gastrointestional (infected milk)• genito-urinary system (kidney tbc)• bone (deformity)• skin tbc (erythema multiforme, aquarium disease)• scrofula (neck swelling, ulcer)
Mycobacterium tuberculosis (tbc): Clinical picture

IMMUNITY
PRIMER
SECUNDER
Source ofinfection
Gate ofentrance

M. tuberculosis: surviving strategies in macrophag es
- high resistency of lipid/wax cell wall- neutralisation of free radicals- ammonia formation, which inhibits
* formation of phagolysosomes* activity of lysosomal enzymes
„dormant” state

I. type II.type III. type IV.typehypersensitivity
anaphylaxias cytotoxikus immunkomplex delayed, tuber-culin type
IgE IgG IgG -- Complement Complement -- - - T lymphocyte
pollen,animal Rh, bact.,virus, intracellularfur, penicillin gyógyszer fungi, etc, microbeanimal sera animal sera
local,gene- self cell Co activation granulomaralised, ADCC formationodema, his- lysis trombocytetamin activationskinprobe - - skinprobe
M. tuberculosis INDUCED IMMUNE DESTRUCTION

Tuberculin test: Mantoux - probe
Suitable to detect tbc infection or validation of the effect of BCG vaccination
Purified,standardised tuberculoprotein : M.tbc PPD (Purified Protein Derivate)
5 TU intracutan inoculation, < 10 mm induration: negatívread after 48 h 10-20 mm induration: BCG-hypersensistivity
> 20 mm induration: infekctious hypersensitivityNot M. tbc specifcConversion (pozitív): M.tbc infection, BCG vaccination
Reversion (negatív): early infection, miliary tbc, meningitis, AIDS, immunosuppression,
morbilli,varicella, wooping cough , influenza, helmintiosis, old age

THE HISTORY OF TUBERCULOSIS
•Kr.e. 1000 egyptian mummies – bone destrucion, abscess•Hyppokrates: aerosol, droplets infection•Middle ages: „phtysis”, the disease of the lung•Franz de la Boë (1614 – 1672) : „tuberculum”•London, XIX.c.:every 3. death due to tbc•Johan Lukas Schönlein (1793 – 1864): the clinical
definition of tuberculosis (1832)•1882: Robert Koch: a ‘Koch-bacillus” the etiological factor
1890 – tuberculin, 1930- diagnostical meaning•1906: Albert Calmette és Camille Guerin : a „BCG”,
the possibility of active immunization (1921)•1930: a Lübeck catastrophy: the significance of virulent/
avirulens strains, not interchangeable•1930: introduction of tbc screening programs,epidemy decr ease•1945: WW II: epidemy increase•1950-1980: significant decreasing•1992: WHO Tbc: global problem•2000: WHO AIDS – Malaria – TBC GLOBAL EMERGENCY


Famous people who have had tuberculosis :Calvin
Anton ChehovBranwell Bronté
Emily BrontéFrédéric Chopin
DescartesJohn Keats
D.H. LawrenceVivien Leigh
Nelson MandelaMoliere
George OrwellPaganini
Edgar Allan PoeRichelieu cardinal
SchillerJean J. RousseauSir Walter Scott
P.B.ShellySpinoza
R.L. StevensonDesmond Tutu
Simonetta VespucciMargaret Gardner (a former Ms. World)

EPIDEMIOLOGY : TB Incidence 2001
25 - 49
50 - 99
100 - 299
< 10
10 - 24
per 100 000 pop
> 300
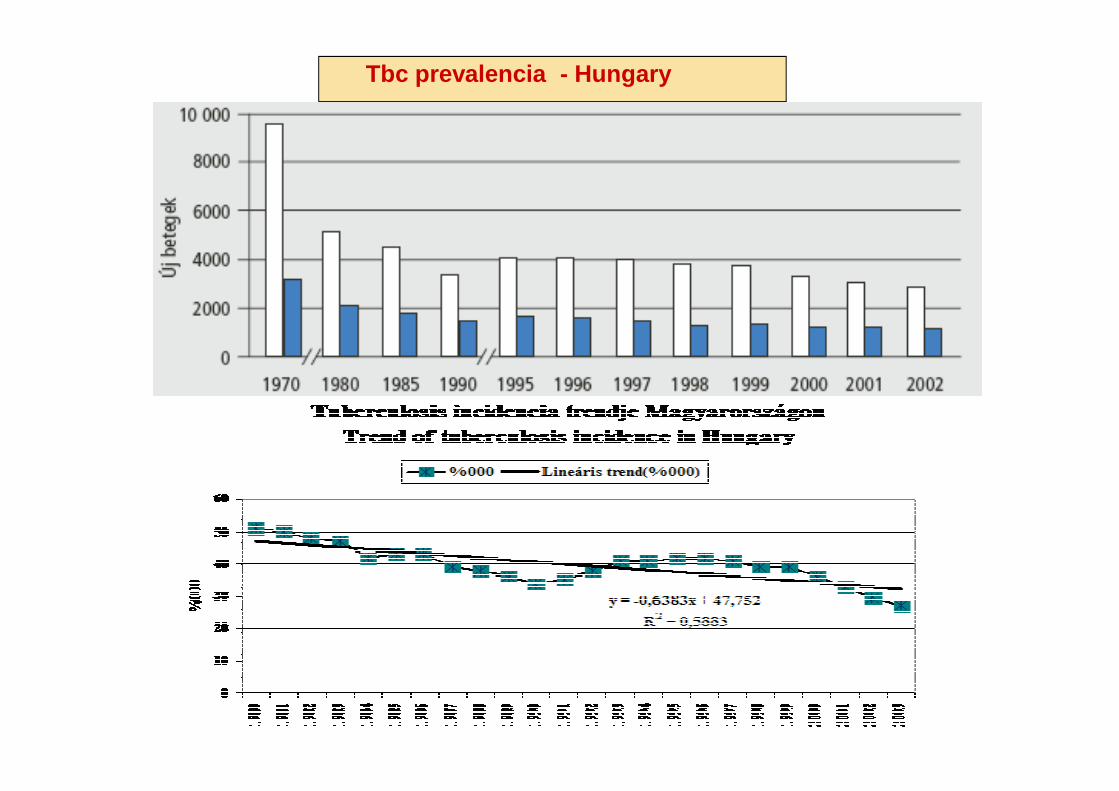
Tbc prevalencia - Hungary

Tbc split by gender and age
MALES FEMALS
RISK FACTORS
HOMLESS
DIRCT CONTACT
IMMIGRANT
LONELY

„Frigyes Korányi” National TBC and Pulmonological Institute

INCIDENCE OF TUBERCULOSIS• TB is responsible for 25% of adult deaths in the developing world- more than those caused
by diarrhea, malaria and AIDS combined • South Africa has one of the highest incidences: >200/100 000 • 35 people die of TB every day in South Africa • The incidence in the 'first world' is less than 10/100 000
THE GLOBAL EMERGENCY1. 8-12 million new infections with M. tuberculosis per year 2. 2-3 million people die from TB per year 3. If present trends continue, deaths will exceed 4 million by 2004 4. There is also the emergence of multi-drug resistant M. tuberculosis5. These trends, and the association of TB with HIV infection, has led to TB being declared
A GLOBAL EMERGENCYby the World Health Organization(1993)


Laboratory diagnosis
The basics of the effective treatment of tbc: early, rapid and accurate diagnosis
Microscopy od stained smear Isolation, culture
sensitivity104 bacterium/ml 102 bacterium/ml
low sensitivity long culture time: 4-8 hétCytocentrifuge (Sauton – and Dubos media )

Laboratory diagnosis
BacTec automats : radioactive palmitinic acid/CO2fluorescent detectionturbidityother color reaction
Rapid growth detection4-14 nap
Biosensors:
Molecular detection : PCR, LCRRFPL, DNA typing, DNS-chipDrug sensitivity/ resistancedetermination( hours, 1-2 days)
< 1 h

Atypical and apathogenic mycobacteria
M. avium-intracellulare, M. kansasi , M. scrofulaceu mM. smegmatis, M. phlei, stb
induce mycobacteriosises
characteristics : occurrence in the naturefaster growthpigment formationniacin negativitydifferent drug resistancymember of the normal flora
disease: local (skin, lung, lymphnodes, etc.) processesno transmission from human to human,nozokomial infectionsgeneralized in AIDS

THERAPY
• Stop infectivity• Inhibit drug resistance• Prevent remission of infection• Goal : complete recovery
Combination treatment, long time (6 -12 month) treatmentInitial, intense phase:
3 -4 anti tuberculotics against extracellular bacteriaStabilisation phase:
fewer drugs against intracellular, slow growing bacteria
INH (isonikotinic acid hidrazid ) - Rifampicin - PirazinamidEthambutol (AIDS, extrapulmonal tbc, meningitis)Ciprofloxacin,ethionamid,cycloserin (Multiresistant M.tbc)Clarithromycin,rifampicin,etambutol,clofazimin (M. avium-intracellulare)Doxicyclin ( M. fortuitum-chelonei)
Multiresistant strains !TBC – AIDS coinfections

PREVENTION
2. Vaccina : BCG inoculationM.bovis live, attenuated strain BCG (Bacillus Calmette-Guerin)2 - 42 day after birth, partial resistency
3. Chemoprofilaxis:
INH monotherapy , Rifampicin (min. 6 month)
1. Prevention of infection:General hygienic rulesEffective treatment of those infectedEradication of infected cattles

Induces lepra (Hansen disease) , does not grow in media or cell culture, Only in mouse sole and in armadillo. Aerob, pálcika alakú, saválló baktérium : Ziehl – Neelsen festésLaboratory diagnosis : from skin disorders, nose mucosaSyphilis serological reactions are fals posistive in lepra

The bacteria grow intracellularly in skin histiocytes, endothel cells and superficialnerves (Schwann-cells) . Optimal temperature: 30 C°
Tuberculoid lepra: normal cellular immunity,
few bacteria growing,
giant cells in granulomas
Lepromin skin tests: positive
Lepromatic lepra: immune response towards M.leprae is weak
skin, mucosa : large number of bacteria (histiocyt es)
Lepromin skin test: negative
Immune response to only M.leprae is defective,
cellular and humoral immune response towards other
microorganisms are intact
Antibodies are not protective

Macular skin disorders:Insensibility ulcer
Long incubation time: 10-15 year ! Gradual disease formation

Nodular skin disorders: „ lion face” (facies leontina)

Fingers, extremitiesexposed to amputation
because trophicalDisorders,
resorption of bonesresulting in
loss of nose cartilagsor digits






Boswelia carteri (Tömjénfa)„Salai guggul”
Dapson (sulfonamid residue)Rifampin (inhibitor of bacterial RNS synthesisClofazimin

Nocardia genusNocardia genusObligate aerob, Gram positive, moderate acid fast , filamental bacteria
Occurrence : widespread, soil, water
Domestic animals, dogs, cows (natural hosts)
In Humans: N.asteroides N. braziliensis
Nocardiosis: chronic, lobular pneumonia, miliary tbc-like
fever, weigh loss, chest pain. Lung abscess, haematogen
dissemination:central nerve system abscesses
Mycetoma: abscess in hand, leg, s.cutan connecting tissues
Laboratory diagnosis : sputum, pus, liquor smearsGram- and acid fast staining
Treatment: Surgical removaltrimetoprimsulfonamids

ActinomycesActinomycesAnaerobic, no spores, Gram positive, irregular shape rods
Actinomyces israelii: non obligate anaerobic, slow growth (7-10 days)

ActinomycosisActinomycosis
Gram positive
Gram negative
Actinomyces mycelium
Pathogenesis : 2 -3 mm, yellow granules (mycelia) consisting of the bacterial bodies

ActinomycosisActinomycosisPathogenesis : typical endogenous infection. Caries teeth, pharyngeal lavage, intestines, Vaginal floraPathogenic process is initiated by: trauma, pyogenic infections, i.u. contraceptive devices
ABSCESS FISTULA DRAINING OF PUS
Lung actinomycosis
Pelvic inflammation
SKINactinomycosis
Therapy:• Surgical removal• Penicillin• sulfonamids








