
`
Mobile Moms/Liga Inan: Improving Quality and Access to Maternal Care in Timor-Leste
September 30 2016
Grantee: Health Alliance International Grant Number: AID-OAA-A-11-00057 Start Date: October 1, 2011 End Date: June 29, 2016
Authors: Susan Thompson
Mary Anne Mercer

1
Table of Contents INTRODUCTION ........................................................................................................................... 2
Broad Issues ........................................................................................................................... 2 Specific Problem and Research Setting ................................................................................. 3 Research Justification ............................................................................................................ 3 Formative & Evaluative Research Questions ......................................................................... 4
METHODS .................................................................................................................................... 7 Study Design........................................................................................................................... 7 Participants ............................................................................................................................ 7 IRB Approval and Informed Consent ..................................................................................... 8 Study Duration ....................................................................................................................... 8 Intervention ........................................................................................................................... 8 Intervention Monitoring ...................................................................................................... 10 Outcomes Variables ............................................................................................................. 10 Data Collection and Analysis ................................................................................................ 12
RESULTS ..................................................................................................................................... 14 Intervention Monitoring ...................................................................................................... 14 Equivalence of Groups and Demographic Characteristics ................................................... 15 Main Results ......................................................................................................................... 15
DISCUSSION & RECOMMENDATIONS ...................................................................................... 19 Main Conclusions ................................................................................................................. 19 Brief Summary of Evidence .................................................................................................. 28 Limitations of the Study ....................................................................................................... 29 Comparison of Results with Other Research ....................................................................... 29 Immediate Intervention Uptake .......................................................................................... 30 Implications of the Results ................................................................................................... 30
ANNEXES
Annex 1: Basic Emergency Obstetric and Neonatal Care Assessment 2012 Annex 2: Liga Inan Telephone Survey Report 2012 Annex 3: HAI 2012 Baseline KPC Report Annex 4: 2015 Final KPC Data Tables

2
INTRODUCTION
Broad Issues
Community knowledge and practices of optimal health behaviors during pregnancy, delivery and the postpartum period, such adequate care seeking behavior, good nutrition including iron supplementation, knowledge of danger signs, and immediate breastfeeding are limited in Timor-Leste. Contact with midwives during pregnancy typically includes only a few antenatal (ANC) visits, which do not allow for the repetition and reinforcement of health messages that are likely to produce behavior change that could improve pregnancy and birth outcomes.
Given the difficult road access and isolation that many pregnant women face in largely rural Timor-Leste, mobile phones are increasingly becoming an important lifeline. Like many other developing countries, Timor-Leste is skipping the fixed-line telephone infrastructure and moving directly into the use of rapidly growing mobile phone technology. In 2003, only 2% of households reported owning a mobile phone.1 By 2010, ownership had increased to between 54-61%.2,3 Health Alliance International’s (HAI) 2015 final Knowledge, Practice and Coverage (KPC) survey found that 96% of households in the intervention district of Manufahi, and 85% in the control district of Ainaro reported owning a mobile phone. Additionally, 79% of women reported being literate in the local Tetun language, and of women who reported owning a phone, 75% reported sending and/or receiving daily or weekly text messages.4
Specific Problem and Research Setting
Maternal and newborn mortality continue to be major problems in Timor-Leste: the last Demographic and Health Survey in 2009/10 reported the maternal mortality ratio (MMR) to be 557 per 100,000 live births and neonatal mortality at 22/1000 live births.5 After Timor-Leste gained independence from Indonesia in 1999, the new government declared universal free access to health care. Although there has been progress in increasing the rates of skilled birth attendance (SBA) since independence, several challenges continue to affect the capacity of the government health system to provide women with high quality skilled care at the time of delivery, particularly when complications arise. Additionally, there are significant disparities in accessing maternal services for women living in the most rural areas of Timor-Leste. For
1 Ministry of Health and National Statistics Office, Timor-Leste, University of Newcastle, The Australian National University, ACIL Australia Pty Ltd. Timor-Leste 2003 Demographic and Health Survey. Newcastle, Australia: University of Newcastle; 2004. 2 National Statistics Directorate Timor-Leste and United Nations Population Fund (UNFPA). Population and Housing Census of Timor-Leste, 2010. Dili, Timor-Leste; 2010. 3 United Nations Integrated Mission in Timor-Leste (UNMIT). Timor-Leste Communication and Media Survey. Dili, Timor-Leste; 2011. 4 Health Alliance International. Maternal and Newborn Health and Mobile Phone Utilization in Manufahi and Ainaro Districts. Final Knowledge, Practices and Coverage Survey for the Mobile Moms/Liga Inan Program. 2015. 5 National Statistics Directorate [Timor-Leste], Ministry of Finance [Timor-Leste], and ICF Macro. 2010. Timor-Leste
Demographic and Health Survey 2009-10. Dili, Timor-Leste: NSD [Timor-Leste] and ICF Macro.

3
example, in 2010 only 21% of rural women had an SBA compared to 59% of women living in a more urban setting.6 Geographic access to delivery facilities is limited by gaps in both communication with and transportation to health facilities. Even with the provision of multifunctional vehicles (ambulances) at the sub-district level, many women do not access transportation to get to a health facility once in labor for a variety of reasons: the ambulances may be in disrepair or out of fuel; there is a family preference for a home delivery; the rainy season makes transportation options to some areas very challenging; and activating the emergency transport system can require too much time (e.g., family members are sent on foot to health facilities in order to dispatch the ambulance).
In HAI’s project area, 2012 baseline data from the KPC survey showed that rates of at least one ANC visit were high at 92% in Manufahi and Ainaro districts, but this rate decreased to 76% and 67% respectively for the recommended four or more ANC visits. Forty-eight percent (48%) of women in Manufahi and 38% in Ainaro delivered with a skilled birth attendant in 2012, and delivery in a health facility was low in both districts at 32% in Manufahi and 29% Ainaro.7
Research Justification
In Timor-Leste, gaps in the ability of the health care system to effectively reach pregnant women have been constrained by lack of access to information and care. Even with the recommended four ANC visits, opportunities are limited to provide and reinforce messages about behaviors that will help women assure a healthy pregnancy and delivery. The use of skilled birth attendants is also constrained by the inability of women to alert midwives in a timely fashion at the onset of labor. The use of mobile phone technology to target individual pregnant women with time-appropriate messages about behaviors she and her family can act upon to improve her health and the health of her baby had not been attempted in Timor-Leste prior to the Liga Inan program. Rapid growth in mobile phone ownership provides the opportunity to test the use mobile phone technology to communicate health messages and connect pregnant women to their health provider. The use of mobile phone technologies to support health programs in low resource settings is growing; however, there is a dearth of published data evaluating the impact of these approaches as well as their sustainability and scalability. The World Health Organization has urged organizations implementing mHealth programs to take seriously the need to evaluate their feasibility, best practices, results and cost-effectiveness.8 HAI conducted research to test the use of mobile phone technology to:
Assess the feasibility in Timor-Leste of sending and receiving SMS messages as part of a maternal/newborn health promotion effort.
Improve pregnant women’s knowledge about pregnancy related health.
6 Ibid. 7 Health Alliance International. Maternal and Newborn Health and Mobile Phone Utilization in Manufahi and Ainaro Districts.
Baseline Knowledge, Practices and Coverage Survey for the Mobile Moms/Liga Inan Program. 2012. 8 mHealth: New horizons for health through mobile technologies: second global survey on eHealth. WHO, Geneva, 2011.

4
Increase utilization of maternal health services, specifically the four recommended antenatal care visits (ANC 4), SBA, facility delivery, and postpartum and newborn care.
Assess the impact of an mHealth program with district-level health staff charged with implementing the program.
Assess the feasibility, sustainability and scalability of an mHealth program, specifically related to integration into the government-run health system.
HAI designed a research plan to evaluate the impact of the Liga Inan program. The research design included intervention and control districts where baseline (2012) and final (2015) Knowledge, Practice and Coverage (KPC) surveys comparing pre- and post-intervention time periods were conducted. HAI was engaged in supporting a cadre of community health workers and providing refresher training in Basic Emergency Obstetric Care (BEmOC) and supportive supervision for midwives in both the intervention and control districts. However, the Liga Inan mHealth intervention was implemented only in Manufahi District; Ainaro District served as the control site where Liga Inan was not implemented. Figure 1: Map of Timor-Leste with Liga Inan program districts highlighted
Formative & Evaluative Research Questions
FORMATIVE RESEARCH
OBJECTIVE 1: To determine the feasibility in Timor-Leste of sending and receiving SMS messages as part of a health promotion effort.
Research Questions:
1. What proportion of households has access to or owns a cell phone? 2. Who in the household is in possession of the cell phone most of the time?

5
3. How frequently do women send and receive SMS messages? 4. How well can women read SMS messages? If they cannot, who could read one to them? 5. What is the best time of day and day of week for women to receive messages? 6. How do households typically charge their cell phones?
Data Source: HAI 2012 Baseline KPC Survey
OBJECTIVE 2: To determine the preparedness of health facilities in Ainaro and Manufahi to deliver high quality basic emergency obstetric care.
Research Questions
1. Which health facilities and maternities are prepared and equipped to deliver high quality BEmOC services? (a facility mapping)
2. Which health facilities have the consistent use of an ambulance or other emergency vehicle that can be used for transport of obstetric emergency cases? Of women in labor who have no other means of transport?
3. Which midwives have received BEmOC training? How long ago? Was there follow-up training? (mapping of midwife training)
4. What are the midwives’ current levels of skills in BEmOC? 5. How do midwives perceive the quality of care that is given to patients with obstetric
complications? 6. What problems do providers face in providing basic emergency care?
Data Source: Basic Emergency Obstetric and Neonatal Care Assessment in Manufahi and Ainaro Districts. A University of Washington graduate student thesis project 2012. EVALUATIVE RESEARCH
OBJECTIVE 3: To determine the success of messages in reaching the program enrollees.
Research Questions
1. Are SMS messages delivered to Liga Inan enrollees? 2. Do Liga Inan enrollees read the SMS messages? 3. If Liga Inan enrollees are illiterate do they find other family members or friends who
read the SMS messages to them? 4. Do Liga Inan enrollees share the messages with others
Data Source: A telephone survey among women enrolled in Liga Inan within the first 5 weeks following launch of the program in Manufahi District.

6
OBJECTIVE 4: To determine whether receiving regular SMS messages that encourage healthy maternal behaviors is associated with significant improvement in maternal health knowledge and behaviors for women enrolled in Liga Inan (Manufahi district) compared to baseline rates and the control area (Ainaro District).
OBJECTIVE 5: To determine whether receiving regular SMS messages that encourage healthy maternal behaviors is associated with increases in use of MNC services for women enrolled in Liga Inan (Manufahi District) compared to baseline rates and the control area (Ainaro District).
Research Questions for Objectives 4 and 5 At the end of the two-year implementation period, among women with children between the ages of 0-23 months, has there been a significant increase in the percent of women who:
know 2 or more danger signs associated with pregnancy, delivery, postpartum and newborns?
put their infant to breast within an hour of delivery?
had four or more antenatal care visits before the birth of their last child?
received assistance from a skilled birth attendant during delivery of their last child?
delivered their last child in a health facility?
received a postpartum (mother) within two days of their last delivery?
received a postnatal (newborn) within two days of their last delivery?
received two tetanus vaccinations before the birth of their youngest child
took iron folate supplementation during their last pregnancy
took antiparasite drugs during pregnancy?
know the optimum birth spacing interval?
use a modern method of contraception after the birth of their last child? Data Source: HAI 2012 Baseline and 2015 Final KPC survey
OBJECTIVE 6: To determine the feasibility of implementing, maintaining and expanding a mobile phone technology program.*
Research questions
1. Was a successful mHealth platform developed? What were the main challenges in developing the Liga Inan technology software, website and server platform? Describe technological problems that occurred and how they were resolved.
2. What was the role of community members and stakeholders in implementation? Was there an important community champion?
3. To what extent did Ministry of Health (MoH) district health staff become engaged and maintain engagement in Liga Inan over the course of the program?
4. What was the engagement of mobile network service providers in Timor-Leste with the Liga Inan program?
5. Has the policy environment for an mHealth program improved in Timor-Leste?

7
*Objective 6 was part of our original OR concept paper. The research questions under Objective 6 were meant to be the focus of an external, independent evaluation that HAI was responsible to deliver as part of our USAID Cooperative Agreement. However, in mid-2015 the MoH informed partners that they intended to carry out their own independent evaluation of the Liga Inan program and requested the Australian Government (DFAT) to financially support this effort. When HAI learned of the MoH intentions we began discussions with USAID and DFAT in order to avoid duplication of efforts. The end result was that HAI maintained control over conducting a final KPC survey, but relinquished the overall program evaluation to the MoH. We agreed to share KPC findings with the MoH research team. In addition, HAI financially supported a consultancy to provide capacity building for the MoH research team to design a research plan and interview tools to carry out their evaluation. USAID gave approval to accept the MoH evaluation report in lieu of HAI submitting a Final Program Evaluation Report and recognized that HAI does not have control over the quality of the evaluation or when a written report will be completed. As of September 1, 2016 a final written report is available in the local Tetum language and is in process of translation into English.
METHODS
Study Design
Objective 1: The study design was cross-sectional using data from the baseline Knowledge, Practice and Coverage (KPC) survey. Objective 2: A mixed methods study design was employed to conduct a BEmOC Facility assessment using both quantitative and qualitative tools to assess the level of preparedness of facilities and health staff capacity to deliver BEmOC services in both Ainaro and Manufahi Districts. Objective 3: A post-test only study design was used by conducting a telephone survey with randomly selected women enrolled in the Liga Inan program within the first five weeks after launch of Liga Inan in the first sub-district of the intervention district. Objectives 4 & 5: A quasi-experimental pretest-posttest study design was employed using data from the KPC survey in both an intervention and control group.
Participants
Objectives 1, 4, and 5: KPC surveys – Women age 15-49 who have a child age 0-24 months living in Manufahi and Ainaro districts. Objective 2: BEmOC Assessment – Midwives and other health staff working at Community Health Centers in each subdistrict in Manufahi and Ainaro districts. Objective 3: Telephone survey – Women who are enrolled in the Liga Inan program within the first five weeks following launch in each of the four sub-districts in Manufahi.

8
IRB Approval and Informed Consent
Objectives 1, 4, and 5: An application for ethical review was submitted and approved by the Institutional Review Board (IRB) at the University of Washington for the baseline and final KPC surveys. The research was also presented to the National Health Training Institute, which functions as the ethnical review board in Timor-Leste and was given approval. Oral informed consent was obtained from all KPC survey participants. Objective 2: The BEmOC Facility Assessment was carried out with the full engagement and approval of the Timor-Leste Ministry of Health to assess the preparedness of health facilities and the capacity of health staff to deliver BEoMC services, and was reported back to the MoH. It was determined that an IRB was not required. Individual oral consent was obtained by health staff participating in questionnaire and interviews. Objective 3: It was determined that as a program evaluation using telephone surveys to evaluate the success of messages in reaching the program enrollees, an IRB review was not required. Oral informed consent was obtained from everyone interviewed in the study.
Study Duration
Objectives 1, 4, & 5: The baseline KPC survey was conducted in Manufahi and Ainaro Districts over a period of one month in Feb/March 2012 and was followed by a one-year period of development of the Liga Inan service, stakeholder engagement and health staff training. Enrolling of pregnant women into the Liga Inan program began Manufahi in March 2013 in one sub-district, in two additional sub-districts in August 2013 and in the final sub-district in October 2013. The final KPC survey was conducted in both Manufahi and Ainaro Districts over a one-month period in Sept/Oct 2015 after at least 24 months of Liga Inan program implementation in all four sub-districts in Manufahi. The total study period was 43 months from the time of the baseline to the final survey. Objective 2: The BEmOC Facility Assessment was conducted over 8 weeks in January and February 2012 in Manufahi and Ainaro Districts. Objective 3: The telephone survey was conducted for a period of about two weeks in April 2013 approximately 5 weeks after the initial launch of the Liga Inan in the sub-district of Same in Manufahi District.
Intervention
In both the intervention and the control districts HAI implemented conventional health interventions: 1) training of community health workers to deliver maternal health education during home visits with pregnant women, and 2) providing Basic Emergency Obstetric Care refresher training for midwives and supportive supervision for district midwives. In Manufahi, the intervention district, the mobile phone technology innovation, Liga Inan, was added with the hypotheses that women provided with health information and increased communication with midwives would be more likely than women in the control district to: 1) have increased

9
maternal health knowledge and adopt recommended home care behaviors, and 2) seek assistance from a health care provider before, during and after delivery. The key functions of the Liga Inan program are:
1. Registration: Pregnant women are registered into the Liga Inan service by their health staff, usually a midwife using the mother’s mobile phone number at her first ANC visit.
2. SMS (text) messages: Pregnant women receive twice weekly SMS messages with health information, tips and reminders, and cues to action relevant to their stage of pregnancy. The messages continued for six weeks postpartum.
3. Community messages: Health staff can send SMS announcements to all pregnant
women registered in their catchment area, such as changes to clinic hours or reminders
about outreach health services.
4. Liga Hau (Call me): Pregnant women who have questions or concerns can use this
function to request a call from health staff.
5. Follow-up: Health staff are prompted by the Liga Inan service to call all pregnant women
three weeks before their estimated due date to check on the families’ preparation and
planning for delivery.
6. Emergency: Pregnant women can find emergency telephone contact information on a
sticker placed in their mother and child booklet by health staff during Liga Inan
registration.
All midwives and some doctors in the intervention district received a 3-day Liga Inan training conducted by HAI and Catalpa staff. The training covers: 1) how to register pregnant women into the program, 2) how to use the functions of the Liga Inan service, 3) review of estimating due dates, 3) effective communication and how to promote Liga Inan, 4) how to follow up with pregnant women when triggered by the Liga Inan service, and 5) review of appropriate telephone triage and referral practices. Clinic managers also participated in the training, as they play a key role in mobilizing emergency transport and managing health staff to ensure that the program runs smoothly. Health facilities are provided with one smart phone and each active health staff engaged in enrolling women into Liga Inan receive a $10 monthly phone credit to support the calls they are expected to make when prompted by the service. HAI staff provide remote and on-site technical support to implementers and managers; the technical service that drives automated delivery of Liga Inan messages was designed and managed by Catalpa International under a sub-contract with HAI as part of our grant.
Table 1: Comparison of Intervention and Control Groups INTERVENTION INTERVENTION GROUP
(MANUFAHI DISTRICT)
CONTROL GROUP
(AINARO DISTRICT)
Train Community Health Workers to carry out home visits with pregnant women
Yes Yes
BEmOC Refresher Training and Supportive Supervision for Midwives
Yes Yes
Mobile Phone Component -health staff training
Yes No

10
-pregnant women registered -follow-up Liga Inan technical support -provision of smart phone & phone credit
Intervention Monitoring HAI provided support to a cadre of MoH-sponsored community health workers and supported refresher training in BEmOC and conducted supportive supervision for midwives in Manufahi and Ainaro districts. Careful attention was paid and records maintained to assure that these interventions were equally implemented across the intervention and control districts during the first two years of the study period. The Liga Inan mHealth intervention was implemented only in Manufahi District; Ainaro District served as the control district where Liga Inan was not implemented. A variety of methods were used to monitor the Liga Inan program:
HAI staff who were 100% dedicated to the program were based in the intervention district.
Catalpa designed and developed a data dashboard that collects real time data that was used to monitor a variety of data points of interest:
o Enrollment data by district, sub-district and health facility o Number and content of every SMS sent to enrollees o Number and content of Liga Hau, or “Call me” messages sent by enrollees o Number and content of broadcast messages sent by midwives to enrolled
women o Number of babies born to enrolled women and place of delivery – home or
facility o Number of opt out requests
Routinely collected HMIS for key maternal indicators: o Antenatal 1 and 4 o Skilled birth attendance at home and at a health facility o Postpartum and postnatal care visits
A telephone survey
Outcome Variables Objectives 1:
% of households reporting ownership of a mobile phone
% women who report they own their own mobile phone
% women who report sending SMS messages and frequency (daily, weekly, monthly)
% women who can read the local Tetum language
% women who report preferred time to receive a SMS message in morning, afternoon, or evening
% households using specific methods to their mobile phones
11
Objective 2:
% health staff who are BEmOC certified
% health staff who BEmOC signal functions in the last three months
% health staff who performed 45 obstetric skills in the last six months and if the health provider felt confident in performing that function
% health facilities where basic BEmOC equipment and supplies were available Objective 3:
% women enrolled in Liga Inan who reported receiving a message within the two weeks prior to the telephone interview
% women who reported reading and understanding Liga Inan messages they received.
% women who could recall a Liga Inan message they received.
% women who reported they required help to read the Liga Inan messages.
% women who reported that they shared a Liga Inan message with someone. Objectives 4 and 5: Enrollment Indicators
% women enrolled in program by district and sub-district (2015)
Main Health Service Utilization Indicators
% women with at least 1 ANC visit
% women with 4 or more ANC visits
% women with a skilled birth attendant at delivery (whether at home or in a facility)
% women who deliver in a health facility
% of women who received a postpartum visit within 2 days of delivery
% of newborns who received a postnatal visit within 2 days of delivery
% women who received tetanus toxoid vaccinations during their last pregnancy
% of women who received iron tablets
% women who took intestinal parasite drug during their last pregnancy
% of women who are currently using a modern method of contraception
Knowledge Indicators
% of women who know two or more danger signs of pregnancy
% of women who know two or more danger signs of delivery
% of women who know two or more danger signs of the postpartum period
% of women who know two or more danger signs of the newborn period
% of women who know that they should wait at least 24 months after delivery before
getting pregnant again
Home Care Behaviors Indicators
% of women who took 90 iron tablets or more
% of newborns who were put to the breast within one hour after delivery

12
Data Collection and Analysis Objectives 1, 4, and 5: A baseline and final household survey of women age 15-49 who had a child age 0-24 months using an 8 by 9 cluster sample was conducted in the intervention and control districts. The aim of this research was to determine whether participation in the Liga Inan program was associated with significant improvements in use of maternal health services and knowledge compared to women in the intervention district at baseline and to women in the control district of Ainaro while controlling for other significant factors. Our main independent or predictor variable in the multivariate model statistically combined those two variables of time (pre/post) and district (intervention/control) in an interaction variable called “timeXtreat.” This variable is also known as the difference in difference estimator, which is defined as the difference in average outcome in the intervention group before and after the intervention minus the difference in average outcome in the control group before and after the intervention. Households were randomly selected for participation using a spin the bottle method (with two ends of the water bottle indicating the directions for the interview pairs to follow). To determine sample size for the KPC survey, we used calculations for community clustered trials using a post-only design9, knowing that this will give us conservative sample size estimates and the pre-intervention measurements will increase power. Multivariate analysis was used to assess the extent to which potential exposure to the mHealth intervention in Manufahi District after the launch of the mobile phone program predicted improved maternal health knowledge and behaviors, such as utilization of health services, when compared to the pre-intervention time period and to those same outcomes in the control area, Ainaro District. Analysis was by ‘intention to treat,’ meaning that the entire population of women who gave birth in Manufahi during the intervention period was assessed for changes, not only women who were enrolled in the program.
To assess these effects, we used multilevel mixed-effects logistic regression models separately for each knowledge and behavior outcome with a dichotomous response. The unit of analysis was the individual woman’s survey responses. The predictor of interest was the intervention delivered at the district level, where the outcome was women’s maternal health knowledge or behavior as measured both at the pre- (baseline KPC) and post-intervention (final KPC) periods. We adjusted for sub-district clustering of measurements by using random effects at the sub-district level in all models. Control variables considered in these models included age group (15-24, 25-29, 30-34, and 35+ years), years of education, and minutes of travel time to a health facility. For postpartum, postnatal, and early initiation of breastfeeding we added skilled birth attendance as a control variable.
9 RJ Hayes and S Bennet. Simple sample size calculation for cluster-randomized trials. International Journal of
Epidemiology (1999) 28 (2): 319-326.

13
For the logistic regression models, odds ratios were used to show the treatment effect (i.e., “timeXtreat,” which is equivalent to the difference in the odds of the outcome in the intervention group before and after the intervention minus the difference in the odds of the outcome in the control group before and after the intervention. In other words, odds ratios in these results indicate that a given effect of the intervention for women in Manufahi is x times greater than the same indicator in Ainaro before and after the intervention. Objective 2: A mixed methods approach was employed using a Ministry of Health-approved UNFPA questionnaire to access staff certification for BEoMC, staff BEmOC knowledge levels, and equipment, supplies and drug availability. Qualitative investigation explored health staff perceptions on barriers to providing BEmOC, quality of home delivery assistance and early complication identification and care. All health facilities in the intervention and control districts were part of this assessment. Qualitative data was compiled and analyzed using an Excel database; quantitative data was compiled, tallied and analyzed using an Excel database. Objective 3: Fifty enrolled women were randomly selected from the Liga Inan database and called to participate in a short questionnaire over the telephone. All surveyed women were from the sub-district of Same, the first sub-district to receive the Liga Inan program, and were sampled proportionate to the number of enrollments per village as tracked on the Liga Inan data dashboard. The purpose of the telephone survey was an early assessment if enrolled women were receiving, opening, reading, understanding and sharing the Liga Inan text messages. The 10 question survey was administered over the phone by HAI staff; data was entered into an Excel database, tallied and analyzed. Table 2: Summary of Data Collection Methods
DATA COLLECTION METHOD
WHEN ADMINISTERED RESPONDENTS SAMPLE SIZE
Liga Inan Data Dashboard
Live in March 2013 (continuous real time data collection dashboard)
Women enrolled into the Liga Inan program
continuous
KPC Household Survey Baseline (Feb/March 2012) Women age 15-49 with a child age 0-24 months
581
KPC Household Survey Final (Sept/Oct 2015) Women age 15-49 with a child age 0-24 months
576
Telephone Survey April 2013 Women enrolled in the Liga Inan program in the sub-district of Same within three months of enrollment
50
BEoMC Assessment January – March 2012 Midwives working in 8 health facilities in Manufahi and Ainaro Districts
17 midwives 7 health facilities

14
RESULTS
Intervention Monitoring HAI approached monitoring the Liga Inan program in a variety of ways as described below. HAI staff dedicated to the Liga Inan program. HAI opened a regional office with staff dedicated to the Liga Inan program who performed the following activities:
Conducted advocacy meetings with health staff and community in all four sub-districts where Liga Inan was implemented
Conducted 3-day training workshops for health staff in all four sub-districts to train on how to register women into the program and interfacing with the Liga Inan service
Provided onsite trouble shooting when problems arose, such as difficulties registering women, using the Liga Inan features, problems with the smart phones provided to health facilities, etc.
Assisted the HAI Communication Specialist to field test the Liga Inan SMS messages
Assisted the HAI M&E Manager to collect HMIS data
Coordinated district level meetings to report out on program successes and challenges Routinely collected HMIS data. The MoH routinely collects HMIS data on key Liga Inan outcomes. HAI has been given permission from the MoH to access HMIS data. Data is disaggregated and analyzed at the sub-district level to monitor the Liga Inan and other programs. We looked at key indicators for which we had high confidence in data quality for the 12-month time period pre-launch of Liga Inan and the 12-months post-launch to monitor progress on uptake of maternal health services. Key indicators monitored were:
ANC 1
ANC 4
Total SBA (whether at home or in a facility)
Facility Delivery
PPC
PNC Liga Inan data dashboard. Catalpa developed a Liga Inan website (www.ligainan.org) and created a password protected link through this website to a data dashboard that collects real time data on a number of data points of interest to monitor the program. HAI in our regional office in Manufahi, in our Dili office in Timor-Leste and our HQ office in Seattle can access the dashboard to monitor the program on the following data points:
Enrollment data by district, sub-district and health facility
Number and content of every SMS sent to enrollees
Number and content of Liga Hau, or “Call me” messages sent by enrollees
Number and content of broadcast messages sent by midwives to enrolled women
Number of babies born to enrolled women and place of delivery – home or facility
15
Number of opt out requests Telephone survey. Shortly after Liga Inan was launched in the first sub-district, HAI conducted a telephone survey of 50 randomly selected women enrolled in the program to ascertain if SMS messages were received, read, understood, recalled and shared.
Equivalence of Groups and Demographic Characteristics
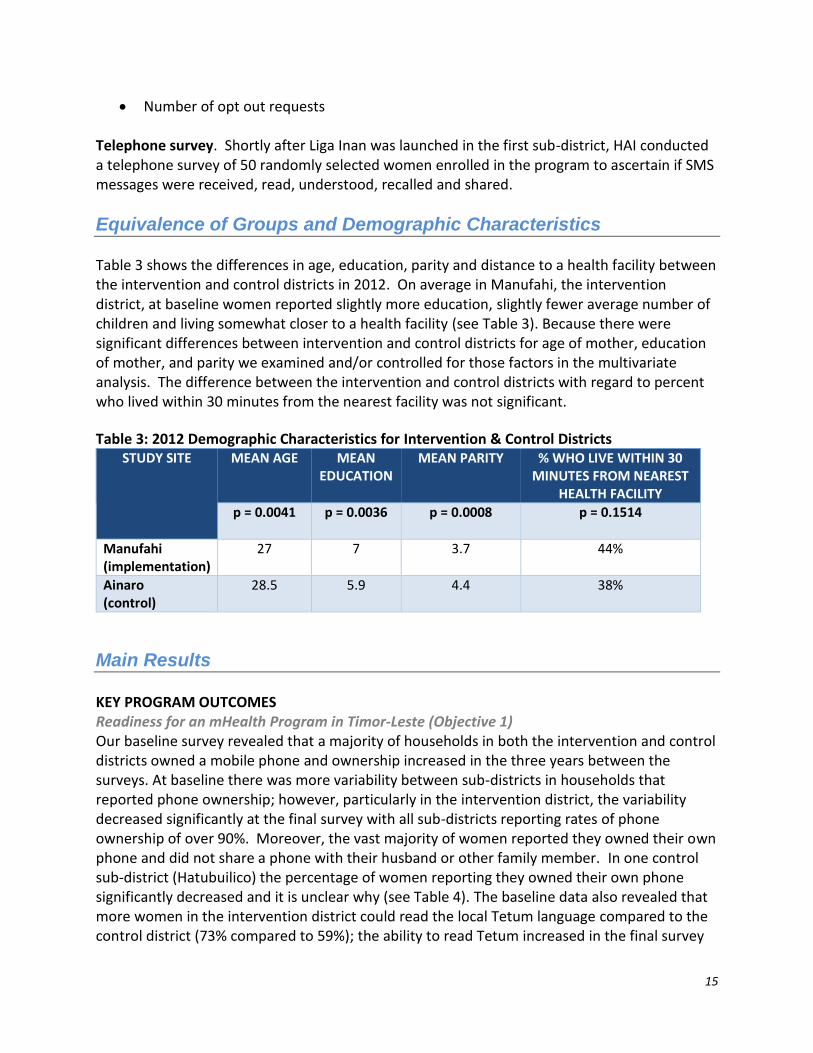
Table 3 shows the differences in age, education, parity and distance to a health facility between the intervention and control districts in 2012. On average in Manufahi, the intervention district, at baseline women reported slightly more education, slightly fewer average number of children and living somewhat closer to a health facility (see Table 3). Because there were significant differences between intervention and control districts for age of mother, education of mother, and parity we examined and/or controlled for those factors in the multivariate analysis. The difference between the intervention and control districts with regard to percent who lived within 30 minutes from the nearest facility was not significant.
Table 3: 2012 Demographic Characteristics for Intervention & Control Districts STUDY SITE MEAN AGE MEAN
EDUCATION MEAN PARITY % WHO LIVE WITHIN 30
MINUTES FROM NEAREST HEALTH FACILITY
p = 0.0041
p = 0.0036
p = 0.0008
p = 0.1514
Manufahi (implementation)
27
7 3.7 44%
Ainaro (control)
28.5 5.9 4.4 38%
Main Results KEY PROGRAM OUTCOMES Readiness for an mHealth Program in Timor-Leste (Objective 1) Our baseline survey revealed that a majority of households in both the intervention and control districts owned a mobile phone and ownership increased in the three years between the surveys. At baseline there was more variability between sub-districts in households that reported phone ownership; however, particularly in the intervention district, the variability decreased significantly at the final survey with all sub-districts reporting rates of phone ownership of over 90%. Moreover, the vast majority of women reported they owned their own phone and did not share a phone with their husband or other family member. In one control sub-district (Hatubuilico) the percentage of women reporting they owned their own phone significantly decreased and it is unclear why (see Table 4). The baseline data also revealed that more women in the intervention district could read the local Tetum language compared to the control district (73% compared to 59%); the ability to read Tetum increased in the final survey
16
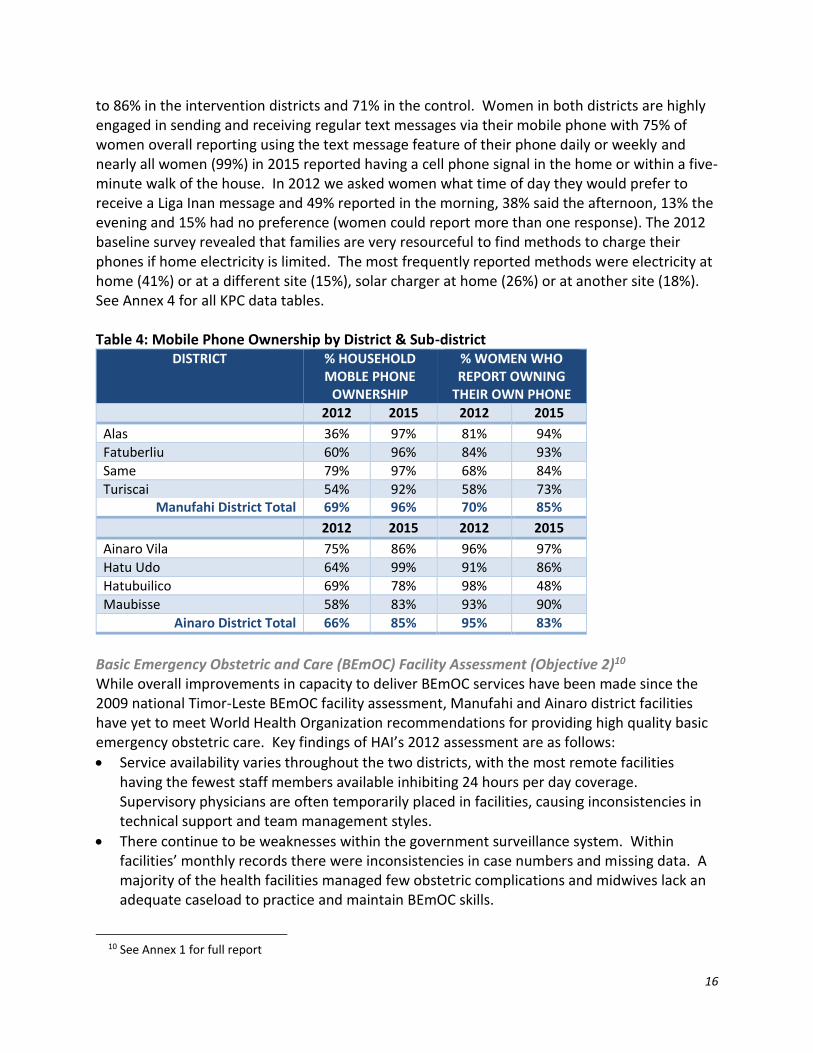
to 86% in the intervention districts and 71% in the control. Women in both districts are highly engaged in sending and receiving regular text messages via their mobile phone with 75% of women overall reporting using the text message feature of their phone daily or weekly and nearly all women (99%) in 2015 reported having a cell phone signal in the home or within a five-minute walk of the house. In 2012 we asked women what time of day they would prefer to receive a Liga Inan message and 49% reported in the morning, 38% said the afternoon, 13% the evening and 15% had no preference (women could report more than one response). The 2012 baseline survey revealed that families are very resourceful to find methods to charge their phones if home electricity is limited. The most frequently reported methods were electricity at home (41%) or at a different site (15%), solar charger at home (26%) or at another site (18%). See Annex 4 for all KPC data tables. Table 4: Mobile Phone Ownership by District & Sub-district
DISTRICT % HOUSEHOLD MOBLE PHONE
OWNERSHIP
% WOMEN WHO REPORT OWNING
THEIR OWN PHONE
2012 2015 2012 2015
Alas 36% 97% 81% 94%
Fatuberliu 60% 96% 84% 93%
Same 79% 97% 68% 84%
Turiscai 54% 92% 58% 73% Manufahi District Total 69% 96% 70% 85%
2012 2015 2012 2015
Ainaro Vila 75% 86% 96% 97%
Hatu Udo 64% 99% 91% 86%
Hatubuilico 69% 78% 98% 48%
Maubisse 58% 83% 93% 90%
Ainaro District Total 66% 85% 95% 83%
Basic Emergency Obstetric and Care (BEmOC) Facility Assessment (Objective 2)10 While overall improvements in capacity to deliver BEmOC services have been made since the 2009 national Timor-Leste BEmOC facility assessment, Manufahi and Ainaro district facilities have yet to meet World Health Organization recommendations for providing high quality basic emergency obstetric care. Key findings of HAI’s 2012 assessment are as follows:
Service availability varies throughout the two districts, with the most remote facilities having the fewest staff members available inhibiting 24 hours per day coverage. Supervisory physicians are often temporarily placed in facilities, causing inconsistencies in technical support and team management styles.
There continue to be weaknesses within the government surveillance system. Within facilities’ monthly records there were inconsistencies in case numbers and missing data. A majority of the health facilities managed few obstetric complications and midwives lack an adequate caseload to practice and maintain BEmOC skills.
10 See Annex 1 for full report

17
Other than the Maubisse Referral Hospital, midwives from the Prince of Monaco II Maternity House in Manufahi were the only interviewees who performed all BEmOC signal functions in the previous three months. Skill confidence varied across facilities, with some midwives acknowledging increased confidence with team care management approaches.
Equipment is not consistently available to provide high quality BEmOC. Basic equipment to monitor and detect early complications was missing from numerous facilities. Equipment to perform BEmOC function was missing or staff lacked knowledge on proper maintenance. At the time of assessment, medicines were well distributed, but staff admitted to experiencing frequent shortages.
Telephone Survey (Objective 3)11 Women interviewed as part of the telephone survey described positive experiences with the program: 96% of women reported they found the program easy to access and 94% were satisfied with the program. Participants found messages easy to understand and 71% of women said they were able to read messages independently. Results show that 65% of women recalled a message from the Liga Inan SMS message list and 35% of women discussed messages with others, exposing more people to key health advice. Although a majority of findings are positive, the survey also revealed the possibility that the program may not be reaching women as consistently as expected: women recalled receiving only 47% of the messages that were estimated to be sent during the previous month. Further investigation was necessary to determine whether this gap was due to recall bias, or to some other issue such as undelivered messages through the service provider, cell signal coverage, phones not being turned on for the entire week, or other user error. Enrollment in Liga Inan (Objectives 4 and 5) The rate of enrollment of pregnant women into the Liga Inan program in the intervention district of Manufahi was 70% of all surveyed women (n=288). Enrollment was high in all four sub-districts with the highest participation in the sub-district of Fatuberliu and lowest in the most rural and remote sub-district of Turiscai. Data analysis for women surveyed who were eligible to participate in Liga Inan, meaning they attended at least one ANC visit and had access to a mobile phone(n=186), showed higher rates of participation compared to all surveyed women (see Table 5).
11 See Annex 2 for full report

18
Table 5: Percent Enrollment in Liga Inan in Intervention District MANUFAHI DISTRICT % ENROLLMENT OF ALL
SURVEYED WOMEN (n=288)
% ENROLLMENT OF ELIGIBLE* SURVEYED WOMEN
(n=186)
Alas 68% 71%
Fatuberliu 79% 81%
Same 71% 78%
Turiscai 60% 70%
Manfuahi District Total 70% 77%
*owned a mobile phone and had ANC 1 Antenatal Care (Objectives 4 and 5) Women who reported receiving at least one ANC visit was high in both the intervention and control districts at baseline and remained high at the time of the final survey. Rates of four or more ANC visits, while higher overall in the intervention district at baseline and final, saw higher percent increases over the study period in the control district (see Table 5 for district results weighted for population size. Multivariate analysis did not show a significant association between the Liga Inan intervention and ANC use (Table 6 & 7). Skilled Birth Attendance & Facility Delivery (Objectives 4 and 5) The rate of SBA was somewhat higher in the intervention district at baseline, during the study period this rate significantly increased while no increase was observed in the control district. The rate of facility delivery was similar in both districts at baseline and increased in the intervention district over the study period with no gains observed in the control district. Multivariate analysis showed that women in the intervention district had nearly twice the odds of using an SBA (p= 0.027) and having a facility delivery (p= 0.025) compared to women in the control district (Table 6 & 7). We also analyzed if increased communication between mothers and health staff as facilitated by the Liga Inan program resulted in more women seeking SBA and a facility delivery. Among Liga Inan enrollees in Manufahi District (n=200) who were called by health staff three weeks prior to their estimated due date (n=101)12, 53% had a facility delivery compared to those who were not called (n=99) and had a facility delivery (32%). The Liga Inan service also facilitates mothers to contact health staff with a question or a concern. Among Liga Inan enrollees (n=200), who reported contacting health staff with a question or concern (n=141), 78% had a SBA compared to women who did not contact health staff (n=59) and had a skilled birth attendant. Postpartum & Postnatal Care Visits within Two Days (Objectives 4 and 5) At baseline the rate of postpartum care (PPC) for the mother within 2 days of delivery was higher in the control district. However, over the study period the rate nearly doubled in the intervention district and decreased in the control district. Similarly, the rate of postnatal care
12 The Liga Inan service sends a text message to health staff three weeks prior to an enrollees estimated due data that should trigger a call to check on the enrollees’ birth plan.

19
for the newborn in the intervention district nearly doubled between the 2012 and 2015 surveys while decreasing in the control district. Multivariate analysis showed that women in the intervention district had seven times the odds (p<0.001) of having a PPC visit within two days of delivery when compared to women in the control district; newborns in the intervention district had over five times the odds (p<0.001) of receiving a newborn care visit within two days of delivery (Table 6 & 7). Knowledge of Danger Signs during Pregnancy, Delivery, Postpartum and for the Newborn (Objectives 4 and 5) Across the board, with the exception of knowledge of newborn danger signs, there was a decrease in knowledge of danger signs (pregnancy, delivery, the postpartum period for mothers) in the final survey compared to baseline in both the intervention and the control districts. Multivariate analysis showed that there was no significant association between participation in the Liga Inan program and increased knowledge of danger signs (Table 6). Use of a Modern Method of Family Planning (Objectives 4 and 5) In the baseline survey the rate of women who reported using a modern method of family planning was over twice as high in the intervention district compared to the control district. During the study period there was an increase in the control district and virtually no change in the intervention district. Multivariate analysis showed that there was no significant association between participation in the Liga Inan program and the rate of use of a modern family planning method (Table 6). Tetanus Toxoid, Iron Tablets Received & Intestinal Parasite Medication (Objectives 4 and 5) Rates of tetanus toxoid vaccination during pregnancy decreased in both districts during the study period. The percent of women who reported they received iron tablets during their most recent pregnancy was high at baseline in both districts and decreased slightly between the two surveys. The provision of intestinal parasite medication during pregnancy is low in both the intervention and control districts, however, it was twice as high at baseline in the intervention district over the control district. During the study period the rate of intestinal parasite medication dropped by nearly half in the intervention district and increased slightly in the control district. Multivariate analysis was not conducted on these indicators (Table 6). Knowledge of Optimal Birth Interval (Objectives 4 and 5) At baseline in both the intervention and the control districts there were high rates of women who knew that they should wait at least 24 months between pregnancies. The rate increased more during the study period in the intervention district compared to the control district. Multivariate analysis was not conducted on this indicator (Table 6). Iron Tablet Consumption (Objectives 4 and 5) The rate of iron tablet consumption was exactly the same in the final survey for intervention and the control districts. However, during the study period the rate increased in the intervention district and decreased in the control district. However, multivariate analysis

20
showed that there was no significant association between participation in the Liga Inan program and increased consumption of iron tablets (Table 6 & 7). Immediate Breastfeeding (Objectives 4 and 5) There was a significant improvement in the rate of newborns who were put to the breast within one hour of birth in both intervention and the control districts during the study period and the rate of increase was nearly exactly the same between the two districts. Multivariate analysis showed that there was no significant association between participation in the Liga Inan program and early initiation of breastfeeding (Table 6 & 7).

18
Table 6: Program Results in the Intervention and Control Districts
VARIABLE Intervention Control
Enrollment Indicators Baseline13 Final14 Baseline Final
% household ownership of a mobile phone 69% 96% 66% 85%
% women who reported they own their “own” phone 70% 85% 95% 83%
% women who send text message once a day or more 77% 88% 67% 73%
% women who can read text message in the local language (Tetum) 73% 86% 59% 71%
% women who report having a cell phone signal at home or within 5 minute walk from house
95% 100% 99% 98%
Total number of pregnant women ever enrolled in Liga Inan n/a 3,287 n/a n/a
% women surveyed in intervention district who women enrolled in Liga Inan n/a 70% n/a n/a
% women with at least 1 ANC visit 93% 94% 91% 93%
% women with 4 or more ANC visits 76% 85% 67% 81%
% women who received tetanus toxoid vaccinations during their last pregnancy 85% 75% 74% 66%
% of women who received iron tablets 90% 94% 87% 93%
% women who took intestinal parasite drug during their last pregnancy 22% 14% 12% 16%
% women with a skilled birth attendant at delivery 48% 62% 38% 36%
% women who deliver in a health facility 32% 49% 29% 28%
% of women who received a postpartum visit within 2 days of delivery 26% 51% 38% 25%
% of newborns who received a postnatal visit within 2 days of delivery 20% 39% 32% 22%
% of women who are currently using a modern method of contraception 54% 55% 23% 32%
% of women who know two or more danger signs of pregnancy 54% 39% 55% 33%
% of women who know two or more danger signs of delivery 42% 27% 37% 32%
% of women who know two or more danger signs of the postpartum period 42% 35% 58% 33%
% of women who know two or more danger signs of the newborn period 42% 40% 37% 39%
% of women who know that they should wait at least 24 months after delivery before getting pregnant again
80% 91% 82% 85%
% of women who took 90 iron tablets or more 45% 57% 61% 57%
% of newborns who were put to the breast within one hour after delivery 51% 85% 60% 90%
13 See Annex 3 for all 2012 baseline KPC full report and data tables 14 See Annex 4 for all 2015 final KPC data tables
19
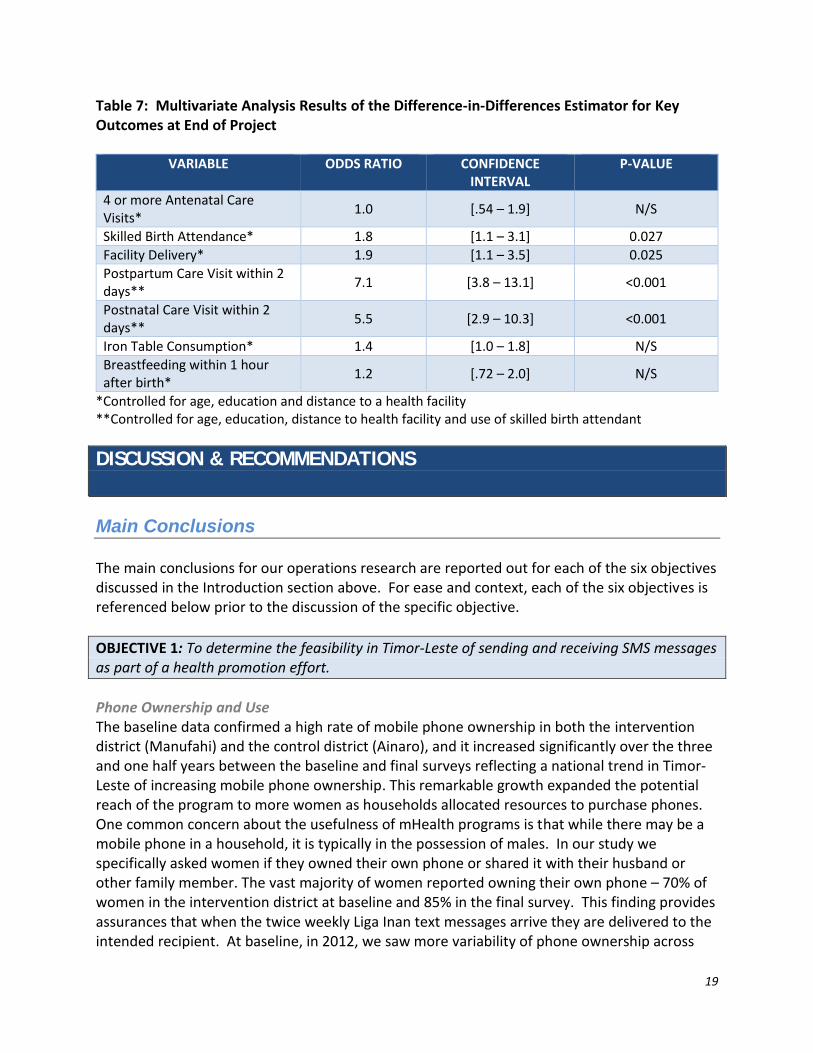
Table 7: Multivariate Analysis Results of the Difference-in-Differences Estimator for Key Outcomes at End of Project
VARIABLE ODDS RATIO CONFIDENCE INTERVAL
P-VALUE
4 or more Antenatal Care Visits*
1.0 [.54 – 1.9] N/S
Skilled Birth Attendance* 1.8 [1.1 – 3.1] 0.027
Facility Delivery* 1.9 [1.1 – 3.5] 0.025
Postpartum Care Visit within 2 days**
7.1 [3.8 – 13.1] <0.001
Postnatal Care Visit within 2 days**
5.5 [2.9 – 10.3] <0.001
Iron Table Consumption* 1.4 [1.0 – 1.8] N/S
Breastfeeding within 1 hour after birth*
1.2 [.72 – 2.0] N/S
*Controlled for age, education and distance to a health facility **Controlled for age, education, distance to health facility and use of skilled birth attendant
DISCUSSION & RECOMMENDATIONS
Main Conclusions The main conclusions for our operations research are reported out for each of the six objectives discussed in the Introduction section above. For ease and context, each of the six objectives is referenced below prior to the discussion of the specific objective.
OBJECTIVE 1: To determine the feasibility in Timor-Leste of sending and receiving SMS messages as part of a health promotion effort.
Phone Ownership and Use The baseline data confirmed a high rate of mobile phone ownership in both the intervention district (Manufahi) and the control district (Ainaro), and it increased significantly over the three and one half years between the baseline and final surveys reflecting a national trend in Timor-Leste of increasing mobile phone ownership. This remarkable growth expanded the potential reach of the program to more women as households allocated resources to purchase phones. One common concern about the usefulness of mHealth programs is that while there may be a mobile phone in a household, it is typically in the possession of males. In our study we specifically asked women if they owned their own phone or shared it with their husband or other family member. The vast majority of women reported owning their own phone – 70% of women in the intervention district at baseline and 85% in the final survey. This finding provides assurances that when the twice weekly Liga Inan text messages arrive they are delivered to the intended recipient. At baseline, in 2012, we saw more variability of phone ownership across

20
sub-districts; for example, in one of the most remote and rural sub-districts, Turiscai, only 54% of households reported owning a phone compared to 79% in Same, a less remote area in the same district. However, by 2015 there was much more similarity in ownership patterns noted across all sub-districts in Manufahi and in all sub-districts phone ownership exceeded 90%. The study also confirmed that women regularly send and receive text messages over their mobile phones. There are no contractual network phone plans offered by the two main Mobile Network Operators in Timor-Leste, rather they are pre-paid phone systems that favor the use of text messages over more expensive voice calls. Eighty-four percent of women in the intervention district reported sending and receiving daily or weekly text messages; this was 64% in the control district. Facilitating the practice of regular text messaging reported by reproductive-age women in the program area is the high rate of literacy in the local Tetum language (79%). In addition, all women who reported they were unable to read in Tetum stated they had available assistance to read messages by family members (husband, child, other) or a neighbor. Most women told us they prefer to receive the Liga Inan text messages in the morning (36%) or afternoon (36%). The proliferation of cell phone towers across the country has brought widespread signal coverage to most areas and certainly is one of the factors facilitating the rapid growth of mobile phone ownership in Timor-Leste. In addition, over the past three years there have been improvements in the electrical grid in Timor-Leste which has resulted in increased ease of charging mobile phones. We learned from the 2012 baseline KPC that families were very resourceful in finding means to charge their phones if they did not have home access to electricity which included solar charger,15 batteries at home, or accessing electricity or solar charger at another site. Liga Inan Enrollment The high degree of readiness for an mHealth program in the intervention district of Manufahi, as evidenced by a high rate of phone ownership and literacy, resulted in high rates of enrollment into the Liga Inan program. We tracked enrollment by sub-district since the onset of the program; however, we estimated coverage based on MoH projected rates of pregnant women, which were extrapolated from old (2010) census data. In the 2015 survey, participation in the Liga Inan program exceeded our previous estimates. Rates were high among all surveyed women (70%). When looking at only women specifically ‘eligible’ to enroll (having had ANC 1 and owning a phone), participation was 77% and was consistently high across all four sub-districts in Manufahi. In addition to high rates of phone ownership and literacy, other factors fostered strong participation in the program. With a high percentage of women attending at least one ANC visit (93% at baseline), ANC proved a very good gateway into the Liga Inan program. Additionally, the emphasis of having trusted MoH health staff enroll women during an ANC visit rather than having unfamiliar program staff carry out the enrollment process, as is done in many other mHealth programs, may have also bolstered enrollment. Another factor that may have contributed to high enrollment is a strong HAI staff presence in Manfuahi. We had five full time
15 There have been a number of development programs focused on solar power in Timor-Leste.

21
staff dedicated to the program based in the district. Along with Catalpa staff, they conducted the initial training for health staff and held community socialization events to inform and advocate for participation in the program. HAI staff, along with our technology partner, Catalpa International, worked closely with MoH health staff to problem solve if they encountered challenges such as registering women or interfacing with the Liga Inan service. Initiation of the first ANC visit in the first trimester increased between the 2012 and 2015 surveys. In the intervention district, women who had an ANC visit during their first trimester increased from 58% to 71% and in the control district it increased from 34% to 48%. Outreach strategies to encourage women to go in early for that first ANC visit would mean more women getting enrolled earlier to Liga Inan resulting in a longer exposure to health messages delivered through the Liga Inan automated service and should be promoted. The integration of the Liga Inan program into routine ANC visits created a strong sense of ownership among health staff (primarily midwives), many of whom became champions for the program. A qualitative study by a graduate student exploring the impact of the Liga Inan program on workload and job satisfaction found that midwives strongly supported the program. Midwives stated that Liga Inan helped them to work more efficiently, assisted them to monitor the condition of their pregnant clients, and provided them with a tool to achieve MoH mandates to increase utilization of maternal health services.16
OBJECTIVE 2: To determine the preparedness of health facilities in Ainaro and Manufahi to deliver high quality basic emergency obstetric care (BEmOC).
While there have been improvements in BEmOC capacity in Timor-Leste since the 2009 national Timor-Leste BEmOC facility assessment, Manufahi and Ainaro district facilities have yet to meet World Health Organization recommendations for providing high quality basic emergency obstetric care. The graduate student who conducted the BEmOC health facility assessment provided a written report to the MoH with the following recommendations based on her findings (reported above in the Main Results section):
Ensure that facilities have equipment to provide basic care management
Increase team approaches to care management.
Improve government monitoring systems
Support the renovation and upgrading of existing facilities
Ensure all providers (midwives and physicians) maintain their basic BEmOC certification
Facilitate the timely distribution of UNFPA BEmOC kits
Conduct BEmOC supportive supervision of health facilities
Research methods to preserve skill level of remotely placed providers that assist with few obstetric complications
Increase resources to transport patients
16 Barnabee, G. Can mHealth strengthen health worker performance? Midwives’ experiences using an innovative mHealth program in Timor-Leste. Unpublished MPH thesis. June 2014.

22
For a full report of the basic emergency obstetric care health facility assessment conducted to answer research questions associated with objective 2, please see Annex 1.
OBJECTIVE 3: To determine the success of messages in reaching the program enrollees.
The aim of the telephone survey of women enrolled in the Liga Inan program was to provide an early program assessment to see if women received messages, read messages, and understood the messages being delivered from the automated Liga Inan service. Women reported being very happy with the program overall and Liga Inan messages were well understood. In addition, a majority of women (65%) could accurately recall message content. The telephone survey also revealed the possibility that the program may not be reaching women as consistently as expected. For example, women only recalled receiving 47% of the messages that were believed to be sent during the previous month. After further investigation is was determined that asking women to recall the number of messages delivered the previous month was likely challenging for women to recall accurately. In subsequent telephone surveys (following program expansion to new districts) this question was revised to ask about the number of messages delivered the previous week which proved to have much better recall. In addition, further investigation revealed that women were missing messages because they often had their phones powered off to save battery. They had not been provided at the time of enrollment with important information that Liga Inan messages would be delivered on Mondays and Thursdays. Subsequently, HAI staff worked with the health staff enrolling women into Liga Inan to assure that women were provided with this important information in order to have their phones powered on when messages were delivered. For a full report of the telephone survey please see Annex 2.
OBJECTIVE 4: To determine whether receiving regular SMS messages that encourage healthy maternal behaviors is associated with significant improvement in maternal health knowledge and behaviors for women enrolled in Liga Inan (Manufahi district) compared to baseline rates and the control area (Ainaro District).
OBJECTIVE 5: To determine whether receiving regular SMS messages that encourage healthy maternal behaviors is associated with increases in use of MNC services for women enrolled in Liga Inan (Manufahi District) compared to baseline rates and the control area (Ainaro District).
The Liga Inan study suggests that tips and reminders to seek appropriate care delivered via mobile technology were successful in increasing the likelihood of having a skilled birth attendant at delivery (whether at home or in a facility), delivering in a health facility, and having timely postnatal care. The study did not show that women living in the intervention district, compared to the control district, were more likely to have four or more ANC visits, consume iron tablets during pregnancy, initiate early breastfeeding, or use a modern method of contraception. They were also no more likely to have increased knowledge about danger signs
23
or the benefits of waiting at least 24 months after delivery before getting pregnant again. These findings covering objectives 4 and 5 will be discussed in this section. UTILIZATION OF MATERNAL AND NEWBORN CARE Antenatal Care In the 2012 baseline KPC survey, the rate of four or more ANC visits was 75% in Manufahi and 67% in Ainaro. In the final 2015 survey both districts showed impressive gains in ANC 4, to 85% in Manufahi and 81% in Ainaro. It is unclear what generated the gains in ANC 4 in Ainaro during the study period, particularly given that these same gains in service utilization were not observed for skilled birth attendance, facility delivery or postnatal care (reported below). Mulitvariate analysis showed no association between Liga Inan and women’s receipt of four or more ANC visits. Skilled Birth Attendant, Facility Delivery, Postpartum & Postnatal Care In Timor-Leste women can elect to deliver with a skilled birth attendant (SBA) at their home or in a health facility, both options are supported by the government-run health system. A SBA is defined in our study as a doctor, midwife, or nurse being present at delivery. In Manufahi after the launch of Liga Inan, there were significant increases in delivery with a SBA, facility delivery, and postpartum and postnatal care compared to baseline and to the control district of Ainaro. These increases were consistent across all sub-districts in the intervention district of Manufahi. We speculate that factors that increase the likelihood that women will act upon a text message and seek care may be related to enhanced and more frequent communication between mothers and their midwives; bridging a communication gap appears to be an important element of the Liga Inan program. The regular communication via weekly automated text messages may be enhancing the perceived relationship between client and provider. Many enrolled women seem to believe that the text messages are coming directly from their midwife and not via an automated service. Mothers often send a reply “thank-you” text after receiving the automated Liga Inan message (per data collected by the Liga Inan dashboard). In addition to the automated messages, the Liga Inan service facilitates two-way voice communication. Pregnant women enrolled in Liga Inan are provided the ability to send a text via the service to their midwife requesting a call back from the midwife. Seventy percent of women enrolled in Liga Inan reported using this feature, and 92% stated the midwife called back quickly. Some women chose to bypass this system and call their midwife directly using the phone number that is stamped into their maternal handbook when they are enrolled into Liga Inan. The Liga Inan program also facilitates communication from health staff to expectant mothers. Health staff receive a list of their clients who are three weeks away from their estimated due date that includes the mother’s name and phone number which should trigger a phone call from health staff to mother to check in about the family’s birth plan. Our research revealed compelling data that shows that women who have been in more communication with health staff are more likely to have a skilled birth attendant and a facility delivery. In graduate student research exploring both midwives’ and mothers’ experiences with the Liga Inan program, both groups remarked on improved communication and stronger

24
relationships due to the program. Midwives reported that through Liga Inan they can build good relationships by having more contact with mothers.17 The facilitation of communication between women and the health system was described by enrolled women as an important benefit of participating in the Liga Inan program.18 Increasing a sense of connection between health provider and pregnant women appears to influence women’s choice about seeking care at the time of delivery. Tetanus Toxoid Vaccination and Anti-Parasite Medication Our study showed that rate of women who received tetanus toxoid (TT) vaccination during their most recent pregnancy actually decreased slightly from 2012 to 2015 in both Manufahi and Ainaro districts: in Manufahi it went from 85% coverage to 75%; and in the control district, Ainaro, it dropped from 74% to 66%. When health staff in Manufahi were presented with data from the final KPC survey, they suggested that the higher coverage rates for TT noted at baseline was likely the result of a massive national TT vaccination campaign that was conducted in early 2012. The TT vaccination is not something specifically the Liga Inan program would be expected to impact, except in terms of facilitating getting women into four or more ANC visits where this service would be delivered. The high rates of ANC 4 in both districts mentioned above would support the argument that there may have been an artificially high baseline rate of TT vaccination due to the national campaign conducted just prior to 2012 data collection. The reported coverage rates for anti-parasite medication provided to pregnant women is generally low and decreased during the study period. It dropped significantly in Manufahi from 22% coverage in 2012 to only 12% in 2015; in Ainaro it was low in 2012 at 14% and increased to only 16% in 2015. It is unclear whether the poor coverage rates overall, and the drop in coverage in Manufahi, is related to stock outs of medication, issues related to quality of care, or perhaps even a lack of understanding or recall by the women about a medication taken. Use of a Modern Method of Family Planning Liga Inan text messages, particularly during the six weeks after delivery, promote the use of family planning. There was essentially no change in the percentage of women using a modern method of family planning among women in the intervention district between the baseline (54%) and final (55%) surveys, while in the control district there was an increase from 23% to 32% in modern contraceptive use. Whether or not a Timorese woman chooses to use a modern contraceptive method has a number of potential influencing factors including: the dominant Catholic religion, a cultural desire for large families, the strong influence on reproductive choice by husbands and parents, and some prevailing myths and rumors that discourage use of several methods.19 At the time of the DHS 2009/10, contraceptive prevalence was only 22% nationally, with rates of 25% in Manufahi and 14% in Ainaro.20 Given these contextual factors we were 17 Barnabee, G. Can mHealth strengthen health worker performance? Midwives’ experiences using an innovative mHealth program in Timor-Leste. Unpublished MPH thesis. June 2014. 18 Dyer, J. Maternal health behavior change: Women’s experiences as participants in an mHealth program in Timor-Leste. Unpublished Report for the Timor-Leste Ministry of Health. October 15, 2015 19 Health Alliance International. Child Spacing Qualitative Community Assessment in Aileu and Manatuto Districts. October 2006. 20National Statistics Directorate [Timor-Leste] MoFT-L, and ICF Macro.,Timor-Leste Demographic and Health Survey 2009-10. Dili, Timor-Leste: NSD [Timor-Leste] and ICF Macro, 2010.

25
surprised in the 2012 baseline survey that 54% of women in Manufahi reported using a modern method, compared to 23% in the control district, Ainaro. Because of the high baseline rate in Manufahi, it may have been difficult to realize a significant increase in that practice during the study period. Another factor that may also be impacting rates of method utilization in both districts is the strong presence of Marie Stopes International, which partners with the MoH to build capacity to deliver high quality family planning services, directly delivers family planning services, and promotes family planning in communities. KNOWLEDGE AND HOME CARE BEHAVIORS Knowledge of Danger Signs While the study confirmed that text messages as tips and reminders to seek care appear to be effective to nudge enrolled women into utilizing important maternal services, it did not show evidence that a text message approach is effective for increasing knowledge. The study showed no association between participation in the Liga Inan program and increased knowledge of danger signs during pregnancy, delivery or the postnatal periods, and in fact, knowledge of danger signs decreased from 2012 to 2015. The text message format used to deliver weekly Liga Inan messages to women has limitations in the length and complexity of the messages that can be effectively conveyed given it is limited to 160 characters per message. Messages communicating simple tips and reminders to seek care appear to be a good fit for this format while more complex messages conveying multiple danger signs across four different time periods may not be as suitable. These more complex messages to increase knowledge around danger signs would benefit from being reinforced through more conventional health promotion approaches, for example, mother’s groups. Benefits of Child Spacing The knowledge that women should wait at least 24 months after delivery before getting pregnant appears to be quite common in Timor-Leste. At baseline, 80% of women in Manufahi and 82% in Ainaro reported they should wait at least 24 months and this increased to 91% and 85%, respectively over the study period. There was no association of increased knowledge of the recommended birth interval with participation in the Liga Inan program. Once again, Marie Stopes International is active in community family planning promotion in both districts, which may contribute to the high rate of knowledge of the ideal birth interval. Iron Tablet Consumption Some home care practices may be strongly culturally bound or socially influenced, and for those the SMS format does not appear to be effective in promoting behavior change. For example, there is a strong belief in Timor-Leste that consuming iron tablets during pregnancy will produce a large baby, resulting in a difficult delivery, and as a result pregnant women are often reluctant to consume the recommended number of iron tablets.21 Our study showed that most women in Manufahi and Ainaro received iron tablets during pregnancy, 94% and 93% respectively in 2015; however, only 57% of women in both districts reported consuming 90 tablets or more. There 21 Health Alliance International. Strengthening Maternal and Newborn Care in Timor-Lest: Qualitative Community Assessment. February 2005.

26
was no association between participation in the Liga Inan program and consumption of iron tablets. Overriding strong belief patterns may require complementary efforts through more conventional health promotion approaches to achieve behavior change. Immediate Breastfeeding There was no association between immediate breastfeeding of newborns and participation in the Liga Inan program, although the rate of newborns receiving breastmilk within one hour following delivery increased significantly in both districts during the study period, from 51% to 85% in the intervention district, and 60% to 90% in the control district. One contextual factor that may be contributing to high rates of early breastfeeding in both Manufahi and Ainaro is a local NGO that has been very active in both districts promoting breastfeeding.
OBJECTIVE 6: To determine the feasibility of implementing, maintaining and expanding a mobile phone technology program.
As mentioned previously, HAI planned to employ an external consultant to travel to Timor-Leste and carry out an independent evaluation as required by the terms of our USAID Cooperative Agreement. This consultant would have been tasked with answering questions associated with Objective 6. However, in mid-2015 the MoH informed donors that they intended to carry out an independent evaluation of the Liga Inan program and requested the Australian Government, Department of Foreign Affairs and Trade (DFAT) to financially support this effort. When HAI learned of the MoH intentions, we opened discussions with USAID and DFAT Mission staff in order to avoid a duplication of efforts between HAI and the MoH research team. The end result of those negotiations was that HAI maintained control over conducting our final KPC survey, but relinquished overall program evaluation to the MoH team. In addition, HAI with USAID approval, financially supported a consultant to provide capacity building for the MoH research team to develop a research plan and interview tools for their evaluation. USAID Washington D.C. gave approval to accept the MoH evaluation report in lieu of HAI submitting a Final Program Evaluation Report. At the time of this writing the MoH evaluation is completed and a written report in the Tetum language is available. The report is in process of being translated into English and will be provided to USAID once finalized. While HAI did not employ an external consultant to address the research questions under Objective 6, we can offer commentary on the questions as follows: Was a successful mHealth platform developed? What were the main challenges in developing the Liga Inan technology software, website and server platform? Describe technological problems that occurred and how they were resolved. These questions were intended to be addressed to Catalpa International, our technology partner for the Liga Inan program, by an external evaluator tasked with the overall program evaluation. To our knowledge Catalpa was not interviewed as part of the MoH evaluation plan. We can confirm that a high performing and successful mHealth platform was developed, but cannot respond to the other questions as this work was the purview of Catalpa.

27
What was the role of community members and stakeholders in implementation? Was there an important community champion? During the development phase of the Liga Inan program in 2012 when Catalpa was developing the Liga Inan service, we encountered some opposition to the idea of implementing an mHealth program at the national MoH level. One high ranking MoH official declared that households in Manufahi did not have mobile phones and that most women were illiterate and could not read text messages and therefore, the program would fail. It was only through our baseline KPC data that showed that 69% of households in Manufahi had phones and that 73% of women could read that changed the mind of this official and we were given approval to implement the pilot. HAI carried out advocacy meetings with district health leadership, CHC managers, and health providers, primarily midwives, prior to the launch of Liga Inan in Manufahi District. Because of the novelty of implementing an mHealth approach in Timor-Leste it was essential to gain strong buy in from the district health team. In addition, the program was being integrated into their work and would change their clinical practice. We encounter overwhelming support for the Liga Inan program by health staff in Manufahi. The Director of Health for the district was a very strong advocate of Liga Inan and provided strong advocacy for the program at the national level. In 2015, a new Director was appointed in Manufahi who is herself a midwife and she is also a very strong advocate of Liga Inan. In addition, midwives in Manufahi universally support the program. Graduate student research on the impact of Liga Inan on job motivation and satisfaction showed that midwives believed Liga Inan improved their relationship with their community and their patients, and gave them a tool to meet MoH targets for service utilization.22 HAI also conducted extensive promotion for the Liga Inan program in all villages in every sub-district of Manufahi. It was important to inform community leadership and families about the availability of this new program, how it worked and to encourage women to go in for ANC and bring their phone so they could get registered. We believe that strong community promotion bolstered participation in the Liga Inan. To what extent did MoH district health staff become engaged and maintain engagement in Liga Inan over the course of the program? As mentioned above, district health staff in Manufahi were highly engaged with the program from the onset and have remained engaged three years later. We first launched Liga Inan in the sub-district of Same and four months later rolled out to the additional three sub-districts. Midwives from Same sub-district participated in the three-day Liga Inan training for health staff in subsequent sub-districts. Their enthusiasm for the Liga Inan program and sharing their lessons learned proved a very effective peer-to-peer training strategy to engender a strong motivation to implement the program among new trainees. Furthermore, in 2014 when DFAT provided funds to expand Liga Inan, we carried out a study tour where midwives from the new
22 Barnabee, G. Can mHealth strengthen health worker performance? Midwives’ experiences using an innovative mHealth program in Timor-Leste. Unpublished MPH thesis. June 2014.

28
expansion district traveled to Manufahi to learn about Liga Inan from the midwives who were then seasoned implementers. One strategy we have employed to maintain engagement in the program was to conduct an annual review meeting where we bring all the health staff in the district together with managers for one day to review key HMIS data, share lessons learned and spread good ideas, such as examples of how midwives are using the broadcast message feature of the Liga Inan service. We believe this has assisted in keeping motivation and engagement high. What was the engagement of mobile network service providers in Timor-Leste with the Liga Inan program? When Liga Inan was launched in Manufahi in March 2013 there was only one Mobile Network Operator (MNO) in Timor-Leste, Timor Telecom who held a government-supported monopoly. However, only months after launching Liga Inan this monopoly was broken and two new MNOs were granted license to operate in the country – Telmor and Telkomcel. As of June 2016, the only real competitor to Timor Telecom with substantial market share is Telemor. In October 2014, HAI and Catalpa entered into an agreement with Timor Telecom whereby they support the cost of all Liga Inan messages going to their customers. Timor Telecom also offered to support the cost of $10 phone credit to health staff engaged in the Liga Inan program up to $1,000/month. The phone credit is automatically delivered to their mobile phones the first of each month. HAI and Catalpa renewed this agreement in October 2015 and are currently negotiating to renew for another year. Timor Telecom sponsorship has been a very significant step toward sustainability of the Liga Inan program. Catalpa is currently in discussions with Telemor to provide support for Liga Inan text messages for their customers which would essentially bring the program cost of SMS to zero. Our hope is that future agreements will be between the MoH and the MNOs. Has the policy environment for an mHealth program improved in Timor-Leste? The policy environment for an mHealth project has significantly improved over the past four years. Liga Inan is the first ever mHealth program in Timor-Leste. When the program was first proposed to the MoH in 2012 there was reluctance to give approval to implement such a novel approach. However, four years later, the MoH has not only given approval for scale up of Liga Inan, but has also taken over management of the program in Manufahi and has provided a dedicated budget for the program in that district. We will be handing over a second district to MoH management in October 2016.
Brief Summary of Evidence This study shows evidence of the success of the Liga Inan intervention in motivating mothers to access SBA, facility delivery and timely postnatal care. The study did not show that women living in the intervention district, compared to the control district, were more likely to have four or more ANC visits, consume iron tablets during pregnancy, initiate early breastfeeding, or use a modern method of contraception. They were also no more likely to have increased knowledge

29
about danger signs of pregnancy, delivery, and the postnatal period or the benefits of waiting at least 24 months after delivery before getting pregnant again. The SMS format that is limited to 160 characters appears to be an effective format as tips and reminders to seek care, however, it may be constrained in conveying more complex messages, such as danger signs of pregnancy, delivery and the postnatal period and it may not have sufficient “power” to influence behavior change that is strongly culturally influenced.
Limitations of the Study The 2012 baseline survey was carried out during the rainy season and two of the most remote enumeration areas (EAs) in the intervention district were inaccessible. Two accessible EAs were randomly selected as substitutes. The communities in the more accessible EAs may have been different in some regards from the more remote EA communities that were not included in the baseline survey. In 2015, striving for comparability between the two surveys we elected to exclude these remote areas from the final survey. Additionally, the survey relied on self-reported information by women who had to recall specific information regarding events that occurred up to two years previously.
Comparison of Results with Other Research Our findings that show an uptake of maternal health services are similar to research done on other mHealth programs focused on maternal and newborn healthcare. The wired mothers’ mobile phone project in Zanzibar that employed a SMS intervention for pregnant women showed increased odds of skilled delivery attendance, however while a significant increase was noted among urban women, the same increase was not seen for rural women.23 In our study, the majority of the study area, both intervention and control, is rural and our analysis controlled for distance to a health facility. We saw increases in SBA, facility delivery, and postnatal care across all the intervention sub-districts, however, the most remote area did see smaller increases compared to the less remote areas. The wired mothers study also showed that women in the mobile phone intervention group had more than double the odds of having four or more ANC visits, which our study did not show.24 An evaluation of an mHealth project in Malawi, the Chipatala Cha Pa Foni Project, found that that providing personalized health advice and tips and appointment reminders by phone increased home-based MNCH practices, such as use of bed nets during pregnancy and also increased attendance of ANC within the first trimester, but like our study it did not have an effect on increasing knowledge indicators.25 23 Lund S and Hemed M (2010) Wired mothers: use of mobile phones to improve maternal and neonatal health in Zanzibar. [Internet]. Copenhagen: University of Copenhagen [cited 2010 Dec 10]. Available from: http://www.oresund.org/logistics/content/download/74534/429853/file/Ida%20Marie%20Boas_Wired%20Mothers.pdf 24 Lund, et al. BMC Pregnancy and Childbirth. 2014. 14:29 http://www.biomedcentral.com/1471-2393/14/29 25 Watkins, S, Robinson, A, Dalious, M. Evaluation of the Information and Communications Technology for Maternal, Newborn
and child Health Project. December 2013. Available from:
http://innovationsformnch.org/uploads/resources/pdfs/ICT_for_MNCH_Report_131211md_FINAL,_AY_to_Gates_language.pdf

30
Immediate Intervention Uptake Results from this study have been presented to national and district health authorities in Timor-Leste, donors and other stakeholders in both oral and written presentations. In addition to the baseline and final KPC evaluation of the Liga Inan program, HAI has collected and analyzed HMIS data to assess uptake in maternal health services. We examined key indicators in a times series analysis comparing 12 months prior to Liga Inan launch and 12 months post-launch in Manufahi District. The data is disaggregated at the sub-district level. One year after the launch of the Liga Inan pilot, the Australian Government/DFAT was impressed with early program results that showed uptake in SBA, facility deliveries, and postnatal care. With MoH approval for scale up, DFAT awarded HAI and Catalpa International funding to expand Liga Inan to additional districts in the country. Between June 2014 and June 2016, HAI and Catalpa have expanded Liga Inan into four additional districts with three more planned in the next 12 months. By June 2017, Liga Inan will be operational in eight of the country’s 13 districts. In March 2016, HAI and Catalpa handed over management and partial resourcing of Liga Inan in Manufahi District. The Manufahi District Health Management Team has selected a Liga Inan focal point responsible for managing and monitoring the program and the MoH has approved a modest budget for Liga Inan in Manufahi. HAI and Catalpa will continue to monitor enrollment and service utilization in Manufahi District to track progress during a handover transition period. Handover of Liga Inan management and resourcing to the MoH is planned in additional districts over the next 12 months.
Implications of Results The study findings suggest that there is an enabling environment in Timor-Leste to support the implementation of an mHealth program with high rates of mobile phone ownership and literacy. High rates of participation in the program demonstrate community engagement and health staff support for integrating Liga Inan into their clinical practice. Based on the study findings, the Liga Inan program can assist the MoH to achieve desired goals of increasing the rates of SBA, facility delivery and timely postnatal care and provides a strong case for the decision to scale up the program to additional areas of Timor-Leste. An mHealth approach does not appear to be as effective at increasing mother’s knowledge or changing behaviors that are heavily influenced by culture and social contexts. To increase maternal knowledge of danger signs or to change some home care behaviors we would suggest partnering with other community health promotions efforts, such as mother’s groups, to reinforce these Liga Inan messages in a peer-to-peer approach.

Basic Emergency Obstetric and
Neonatal Care Assessment Manufahi and Ainaro Districts
Final Report
March 2012
Annmarie Nolan, BSN, RN, MN
Health Alliance International University of Washington
Annex 1: Basic Emergency Obstetric and Neonatal Care Assessment

Acknowledgements The author would like to thank Health Alliance International staff, United Nations Population Fund’s Dr. Angela Bismark and Dr. Amita Pradhan Thapa for their input, the Ministry of Health staff for their participation, and lastly USAID and Health Alliance International for project funding.

Table of Contents Executive Summary ………………………………….……………………………...…………………………………………………... 1 Background…………………………………………………………………………………………………………………………………….. 3 Problem Statement…………………………………………………………………...…………………………………………………... 3 Methods…………………………………………………………………………..………………………………………………………….…... 4 Results
Staffing……………………………………………..…………………………………………………………………………………. 5 Case Summaries………………………………………………………………………………………………………..………. 6 Service Availability…………………………………………………………………………………………………...……… 6 Staff Knowledge Levels…………………………………………………………………………………………………… 7 Equipment and Supplies…………………………………………………………………………………………………. 9
Conclusions………………………………………………………………………………………………………………………………….. 10 Recommendations……………………………………………………………………………………………………………………… 11 Immediate Recommendations…………..………………………………………………………………………… 11 Long-term Recommendations…………………………...…………………………………………...…………… 12
Annex 1: Government Health Facilities providing Emergency Obstetric Care Services…14 Annex 2: Midwife Assessment Supplement ………………………………………………………………………….. 15 Annex 3: Service Availability and Staffing Table ………………………………….…………………………..….. 16 Annex 4: Facility Condition and Staffing ……………………………………………………………………………….. 17 Annex 5: Midwife Knowledge Survey………………………………………………………………………………………. 18 Annex 6: Equipment List to Perform BEmOC by Facility ……………….………………………………….. 20

Abbreviations: Demographic and Health Survey (DHS) National Reproductive Health Strategy (NRHS) Health Alliance International (HAI) Averting Maternal Death and Disease (AMDD) United National Population Fund (UNFPA) Ministry of Health (MOH) Community Health Centers (CHCs) Family Health Promoters (PSFs) Integrated Community Health Services (SISCa) Emergency obstetric care (EmOC) Emergency obstetric and neonatal care (EmONC) Basic emergency obstetric care (BEmOC)

1
Executive Summary The Timor-Leste government has fought to reduce maternal mortality using safe motherhood strategies on a national scale. Despite efforts to reduce maternal deaths, the 2009/10 Demographic and Health Survey (DHS) found that the maternal mortality ratio remains high at 557 per 100,000 live births. In January and February of 2012, Health Alliance International (HAI) assessed basic emergency obstetric care in mid-level health facilities in the districts of Ainaro and Manufahi. The purpose of the assessment was to monitor the scale-up of basic emergency obstetric care in rural areas and to assist the development of Mobile Moms, a maternal health project aiming to improve health and care-seeking behaviors of pregnant women and their newborns. A United National Population Fund survey tool enhanced with additional interview questions was used to assess seven district and sub-district level health facilities and seventeen midwives. Results were compared between facilities and World Health Organization emergency obstetric care (EmOC) policies and recommendations. The findings show that: Service availability varies throughout the two districts, with the most remote
facilities having the fewest staff members available inhibiting 24 hours per day coverage. Supervisory physicians are often temporarily placed in facilities, causing inconsistencies in technical support and team management styles.
There continue to be weaknesses within the government surveillance system. Within facilities’ monthly records there were inconsistencies in case numbers and missing data. A majority of the health facilities managed few obstetric complications and midwives lack an adequate caseload to practice and maintain basic EmOC skills.
Other than the Maubisse Referral Hospital, midwives from the Prince of Monaco II
Maternity House were the only interviewed who performed all basic EmOC signal functions in the past three months. Skill confidence varied across facilities, with some midwives acknowledging increased confidence with team care management approaches.
Equipment is not consistently available to provide high quality basic EmOC. Basic
equipment to monitor and detect early complications was missing from numerous facilities. Equipment to perform basic EmOC function was missing or staff lacked knowledge on proper maintenance. At the time of assessment, medicines were well distributed, but staff admitted to experiencing frequent shortages.
While improvements have been made since the 2009 national EmOC assessment, the Manufahi and Ainaro district and sub-district facilities have yet to meet World Health Organization recommendations for providing high quality basic emergency obstetric care. Before additional emphasis is focused on quality improvement, efforts need to target health system improvements based on district and individual facility level need.

2
Key Recommendations: Immediate 1. Ensure that facilities have equipment to provide basic care management.
Revamp the MOH equipment and supply request process to decrease waiting periods. Supervisory staff should be knowledgeable in and oversee equipment maintenance.
2. Increase team approaches to care management. Inter-professional approaches to managing maternal health care have shown to be more effective to improving quality of care. Prenatal and delivery care staff and records should be located within the same health facility increasing continuity of care.
3. Improve government monitoring systems by mentoring health staff through routine Safe Motherhood and EmOC supervision and reviewing case summary reporting.
Long-term 4. Support the renovation and upgrading of existing facilities to improve power
supplies and water and sanitation systems. 5. Ensure all providers (midwives and physicians) maintain their basic EmOC
certification. All midwives should complete the certification, prioritizing district health facility staff. Routine refresher trainings should integrate physician and midwives together to reinforce team care management approaches and maintain skill levels. Upon basic EmOC certification, all providers should be universally approved to independently perform functions as described by MOH policy.
6. Facilitate the timely distribution of UNFPA EmOC kits, ensuring that all facilities have the equipment necessary to perform basic emergency obstetric care. Kits should be reviewed with receiving staff to ensure proper maintenance of equipment.
7. EmOC supportive supervision should be integrated in safe motherhood visits to sustain longevity of skill quality after training completion. Measures that can preserve skill quality include hands-on practice, team approaches, and follow-up training, which can be provided during supervision visits.
8. Research methods to preserve skill level of remotely placed providers that assist with few obstetric complications. Consider developing a rotation for remote midwives to practice obstetric skills within facilities with a higher number of abnormal obstetric cases providing them the hands-on practice. Alternatively, the MOH can consider a trial of low technology simulation-based EmOC practice, such as that available at the University of Washington’s PRONTO project.
9. Increase resources to transport patients, ensuring that timely care is accessible. Increase fuel supply for emergency transportation and primary care SISCa’s. Consider monitoring the referral transportation system to ensure that an appropriate number of vehicles are available to serve population needs

3
Background Timor-Leste has been invested in health system strengthening since independence in 2002. Efforts by the Ministry of Health and non-government agencies have targeted numerous sectors, but have largely focused in maternal health. Yet the 2009/10 Demographic and Health Survey (DHS) found that the maternal mortality ratio remains high at 557 per 100,000 live births.1 Behind this statistic, it also found that 70 percent of births are not assisted by a skilled attendant and only 22 percent of deliveries occur within a health facility. The 2004 Timor-Leste National Reproductive Health Strategy (NRHS) provides a four-strategy approach to make pregnancy safer.2 These Safe Motherhood approaches included 1) increasing the knowledge level in the general population on issues related to pregnancy and childbirth; 2) improving the quality and coverage of prenatal, delivery, postnatal, and perinatal health care; 3) improving emergency obstetric care (EmOC) through recognition, early detection, and management or referral of complications of pregnancy and delivery; and 4) integrating effective detection and management of STI cases into maternal and perinatal care. Health Alliance International (HAI) is currently launching a four-year project aimed at supporting the Safe Motherhood component of the NRHS. The Mobile Moms project uses an integrated approach in working with district and sub-district MOH health facilities down to Family Health Promoters (PSFs), who provide access to the individual households. The health staff strengthening component of the Mobile Moms project aims to improve skills of health teams to provide quality maternal care services through supportive supervision of midwives in maternal care services and training in basic emergency obstetric and neonatal care. Problem Statement The overall goal of the Health Alliance International project Mobile Moms is to improve the health and care-seeking behavior of pregnant women and their newborns. As a part of this effort, HAI aims to support government health facilities to ensure that pregnant women and their newborns receive high quality care. This aim will be accomplished through technical support in Safe Motherhood and emergency obstetric and neonatal care (EmONC). In 2008, the United National Population Fund (UNFPA) conducted a national EmOC needs assessment. This assessment found multiple limitations to providing quality EmOC in Timor-Leste, such as poor infrastructure, lack of maternity space, inadequate equipment and supplies, poor transportation and communication schemes, weak
1 National Statistics Directorate (NSD) [Timor-Leste], Ministry of Finance [Timor-Leste], and ICF Macro.
2010. Timor-Leste Demographic and Health Survey 2009-10. Dili, Timor-Leste: NSD [Timor-Leste] and ICF Macro. 2 Ministry of Health [Tmor-Leste]. 2011. National Health Sector Strategic Plan. 2011-2030: Towards a Health East Timoree People in a Health Timor-Leste.

4
logistic system, and lack of confidence of trained midwives to perform some signal functions.3 In 2010, HAI field-tested a basic EmOC supervision assessment form with the Ministry of Health (MOH) in Manatuto and Ainaro district centers.4 In 2012, UNFPA and the MOH initiated EmONC supervision visits in all district and sub-district Community Health Centers (CHCs) with a focus on basic EmONC identified sites. See Appendix 1 for a list of EmOC sites. To appropriately support the Ainaro and Manufahi midwives within the Mobile Moms project, HAI assessed current basic EmONC conditions within the two districts. Results from the assessment will be used to increase EmONC capacity within the two districts and can be applied nationally. Methods This baseline assessment targeted government health facilities within the Manufahi and Ainaro districts. To measure the availability of BEmONC throughout this geographic region, district and sub-district CHCs and Maternity Houses were targeted for assessment. District and sub-district health facilities have been identified by the Ministry of Health and UNFPA to be developed into BEmONC facilities by 2015. A University of Washington graduate nursing student, assisted by HAI technical staff, visited eight sites between January 17th and March 2nd 2012. Those sites included health facilities in all four sub-districts in Manufahi, and three sub-districts in Ainaro (see Table 1). Approval from district government staff and individual consent was received prior to survey initiation. The BEmONC assessment was conducted using a mixed method approach. Multiple indicators were gathered from health facilities using a MOH approved UNFPA questionnaire; indicators included staffing, case summary reports, service availability, staff knowledge levels, equipment, supplies, and drugs.5 These quantitative results were compiled into an excel database.
3 Ministry of Health [Timor-Leste]. 2004. National Reproductive Health Strategy 2004 – 2015. Dili, Timor-
Leste: Ministry of Health. 4 Ministry of Health [Timor-Leste], and United Nations Population Fund (UNFPA). 2008. Emergency Obstetric Care (EMOC) Needs Assessment. Dili, Timor-Leste: NSD [Timor-Leste] and UNFPA. 5 Ministry of Health [Timor-Leste], and United Nations Population Fund (UNFPA). 2008. Emergency
Obstetric Care (EMOC) Needs Assessment. Dili, Timor-Leste: NSD [Timor-Leste] and UNFPA.
Table 1. BEmOC Asssessment Sites
Number of Midwives
Number of EmOC Certified Midwives
Completed Facility Assessments
Number of Completed Midwife Assessed
Manufahi CHC Same 2 x - -
Prince of Monaco Maternity House 7 5 1 6 Turiscai Maternity House 1 0 1 1 Fatuberlihu Maternity House 3 2 1 1
CHC Alas 1 0 1 1 HP Betano 1 1 - 1
Ainaro
CHC Ainaro 3 2 1 3
CHC Hatudu 1 1 1 1
CHC Maubisse 1 0 - -
RSU Maubisse 5 4 1 3
CHC Hatubelico 1 1 - -
Total: 26 15 7 17

5
Midwife capacity was assessed using a UNFPA individual staff knowledge level questionnaire enhanced with additional interview questions. This tool aimed to measure the frequency and confidence of treating obstetric cases while gathering additional background information. Qualitative questions inquired on barriers to providing BEmONC, quality of home delivery assistance, and early complication identification and care. See Annex 2 for the interview supplement. This individual assessment was distributed to seventeen midwives in the Ainaro and Manufahi districts, from every level of MOH facilities ranging from the Maubisse Referral Hospital to a Manufahi health post. The number of midwives interviewed at one facility ranged between one and six midwives. Midwives’ names were not used, however survey identification numbers were linked to facility assessments allowing staff and facility data to be combined. Results The facility and midwife assessment results were collected and entered into separate excel databases. Data gathered provide a geographic representation of the two districts, with survey sites distributed over seven of the eight sub-districts. One planned Ainaro sub-district CHC was not visited due to time constraints. The following results are separated into staffing, case summary reports, service availability, staff knowledge levels, equipment, supplies, and drugs. Staffing Facilities ranged in human resource support. Four of the sub-district health facilities (CHCs and Maternity Houses) have only one midwife providing obstetric services. Only two of the facilities admitted to having midwives present twenty-four hours a day, everyday. On average, midwives interviewed assist with only seven births a month. While physicians were not included in the MOH questionnaire, midwives commented on their presence within health facilities due to their supervisory role. The Maubisse Referral Hospital is the only facility with a permanent obstetrician physician position. District CHCs have general physicians, however, most positions are filled with internationals under contract that leave the facility after a year or two.

6
Case Summaries
Table 2. 2012 Facility Case Summaries (#)
Obstetric cases Complications Referral
An
ten
atal
car
e co
nsu
ltat
ion
s
To
tal d
eliv
erie
s
Liv
e b
irth
s
New
bo
rns
wit
h n
orm
al
bir
thw
eigh
t
Ho
me
bir
ths
Fac
ilit
y b
irth
s
To
tal o
bst
etri
c ad
mis
sio
ns
Hem
orr
hag
e ca
ses
Dy
sto
cia
or
pro
lon
ged
b
irth
cas
es
Po
st-p
artu
m in
fect
ion
ca
ses
Ecl
amp
sia
case
s
Ab
ort
ion
cas
es
Ref
erre
d o
bst
etri
c ca
ses
Rec
eiv
ed o
bst
etri
c ca
ses*
Prince of Monaco Maternity House
2339 329 329 319 12 317 396 27 1 1 7 18 49 x
Turiscai Maternity House
402 95 92 92 85 7 7 0 0 0 0 0 1 0
Alas Maternity House 438 63 63 62 33 30 30 0 0 0 0 2 10 0
Faterberlihu Maternity House
514 108 108 108 31 77 77 5 3 0 0 6 2 0
Maubisse Referral Hospital
1567 188 184 163 13 175 194 9 6 11 23
15 4 137
Ainaro CHC 844 186 186 177 64 122 122 0 1 0 1 8 2 x
Hatudo CHC 686 89 89 87 37 52 52 1 0 0 0 1 1 0
*x = these facilities did not record the number of obstetric cases received
2011 case summary data was collected from seven facilities (see Table 2). The Prince of Monaco II Maternity House performs a notably higher number of births, even when compared to the referral hospital or Ainaro district CHC. The Turiscai Maternity House is the only facility that performs substantially more home than facility-based births. It is a new addition to that sub-district, so facility-based births are expected to rise in 2012. While the maternity houses have increased access to facility-based deliveries across the two districts, there has been no evident shift of home to facility-based births during 2011. Additionally, the frequency of reported obstetric complications remains low in most facilities. Few obstetric patients were referred from the Turiscai, Alas, and Hatudo facilities, reinforcing the infrequency of complication cases managed by health professionals. Indications of obstetric referrals were difficult to monitor as many referrals were excluded from facility complication case reports. Also, records did not uniformly document cause of referral. Referral cases were difficult to track through facilities and inconsistencies within facility forms suggested some erroneous reporting. Service Availability All facilities reported having midwives available on-call as needed. Midwives lived in varying proximities to health facilities and inconsistent transportation sometimes caused a delay of services. The Maubisse Referral Hospital and the district CHCs had other health staff (nurses, midwives and nurse assistants) available twenty-four hours a day if skilled assistance was required during evening or night hours. Medicines are available during evening hours at all monitored facilities, faulting Turiscai, which was not measured. Maubisse Referral Hospital was the only facility with laboratory technicians available at night, however numerous midwives claimed to independently

7
test for malaria if needed. Overall, very few laboratory tests are conducted at rural sites. See Annex 3 for a complete list of service availability and staffing. Staff Knowledge Levels Sixteen of the seventeen midwives interviewed assisted with deliveries in 2012. Quantitative data is based on the sixteen midwives currently providing maternity care. Qualitative data includes the seventeenth midwife who provides antenatal in the Maubisse Referral Hospital. Eight (47.1%) of the midwives interviewed work in Maternity Houses. Five (29.4%) midwives work in CHCs, one in a health post, and three (17.6%) in a hospital. Seventy one percent of the midwives interviewed are EmOC certified by the Ministry of Health.
WHO categorizes a BEmONC facility by determining if all signal functions were performed in the last three months.6 Every midwife who assisted with deliveries administered uterotonic drugs within the last three months. Eleven (68.8%) administered parenteral antibiotics, nine (56.3%) removed retained products, eight (50.0%) performed a manual removal of placenta, while only five (31.3%) administered parenteral
anticonvulsants. Assisted vaginal delivery and newborn resuscitation was assessed during a six-month duration and not included in Table 4. Additionally, midwives were given a questionnaire on forty-five obstetric skills, inquiring whether they were conducted in the last six months and if the practitioner felt confident in performing that function. Skills varied for normal assessments, treating abnormal cases, and BEmONC skills. While many midwives reported that they had not conducted numerous functions in the last six months, they claimed to feel confident in performing them.
6 World Health Organization (WHO). 2009. Monitoring Emergency Obstetric Care: a Handbook. WHO
Press, Geneva, Switzerland.
Table 3. Midwife EmOC Education (N=17) # %
EmOC certified 12 70.6
Incomplete EmOC training 5 29.4
Table 4. BEmOC Signal Functions Performed in Last Three Months (N=16)
# %
Administered parenteral antibiotics 11 68.8
Administered uterotonic drugs 16 100.0
Administered parenteral anticonvulsants
5 31.3
Performed manual removal of placenta
8 50.0
Remove retained products 9 56.3
Table 5. Obstetric Skills Performed in Last Six Months & Confidence Levels (N=16) # %
Managed bleeding in early pregnancy 12 70.6 Confident in managing bleeding in early
pregnancy 14 87.5
Manage bleeding in late pregnancy and labor 7 43.8
Confident in managing bleeding in late pregnancy and labor
15 88.2
Manage pre-eclampsia 11 68.8
Confident in managing pre-eclampsia 14 87.5
Manage fever before delivery (amnionitis) 10 62.5
Confident in managing a fever before delivery (amnionitis)
15 93.8
Performed vacuum delivery† 8 57.1
Confident in performing vacuum deliveries† 6 42.9
Performed newborn resuscitation 9 56.3
Confident in performing newborn resuscitation 15 93.8 †Statistic based off of 14 midwives

8
From the qualitative interviews, midwives listed multiple barriers to providing BEmONC. The most common theme found was the lack of support. It was frequently linked to the limited number of health professionals (obstetricians and midwives) available to assist with abnormal obstetric cases. Another issue that they presented was inconsistencies in the supervision styles of contract physicians. Some midwives reported that facility policies determining whether functions could be independently managed by a midwife changed under different physicians depending on their obstetric experience level. Midwives claimed to have referred numerous obstetric cases that they were trained in and felt confident in managing because the supervising physician was not confident of his or her skills. The second most common theme identified was inadequate equipment or supplies to provide BEmONC functions. Many facilities reported having requested replacement equipment, but are subject to lengthy wait periods. The third barrier commonly listed was limited emergency transportation. Reasons behind this barrier included a limited number of emergency vehicles available, limited access due to poor road conditions, and inadequate fuel availability. When asked about their ability to provide quality of BEmONC during home deliveries, midwives overall reported limited ability. Most midwives reported transferring patients to a facility prior to providing BEmONC. They reported that intravenous fluids would be placed in the home if necessary; however, all other complications are treated at a health facility. Additionally, when midwives were requested to provide skilled assistance during a normal, early-stage home delivery, they consistently transferred the patient to a facility to give birth. Very few “home births” assisted by facility staff actually delivered within the home. When asked how the midwives manage obstetric complications during the prenatal period, the most common response was a list of diverse factors taken into consideration to develop a care plan. Midwives commonly listed acuity, gestation, previous medical history, and geographic location of the patient’s home as factors. Few mentioned resources used to develop a birth plan, which included team approach or EmOC materials. Midwives also listed various care strategies, such as providing inpatient care, additional consultations, and requesting pregnant mothers in their ninth month gestation to stay within a short distance from a health facility. However, no universal protocol was mentioned. Almost all midwives requested continuation of EmONC training, either initial certification or refresher training. One midwife received EmOC training as early as 2006, and many requested routine updates to ensure skill quality. Equipment and Supplies The original equipment and supply questionnaire included 172 items, with sections on facility, equipment and supplies, staff transportation, referral system, laboratory equipment, infection prevention, basic medical items and supplies, records and forms, registries, drugs, and delivery equipment. Items pertinent to general facility condition

9
and performing direct BEmONC functions were reviewed first. Some items were not assessed due to a lack of time or availability of staff during site visits. These findings show that the general conditions of the district and sub-district facilities were not ideal for providing high quality BEmOC. Only the Maubisse Referral Hospital had access to electricity 24 hours a day. Three facilities had access to electricity during limited hours of the day. Two facilities only had electricity for specific electronics. One facility, Alas Maternity House, had no electricity. The only facilities with a reliable water supply directly to the clinic were the Maubisse Referral Hospital and the Ainaro CHC. Additionally, only three facilities had an oxygen supply (Maubisse Referral Hospital, Ainaro CHC, Prince of Monaco II Maternity House). See Annex 4 for a list of facility conditions and basic medical equipment by facility. World Health Organization policies for managing pregnancy complications were used to develop an abbreviated list of equipment used to perform BEmONC functions (see Annex 6). This list of necessary items was developed from the 2007 WHO provider manual, Managing Complications during Pregnancy and Childbirth: A Guide for Midwives and Doctors.7 This manual is used as a training resource in Timor-Leste. This equipment list does not include basic care management supplies or equipment needed to address complications that may arise while performing BEmONC. This list was used solely for analysis of BEmONC equipment. Equipment within Timor-Leste varies slightly from the WHO recommendations, so some variation exists. Table 6 depicts the percentage of equipment currently available at facilities during the 2012 site visit to complete BEmONC functions. See Annex 6 for a breakdown of equipment by BEmONC function and facility. Table 6 shows that no facilities had a complete set of equipment to provide high quality care. Rural sub-districts of Turiscai, Alas, and Hatudu lacked the most equipment.
7 World Health Organization (WHO). 2007. Managing Complications in Pregnancy and Childbirth: A guide for midwives and doctors. WHO Press, Geneva, Switzerland.
Table 6. Basic EmOC Equipment and Supplies (percentage available)
Maubisse Hospital
Monaco Maternity House
Turiscai Maternity House
Alas Maternity House
Fater-berlihu Maternity House
Ainaro Maternity House
Hatudu Maternity House
1 Admister parenteral antibiotics 100.0% 100.0% 81.8% 81.8% 90.9% 100.0% 90.9%
2 Administer uterotonic drugs (i.e. parenteral oxytocin) 91.7% 91.7% 66.7% 75.0% 83.3% 91.7% 91.7%
3 Administer parenteral anticonvulsants for pre-eclampsia and eclampsia 81.8% 81.8% 63.6% 54.4% 63.6% 81.8% 72.7%
4 Manually remove the placenta 100.0% 87.5% 62.5% 87.5% 93.8% 100.0% 87.5%
5 Remove retained products (vacuum extraction, dilation and curettage)
90.0%, 93.8%
90.0%, 87.5%
60.0%, 62.5%
65.0%, 81.3%
75.0%, 68.8%
90.0%, 93.8%
55.0%, 62.5%
6 Perform assisted vaginal delivery (i.e. vacuum extraction) 83.3% 83.3% 33.3% 50.0% 50.0% 100.0% 33.3%
7 Perform basic neonatal resuscitation (i.e. with bag and mask) 100.0% 100.0% 75.0% 87.5% 100.0% 100.0% 0.0%
Based on World Health Organization's provider manual "Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors"

10
Conclusion In 2002, the National Planning Committee elegantly summarized the state of maternal health, stating that “women bear an unacceptable burden of mortality and morbidity, with maternal mortality rates at 350-800 per 100,000 live births”.8 Eight years later, women continue to be subject to this heavy burden. Since 2002, emergency obstetric services have improved. However, Ainaro and Manufahi facilities provide incomplete basic services, especially at rural sub-district sites. Identifying and targeting individual facility weakness is the most effective strategy to increasing district BEmONC capacity.9,10, This assessment found many of the limitations listed in the 2008 UNFPA EmOC Needs Assessment still exist and require additional focus and resources. The framework on the right is Columbia University’s “Averting Maternal Death and Disability” (AMDD) tool to measure EmOC implementation.11 This building block framework breaks down how each activity relates to the others and in what sequence they must be initiated. The bottom two rows are the foundation to providing sustainable, high quality emergency obstetric care and make-up the preparation stage. AMDD and UNFPA agree that developing strong health systems precludes EmONC quality improvement interventions.12 Focusing on the framework’s bottom level: while the health facilities have made improvements in renovations, facility setup, supplies and equipment since the 2008 EmOC assessment, many weaknesses are still evident. Additional effort is still needed to improve facility conditions, equipment maintenance, supplies and equipment, and improve the accuracy of data collection. Equipment and supplies were well stocked and functioning in the Maubisse Referral Hospital. However, other facilities are subject to long waiting periods for equipment and supply replacement and restock. Basic medical equipment needed for care of routine and emergency conditions were missing from numerous facilities, especially the most remote sites. Better maintenance and supply of equipment is needed to detect and confirm early obstetric complications.
8 National Planning Committee. 2002. National Development Plan. Dili, East Timor. 9 Freedman, L. P., Graham, W. J., Brazier, E., Smith, J. M., Ensor, T., Fauveau, V., Themmen, E., Currie, S., Agarwal, K. 2007. Practical lessons from global safe motherhood initiatives:time for a new focus on implementation. Lancet, 370:1383–91. 10 Averting Maternal Death and Disability. 2006. Averting Maternal Death and Disability Program Report 1999-2005. Columbia University, New York, USA. 11 Campbell, O.M.R. and Graham, W. J. 2006. Strategies for reducing maternal mortality: getting on with what works. Lancet, 368: 1284–99. 12 Freedman et al. 2007.

11
These first-layer activities within the tool support the subsequent preparation stage layer. Routine refresher trainings on EmONC and safe motherhood need to be integrated into health professional’s careers. Increasing staffing would provide midwives support to provide BEmONC in rural sites during 24 hours per day. Team building trainings and exercises would increase inter-professional approaches and quality of care. Using the AMDD’s framework shows a need for the MOH to focus on improving health system issues before BEmONC quality can be fully addressed. While working on these foundational issues, the MOH can plan how to augment the first layer of the service delivery stage, consisting of continual readiness and constant emergency obstetric care. Obstetric complications at sub-district facilities are infrequent and these cases are often referred to the district or referral hospital level based on acuity. With current levels of health care utilization, remotely placed midwives lack a sufficient number of opportunities to practice their BEmONC skills. Recommendations Many interventions addressing maternal mortality were integrated into the national plan from the Safe Motherhood initiative. Community outreach efforts, such as SISCa (Integrated Community Health Services) and PSFs increased the use of health facility and trained staff services. While quality of care has been supported through specialty trainings and supervision visits, further health system improvements are needed to provide a universal standard of care across facility levels. Globally, there has been an increased focus on the implementation of interventions with evidence-based scale-up strategies.13 Due to inconsistencies in facility conditions, supplies, service availability, and staffing, basic system level factors at the district and sub-district level health facilities have to improve as a condition of expanding EmOC services. Additionally, by addressing system level issues, benefits will occur across a broad spectrum of health conditions including preventive care. The following is a list of immediate system level changes suggested and long-term recommendations focusing on EmOC. Recommendations were developed from assessment results, a literature review, and interviews with field experts. Immediate Recommendations
1. Ensure that the facilities have the basic equipment necessary to provide care management. Revamp the MOH equipment and supplies request process to decrease waiting periods. Frequent equipment allotment should be anticipated and distributed in a timely manner. Equipment must be available for complications to be detected early and appropriate managed.
2. Ensure staff is knowledgeable in equipment maintenance, i.e. sterilization of manual suction machine. Supervising staff should be responsible for ensuring equipment maintenance and standards of care. Adequate care of equipment increases its longevity and quality of care.
13 Freedman et al. 2007.
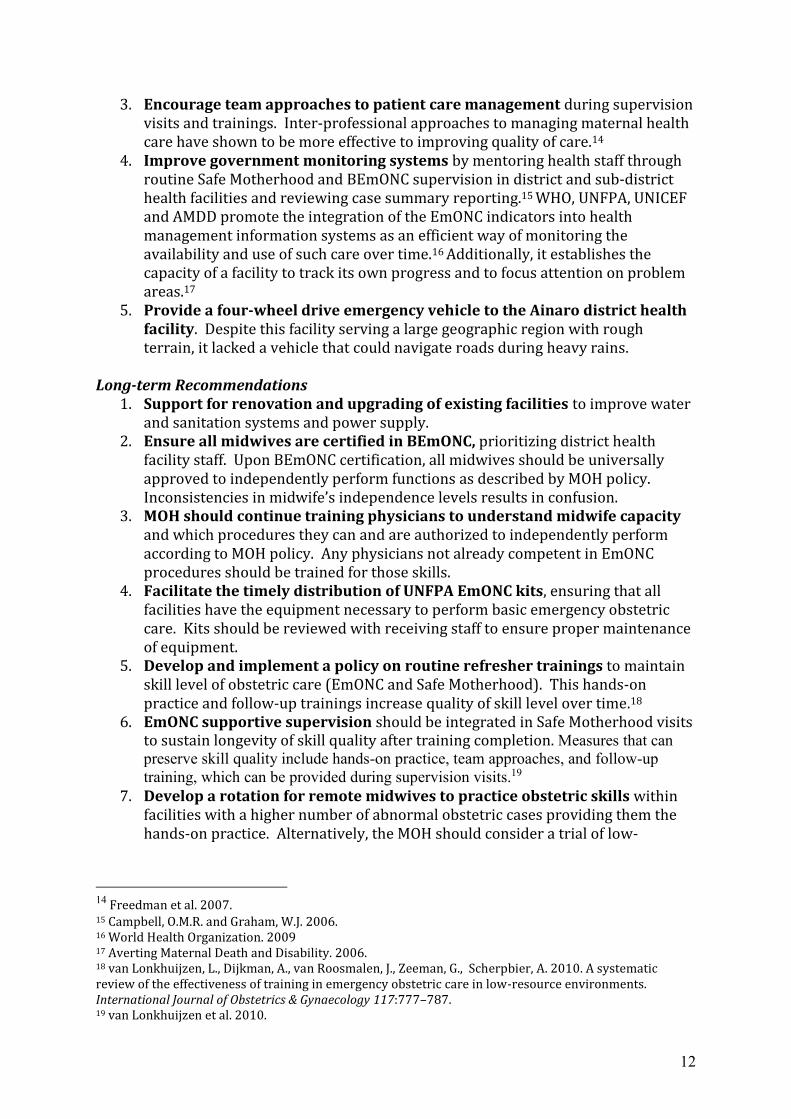
12
3. Encourage team approaches to patient care management during supervision visits and trainings. Inter-professional approaches to managing maternal health care have shown to be more effective to improving quality of care.14
4. Improve government monitoring systems by mentoring health staff through routine Safe Motherhood and BEmONC supervision in district and sub-district health facilities and reviewing case summary reporting.15 WHO, UNFPA, UNICEF and AMDD promote the integration of the EmONC indicators into health management information systems as an efficient way of monitoring the availability and use of such care over time.16 Additionally, it establishes the capacity of a facility to track its own progress and to focus attention on problem areas.17
5. Provide a four-wheel drive emergency vehicle to the Ainaro district health facility. Despite this facility serving a large geographic region with rough terrain, it lacked a vehicle that could navigate roads during heavy rains.
Long-term Recommendations 1. Support for renovation and upgrading of existing facilities to improve water
and sanitation systems and power supply. 2. Ensure all midwives are certified in BEmONC, prioritizing district health
facility staff. Upon BEmONC certification, all midwives should be universally approved to independently perform functions as described by MOH policy. Inconsistencies in midwife’s independence levels results in confusion.
3. MOH should continue training physicians to understand midwife capacity and which procedures they can and are authorized to independently perform according to MOH policy. Any physicians not already competent in EmONC procedures should be trained for those skills.
4. Facilitate the timely distribution of UNFPA EmONC kits, ensuring that all facilities have the equipment necessary to perform basic emergency obstetric care. Kits should be reviewed with receiving staff to ensure proper maintenance of equipment.
5. Develop and implement a policy on routine refresher trainings to maintain skill level of obstetric care (EmONC and Safe Motherhood). This hands-on practice and follow-up trainings increase quality of skill level over time.18
6. EmONC supportive supervision should be integrated in Safe Motherhood visits to sustain longevity of skill quality after training completion. Measures that can preserve skill quality include hands-on practice, team approaches, and follow-up training, which can be provided during supervision visits.19
7. Develop a rotation for remote midwives to practice obstetric skills within facilities with a higher number of abnormal obstetric cases providing them the hands-on practice. Alternatively, the MOH should consider a trial of low-
14 Freedman et al. 2007. 15 Campbell, O.M.R. and Graham, W.J. 2006. 16 World Health Organization. 2009 17 Averting Maternal Death and Disability. 2006. 18 van Lonkhuijzen, L., Dijkman, A., van Roosmalen, J., Zeeman, G., Scherpbier, A. 2010. A systematic review of the effectiveness of training in emergency obstetric care in low-resource environments. International Journal of Obstetrics & Gynaecology 117:777–787. 19 van Lonkhuijzen et al. 2010.

13
technology simulation-based EmOC practice, such as that available at the University of Washington in the PRONTO project.
8. Integrate prenatal care into Maternity Houses to facilitate record sharing and continuity of care. Midwives practicing prenatal care should be based out of the maternity houses.
9. Increase resources to transport patients, ensuring that timely care is accessible. Increase fuel supply for emergency transportation and primary care SISCa’s. Monitor the referral transportation system to ensure that an appropriate number of vehicles are available to serve population needs.

14
Annex 1: Government Health Facilities providing Emergency Obstetric Care Services in East Timor Basic EmOC Service Facilities; Functioning in 2008 1. Los Palos District CHC 2. Viqueque District CHC 3. Manatuto District Maternity House 4. Same Prince of Monaco II Maternity House Bacis EmOC Service Facilities; Planned for 2015 1. All district and sub-district maternal health facilities Comprehensive EmOC Service Facilities; Functioning in 2012: 1. Baucau Referral Hospital 2. Maubisse Referral Hospital 3. National Dili Hospital

15
Annex 2: Midwife Assessment Supplement Please answer the following questions about EmOC in your health facility?
What do you perceive as barriers to providing quality basic emergency obstetric care?
How well can you provide basic emergency obstetric care while managing home births?
Are special care plans used for pregnant women with known complications?
Comments

16
Annex 3: Service Availability and Staffing Table
Service Availability & Staffing
Monaco Maternity
House
Turiscai Maternity
House
Alas Maternity
House
Fater-berlihu
Maternity House
Maubisse Referral Hospital
Ainaro Maternity
House
Hatudu Maternity
House
Immediate Service Availability During 24 Hours a Day
Labor and delivery service by midwife √ - - - √ - -
Labor and delivery services by other health staff √ - - - √ √ -
EmOC medications √ x √ √ √ √ √
Laboratory services - - - √ √ - -
Staffing
Midwives Total 6 1 1 3 5 3 1 Present 24 hours per day 1 0 0 0 2 0 0 EmOC certified 4 0 2 2 5 2 1
Pharmacist Total 1 1 1 1 3 2 x Present 24 hours per day 0 0 0 0 1 0 x
Lab technician Total 1 1 1 1 4 1 1 Present 24 hours per day 0 0 0 1 1 0 0
Midwife Assistant or Nursing Assistant Total 0 1 0 0 6 x x Present 24 hours per day 0 0 0 0 x x x
Physician Total 5 x x x 4 2 x Present 24 hours per day 0 x x x x 0 x
Ambulance Driver Total 2 1 1 1 x 2 1 Present 24 hours per day 1 0 0 0 x 2 0
Cleaner Total 3 1 1 1 17 5 1 Present 24 hours per day 0 0 0 0 2 0 0
x= not reported by facilities

17
Annex 4: Facility Condition and Basic Equipment Supply
Facility condition
Clean water supply
directly inside clinic
Electricity and/or power source Radiant warmer/work
surface for newborn
resuscitation
Operating oxygen
source with flow meter
Clock with second hand
visible from the delivery table
Working refrigerator
24 hrs daily
Only a few hours daily
Only for specific appliances
Prince of Monaco II Maternity House - - √ - √ √ √ √
Turiscai Maternity House - - - √ - - - √
Alas Maternity House - - - - - - - √
Faterberlihu Maternity House - - - √ √ - - √
Maubisse Referral Hospital √ √ - - √ √ √ √
Ainaro CHC √ - √ - √ √ √ √
Hatudo CHC - - √ - - - - -
Basic Equipment
Blood pressure
apparatus
Stethoscope
Therm -o- meter
Ambubag with mask Scales Plastic or
rubber aprons
Povidone iodine 10% antiseptic (Betadine)
Sterile gloves (fitted) Adult Fetal Adult
Neo-nates Adults Infant
Prince of Monaco II Maternity House √ √ √ - √ √ √ √ √ √ √
Turiscai Maternity House - √ √ √ - √ √ √ √ √ √
Alas Maternity House - √ √ - √ - - √ √ √ √
Faterberlihu Maternity House √ √ √ √ - √ √ √ √ √ √
Maubisse Referral Hospital √ √ √ √ √ √ √ √ √ √ √
Ainaro CHC √ √ √ √ √ √ √ √ √ √ √
Hatudo CHC √ √ √ √ - - √ - √ √ √

18
Annex 5: Midwife Knowledge Survey
Obstetric skills (last six months)* #
Total Inter-
viewed Managed bleeding in early pregnancy 12 16 Confident in managing bleeding in early pregnancy 14 16 Manage bleeding in late pregnancy and labor 7 16 Confident in managing bleeding in late pregnancy and labor 15 16 Manage pre-eclampsia 11 16 Confident in managing pre-eclampsia 14 16 Made a referral for eclampsia 6 16 Confident in referring eclampsia cases 13 16 Managed a fever before delivery 10 16 Confident in managing a fever before delivery 15 16 Managed a fever after delivery 9 16 Confident in managing a fever after delivery 14 16 Assessed the fetal position 12 12 Confident in assessing fetal position 12 12 Assessed progress of labor 12 12 Confident in assessing labor progress 12 12 Use a partograph correctly & completely up to phase 4 14 16 Confident in using a partograph 16 16 Managed a normal labor 12 12 Confident in managing a normal labor 12 12 Managed abnormal early labor 13 15 Confident in managing abnormal early labor 14 15 Managed abnormal active labor (first stage) 11 16 Confident in managing abnormal active labor (first stage) 15 16 Managed abnormal active labor (second stage) 11 16 Confident in managing abnormal active labor (second stage) 7 16 Managed abnormal active labor (third stage) 7 16 Confident in managing abnormal active labor (third stage) 14 16 Induced labor 11 16 Confident in inducing labor 13 16 Managed a normal birth 12 12 Confident in managing a normal birth 12 12 Performed vacuum delivery 8 16 Confident in performing a vacuum delivery 6 16 Performed forceps delivery 1 16 Confident in performing forceps delivery 1 16 Removed of placenta 8 12 Confident in removal of placenta 12 12 Performed manual vacuum aspiration in last 6 months 11 14 Confident in performing manual vacuum aspiration 13 16 Recognized breech position 12 16 Confident in identifying breech position 12 16 Managed prolapsed umbilical cord 6 16 Confident in managing a prolapsed umbilical cord 5 16
Managed malaria during labor & delivery 8 12
Confident in managing malaria during labor & delivery 12 12
Performed an amniotomy 12 15

19
Confident in performing an amniotomy 13 15 Sutured an episiotomy with absorbable stitches 12 14 Confident in suturing an episiotomy 14 14 Repaired first degree episotomy tear 12 14 Confident in repairing first degree episiotomy tears 14 14 Repaired second degree episiotomy tear 10 14 Confident in repairing second degree episiotomy tears 10 14 Repaired third degree episiotomy tear 3 14 Confident in repairing third degree episiotomy 3 14 Repaired a cervical tear 5 14 Confident in repairing a cervical tear 7 14 Performed maneuvers for shoulder dystocia 9 16 Confident in performing maneuvers for shoulder dystocia 16 16 Managed a twin delivery 9 16 Confident in managing twins deliver 16 16 Performed manual removal of placenta 10 14 Confident in manual removal of placenta 11 12 Performed curettage or exploration 9 16 Confident in performing a curettage or exploration 13 16 Perform bimanual compression 14 16 Confident in performing a bimanual compression 14 16 Performed abdominal aortic compression in last 6 months 3 16 Confident in performing abdominal aortic compression 12 15 Do postpartum care visits at day 1,3,7 (BSP) & day 3, 7 and week 6 (lisio)
5 5
Confident in postpartum care 5 5 Performed an IUD insertion after delivery or abortion 4 4 Confident in inserting IUD 4 4 Provided contraception pills (COC/POP) 4 4 Confident in providing contraception pills 4 4 Injected depo-provera 4 4 Confident in injecting depo-provera 4 4 Inserted norplant implant 2 3 Confident in inserting norplant 3 3 Performed newborn resuscitation 9 16 Confident in performing newborn resuscitation 15 16 Conducted rapid initial assessment for emergencies 13 16 Confident in conducting rapid initial assessment for emergencies 13 16 Managed shock from bleeding 10 16 Confident in managing shock from bleeding 15 16 Managed shock from sepsis 13 16 Confident in managing shock from sepsis 13 16 Implemented infection prevention measures 13 13 Confident in implementing infection prevention measures 13 13

20
Annex 6: Equipment List to Perform Basic Emergency Obstetric Care Services by Facility (Developed from the WHO provider manual.)
BEmOC Signal
Functions and their
Equipment According to
WHO standards
Monaco Maternity House
Turiscai Maternity House
Alas Maternity House
Fater-berlihu Maternity House
Maubisse Referral Hospital
Ainaro Maternity House
Hatudu Maternity House
Administer parenteral antibiotics
Ampicillin 1 gram/vial √ - √ √ √ √ √
Gentamicin 80mg/ampule √ √ - √ √ √ √
Metronidazole 500mg/vial √ √ √ √ √ √ √
IV tubing √ √ √ √ √ √ √
IV cannula g16 and/or g20/22/24/28 √ √ √ √ √ √ √
Ringer's Lactate √ √ √ √ √ √ √
Normal saline 0.9% √ - √ √ √ √ √
Sterile gloves √ √ √ √ √ √ √ Sterile cotton or gauze √ √ √ √ √ √ √
Ring forceps √ - - - √ √ - Povidone iodine 10% Antiseptic (Betadine) √ √ √ √ √ √ √
Administer uterotonic drugs (i.e. parenteral oxytocin)
Oxytocin 10 Units/ampule - √ √ - √ √ √ Methylergometrine 0.2mg/ampule √ - - √ √ √ √
Salbutamol 4mg/tablet √ √ √ √ √ √ √ Salbutamol 1mg/ampule √ - - √ - - √
IV tubing √ √ √ √ √ √ √ IV cannula g16 and/or g20/22/24/28 √ √ √ √ √ √ √
Ringer's Lactate √ √ √ √ √ √ √ Normal saline 0.9% √ - √ √ √ √ √
Sterile gloves √ √ √ √ √ √ √
Sterile cotton or gauze √ √ √ √ √ √ √
Ring forceps √ - - - √ √ -
Povidone iodine 10% Antiseptic (Betadine) √ √ √ √ √ √ √

21
Annex 6: Continued - Equipment List to Perform BEmOC by Facility BEmOC Signal
Functions and their
Equipment According to
WHO standards
Monaco Maternity
House
Turiscai Maternity
House
Alas Maternity
House
Fater-berlihu
Maternity House
Maubisse Referral Hospital
Ainaro Maternity
House
Hatudu Maternity
House
Administer parenteral anticonvulsants for pre-eclampsia and eclampsia Magnesium sulfate 50% solution √ √ - - √ √ √ Magnesium sulfate 20% solution - √ - - - - - Diazepam 10mg/2ml √ - √ √ √ √ √ Calcium gluconate 10% - - - - √ - - IV tubing √ √ √ √ √ √ √ IV cannula g16 and/or g20/22/24/28 √ √ √ √ √ √ √ Sterile gloves √ √ √ √ √ √ √ Sterile cotton or gauze √ √ √ √ √ √ √ Ring forcepts √ - - - √ √ - Povidone iodine 10% Antiseptic (Betadine) √ √ √ √ √ √ √ Blood pressure apparatus √ - - √ √ √ √
Manually remove the placenta Diazepam 10mg/2ml √ - √ √ √ √ √ Ampicillin 1 gram/vial and Metronidazole 500mg/vial √ - √ √ √ √ √ Umbilical clamp (artery clamps) √ √ √ - √ √ √ Sterile gloves √ √ √ √ √ √ √ Plastic or rubber aprons √ √ √ √ √ √ √ Oxytocin 10 units - √ √ √ √ √ √ Normal saline 0.9% √ - √ √ √ √ √ Ringer's Lactate √ √ √ √ √ √ √ IV tubing √ √ √ √ √ √ √ IV cannula g16 and/or g20/22/24/28 √ √ √ √ √ √ √ Sterile gloves √ √ √ √ √ √ √ Sterile cotton or gauze √ √ √ √ √ √ √ Povidone iodine 10% Antiseptic (Betadine) √ √ √ √ √ √ √ Ergometrine 0.2 mg IM or prostaglandins Medicine not included on Question- naire
Ovum forceps - - - √ √ √ - Wide curette (Curette small, medium, postpartum) √ - √ √ √ √ - Blood pressure apparatus √ - - √ √ √ √

22
Annex 6: Continued - Equipment List to Perform BEmOC by Facility BEmOC Signal
Functions and their
Equipment According
to WHO standards
Monaco Maternity
House
Turiscai Maternity
House
Alas Maternity
House
Fater-berlihu
Maternity House
Maubisse Referral Hospital
Ainaro Maternity
House
Hatudu Maternity
House
Remove retained products (i.e. vacuum extraction, dilation and curettage) Vacuum extraction
MVA syringe √ √ - √ √ √ -
MVA adaptors for size 6,7,8,9,10 √ - - √ √ √ -
Paracetamol 500mg/ tablet √ √ √ √ √ √ √
Oxytocin 10 Units/ ampule - √ √ √ √ √ √
IV tubing √ √ √ √ √ √ √
IV cannula g16 and/or g20/22/24/28 √ √ √ √ √ √ √ Ringer's Lactate √ √ √ √ √ √ √
Normal saline 0.9% √ - √ √ √ √ √
Sterile gloves √ √ √ √ √ √ √
Sterile cotton or gauze √ √ √ √ √ √ √
Ring forceps √ - - - √ √ -
Povidone iodine 10% Antiseptic (Betadine) √ √ √ √ √ √ √
Vaginal speculum or vaginal retractor √ √ √ - √ √ √
Ring or sponge forceps √ - - - √ √ -
Cannulae size 6,7,8,9,10,12 √ √ - √ √ √ - Curette: small, medium, postpartum √ - √ √ √ √ -
Vulsellum or single-toothed tenaculum √ - √ √ √ √ -
Small bowl √ √ √ √ √ √ √
Dilators - - - - - - -
Dilation and Curettage
Oxytocin 10 units IM - √ √ √ √ √ √
IV tubing √ √ √ √ √ √ √ IV cannula g16 and/or g20/22/24/28 √ √ √ √ √ √ √
Sterile gloves √ √ √ √ √ √ √
Sterile cotton or gauze √ √ √ √ √ √ √
Ring forceps √ - - - √ √ - Povidone iodine 10% Antiseptic (Betadine) √ √ √ √ √ √ √
Vaginal speculum OR vaginal retractor √ √ - - √ √ √
Povidone iodine 10% Antiseptic (Betadine) √ √ √ √ √ √ √
Ring or sponge forceps √ - - - √ √ - Vulsellum or single-toothed tenaculum √ - √ √ √ √ -
Wide curette √ - √ √ √ √ -
Dilators - - - - - - -
Ring forceps or a large curette √ - - √ √ √ -
Paracetamol 500 mg √ √ √ √ √ √ √

23
Annex 6: Continued - Equipment List to Perform BEmOC by Facility BEmOC Signal
Functions and their
Equipment According
to WHO standards
Monaco Maternity
House
Turiscai Maternity
House
Alas Maternity
House
Fater-berlihu
Maternity House
Maubisse Referral Hospital
Ainaro Maternity
House
Hatudu Maternity
House Perform assisted vaginal delivery (vacuum extraction only since forceps are rarely performed)
Tubings/rubber hose for suction √ - - - √ √ - VE plastic suction cup √ - √ √ √ √ -
Vacuum pump with pressure gauge √ - - - √ √ - Manual pump - - √ √ √ √ - Sterile gloves √ √ √ √ √ √ √ Mayo/episiotomy scissor √ √ - - - √ √
Perform basic neonatal resuscitation (i.e. with bag and mask) Suction machine (manual or electric) √ √ √ √ √ √ - Ambubag for neonates √ √ √ √ √ √ -
Oxygen mask and tubing for neonates √ √ √ √ √ √ - Mask for neonates No.0 √ √ √ √ √ √ - Mask for neonates No.1 √ √ √ √ √ √ - Blankets/linen √ √ √ √ √ √ - Clock with second hand in delivery room √ - √ √ √ √ - Radiant warmer/Work surface for NBR near delivery area √ - - √ √ √ -

24

Annex 2: Liga Inan Telephone Survey Report
Liga Inan Program
Preliminary Results Follow-up Phone Calls with Enrolled Women
from Sub-district Same
August 2013

1
Contents
Summary
Program Background
The Same Sample
Contacting the participants
Table 1: Method of contacting participants
Accessibility
Are women receiving messages?
Table 2: Average number of messages recalled in the past month
versus number of messages sent by system
Ease in accessing the program
Recalling, Understanding and Sharing Message Content
Recalled messages
Assistance to read messages, sharing message content
Participant Evaluation of the Program
Recommendations
Conclusion
HAI would like to thank Jessie Lopez for compiling this report and the Liga Inan Field Officers,
Jacob Fernandes and Madalena Soares, for conducting the interviews.
For more information on the Liga Inan Project, please visit www.ligainan.org or send an
email to [email protected].

2
Summary
Health Alliance International is implementing an mHealth project for pregnant women with Ministry of Health
staff in Manufahi District. This report describes the results of interviews in Same sub-district of the initial
experience of 48 women enrolled in the project, known as Liga Inan. The women enrolled in Liga Inan receive two
text messages a week about healthy behaviors and planning during pregnancy, for delivery, and through six
weeks postpartum. Three-fourths of women were contacted by mobile phone and others at community venues.
Women described positive experiences with the program: 96% of women reportedly found the program easy to
access and 94% were satisfied with the program.
Participants found messages easy to understand and 71% of women said they were able to read messages
independently. Results show that message content is being remembered and 35% of women discussed messages
with others, exposing more people to key health advice.
Although a majority of findings are positive, the survey also revealed the possibility that the program may not be
reaching women as consistently as expected: women can recall receiving only 47% of the messages that were
sent during the previous month. Further investigation will be necessary to determine whether this gap is due to
recall bias, or to some other issue such as undelivered messages through the service provider, Timor Telecom, cell
signal coverage, phones not being turned on for the entire week, or other user error.
Survey results have been essential in understanding barriers women might encounter in accessing the program,
and has highlighted hamlets where access to the program may be more difficult. Comments about the program
were overwhelmingly positive, but some indicate areas that could be improved.
Program Background The Liga Inan (“Mobile Moms”) Program began in September 2011 when Health Alliance International (HAI) was
awarded funding by USAID to implement a maternal and newborn care project in Manufahi District. The program
aims to reduce maternal and neonatal morbidity and mortality by improving health and care-seeking behavior of
pregnant women.
As of 2010, contact between midwives and pregnant women during antenatal care may be inadequate to
reinforce the key health messages that should be provided during pregnancy: only 55% of women were receiving
four or more antenatal care visits1. A knowledge, practice, and coverage survey conducted by HAI in early 2012
indicated that the majority of women could not indentify two or more danger signs during pregnancy or delivery,
nor could they identify many dangers signs during the postpartum period related to their own or their newborn’s
health.
1 2009-10 Timor-Leste Demographic and Health Survey

3
To inform and remind women of key health behaviors during pregnancy and postpartum, Catalpa International
designed an automated service with HAI that would allow the MOH to share important gestation-specific
maternal health messages with mothers twice weekly. From registration through six weeks postpartum, mothers
receive messages relevant to antenatal care, nutrition, importance of delivering with a midwife, danger signs, and
care of the newborn. The Liga Inan program also allows midwives to send messages to pregnant women about
health outreach events (known as SISCa) in the sub-district. To enable communication between pregnant women
and their midwives, a Liga Hau (“Call Me”) was also incorporated to allow mothers to send a messages to their
midwife requesting that the midwife contact them with advice or information.
At the time of this analysis, the Liga Inan Program was only operating in the eight hamlets (suco) of Same Sub-
district: Betano, Daisua, Grotu, Holarua, Letefoho, Rotutu, Tutuluro. The program and enrollment commenced in
Same in February 2013, and an estimated 30% of pregnant women in Same are now registered in the Liga Inan
Program2. Training and enrollment has now commenced in two additional sub-districts of Manufahi, Fatuberliu
and Alas, applying some of the lessons learned from this report.
The Same Sample In order to learn more about the experience of women in this
Program, 50 women were sampled who had enrolled during the
first three weeks of the program (February 20-March 14). These
women were all from the first sub-district to receive the Liga Inan
Program (Same) and were sampled proportionate to the number
of enrollments per suco. To ensure accurate representation of
smaller suco that have fewer enrollments, a few additional
women from Grotu and Tutuluro were included.
Contacting the participants
Two Liga Inan Program Officers attempted to contact each woman on the survey list between 3 April and 25 April
by phone, after women had been enrolled in the program at least one month. If a woman could not be contacted
by mobile phone after three attempted calls on different days and at different times of day, the Program Officers
attempted to contact women via SISCa posts or home visits.
Table 1 shows the number of women from each suco that were sampled and the method in which they were
contacted. Thirty-eight women (76%) were reached by mobile phone, including two husbands who participated in
the interview on behalf of their wives. Ten women (20%) could not be reached by Liga Inan staff on three or more
occasions by mobile and were contacted in person. Of these, five women (10%) were met at SISCa, four women
(8%) on a home visit and one woman was met at Centro Saude Same.
2 Program enrollment data compared to Population Projections for 2013 from the MOH and National Statistics Directorate (2013)
“Thank you Liga Inan Program because you help send health
messages to us.”
Dina, Monaco

4
Table 1: Method of contacting participants
Suco
Women
sampled
Method of contact Unable
to
contact Phone call SISCa Home
CHC
Same
Babulo 8 6 1 1
Betano 6 4 1 1
Daisua 8 3 4 1
Grotu 4 4
Holarua 5 4 1
Letefoho 11 10 1
Rotutu 4 4
Tutuluro 4 3 1
Sub-district
Total
50 38 5 4 1 2
Women from Daisua proved most difficult to reach by mobile phone. Liga Inan staff were unable to contact five
of the eight women from Daisua via phone call, and subsequently four women were met at SISCa and one by
home visit. Staff indicated that women in Daisua are particularly affected by inconsistent mobile phone signal
coverage. This was evidenced during the survey when a majority of phone calls to women in Daisua would divert
to the automated Timor Telecom message stating the mobile was outside of the coverage area. This information
assists to understand why Daisua was most difficult to contact and also issues women in the suco may encounter
with accessing program.
Staff noted that most women and husbands seemed happy to answer questions and discuss their experiences
with Liga Inan staff. Three women were not able to talk for long: one woman was busy with her child, one was not
feeling well and one was grieving the loss of her newborn child.

5
Accessibility The accessibility of the program is measured by
assessing the consistency and ease for women
to access the program and the program to reach
women. Responses have revealed some access
barriers that women encounter from home, and
also with the consistency of the Timor Telecom
service. The percentages given are out of 48
respondents interviewed.
“My second pregnancy is different after Liga Inan’s interest in mothers and
babies. With my first child I only went to the hospital for consultations, but now
with my second child I want to give birth in a health facility because there is
health staff and all equipment.”
Amelia, Holarua

6
Are women receiving messages?
Women were asked when they recalled receiving the most recent message from the Liga Inan service. Thirty
women (63%) said they received a message within the two weeks prior to the interview, nine women (19%) more
than two weeks prior to the interview and eight women (17%) could not identify a time frame. One woman
sampled had not received a message due to the incorrect number being recorded when registering, and one
woman stated she received the same message four times in one day. Although nearly 2/3 of women received one
or more messages close to the time being interviewed, one-fifth of women had not received a message for ‘a
while’.
Table 2 presents findings from survey question ‘How many messages have you received since enrollment?’ and is
then compared against the estimated amount of messages the women should have received in that time.
Estimated messages received were calculated between each woman’s enrollment dates to interview date,
coupled with the knowledge that two messages are sent each week.
Table 2: Average number of messages recalled in the past month versus number of messages sent by system
Suco
Average number of
recalled messages
by women per suco
Average number of
messages expected for
women enrolled per suco
Percentage of
messages received
based on recall
Babulo 4.8 * 7.8 62%
Betano 4.4 * 7.8 56%
Daisua ** 4.3 9.1 47%
Grotu 1.8 * 9.5 19%
Holarua 9.8 10.4 94%
Letefoho 5.2 9.9 53%
Rotutu 5.5 11.5 48%
Tutuluro 5.7 11.3 50%
Sub-district
Same Total 5.2 8.7 60%
* One woman from each of these suco could not recall how many messages they had received since enrolling in
the program. In order to calculate the suco average, each woman’s number of received messages has been
estimated at zero. This is a low estimation and therefore suco Babulo, Betano and Grotu would likely have a
higher average of messages received since registration with the program.
**One woman from Daisua was enrolled using an incorrect number and therefore never received a message.
She is therefore unaccounted for in this tally.

7
Overall, women recalled receiving an average of 5.2 messages in their first month in the Liga Inan program, a low
figure when compared with the expected average of 8.7 per woman. The results vary across suco: in Holarua,
women reported receiving close to the expected number of messages (94% of messages received), while women
in Grotu reported receiving only 19% of messages sent. Women from the other six suco reported receiving
between 47% and 62% of expected messages.
These results require more investigation. If women accurately recalled all messages received, then these figures
suggest that 40% of messages sent were not received by women across the sub-district. The low sub-district
average number of messages received and also one woman’s account of multiple messages received in one day
may suggest that there may be some problems with inconsistent service delivery, unclear messaging during
socialization or enrollment about the number and timing of messages being delivered by the program, or other
household barriers to mobile phone use.
We also suspect that our expectations of accurate recall during the 4-week period prior to our interviews might
have been unrealistic and skewed our results to a lower total than expected. In future assessments, we will
consider shortening the recall period to two weeks to determine whether women have received the expected two
messages a week. If future results stay consistent, however, we will further investigate the cause of these gaps.
Ease in accessing the program
Overall, forty-six women (96%) reportedly found the program easy to access. Additionally, seven women (15%)
provided insight into the barriers they had encountered to receiving the automated phone messages. Three
women’s phones are turned off regularly, two women’s children often delete messages before they can read
them, one woman’s husband takes the mobile when he is away for work and one woman provided the wrong
mobile number when enrolling.
With the exception of the one woman who was registered with an incorrect phone number, the explanations
provided are all barriers in accessing the program that are confronted at the household level. There are ways to
navigate around many of the barriers, such as that women can be informed that messages should arrive on
Mondays and Thursdays. This may encourage women to be attentive of their mobile on days a message is due to
arrive and therefore enable women to access the program more consistently.
During a visit to a SISCa event in Maurem (an area within Suco Daisua) in March, discussions between HAI staff
and enrolled women revealed similar obstacles. Of the five women present at the mobile outreach event who had
enrolled in the LI program a month previously, none had received any messages since registration. Barriers
mentioned included one husband that had dropped their phone in the river after enrollment so it was unusable,
one woman explained that she lives in an area with no signal and due to heavy rains had been unable to charge
her phone that requires a solar charger, and two women live in a location with inconsistent mobile phone
coverage and have to walk approximately one hour to get a signal3. Staff informed the women that messages
should arrive on Mondays and Thursdays and they all agreed to try and access their mobiles on these days.
3 HAI staff notes

8
Recalling, Understanding and Sharing Message Content Women report that information sent to them is being understood, shared and remembered, all of which are
positive signs for the program. Survey findings state that comprehension of message content is high amongst
women, a large majority of who can read messages independently. No women found the messages difficult to
understand, and forty-five women (94%) stated that messages are easy to understand. This is supported by the
high comprehension of message content demonstrated by SMS messages remembered by women.
Recalled messages
One question asked women to recall the last message they had received to determine whether incoming
messages are corresponding with each woman’s estimated week of pregnancy. For the most part it was difficult
to match the answers provided with a message surrounding the estimated week of pregnancy. Understandably,
women did not recall messages exactly as they were received, instead explained what information they
remember and rephrased messages they recalled. All responses provided are consistent with one or more
messages on the SMS list.
Thirty-one women (65%) recalled a message from the Liga Inan SMS list, twenty-eight women recalled a health
message and three women recalled a program related message such as the welcome to program SMS. Nine
women (19%) remembered a message about healthy pregnancy, including sleeping under a mosquito net, not
smoking or drinking alcohol during pregnancy and taking vitamins during pregnancy. Seven women (15%)
recalled a message about danger signs during pregnancy, six women (13%) remembered preparatory messages
for birth, three women (6%) explained the benefits of giving birth in a health facility and one woman (2%) recalled
a message related to newborn health. Two women recalled multiple messages related to healthy pregnancy.
Assistance to read messages and sharing message content with others
The respondents were asked if they require help to read the messages. Thirty-four women (71%) stated they read
messages without assistance. Twelve women (25%) stated they received assistance to read messages: nine
women (19%) had help from their husband/partner, two (4%) from adult members of the family, and one (2%)
from a neighbor. Two women (4%) did not indicate if they received assistance to read messages.
Women were also asked whether they discuss information from messages with other people. Thirty-five percent
of women reported that they had shared the messages they had received from the Liga Inan Program with their
family or neighbors: ten women reported sharing with one other person and an additional seven women (15%)
shared this message with multiple people. Husbands or partners were the most common person with whom
women discussed messages (33%), followed by adult family members (15%), neighbors (4%), and children or
friends.
65% of women recalled one or more messages
15% of women remembered dangers since during pregnancy
19% of women recalled a message about healthy pregnancy

9
Information shared with others included the importance of preparation before birth and the benefits of giving
birth in a health facility where equipment is available and health staff are present. One woman said she gave her
emergency contact details to her neighbor and one woman from Babulo said “I always read messages and explain
to others that have not received the SMS yet”.
Results prove a high number of women read messages independently. This is consistent with 67% Tetum literacy
rate of women in Same with children between 0-23 months of age4. Results also demonstrate that messages are
being shared with others. Discussing information or asking for help to read messages is a positive means of
reinforcing health information and increases the number of people exposed to the key health information.
Another positive result evidenced by the telephone survey is that women are remembering key health
information, a great outcome from the program.
Participant Evaluation of the Program Participant feedback was mostly positive and shows
women are confident with health facilities and
midwives. Forty-six women (96%) were satisfied with
the messages they received and forty-two women
(88%) reported that they have had “no problems with
the service”.
Four women made recommendations, yet only one recommendation to the program was related to the program
itself: one woman asked HAI to include more information about family planning. The remaining three
recommendations, two from Daisua and one from Rotutu, asked for continued support with transport from the
program because they live far from hospitals and Same Vila (these women are referring to the ambulance service
in their sub-district). Five women (10%) expressed concern that their remoteness impacts their ability to access
health care and they urged the program to assist them with accessing transport.
Twenty-two women (46%) commented on the program and all made positive remarks. Nine women (19%) feel
the program supports them to access health staff and facilities for ANC’s or giving birth in a health facility. Six
women (13%) are grateful for the Liga Inan Program because the program “cares for me during pregnancy”. Five
women (10%) appreciate receiving health information and information about facilities being “fully equipped” with
health professionals and resources. One woman is content the program is free to access so she doesn’t use her
own money and one woman is happy the program has put her in direct contact with her midwife.
Interestingly, messages about the benefits of giving birth in a health facility resonated greatly in Daisua. Of eight
women in Daisua, seven women expressed appreciation for the program because it assists them to give birth in a
health facility or recalled the importance of giving birth in a health facility. The consistency of this message is
encouraging given that women in this suco had one of the lowest percentages of message recall: even if they are
not receiving all individual messages, they are clear on one of the most important concepts of this program.
4 HAI KPC Survey 2012
“The Liga Inan Program is a great help for us and has given me information about
giving birth in a health facility.”
Monica, Daisua
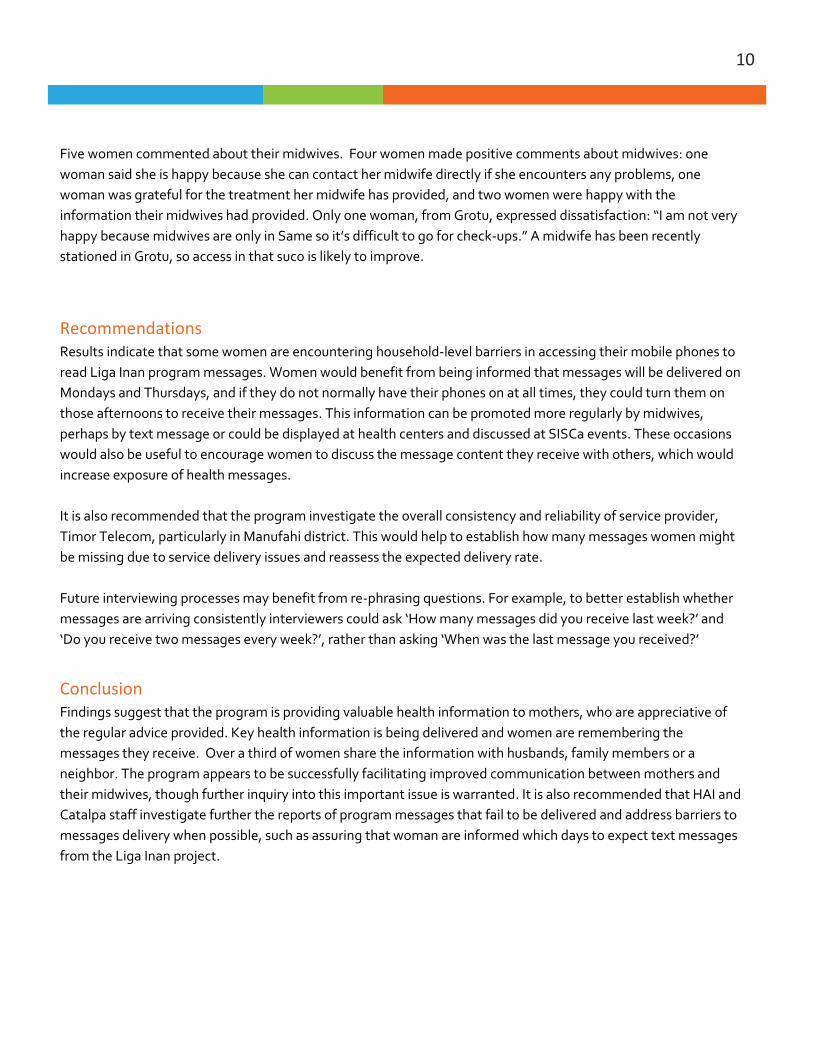
10
Five women commented about their midwives. Four women made positive comments about midwives: one
woman said she is happy because she can contact her midwife directly if she encounters any problems, one
woman was grateful for the treatment her midwife has provided, and two women were happy with the
information their midwives had provided. Only one woman, from Grotu, expressed dissatisfaction: “I am not very
happy because midwives are only in Same so it’s difficult to go for check-ups.” A midwife has been recently
stationed in Grotu, so access in that suco is likely to improve.
Recommendations Results indicate that some women are encountering household-level barriers in accessing their mobile phones to
read Liga Inan program messages. Women would benefit from being informed that messages will be delivered on
Mondays and Thursdays, and if they do not normally have their phones on at all times, they could turn them on
those afternoons to receive their messages. This information can be promoted more regularly by midwives,
perhaps by text message or could be displayed at health centers and discussed at SISCa events. These occasions
would also be useful to encourage women to discuss the message content they receive with others, which would
increase exposure of health messages.
It is also recommended that the program investigate the overall consistency and reliability of service provider,
Timor Telecom, particularly in Manufahi district. This would help to establish how many messages women might
be missing due to service delivery issues and reassess the expected delivery rate.
Future interviewing processes may benefit from re-phrasing questions. For example, to better establish whether
messages are arriving consistently interviewers could ask ‘How many messages did you receive last week?’ and
‘Do you receive two messages every week?’, rather than asking ‘When was the last message you received?’
Conclusion Findings suggest that the program is providing valuable health information to mothers, who are appreciative of
the regular advice provided. Key health information is being delivered and women are remembering the
messages they receive. Over a third of women share the information with husbands, family members or a
neighbor. The program appears to be successfully facilitating improved communication between mothers and
their midwives, though further inquiry into this important issue is warranted. It is also recommended that HAI and
Catalpa staff investigate further the reports of program messages that fail to be delivered and address barriers to
messages delivery when possible, such as assuring that woman are informed which days to expect text messages
from the Liga Inan project.

A Baseline Knowledge, Practices and Coverage Survey
for the Mobile Moms/Liga Inan Program
Extended Report
September 2012
Health Alliance International
Maternal and Newborn Health
and Mobile Phone Utilization in
Manufahi and Ainaro Districts
Annex 3: HAI 2012 Baseline KPC Report

i
Table of Contents
Acknowledgements .............................................................................................................. ii
Summary of findings ........................................................................................................... iii
Background ......................................................................................................................... 1
Methods .............................................................................................................................. 2
Results Summary................................................................................................................. 4
Recommendations ............................................................................................................ 14
Conclusion ......................................................................................................................... 15
List of Tables—English ...................................................................................................... 16
List of Tables—Tetun ........................................................................................................ 18
Tables for Results on Participant Demographics .............................................................. 20
Tables for Results on Maternal and Newborn Health ...................................................... 24
Tables of Results on Family Planning ................................................................................ 38
Tables of Results on Mobile Phone Ownership and Use in Manufahi and Ainaro ........... 44
Tables on Results of SMS Message Preferences in Manufahi District .............................. 50

ii
Acknowledgements
Production of this report required a very large team, both in Timor-Leste and at the Health Alliance International (HAI) headquarters in Seattle, Washington. HAI would like to give a sincere thanks to all the following people who made this report possible:
Research design
Marisa Harrison Susan Thompson
Mary Anne Mercer Mark Micek
Survey team members and supervisors(*)
Adelina Belo Agucao Fernandes
Carlito da Costa Cecilia F. do Carmo
Filomena Mendonca Henrique Amaral
Juliao Soares
Luizinha Soares* Maria Chang
Maria Diana li do Santos Maria Eliza M de Araujo
Marisa Harrison* Melania Madeira Soares
Paulo Vasconcelos*
Petra Wisse* Ponciano Ximenes Belo
Salvador Torrezao* Sergio da Silva
Teresinha Sarmento* Vitoria Neves
Yovita Abuk Bere
Data entry
Barbara J.A. Adelina Soares Julio Maia
Lucio A.X. Borges Health Net and HAI team members
Data analysis
Tina Neogi Marisa Harrison Gabriella Boyle
Report writing and additional support
Susan Thompson Marisa Harrison
Beth Elson Mary Anne Mercer
Health Alliance International would also like to thank:
the Timor-Leste Cabinet for Health Research for their consideration and helpful feedback,
the National Statistics Directorate for their support with Census data,
and the staff from HealthNet Timor-Leste who assisted us in completing this study.

iii
Summary of findings
This survey provided essential information on key program and health indicators for Manufahi and
Ainaro districts and the program area overall (Manufahi and Ainaro Districts combined). Overall, the
majority of women appear to be accessing care at least once during pregnancy, however they do not
appear to be completing all key maternal health behaviors during pregnancy nor are they all receiving
assistance during and after birth. This narrative briefly examines these results, and the tables that follow
reveal a much more detailed picture of maternal and newborn health in all eight subdistricts.
Knowledge and practices during pregnancy
Access to care during pregnancy is high: 91% of women in Manufahi and Ainaro attend one or more
antenatal care (ANC) visits. While this coverage rate varies by subdistrict, all eight subdistricts have
greater than 80% coverage of ANC and most have greater than 90% coverage. This is a very encouraging
result, indicating that midwives have at least one opportunity to deliver key health messages to women
during pregnancy. On average, 72% of women in these districts returned for care at least 4 times
during their last pregnancy. This varies more widely across subdistricts, with Same having the strongest
completion rate (83%) and Turiscai having a very low ANC completion rate (45%).
Percent of women who… Manufahi Ainaro Program
area
Attended one or more ANC visits 91% 91% 91%
Attended four or more ANC visits 77% 67% 72%
Received an estimated date of delivery during antenatal care
74% 96% 85%
Received 2 or more TT vaccinations during last pregnancy
74% 60% 67%
Received any iron supplements during pregnancy
90% 87% 88%
Took intestinal parasite drugs during pregnancy
22% 14% 19%
Recognized 2 or more danger signs during pregnancy
55% 54% 54%
During ANC, women should receive key messages and services such as reminders about their estimated
date of delivery (EDD), anti-parasite treatment, tetanus toxoid vaccinations, and iron supplements. They
also should receive information about danger signs during pregnancy, delivery, and postpartum that help
women identify when they need to seek immediate medical assistance. Results from this survey show
that while most women are attending at least one ANC visit, they are not receiving all the minimum
services throughout their pregnancies.

iv
These results indicate gaps between the relatively high coverage of antenatal care visits and some of the
key health services that should be provided during those visits, such as anti-parasite drugs and health
education messages about danger signs during pregnancy, delivery and the postpartum period.
Health practices surrounding birth
Less than half of women in Manufahi (48%) are supported by a health professional during birth; 32%
of all births occur in a health facility. Fewer women in Ainaro seek a skilled attendant at birth (38%), but
a similar percentage report delivering at a facility (29%).
Key health practices around birth include sanitary treatment before cutting the umbilical cord,
immediate breast feeding, and receiving a post-partum consultation from a midwife within two days of
delivery. Results show that coverage of these behaviors is still low. Coverage of each practice was
higher in Ainaro, however, than in Manufahi.
Percent of women who… Manufahi Ainaro Program
area
Gave birth with a skilled birth attendant 48% 38% 43%
Gave birth in a health facility 32% 29% 31%
Clean cord care 58% 71% 64%
Immediate breastfeeding within 1 hour of delivery
51% 64% 55%
Received postpartum care within 2 days 26% 38% 32%
Recognized 2 or more danger signs in newborns
42% 37% 40%
Child spacing knowledge and practices
Effective child spacing is also important to improving the health of mothers and their children. When
asked for the ideal time period to space their children, approximately 75% reported they thought a
woman should wait 2 or more years, 17% said they should wait a shorter amount of time, and 12%
reported they did not know. Many women in Manufahi reported wanting to wait longer between
births: 43% of women wanted to wait 3 or more years. Only 22% wanted to wait 3 years in Ainaro. This
may be one reason that the contraceptive prevalence rate for women with a child under 2 years of age
was much higher in Manufahi (55%) than in Ainaro (30%).
Mobile phone acceptance and penetration
This survey clearly demonstrates that women have access to phones in these two districts: 69% of
women in Manufahi and 67% in Ainaro have a mobile phone in the home. While some of these
phones were shared among family members, 70% of women in Manufahi and 95% of women in Ainaro
reported that one or more of the household phones belonged to the woman herself. This indicates a
high level of access to phones in the populations of these two districts.

v
Mobile phone use is also high in these two districts. We asked women how often they used their
phones to make phone calls and to send or receive SMS messages. Of women who report access to a
household cell phone nearly all of them (98%) report using the phone to send and receive SMS
messages, and over 72% report sending a text message
once a day or more.
Expected barriers to phone use were examined including
access to cell phone signal coverage, ability to charge
phones, and potentially low levels of literacy. This
survey found none of these would be significant barriers
to a mobile phone project. Among these women, few
reported any difficulties accessing signal: 97% reported
that they either had signal coverage in the home or
within a 5 minute walk. We did not ask this question of
women who did not have phones, so we do not know if
signal coverage is so widespread as this result suggests
or if these results demonstrate that where there is
coverage, phones are subsequently purchased. Most
phones were used at least once a day or kept turned on
to be able to receive calls or messages. While methods
of charging phones varied between use of electricity,
solar chargers, batteries and generators, over two-thirds
of women could charge their phones in their home.
Not surprisingly the survey shows high rates of Tetun language literacy with 68% in Manufahi and 56%
in Ainaro able to speak and read Tetun. However, given the high rate of experience with sending and
receiving text messages (98%) for women who have phones, literacy is not an obstacle to use of mobile
phones for texting. This could be due to the availability of husbands, children, neighbors, and other
family members who are reportedly assisting women to reading Tetun when necessary. Tetun was
almost unanimously (98%) requested as the language to receive health messages (other options
included Portuguese, Indonesian, or local languages).
Mobile phones are not only prevalent, but frequently used tools for communication in this population.
69% of women in Manufahi and
67% in Ainaro have a mobile
phone in the home
Of women who had phones, 97%
reported that they either had
signal coverage in the home or
within a 5 minute walk
72% of women report sending a
text message once a day or more
Tetun was requested by 98% of
women at the language in which
to receive health messages

1
Background
In September 2011, Health Alliance International was awarded funding by USAID to implement a
maternal and newborn care project in two districts of Timor-Leste, Manufahi and Ainaro. The goal of
the Mobile Moms/Liga Inan project is to reduce maternal and neonatal morbidity and mortality by
improving the health and care-seeking behavior of pregnant women. The project will be implemented
over four years from September 30, 2011 to September 30, 2015.
Maternal and newborn mortality continue to be major problems in Timor-Leste: MMR is 557 per
100,000 births and neonatal mortality is 22/1000 live births, as of the 2009/10 DHS. Community
understanding of optimal health behaviors during pregnancy, such as nutritional guidelines, danger signs
of pregnancy, and care-seeking behaviors, is limited. Contact with midwives is limited to antenatal care
(ANC) visits, which do not allow for the repetition and reinforcement of health messages that are most
likely to produce behavior change. Although there has been progress in increasing the rates of skilled
birth attendance since independence in 2002, several problems continue to affect the capacity of the
current system to provide women with high quality skilled care at the time of delivery, particularly when
complications arise. Many birth attendants have not received training in emergency obstetric care
(EmOC). Geographic access to delivery facilities is limited by gaps in both communication and transport
to the facilities. Even with the provision of multiuse vehicles at birthing facilities, many women do not
have transport to get to the facilities once in labor.
Research objectives
This report describes the results of a survey conducted in February and March 2012. The survey was
undertaken for two reasons: 1) to assess the current level of knowledge, practices, and health service
coverage in the community, as well as current information about cell phone ownership and usage
patterns by women who have had a child within the past two years, in order to guide program
development, and 2) to provide baseline data for later program evaluation. The first and last arms of the
project (in box above) will be implemented in both Ainaro and Manufahi districts, while the mobile
phone arm of the project will be implemented in Manufahi only. An additional facility survey was
completed in January and February 2012 to assess facilities’ capacity to deliver EmOC services. The
results of that study are published in another report.
The Liga Inan project will facilitate the maternal continuum of care using three approaches:
Support the national health volunteers (PSF) by training them to deliver health
promotion messages at the household and SISCa level.
Register pregnant women who own or have access to a mobile phone into an automated
system that will deliver weekly health promotional SMS messages based on gestational
stage.
Improve and support the skills of district midwives to provide basic emergency obstetric
care.

2
Methods
Questionnaire development
The survey questionnaire was modeled on USAID’s KPC Rapid Catch Survey, a standardized
questionnaire used worldwide. Additional questions on media and practices surrounding birth were
developed and field tested by HAI staff. The survey includes questions on antenatal care (including
number and timing of visits and tetanus toxoid vaccinations), birthing practices (including skilled birth
attendance and facility deliveries), immediate breastfeeding, postnatal care, child spacing and
contraceptive use, and cell phone ownership and use. Further translation into local languages was done
by interviewers at the time of the interview, although most of the interviews were conducted in Tetun.
Sampling design
The survey was conducted in both Ainaro and Manufahi Districts and employed both stratified and
cluster sampling. The sample was first stratified at the subdistrict level and then 8 Enumeration Areas
(EA) were drawn from each subdistrict using population data from the 2010 Census. A total of 72-77
women were interviewed in each of the 8 subdistricts in Manufahi and Ainaro.
All accessible aldeias within each EA were sampled according to population size with the assistance and
population records from local Chefe Suco. Occasionally an alternate community was chosen when the
first EA was 1) not accessible by road or was further than a 1 hour walk from a road, or 2) the originally
selected aldeia did not contain enough participants. When the former occurred, a backup EA was
randomly selected from within the same suco from a list of accessible EA. When the latter occurred, the
survey team continued with the next nearest aldeia.
After the aldeia was identified, the starting household was determined by one of two methods: counting
all households and randomly selecting one, or the spin-the-bottle method. The former was used in
“urban” settings where households were spread along a number of roads that would make the spin-the-
bottle method difficult to implement. In the second method, supervisors would identify the center of
the community—the area where there were roughly equal number of houses in all directions as
identified by the Chefe de Aldeia—and spin a bottle or pen, with the two ends of the bottle/pen
indicating the directions for team pairs to follow. Each pair, consisting of a supervisor and interviewer or
two interviewers, would follow as straight a line as possible from the bottle site until they reached the
edge of the aldeia. As they walked, they would number the houses within ~15 feet from their path.
When they got to the edge, they would use a currency note to identify the initial house and return to
that house for the start of the surveying process. For both methods, additional houses were identified
as the nearest visible door from the doorway of the initial house.
Selection process and consent
Women were included in the survey if they were between the ages of 15-49 and had a child who was
under 24 months old. If two women fit that description within one household, we interviewed the
mother of the youngest child. If a woman meeting the selection criteria was absent from the house, the
study team would return if possible. Sixteen eligible women were excluded from the survey because

3
they were not at home and not expected to return home. Informed consent was given by each
participant and refusals were rare.
Survey teams
Interviewers came from HAI staff and from two teams from HealthNet Timor-Leste. Managers from both
organizations took the role of team supervisors. Training took place over 4 days in February, with one
day of supervisor training and an additional three days that included supervisors and interviewers. The
training was conducted by Marisa Harrison, Beth Elson, and Paul Vasconcelos, HAI staff, and covered
good interviewing skills, random sampling, confidentiality and consent, and detailed review of the survey
questionnaire. Time was given to practice the survey, including a half day field test on Day 3.
Data Entry and Analysis
Entry was done with EpiInfo 7.0. Preliminary analysis of the frequencies of key questions was conducted
using Stata statistics package.
The results of this survey have been weighted to accommodate for differences in population size or
sample size between clusters, between subdistricts, and between the two program districts. The original
plan called for 8 strata (the subdistricts) and then 8 clusters of 9 women. In a few cases, we weighted
the data for the clusters where all 9 women were not available for interview. This occurred occasionally
due to small population size of some aldeias or inclement weather prohibiting a full day of interviewing.
To calculate district-level coverage rates, we weighted the subdistrict-level findings by subdistrict
population sizes. Program area totals were weighted by the relative size of the two districts.
Health Alliance International would like to
thank all the mothers who participated in this
survey process.

4
Results Summary
Section One: Demographic and Housing Characteristics of Survey Participants
A total of 581 women were interviewed for this survey, 293 in the innovation implementation district of
Manufahi and 288 in Ainaro district. Women were considered eligible if they had a child 0-23 months of
age. The average age of the participants was 27.8 years and all were between the ages of 16 and 45
(Table 1 and Figures 1-3). The average years of schooling was 6.5 with women in Manufahi have more
years of schooling (7) as compared to Ainaro (5.9). The average number of children ever born to survey
participants was 4.1 and was slightly lower in Manufahi (3.7) than in Ainaro (4.4), however this may be
partially due to the slightly older population sample in Ainaro. On average, women in the program area
reported 4 children ever born and 3.7 still living.
The majority of women (83%) reported that they did not work outside the home. There was some
variation between the two districts with 87% of women in Manufahi reporting no work outside the
home compared to 78% in Ainaro. The most frequently reported outside work was harvesting. Eleven
percent of women in Ainaro subdistrict reported salaried positions.
Housing characteristics and available household amenities and assets are an indication of general
socioeconomic status of the survey participants. The survey collected data on roofing and flooring
materials, presence of electricity and ownership of durable goods. Three-fourths of respondents in
Manufahi and Ainaro districts had a sheet iron roof (Table 2). The coastal subdistricts of Alas,
Fatuberliu, and Hatu Udo had higher percentages of natural roofing materials, possibly due to easier
access to natural resources and the cooler household temperatures that natural materials offer in the
warmer coastal climate. Sixty percent of women in Manufahi and 67% in Ainaro reported earthen
floors. Wooden floors were found in traditional style homes, which may not indicate wealth but often
belong to families with higher status in the community. Only 46% of women surveyed in Manufahi and
24% in Ainaro reported having electricity in the home. Ownership of motorized means of transportation
remains low with 18% in the program area having a motorbike and less than 2% owning a car or truck
(Table 3).
Section Two: Maternal and Newborn Health
Women were asked a variety of questions about their knowledge and utilization of health services
across the continuum of care through pregnancy, delivery and the postpartum period.
ANTENATAL CARE
The quality of antenatal care (ANC) can be measured by the qualifications of the provider delivering the
service, the number and frequency of ANC visits, the content of services received and the kinds of
information provided to mothers during this important medical encounter during pregnancy. Women
were asked questions in each of these areas.

5
Almost all women in Manufahi and Ainaro reported seeing a health professional for ANC during their
last pregnancy: Manufahi (93%) and Ainaro (91%) (Table 4). There was variation between subdistricts
with the lowest rates of 83% in Hatu Udo (Ainaro) and 84% in Turiscai (Manufahi). Rates for the
recommended four or more ANC visits during a pregnancy were considerably lower and showed more
variation between the two districts and between subdistricts: 76% of women in Manufahi report having
four or more ANC visits compared to 67% in Ainaro, and that rate was as low as 45% in the subdistrict of
Alas. These rates are higher than the rates of the national health system indicator for four or more ANC
visits, probably because the national indicator requires women to have received these visits as per a set
schedule—one during the first trimester, one during the second, and two during the third with the last
ANC visit occurring during the last month of pregnancy—whereas we measured total number of
reported visits at any point over the course of a woman’s pregnancy.
Location of care
Most women receive their ANC through the government-run health system, which is free. There are
several types of facilities in the government system that offer ANC care: there is one referral hospital in
the subdistrict of Maubisse; Community Health Centers (CHC) are located in each of the eight
subdistricts; Health Posts serve the more remote population; and SISCa (Servisu Integradu de Saúde
Communitaria) or Integrated Community Health Services that are mobile health clinics are carried out
monthly at fixed posts in 442 villages throughout Timor-Leste. SISCas are supposed to be staffed by a
midwife for the provision of ANC, but the degree to which a private space is available and a midwife
present varies considerably. Only 10% of women overall report receiving any ANC at a SISCa, although it
is higher in Manufahi (16%) than in Ainaro (4%) (Table 5). Most women report receiving ANC at the
subdistrict CHC, but this was significantly lower for women in Ainaro (37%) compared to Manufahi
(62%). Thirty-three percent of responses for women in Ainaro included going to a hospital for ANC,
compared to only 14% in Manufahi. However, this was influenced by the 82% of women in Maubisse
who reported they sought ANC at a hospital since there is a referral hospital there. A few women also
reported receiving ANC through home visits, which are not common but do sometimes occur.
Timing of first ANC
Given that the first ANC visit will be the gateway to the Mobile Moms project in Manufahi, it is
important to know when women come in for their first visit. We found that 58% of women in Manufahi
report coming in for their first ANC in their first trimester while only 34% do so in Ainaro (Table 6). Sixty-
one percent of women in Ainaro report waiting until the second trimester to seek ANC care compared to
37% in Manufahi. If women from Manufahi enroll in the Mobile Moms program during their first ANC
visit, most women should receive the full complement of messages, and almost all enrolled women
should receive every message sent during their final trimester.
Services accessed during ANC
To assess the quality of ANC care provided, women responded to questions regarding the specific
services provided during their ANC visits. Women reported high rates of standard ANC practices such as
tracking weight, measuring blood pressure and examining the stomach, with over 97% of women from
both districts reporting that they received these essential services during ANC (Table 7).

6
Having an estimated date of delivery (EDD) is important for families in forming a birth plan, and is an
essential element in ensuring women are receiving gestationally appropriate messages during this
program. Anecdotal evidence has suggested that some women in Timor-Leste have not been receiving
an estimation of their due date from a midwife during ANC, therefore we needed to determine the level
to which women believe they have been given this information. The practice of providing an EDD was
considerably higher in Ainaro (96%) than in Manufahi (74%) (Table 8). The overall lower rate in
Manufahi is primarily because of the significantly lower rate in the subdistrict of Same (64%) as
compared to the other three subdistricts. Further investigation will be conducted in Same and the rest
of Manufahi to determine the extent of refresher training needed on calculating due dates before
project implementation.
Women were asked if they could spontaneously name symptoms during pregnancy that would cause
them to seek immediate care at a health facility, and from whom they learned this information. Slightly
over half of women (54%) could indentify two or more danger signs related to pregnancy (Table 9).
Manufahi and Ainaro were remarkably similar at 54% and 55%, respectively. However, lower rates were
seen in some subdistricts such as Turiscai (Manufahi) at 46% and Maubisse (Ainaro) at 39%.
Tetanus Toxoid (TT) vaccines are provided during pregnancy to prevent neonatal tetanus. Full
protection is provided by two initial doses with a booster dose every ten years, and five doses is
considered to provide lifetime protection. Rates of women receiving two or more TT injections during
their last pregnancy were higher in Manufahi (74%) than Ainaro (60%); however lifetime rates of two or
more TT vaccination are 86% and 82% respectively (Table 10). The subdistricts of Hatubuilico and
Turiscai had the highest rates of women who have never received any TT.
Important components of ANC are the provision of iron tablets and intestinal parasite drugs. The survey
reveals that the majority of women received iron supplementation during pregnancy (Table 11). Hatu
Udo is the only subdistrict where less than 85% responded that they had received any iron supplements.
Over the past few years, however, there has been shortage of iron pills in Timor-Leste. In the year
before the survey many women were given only 7-10 pills per visit, presumably in an effort to ration
stock. In these two districts, only 52% women report taking iron tablets for 90 days or more, with only
45% in Manufahi reporting 90 days or more of iron supplementation compared to 61% in Ainaro. The
survey also reveals that the vast majority of women, 77% in Manufahi and 84% in Ainaro, report they did
not take any intestinal parasite medication during their pregnancy (Table 12). However, it is unclear if
women were in fact provided this drug but did not know its purpose. This finding will be further
investigated and will be part of the text messaging program.
Malaria infection can lead to adverse birth outcomes, including spontaneous abortions, pre-term labor
and low birthweight babies and still birth. In Timor-Leste the primary prevention strategy for malaria
during pregnancy has been the use of ITNs (Insecticide Treated Nets). Seventy percent of women
surveyed reported that they slept under an ITN all or most of the time with slightly more women in
Manufahi (73%) compared to Ainaro (67%). Nineteen percent of the women in the program districts

7
report they never sleep under an ITN. The risk of malaria in the mountainous areas of the program
districts is considered to be lower than in the coastal regions. It is interesting to note, then, that the two
subdistricts with the highest elevation (Turiscai and Maubisse) also have the highest percentage of
women who reported never using a mosquito net (41% and 44% respectively).
Knowledge of danger signs during pregnancy
Approximately three-quarters of women in Manufahi and Ainaro districts reported they heard about
danger signs from a health provider. Five percent of women reported they had learned about danger
signs from the “lisio”, which is a take-home booklet that includes educational material and the health
record for both a woman during her pregnancy and delivery and her child’s immunizations and growth
charts after birth. Twenty-one percent of respondents in Fatuberliu, 17% of respondents in Hatu Udo,
and 12% of respondents from Alas said they had learned about danger signs through their lisios. These
three subdistricts have been receiving HAI support for health promotion activities at SISCa for the past
two years, which have included reminding women to compare messages from their lisios to messages
delivered during SISCa. None of the other subdistricts saw over 5% of women reporting lisios as a
source of knowledge. Six percent reported that they had learned about dangers signs from a
community health worker (or PSF). The percent of women who reported PSF as a source of knowledge
was highest in Alas (15%) and Same (11%). An additional 23% of women reported learning about danger
signs from another source. One half of these ‘other’ responses included women who reported they had
this knowledge already, and the remainder said they had heard of these danger signs from another
person or a family member.
Preparations for birth
There are many important preparations that should be undertaken before birth, such as saving money,
arranging transport to a health facility, contacting health staff to alert them about your preferred
location for delivery, and finding a blood donor in case of emergency. When asked whether they had
done anything to prepare for the birth of their last child, however, the most frequent responses were
that they purchased new clothes for the baby, or purchased other delivery, or baby-related items such
as a thermos for hot water, soap and a basin for washing the baby, or food or clothes for the mother.
The only stage of the birth plan that was mentioned by women was saving money before birth, and then
only 10% of women claimed to have done so. The near absence of planning for transportation presents
a key barrier to having a skilled attendant or reaching a facility at the onset of labor. However, some
survey team members stated they believe this question was not very well understood and may not have
elicited accurate responses.
DELIVERY CARE
Having a skilled health provider present at delivery and a hygienic environment can reduce the risk of
complications and infections that can cause illness or death in the mother or newborn. Skilled birth
attendant (SBA) is defined in this survey as a doctor, midwife or nurse being present at the last delivery.

8
Access to care
Interviews revealed that women can use a variety of methods to contact midwives around the time of
birth (Table 13). Almost half of women (47%) reported that they could contact a midwife by telephone
(theirs or someone else’s), but those rates varied considerably from 6% in Fatuberliu subdistrict to 64%
in Ainaro subdistrict. Thirty percent of women of women said they could send a messenger to the
midwife and 12% of women said they had to go in person to meet the midwife. Eighteen percent of
woman said they had no method with which to contact the midwife around birth. This was highest in
Alas where 40% of women could not contact a midwife for assistance during birth, and lowest in the
more urban subdistricts of Same and Ainaro (8% and 7% respectively). Multiple responses were given by
some women.
Birth attendance
Less than half of women in Manufahi (48%) and only 38% in Ainaro reported delivering with a SBA
during the birth of their last child (Table 14). There was similarly wide variation of reported SBA use
across subdistricts in both Manufahi and Ainaro. In Turiscai, for example, only 16% of women reported
having a SBA compared to 63% in Fatuberliu, and in Ainaro, the rates ranged from a low of 18% in
Hatubuilico to a high of 63% in the subdistrict of Ainaro. Eighteen percent of women reported the
presence of a Traditional Birth Attendant (TBA), or dukun, at their delivery, and 35% of women deliver
with only a family member or friend to assist them.
Essential elements of active management of the third stage of labor include stimulation of uterine
contractions via an injection of an oxytocic drug prior to delivery of the placenta, and manual massage
of the uterus after placental delivery. Only 29% of women received both an oxytocic drug and uterine
massage with slightly higher rates in Ainaro (31%) compared to Manufahi (26%). Overall, 39% of women
reported that they received an oxytocic injection and 46% that they received uterine massage. Both of
these figures are similar to the 43% of women who delivered with a skilled birth attendant.
Facility births
Facility deliveries remain quite low in Timor-Leste. A health facility is defined in this survey as a hospital,
community health center, maternity home (1 in each subdistrict), health post, or a private clinic. Only
32% of women in Manufahi and 29% in Ainaro report going to a health facility for delivery of their
youngest child (Table 15). Of note, in the subdistricts of Turiscai (Manufahi) and Hatubuilico (Ainaro)
only 1% and 7%, respectively of births occurred in a health facility.
Table 16 shows that of those who delivered at a health facility the majority (75% of women in Manufahi
and 53% in Ainaro) reported that they traveled to that facility by ambulance or another MOH vehicle. In
Manuhahi only 2% stated that they walked to the facility, while in Ainaro fully 24% walked to the health
facility for their last delivery. Private car use was very low, and not reported at all in 5 of the 8
subdistricts.
One of several possible barriers to delivery at a facility is the travel time to a health facility as well as the
lack of privately owned and publically operated modes of transportation available in the rural areas.
Table 17 shows the reported travel time to the nearest health facility. Overall 41% said that they could

9
reach a facility for delivery within 30 minutes. Travel times of 30-60 minutes were reported by one-third
of women in Manufahi and by one-fourth of the women in Ainaro.
Knowledge of danger signs during delivery
Given the high rates of home delivery without a skilled attendant is it critical that women know danger
signs associated with a delivery complication. Women were asked to spontaneously list the signs of a
delivery complication that would require immediate medical attention. Overall, about one third of
women in both districts could name two or more danger signs of delivery (Table 24).
Newborn care
Regardless of the birth site or birth attendant, women were asked what instrument was used to cut the
newborn’s umbilical cord. Traditionally the cord is cut using a razor blade, knife, scissors or a piece of
bamboo. “Clean” cord cutting was defined as all women who had a skilled birth attendant or cut the
cord with new razor blade, boiled razor blade (new or used), or boiled scissors. In Manufahi 58% and in
Ainaro 71% of women reported using a clean instrument (Table 18).
Women were asked additional questions about practices related to their newborn immediately
following delivery. Seventy-four percent of women in Manufahi and 69% in Ainaro reported putting
nothing on the umbilical cord before or after it was cut; 9% of women reported applying antiseptic. The
relatively few replies of “other substance” were talcum powder and alcohol (Table 19).
It is recommended that newborns not be bathed for at least 24 hours after delivery to prevent
hypothermia. Drying and wrapping a newborn immediately after birth is an important aspect of
appropriate newborn care. An average of 72% of women reported drying and wrapping their newborn
with very few reporting only drying the infant (1%) or only wrapping (8%). However, 18% reporting
neither drying or wrapping. The extent to which bathing the newborn after birth may have been
practiced by this 18% is not clear.
The provision of eye ointment or drops to prevent eye infections is low in the program area.
Only 10% of women in Manufahi and 20% in Ainaro stated that their newborns received eye
ointment or drops in the first hour after delivery. This indicator requires further attention.
Anecdotally, stock of eye ointment has been low in health facilities in the past year and
midwives may forget to bring it with them when they assist home deliveries.
Breastfeeding
Breastfeeding is nearly universal in Timor-Leste. Interestingly, we found that while only half of women
in Manufahi (51%) and 60% in Ainaro stated they breastfed their infant within the recommended time of
one hour after delivery, 95% of mothers in Manufahi and 88% in Ainaro provided colostrum to their
newborn (Table 20). There appears to be a delay in immediate breastfeeding, but positive association
with colostrum or “susuben kinur”. The only exception seems to be the subdistrict of Maubisse where
only 77% of mothers reported the provision of colostrom.
Exclusive breastfeeding indicates that nothing is given to the infant to drink other than breast milk,
providing no other substance before initiating breastfeeding and providing nothing other than a

10
mother’s milk. The majority of women surveyed reported that they did not feed their newborn anything
before initiating breastfeeding (78%), and most women did not provide any other substances to their
infants in the first month (83%) (Table 21). The most common foods provided to newborns were plain
water or sugar water, and a number of women in Manufahi reported giving their infants another
woman’s breastmilk. Few women reported giving their newborns infant formula. More than 25% of
women in Turiscai, Fatuberliu, and Hatubuilico reported giving something to their newborn before
providing breastmilk, but interestingly two of those subdistricts (Turiscai and Hatubuilico) had the
lowest percentages of children who received any other foods after breastfeeding was started (Table 21).
In the future, it would be useful to examine the rationale for the provision of substances before
commencing breastfeeding, whether due to delayed milk production from the mother or other beliefs,
and the later justification for providing other substances during the first month of life.
POSTPARTUM AND POSTNATAL CARE
A large proportion of maternal and newborn deaths happen within 24 hours of delivery. The first two
days following birth are recognized as an important period for mother and newborn to be checked by a
trained health professional. The adequate provision of postnatal care not only can help reduce
mortality and morbidity among mothers and their babies, but also serves as an ideal time to educate a
new mother on how to care for herself and her newborn. We asked all women if anyone had checked
on her health or her baby’s health after delivery, how long after delivery that check occurred, and who
provided the service.
Postnatal care by a trained professional within two days of the delivery was reported by 26% of women
in Manufahi and 37% in Ainaro (Table 22). One-third of women in both districts reported receiving no
postpartum care at all.
An early newborn care visit by a trained health professional within two days of birth is a critical newborn
health service to avert newborn death and illness. Only a quarter of newborns in the program area
received this important early checkup (Table 23). Rates were lower in Manufahi at 20% compared to
32% in Ainaro. Alarmingly, 44% of newborns in Manufahi never receive a postpartum check.
Surprisingly, the rates of reported postpartum and postnatal care were considerably lower than the
rates of skilled birth attendance (43%), and the reported rates for maternal health checks after delivery
(32%) were higher than the reported rates of health checks for newborns (25%). During many facility
births, these post-delivery consultations are provided while the woman is still recuperating at the
facility, and the coverage rate for facility births (32%) is similar to the percentage of women who
reported receiving postpartum care. Further investigation is needed to determine whether these results
are a consequence of poor health education levels in women regarding what constitutes postpartum
and postnatal care, or whether there is a gap in follow-up by district midwives.
Knowledge of danger signs in the post-partum period
It is important for women to know the danger signs of the postpartum period. This is particularly true
when rates of facility delivery or skilled attendance at birth are low as they are in Timor-Leste. When
asked to name postpartum danger signs for mothers during delivery, on average only half of surveyed

11
women could name two or more danger signs (Table 24). It was higher in Ainaro (58%) compared to
Manufahi (42%). Additionally, only 40% of mothers in the program area could identify two or more
danger signs indicating that a newborn child that would require immediate medical attention (Table 24).
It is interesting to note that knowledge of danger signs for delivery, postpartum, and in newborns are
not consistent within each subdistrict—sometimes knowledge is higher in one of the three categories
than in others. A focused educational campaign should rectify these differences.
Section 3: Family Planning
Access to family planning services can save women’s lives. UNFPA estimates that one in three deaths
related to pregnancy and childbirth could be avoided if all women had access to contraceptive
services. Timorese women surveyed were asked about their knowledge of the benefits of spacing their
pregnancies, contraceptives methods, and their use of specific contraceptives.
Ideal child spacing
When asked about their opinion on how long after the birth of one child a woman should wait before
trying to become pregnant again, 81% of women reported that they should wait at least two years
(Table 25). These results were relatively consistent between the districts. Interestingly, women in
Manufahi wanted to wait longer than women from Ainaro: 43% of women in Manufahi wanted to wait
at least three years whereas 22% of women from Ainaro wanted to wait that long.
Women were asked to about the risks of becoming pregnant too soon after the birth of a child.
Seventy-seven percent of women could identify at least one risk of inadequate birth intervals (Table 26).
The percentage of women who could identify a risk factor was lower in Manufahi (71%) than in Ainaro
(84%). The most commonly reported risk was that it was “bad for the health of the mother and the
baby”. This answer was mentioned by 44% of women overall. However, more specific risks, such as low
birth weight (13%), preterm birth (1%), and miscarriage (2%) were mentioned far less commonly (Table
26).
Knowledge of family planning methods
When women were asked to spontaneously name methods that could be used to space pregnancies,
91% of women in Manufahi and 85% of women in Ainaro were able to name any method, and slightly
fewer women in both districts were able to name any modern method (90% and 82% respectively)
(Table 26). The subdistricts of Turiscai and Maubisse had the highest percentages, 17% and 28%
respectively, of women who could not identify a single method for child spacing. Of the methods that
were identified by women, the injectable method was the most commonly listed, followed by the pill
and implants (Table 27).
Use of contraceptives
Women were asked if they were currently using a method to delay or avoid getting pregnant, and for
those using a method, the type of contraception they were using. Fully 56% of women in Manufahi
report using a method; this was significantly lower at 29% in Ainaro (Table 29). The percent of women
who are currently using a modern method of contraception is slightly lower: 54% in Manufahi and 23%

12
in Ainaro report they are currently using a modern method of contraception. These findings are
interesting in light of the similarly high percentages of women who believe they should wait 2 or more
years before their next pregnancy across both districts: the value for delaying birth is not being
translated into action in Ainaro.
Among women surveyed, injectable contraception is the most commonly used in the program area
(Table 30). Forty-five percent of women In Manufahi and 13% in Ainaro are currently using an injectable
contraceptive. All other methods of contraception were used by less than 5% of the population.
Interestingly, implants were reportedly used by between 6-8% of women in four of the subdistricts—
Same, Ainaro, Hatu Udo, and Alas—demonstrating their growing popularity in Timor-Leste.
Section 4: Cell phone ownership and use in Manufahi and Ainaro
Several studies conducted in Timor-Leste over the past few years have shown a rapid escalation in
mobile phone ownership. HAI’s KPC survey collected data on mobile phone ownership and use to
inform implementation of the Mobile Moms project. Women surveyed in Manufahi and Ainaro
reported high rates of household mobile phone ownership: 69% in Manufahi and 66% in Ainaro (Table
31). Alas subdistrict had the lowest rates of household ownership at 36%, while in all other subdistricts
a majority of women reported that there was a mobile phone in their household. Not only are there
phones in the majority of households, but over a quarter of households reported owning two phones,
and 8% said they had 3 or more in the household (Table 32).
Of women who reported mobile phone ownership in the household, 70% in Manufahi and 95% in Ainaro
reported that they owned their own phone (Table 33). This finding is crucial in ensuring that women
should be able to receive and preserve messages meant predominantly for them. The program does,
however, hope to tailor messages to be shared among family members, so the subdistricts in which a
lower percentage of women reported that they own their own phones—Turiscai (58%) and Same
(68%)—will hopefully give us more insight into how often messages are shared and discussed with
partners and other family members.
Text messaging is very common in Timor-Leste. Most Timorese buy inexpensive scratch phone credit
(locally called pulsa) sold on the street to add time on their phones. Because text messaging uses far
less phone credit compared to making phone calls it is typically the preferred mobile phone
communication method. Therefore, it was not surprising that women who report household ownership
of a phone are experienced with text messaging. Fully 98% of all women who report access to a mobile
phone used the phone to send or receive text messages (Table 34). Over 70% of women with a phone in
the household sent messages at least daily (Table 35).
EXAMINING POTENTIAL BARRIERS TO MOBILE PHONE USE
Household ownership of mobile phones does not guarantee that these phones are used by women, that
the phones are charged and available for use on a daily or weekly time frame, or that women might be
able to read SMS messages that they receive. In the following section, we examine some of these
possible barriers.

13
Recharging mobile phones
When families own a mobile phone, they are very resourceful to find methods to charge their phone.
Overall, 56% of women reported that they charge their mobile phone in their home using electricity, a
solar charger, or a battery (Table 36). Fifteen percent of women used electricity at another site and 26%
of women used a solar charger at another site. Occasionally women reported using generators to
charge phones. The mix of methods used varies by subdistrict. For example in Alas, only 16% of women
reporting using electricity to charge their mobile phones at their home or another site versus 61% using
a solar charger. In Ainaro subdistrict, however, 86% of women report using electricity. What is
important was that all mobile phone owners found a way to charge their phone.
Mobile phone signal strength
Among surveyed women who reported mobile phone ownership in the household, 95% in Manufahi and
99% in Ainaro said that a cell phone signal was available either in their home or within a five minute
walk of their home (Table 37). These high percentages make us hopeful that signal coverage is adequate
for this program. We only asked this question of women who already owned phones, however so it is
difficult to know whether cell phone coverage in these districts is almost universally available or
whether the presence of a cell phone signal near to the home may be a precursor to households
allocating resources to purchase a mobile phone.
Literacy
An important component of the Mobile Moms/Liga Inan project is providing pregnant women with text
messages about healthy maternal behavior and appropriate care seeking practices. Women surveyed
were asked if they could speak, read or write Tetun, the local language spoken by the majority of
Timorese and the language that will be used for the Mobile Moms/Liga Inan text messages. Seventy-
three percent of women in Manufahi and 59% of women in Ainaro stated that they could read Tetun
(Table 38). Of those women who said that they were unable to read in the Tetun language, all stated
that there was someone in the household or nearby who could assist them in reading a message in
Tetun (Table 39). Husbands were most often mentioned, followed by other family members.
Section 5: Message preferences in Manufahi District
In order to tailor our program more specifically to the preferences of the women who will receive the
SMS messages in the Mobile Moms/Liga Inan program, women in Manufahi District were asked in which
language they would prefer to receive health-related text messages and which time of day they would
prefer to receive them. Almost all women (98%) said they would like to receive messages in Tetun, the
most widely spoke language in Timor-Leste (Table 40). This varied little cross the four subdistricts.
Greater variation was found for message timing: both morning and afternoon were equally preferred
overall, however the mix of daytime preferences varied by subdistrict (Table 41).

14
Recommendations
This survey indicates that there is a need to increase both the rates of full attendance at ANC by
pregnant women in the project area, and also improve the knowledge and several key practices related
to the pregnancy, delivery and postpartum periods.
Improve understanding and recall of health messages
Remind women of the importance of returning for
the full complement of ANC visits
Increase women’s knowledge of danger signs during
pregnancy, delivery, and postpartum to ensure that
they will seek care when medical attention is
required
Improve knowledge of health practices around
delivery for those women who have a home delivery,
including properly boiling umbilical cord-cutting
equipment, immediately providing colostrum to
newborns, and seeing a midwife for care within two
days of delivery
Provide a ready means of contact with the midwife or
clinic in case of the need for transport to the facility
Build on the rapid growth of
cell phone ownership and use
among families in Manufahi
District to implement, test, and
rigorously evaluate a mobile
phone strategy aimed to
increase health knowledge and
uptake of maternal services
among pregnant women
Assist midwives to
strengthen the ANC
care they provide
Review methods of estimating due dates with district
midwives, especially in Same subdistrict
Standardize the practice of establishing a birth plan during
ANC visits to facilitate the increase of skilled birth attendance
at delivery
Examine current practices around distribution of anti-parasite
drugs to determine the reasons for low recall by pregnant
women of that standard ANC regimen
Continue to support PSF to
deliver health promotion
messages to pregnant
women and communities
Increase women’s knowledge of danger signs during
pregnancy, delivery, and postpartum to ensure that they
will seek care when medical attention is required

15
Conclusion
A high percentage of women have at least one interaction with the health system in Manufahi and
Ainaro districts. This provides a powerful platform for improving maternal and newborn health;
however it is difficult to provide all necessary care in a single visit. Assuring that key messages are
shared during that visit and that all relevant services are available is important, but we also need to
focus on assuring that women return for additional consultations. Improving the connection between
midwives and women, and ensuring that the consultation is a positive, reinforcing experience, is
important to increasing health knowledge and health seeking behaviors among women.
The Mobile Moms/Liga Inan project is designed to help MOH midwives remind women of key health
messages and to return for other key health services, as well as improve the feeling of connection
between women and midwives. By using mobile phones, which women already have, and sending
simple text messages, which women frequently use, we can send these messages to women in their
homes. Some women may read the messages to themselves on their own phone, but other women may
share these messages with family members through a shared mobile phone or assistance during
translation. Sharing these messages or asking for help increases the number of people exposed to these
key health messages, and is a strength of the program and not a weakness. More people will read
messages about the importance of taking iron tablets, receiving tetanus toxoid vaccinations, or starting
breastfeeding within one hour of delivery.

16
List of Tables—English
Section 1: Participant Demographics Table 1: Demographics of study population Figure 1: Distribution of participant’s age in 2 year increments from Manufahi and Ainaro Figure 2: Distribution of years of school attended by participants from Manufahi and Ainaro Figure 3: Distribution of number of children per woman from Manufahi and Ainaro Table 2: Materials used floor and roofing among survey participants Table 3: Women who report having specific household commodities
Section 2: Maternal Health Indicators
Table 4: Percent of women with children between the ages of 0-23 months who received antenatal care (ANC) from a skilled health provider
Table 5: Reported sites of antenatal care among women who reported they attended at least one ANC visit
Table 6: Timing of initiation of the first antenatal care visit Table 7: Women who obtained at least one ANC visit who received selected services Table 8: Women who received any antenatal care who report that a midwife calculated their
Estimated Due Date (EDD) during ANC Table 9: Women surveyed who can identify 2 or more danger signs of pregnancy Table 10: Women who received tetanus toxoid (TT) vaccinations during their last pregnancy
and over their lifetime Table 11: Percent of women who received iron supplementation during their last pregnancy Table 12: Women who took intestinal parasite drugs during their last pregnancy Table 13: Reported methods available for women to contact midwives around the time of birth Table 14: Percentage of women who had a skilled birth attendant present at last birth Table 15: Place of last delivery for women with a child 0-23 months of age Table 16: Method of transportation used to reach health facility among women who delivered
at a health facility Table 17: Reported travel time to nearest health facility where a woman could deliver Table 18: Women who reported clean cord cutting practices during the birth of their last child Table 19: Women reporting application of substance on the umbilical cord before or after
delivery of the placenta, by substance Table 20: Percentage of children 0-23 months of age who were put to the breast within one
hour after delivery and/or were given colostrum Table 20: Percentage of children 0-23 months of age who were put to the breast within one
hour after delivery and percentage who were given colostrum Table 21: Percentage of newborns who received another food prior to receiving breastmilk or
during their first month after birth Table 22: Women who received a postpartum visit within two days of delivery Table 23: Percent of babies that received a postnatal visit from a trained health worker within
two days after birth Table 24: Knowledge of danger signs danger signs during delivery and in newborns

17
Section 3: Family Planning Table 25: Reported ideal birth interval among women with children 0-23 months of age Table 26: Reported risks of getting pregnant too soon after the birth of a child Table 27: Women who could spontaneously name a contraceptive method Table 28: Knowledge of contraceptive methods by women as determined by spontaneous
recall Table 29: Table 30: Family planning methods used by women with children under 2 years of age
Section 4: Cell phone ownership and use in Manufahi and Ainaro Table 31: Women who reported mobile phone ownership in household Table 32: Number of mobile phones per household for women with any mobile phones in the
home Table 33: Percentage of women who report there is their “own” phone in the household Table 34: Women who report using their mobile phone to send or receive text message Table 35: Frequency of text message sending among women who own mobile phones Table 36: Methods reported by women to charge mobile phones Table 37: Reported distance to cell phone signal among women with children 0-23 months of
age who have a cell phone in their household Table 38: Level of Tetun language literacy reported by women with children 0-23 months of
age Table 39: Available assistance in reading tetun messages by women who reported being unable
to read the Tetun language themselves
Section 5: Message preferences in Manufahi District Table 40: Preferred language for text messages among women in Manufahi District Table 41: Preferred time of day to receive health-related text messages in Manufahi District

18
List of Tables—Tetun
Section 1: Demografia participante Table 1: Estudo demografia populasaun Figure 1: Distribusaun participante nia idade iha grupo tinan rua husi Manufahi no Ainaro Figure 2: Numeru tinan participantes ba eskola husi Manufahi no Ainaro Figure 3: Distribusaun numeru oan per inan husi Manufahi no Ainaro Table 2: Materias ne’ebe uja ba uma kakuluk no rai (Uma laran) husi participante Table 3: Inan ne’ebe relata iha sasan uma laran spesifiko
Section 2: Indicadores saúde maternais no infantil Table 4: Percentajen inan ho oan ho idade fulan 0-23 ne’ebe simu konsulta isin rua (ANC) husi
pesoal saúde Table 5: Reporta fatin ne’ebe inan uja atu hetan konsulta isin rua entre inan ne’ebe reporta
katak sira atende Vizita ANC maizumenus dala ida. Table 6: Fulan ne’ebe inan simu konsulta isin rua dala primero Table 7:Inan ne’ebe hetan vizita ANC maizumenus dala ida mak servi ho selesionado Table 8: Inan ne’ebe simu ANC ne’ebe dehan katak parteira halo kalkulasaun ba estimasaun
loron partus (EDD) nian durante inan mai halo kuidado antenatal Table 9: Inan ne’ebe iha estudo nee bele identifika sinal perigu durante isin rua nina 2 ka liu Table 10: Inan ne’ebe simu vacina tetanus toxoid (TT) durante isin rua ba sira nia oan ida ikus
(kiik) ka inan ne’ebe simu durante moris tomak Table 11: Persentajen inan ne’ebe hemu aimoruk aumenta ran durante isin rua ikus Table 12: Inan ne’ebe hemu aimoruk intestinal parasite durante sira nia isin rua ida ikus nee Table 13: Relatori ba metode sira ne’ebe iha ba inan sira hodi kontakto parteira iha tempu
ne’ebe atu partus Table 14: Persentajen inan ne’ebe simu supporta husi pesoal saúde treinado (Dotor, Parteira
ka Infermeiro) durante partus ida ikus nee Table 15: Fatin partu ida ikus nian ba inan ho oan idade 0-23 Table 16: Metode ba uza transporte atu ba to iha fasilidade saúde ba inan sira ne’ebe partus
iha fasilidade saúde Table 17: Relatori kona ba tempu viajen ba besik fasilidade saúde atu hodi partus Table 18: Inan ne’ebe relata pratika koa husar moos durante partus sira nian oan ida ikus Table 19: Inan ne’ebe relata tau buat ruma ba bebe nia husar antes ka depois deka’an moris Table 20: Percentajen husi oan idade fulan 0-23 ne’ebe simu susu ona iha oras ida nia laran depois
the partus no simu susuben kinur Table 21: Percentajem bebe foin moris ne’ebe hemu buat ruma antes de simu susuben inan nian ka
hemu buat seluk durante fulan primero depois de moris Table 22: Inan sira ne’ebe simu vizita postpartum iha loron rua nia laran husi partus Table 23: Persentajen bebe ne’ebe simu vizita postnatal husi pesoal saúde treinado iha loron rua nia
laran husi moris
Table 24: Inan sira ne’ebe hatene sinal perigu durante partus no iha ba bebe foin moris
Section 3: Indicadores kona ba planementu familiar

19
Table 25: Relatorio kona ba espaso oan ideal husi inan ne’ebe ho oan idade fulan 0-23 Table 26:Relata risko husi hetan isin rua fali iha tempu badak nia laran depois partus Table 27: Inan ne’ebe bele identifika naran methodu contraceptive ruma
Table 28: Koinesimentu kona ba methodu kontraseptivu husi inan sira ne’ebe sira identifika rasik
Table 29: Inan ne’ebe ho oan idade fulan 0-23 mak agora dadaun uza metode planeamentu familiar modernu ka tradisional
Table 30: Methodu planementu familiar ne’ebe uza husi inan ne’ebe iha bebe tinan 2 mai kraik
Section 4: Cell phone ownership and use in Manufahi and Ainaro Table 31: Inan sira ne’ebe iha telemovel rasik iha uma Table 32: Numero telemovel kada uma kain husi inan ne’ebe iha telemovel ida ka liu Table 33: Persentajen inan sira ne’ebe iha telemovel rasik Table 34: Inan ne’ebe iha relatori uza sira nia telemovel rasik hodi haruka no simu mensagen Table 35: Entre inan sira ne’ebe haruka mensagen frequentamente husi sira nia telemovel rasik Table 36: Relaori kona ba metode husi inan sira atu chas telemovel Table 37: Relatori kona ba distancia ba signal telemovel husi inan ho oan idade fulan 0-23
ne’ebe iha telemovel rasik iha uma Table 38: Nivel education iha lingua Tetun tuir relatori husi Inan ne’ebe iha oan idade fulan 0-
23 Table 39: Iha ema ne’ebe ajuda le’e mensagen iha tetum ba inan sira ne’ebe tuir relatori labele
atu le’e iha lian Tetun
Section 5: Message preferences in Manufahi District Table 40: Lingua ne’ebe prefere liu ba texto mensagen nian husi inan iha Distritu Manufahi Table 41: Tempu iha loron ne’ebe prefere liu atu simu mensagen saúde nian iha Distrito
Manufahi

20
Tables for Results on Participant Demographics
Table 1: Demographics of study population* Table 1: Estudo demografia populasaun*
Area Average age of Woman
(Years)
Average Years of School
Average Number of
Children per Woman
Number of Women
interviewed
Area Medida
idade inan (Tinan)
Medida tinan eskola
Medida numeru oan husi kada
inan
Numeru inan tuir intervista
Alas 27.4 5.5 3.6 72
Fatuberliu 27.8 8.5 3.9 72
Same 26.6 7.0 3.5 72
Turiscai 28.2 7.1 4.5 77
Manufahi District Total
27.0 7.0 3.7 293
Ainaro 28.8 8.6 4.0 72
Hatu Udo 27.2 6.2 3.4 72
Hatubuilico 28.9 5.3 4.6 72
Maubisse 28.8 4.5 5.1 72
Ainaro District Total
28.5 5.9 4.4 288
Combined District Total
27.8 6.5 4.1 581
*The data presented in this and all following tables are weighted with respect to variations at the sample level, the subdistrict population, and district population as follows:
at the subdistrict level: the data is weighted with respect to variations in sample size only at the district level: the data is weighted with respect to variations in sample size and the
variations in population of the subdistrict at the combined district level: the data is weighted with respect to variations in sample size, the
variations in population of the subdistrict, and variations in the population of the district *Dadus ne’ebé aprezenta iha ne’e no tabela sira tuir mai ne’e tetu ona ho variasaun iha nivel amostra, populasaun sub-distritu, no distritu hanesan tuirmai ne’e:
Iha nivel sub-distritu: dadus sira tetu haktuir variasaun iha amostra nia tamañu de’it Iha nivel distritu: dadus analiza tuir variasaun iha tamañu amostra, variasaun populasaun iha sub-
distritu Iha nivel distritu kombinadu: dadus analiza ka tetu tuir variasaun iha tamañu amostra, variasaun
populasain iha distritu

21
Figure 1: Distribution of participants’s age in 2 year increments from Manufahi and Ainaro Figure 1: Distribusaun participante nia idade iha grupo tinan rua husi Manufahi no Ainaro
Figure 2: Distribution of years of school attended by participants from Manufahi and Ainaro Figure 2: Numeru tinan participantes atende eskola husi Manufahi no Ainaro
Figure 3: Distribution of number of children per woman from Manufahi and Ainaro Figure 3: Distribusaun numeru oan kada inan husi Manufahi no Ainaro
0
.02
.04
.06
.08
.1
Dens
ity
10 20 30 40 50
Age in 2 year increments

22
Table 2: Materials used floor and roofing among survey participants Table 2: Materias ne’ebe uja ba uma kakuluk no rai (Uma Laran) husi participante
Program Area
Roof Material Floor Material Total
Women Palm Leaves
Sheet Iron Other Earth Concrete Wood/
Bamboo Other
Area Programa
Uma Kakuluk Rai iha Uma Laran
Inan total
Tali Tahan Kalen Seluk Rai Semente Ai ou
Fafulu ka Au
Seluk
Alas 51% 43% 6% 68% 19% 12% 0% 72 Fatuberliu 22% 78% 0% 53% 43% 4% 0% 72
Same 22% 78% 0% 60% 35% 6% 0% 72 Turiscai 3% 87% 10% 65% 34% 1% 0% 77
Manufahi District Total
23% 75% 2% 60% 34% 6% 0% 293
Ainaro 7% 93% 0% 56% 39% 3% 3% 72 Hatu Udo 51% 46% 3% 64% 32% 4% 0% 72 Hatubuilic
o 10% 90% 0% 71% 29% 0% 0% 72
Maubisse 22% 68% 10% 75% 25% 0% 0% 72
Ainaro District
21% 75% 4% 67% 30% 1% 1% 288
Combined District Totals
22% 75% 3% 64% 32% 4% 0% 581

23
Table 3: Women who report having specific household commodities* Table 3: Inan ne’ebe relata iha sasan uma laran spesifiko
Program Area Electricity Radio Television Mobile Phone
Bicycle Motor bike
Car/ Truck
Horse/ Animal
Transport
Total Women
Area Programa
Electricidade Radio Televizaun Telemovel Bicikleta Motor Kareta ka trek
Kuda ka animale
ne’ebe usa ba
transporte
Inan total
Alas 19% 22% 7% 36% 22% 13% 1% 43% 72 Fatuberliu 54% 19% 22% 59% 48% 21% 6% 20% 72
Same 50% 35% 24% 69% 17% 18% 0% 44% 72 Turiscai 42% 36% 20% 49% 6% 13% 2% 67% 77
Manufahi District Total
46% 31% 21% 62% 20% 17% 1% 44% 293
Ainaro 54% 29% 42% 72% 6% 31% 4% 15% 72 Hatu Udo 19% 38% 7% 60% 1% 8% 3% 56% 72
Hatubuilico 3% 46% 14% 65% 0% 24% 0% 35% 72 Maubisse 17% 46% 13% 47% 4% 11% 1% 49% 72
Ainaro District Total
24% 40% 19% 59% 3% 18% 2% 39% 288
Combined District Totals
35% 35% 20% 61% 12% 18% 1.6% 41% 581
*This table displays the proportion of total responses. Women could report more than one answer. *Tabela ne’e hatudu proporsionalidade husi total resposta. Inan bele reporta liu tan husi resposta ida.

24
Tables for Results on Maternal and Newborn Health
Table 4: Percent of women with children between the ages of 0-23 months who received antenatal care (ANC) from a skilled health provider
Table 4: Percentajen inan ho oan ho idade fulan 0-23 ne’ebe simu konsulta isin rua (ANC) husi pesoal saúde
Program Area Percent women who
received at least 1 ANC visit
Percent women who received 4 or more
ANC visits No ANC visits
Total Women
Area Programa
Percentajen husi inan ne’ebe simu vizita ANC
dala 1 ka liu
Percentajen husi inan ne’ebe simu vizita ANC
dala 4 ka liu
Percentajen husi inaan ne’ebe la simu
ANC
Inan Total
Alas 96% 75% 4% 72 Fatuberliu 99% 72% 1% 72
Same 93% 83% 7% 72 Turiscai 84% 45% 16% 77
Manufahi District Total
93% 76% 7% 293
Ainaro 90% 67% 10% 72 Hatu Udo 83% 71% 17% 72
Hatubuilico 93% 69% 7% 72 Maubisse 94% 64% 6% 72
Ainaro District Total
91% 67% 9% 288
Combined District Totals
92% 72% 8% 581

25
Table 5: Reported sites of antenatal care among women who reported they attended at least one ANC visit* Table 5: Reporta fatin ne’ebe inan uja atu hetan konsulta isin rua entre inan ne’ebe reporta katak sira atende Vizita ANC maizumenus
dala ida
Program Area
Home Hospital Maternity
Community Health Center (CHC)
Health Post
SISCA Outreach
Event Private Clinic
Other
Women who
received at least 1
ANC
Area Programa
Uma Hospital Maternid
ade CHC
Postu Saúde
SISCa Eventu
outreach Clinika privadu
Seluk
Inan ne’ebe
simu ANC dala 1 ka
liu
Alas 0% 1% 1% 26% 42% 35% 4% 0% 0% 69 Fatuberliu 0% 1% 0% 85% 14% 1% 0% 0% 16% 71
Same 0% 21% 1% 58% 22% 18% 0% 0% 0% 67 Turiscai 2% 6% 0% 94% 0% 2% 0% 0% 0% 66
Manufahi District Total
0% 14% 1% 62% 21% 16% 1% 0% 2% 273
Ainaro 0% 0% 0% 83% 15% 0% 0% 2% 0% 65 Hatu Udo 2% 0% 0% 48% 42% 7% 0% 0% 0% 60
Hatubuilico 1% 1% 0% 27% 31% 13% 0% 25% 0% 67 Maubisse 0% 82% 0% 9% 7% 0% 0% 6% 0% 68
Ainaro District Total
1% 33% 0% 37% 21% 4% 0% 8% 0% 260
Combined District Totals
0% 23% 1% 50% 21% 10% 0% 4% 1% 533
*This table displays the proportion of total responses. Women could report more than one answer. *Tabela ne’e hatudu proporsionalidade husi total resposta. Inan bele reporta liu tan husi resposta ida.

26
Table 6: Timing of initiation of the first antenatal care visit Table 6: Fulan ne’ebe inan simu konsulta isin rua dala primero
Program Area 1-3 months 4-6 moths 7-9 months Don’t Know
or Forgot Women who received ANC
Area Programa
Fulan 1-2 Fulan 4-6 Fulan 7-9 La hatene ka
haluha Inan ne’ebe simu ANC
Alas 78% 19% 3% 0% 69 Fatuberliu 71% 29% 0% 0% 71
Same 55% 40% 4% 0% 67 Turiscai 37% 51% 12% 0% 66
Manufahi District Total
58% 37% 4% 0% 273
Ainaro 40% 60% 0% 0% 65 Hatu Udo 52% 48% 0% 0% 60
Hatubuilico 49% 46% 3% 1% 67 Maubisse 15% 75% 10% 0% 68
Ainaro District Total
34% 61% 5% 0% 260
Combined District Totals
46% 49% 5% 0% 533
Table 7: Women who obtained at least one ANC visit who received selected services Table 7:Inan ne’ebe hetan visita ANC maizumenus dala ida mak servi ho selesionado
Program Area Weight Taken
Blood Pressure Measured*
Stomach Examined
Women who received ANC
Area Programa Tetu Todan Koko tensaun Koko kabun
Inan ne’ebe simu ANC
Alas 91% 93% 100% 69 Fatuberliu 96% 88% 100% 71
Same 99% 100% 99% 67 Turiscai 69% 79% 90% 66
Manufahi District Total
95% 96% 98% 273
Ainaro 100% 98% 100% 65 Hatu Udo 100% 100% 100% 60
Hatubuilico 100% 97% 97% 67 Maubisse 100% 100% 99% 68
Ainaro District
100% 99% 99% 260
Combined District Totals
97% 97% 98% 533
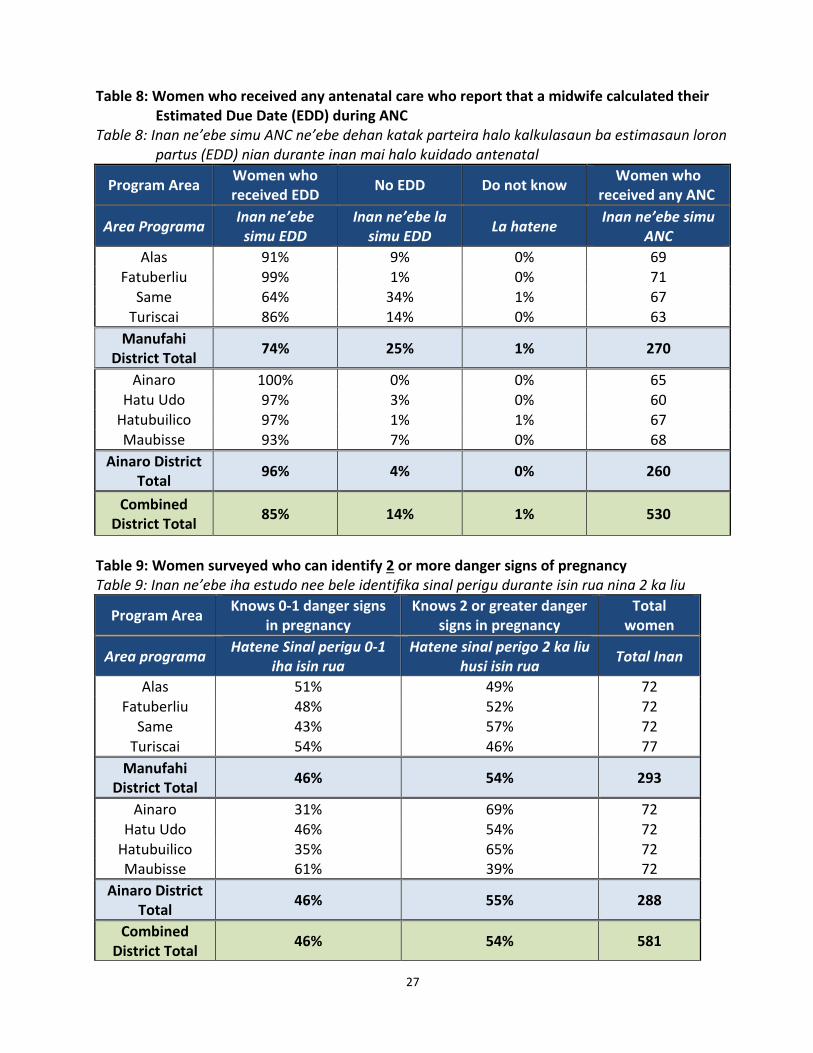
27
Table 8: Women who received any antenatal care who report that a midwife calculated their Estimated Due Date (EDD) during ANC
Table 8: Inan ne’ebe simu ANC ne’ebe dehan katak parteira halo kalkulasaun ba estimasaun loron partus (EDD) nian durante inan mai halo kuidado antenatal
Program Area Women who received EDD
No EDD Do not know Women who
received any ANC
Area Programa Inan ne’ebe
simu EDD Inan ne’ebe la
simu EDD La hatene
Inan ne’ebe simu ANC
Alas 91% 9% 0% 69 Fatuberliu 99% 1% 0% 71
Same 64% 34% 1% 67 Turiscai 86% 14% 0% 63
Manufahi District Total
74% 25% 1% 270
Ainaro 100% 0% 0% 65 Hatu Udo 97% 3% 0% 60
Hatubuilico 97% 1% 1% 67 Maubisse 93% 7% 0% 68
Ainaro District Total
96% 4% 0% 260
Combined District Total
85% 14% 1% 530
Table 9: Women surveyed who can identify 2 or more danger signs of pregnancy Table 9: Inan ne’ebe iha estudo nee bele identifika sinal perigu durante isin rua nina 2 ka liu
Program Area Knows 0-1 danger signs
in pregnancy Knows 2 or greater danger
signs in pregnancy Total
women
Area programa Hatene Sinal perigu 0-1
iha isin rua Hatene sinal perigo 2 ka liu
husi isin rua Total Inan
Alas 51% 49% 72 Fatuberliu 48% 52% 72
Same 43% 57% 72 Turiscai 54% 46% 77
Manufahi District Total
46% 54% 293
Ainaro 31% 69% 72 Hatu Udo 46% 54% 72
Hatubuilico 35% 65% 72 Maubisse 61% 39% 72
Ainaro District Total
46% 55% 288
Combined District Total
46% 54% 581

28
Table 10: Women who received tetanus toxoid (TT) vaccinations during their last pregnancy and over their lifetime
Table 10: Inan ne’ebe simu vacina tetanus toxoid (TT) durante isin rua ba sira nia oan ida ikus (kiik) ka inan ne’ebe simu durante moris tomak
Program Area Last pregnancy Lifetime Total
Women Any TT 2+ TT 2+ TT Never
Area Programa Isin rua ikus Durante moris tomak
Total Inan Dala 1 ka liu 2+ TT 2+ TT Nunka
Alas 85% 75% 93% 4% 71
Fatuberliu 96% 89% 95% 1% 72
Same 86% 75% 85% 7% 72
Turiscai 67% 51% 78% 11% 77
Manufahi District Total
85% 74% 86% 6% 292
Ainaro 76% 64% 83% 4% 72
Hatu Udo 78% 71% 89% 8% 72
Hatubuilico 69% 63% 78% 15% 72
Maubisse 72% 51% 79% 7% 72
Ainaro District Total
74% 60% 82% 8% 288
Combined District Total
79% 67% 84% 7% 580

29
Table 11: Percent of women who received iron supplementation during their last pregnancy
Table 11: Persentajen inan ne’ebe hemu aimoruk aumenta ran durante isin rua ikus
Program Area Women who took
any iron tablets Women who took
more than 90 tablets Did not know or do
not remember Total
Women
Area Programa
Inan ne’ebe hemu tableta aumenta ran
Inan ne’ebe hemu tablet 90 ka liu
La hatene ka haluhan
Total Inan
Alas 86% 66% 0% 72 Fatuberliu 96% 84% 0% 72
Same 90% 31% 0% 72 Turiscai 87% 53% 2% 77
Manufahi District Total
90% 45% 0% 293
Ainaro 88% 33% 0% 72 Hatu Udo 78% 77% 0% 72
Hatubuilico 92% 62% 0% 72 Maubisse 88% 71% 1% 72
Ainaro District Total
87% 61% 1% 288
Combined District Total
88% 52% 0% 581
Table 12: Women who took intestinal parasite drugs during their last pregnancy Table 12: Inan ne’ebe hemu aimoruk intestinal parasite durante sira nia isin rua ida ikus nee
Program Area
Women who took intestinal parasite drugs
Women who did not take intestinal parasite drugs
Did not know
Total Women
Program Area
Inan ne’ebe hemo aimoruk contra intestinal
parasite
Inan ne’ebe la hemu aimoruk contra intestinal
parasite La hatene
Total inan
Alas 17% 81% 3% 72 Fatuberliu 6% 89% 5% 72
Same 23% 77% 0% 71 Turiscai 45% 55% 0% 77
Manufahi District Total
22% 77% 1% 292
Ainaro 1% 99% 0% 72
Hatu Udo 24% 71% 6% 72 Hatubuilico 11% 89% 0% 72 Maubisse 21% 78% 1% 72
Ainaro District Total
14% 84% 1% 288
Combined District Total
19% 80% 1% 580

30
Table 13: Reported methods available for women to contact midwives around the time of birth (multiple responses possible)* Table 13: Relatori ba metode sira ne’ebe iha ba inan sira hodi kontakto parteira iha tempu ne’ebe atu partus*
Program Area
In person only By household
phone By other phone Send messenger Other1
Not able to contact midwife
Area Programa
Ba hasoru deit Husi telefone
uma Husi telefone
seluk Haruka
mensagen Seluk1
La bele atu kontakto ho
parteira
Alas 6% 15% 3% 38% 1% 40% Fatuberliu 2% 0% 6% 74% 0% 17%
Same 10% 50% 25% 13% 0% 8%
Turiscai 3% 16% 8% 66% 0% 17%
Manufahi District Total
7% 35% 18% 30% 0% 14%
Ainaro 24% 54% 10% 21% 0% 7% Hatu Udo 18% 18% 7% 43% 0% 19%
Hatubuilico 15% 40% 4% 21% 0% 21%
Maubisse 11% 22% 4% 38% 3% 31%
Ainaro District Total
16% 33% 6% 31% 1% 21%
Combined District Total
12% 35% 12% 30% 1% 18%
1 Other methods include via community health worker. * This table displays the proportion of total responses. Women could respond to more than one method. 1 Métodu seluk inklui liuhosi traballadór saúde komunidade. * Tabela ne’e hatudu proporsaun totál resposta. Inan bele hatán liu hosi métodu ida.

31
Table 14: Percentage of women who had a skilled birth attendant (doctor, midwife, or nurse) present at last birth
Table 14: Persentajen inan ne’ebe simu supporta husi pesoal saúde treinado (Dotor, Parteira ka Infermeiro) durante partus ida ikus nee
Program Area Skilled birth attendant present Total women
Area Programa Presensa pesoal saúde treinado Total inan
Alas 36% 72 Fatuberliu 63% 72
Same 53% 72 Turiscai 16% 77
Manufahi District Total 48% 293
Ainaro 63% 72 Hatu Udo 44% 72
Hatubuilico 18% 72
Maubisse 29% 72
Ainaro District Total 38% 288
Combined District Total
43% 581
Table 15: Place of last delivery for women with a child 0-23 months of age Table 15: Fatin partu ida ikus nian ba inan ho oan idade 0-23
Program Area At Home Health facility (Hospital, CHC,
or health post) Totals
women
Area Programa Iha uma Fasilidade Suade (Ospital,
CHC, ka postu saúde) Total Inan
Alas 83% 17% 72 Fatuberliu 71% 29% 72
Same 58% 42% 72
Turiscai 99% 1% 77
Manufahi District Total 68% 32% 293
Ainaro 46% 54% 72 Hatu Udo 76% 24% 72
Hatubuilico 93% 7% 72
Maubisse 72% 28% 72
Ainaro District Total 71% 29% 288
Combined District Total
69% 31% 581

32
Table 16: Method of transportation used to reach health facility among women who delivered at a health facility
Table 16: Metode ba uza transporte atu ba to iha fasilidade saúde ba inan sira ne’ebe partus iha fasilidade saúde
Program Area
Walk Private
Car Public
Ambulance or MOH vehicle
Other1
Total Women Who
Reported Transportation
Area Programa
Lao Kareta Privado
Transporte publiko
Ambulancia ka kareta
MdS Seluk1
Total inan ne’ebe relata
kona ba transporte
Alas 9% 18% 18% 55% 0% 11
Fatuberliu 9% 0% 22% 69% 0% 21 Same 0% 0% 13% 77% 10% 30
Turiscai 0% 0% 0% 100% 0% 1
Manufahi District Total
2% 1% 15% 75% 8% 63
Ainaro 21% 8% 8% 49% 15% 39 Hatu Udo 29% 0% 6% 59% 6% 17
Hatubuilico 0% 0% 40% 60% 0% 5 Maubisse 30% 5% 5% 55% 5% 20
Ainaro District Total
24% 5% 8% 53% 10% 81
Combined District Total
12% 3% 12% 64% 9% 144
1 Other includes: rental truck, fireman care, police car, motorcycle, other family’s motorcycle, private motor cycle, and family’s transport.
1 Seluk inklui: aluga kamioneta, bonbeirus, polísia nia karreta, motór, família seluk sira-nia motór, motór privadu, no família nia transporte.

33
Table 17: Reported travel time to nearest health facility where a woman could deliver Table 17: Relatori kona ba tempu viajen ba besik fasilidade saúde atu hodi partus
Program Area 30 minutes
or less 30-60
minutes 60-90
minutes 90-120
minutes 120-150 minutes
150-180 minutes
Greater than 180 minutes
Total women
Area Programa Minutu 30 ka
menus Minutu 30-60
Minutu 60-90
Minutu 90-120
Minutu 120-150
Minutu 150-180
Liu tan 180 minutu
Total inan
Alas 48% 23% 1% 18% 0% 3% 7% 71 Fatuberliu 42% 28% 10% 7% 6% 2% 4% 72
Same 44% 39% 4% 7% 1% 4% 0% 72 Turiscai 36% 21% 13% 9% 2% 18% 1% 77
Manufahi District Total
44% 33% 6% 9% 2% 5% 1% 292
Ainaro 53% 31% 7% 10% 0% 0% 0% 72 Hatu Udo 43% 18% 6% 15% 4% 4% 10% 72
Hatubuilico 44% 29% 11% 13% 0% 3% 0% 72
Maubisse 24% 21% 17% 22% 4% 10% 3% 72
Ainaro District Total
38% 25% 11% 16% 2% 5% 3% 288
Combined District Total
41% 29% 8% 12% 2% 5% 2% 580

34
Table 18: Women who reported clean cord cutting practices during the birth of their last child Table 18: Inan ne’ebe relata pratika koa husar moos durante partus sira nian oan ida ikus
Program Area % of children age 0-23 months who had clean
cord cutting at the time of birth Total women
Area Programa % husi oan idade fulan 0-23 ne’ebe husar koa
ho mos iha tempu partu Total Inan
Alas 43% 72
Fatuberliu 63% 72
Same 58% 72
Turiscai 64% 77
Manufahi District Total 58% 293
Ainaro 75% 72
Hatu Udo 60% 72
Hatubuilico 61% 72
Maubisse 78% 72
Ainaro District Total 71% 288
Combined District Total 64% 581
Table 19: Women reporting application of substance on the umbilical cord before or after delivery of
the placenta, by substance Table 19: Inan ne’ebe relata tau buat ruma ba bebe nia husar antes ka depois de ka’an moris
Program Area Cow Dung
Any type of oil
Antiseptic Ashes Other Nothing Total
Women
Area Programa
Karau ten Mina ruma
Betadin Aahukdes
an Seluk
La tau buat ruma
Inan Total
Alas 0% 0% 7% 7% 8% 77% 71
Fatuberliu 0% 3% 12% 0% 17% 69% 68
Same 1% 1% 7% 4% 4% 81% 67
Turiscai 0% 1% 7% 2% 15% 75% 77
Manufahi District Total
1% 1% 8% 4% 7% 78% 283
Ainaro 0% 1% 30% 1% 19% 46% 69
Hatu Udo 0% 1% 7% 0% 25% 65% 71
Hatubuilico 0% 0% 10% 1% 27% 62% 71
Maubisse 0% 0% 0% 8% 0% 92% 71
Ainaro District Total
0% 1% 10% 4% 14% 69% 283
Combined District Totals
0% 1% 9% 4% 11% 74% 566

35
Table 20: Percentage of children 0-23 months of age who were put to the breast within one hour after
delivery and percentage who were given colostrum
Table 20: Percentajen husi oan idade fulan 0-23 ne’ebe simu susu ona iha oras ida nia laran depois the partus no simu susuben kinur
Program Area Percentage of children who received
breastmilk within one hour of delivery Percentage of children who
received colostrums Total
women
Area Programa Persentajen husi oan ne’ebe tau kedas
ba inan atu fo susu iha oras ida nia laran depois de moris
Persentajen husi oan ne’ebe simu susuben kinur
Total inan
Alas 47% 97% 72
Fatuberliu 36% 99% 72
Same 56% 93% 72
Turiscai 43% 100% 75
Manufahi District 51% 95% 291
Ainaro 75% 99% 72
Hatu Udo 41% 93% 70
Hatubuilico 70% 93% 71
Maubisse 51% 77% 70
Ainaro District 60% 88% 283
Combined District Total
55% 92% 574
Table 21: Percentage of newborns who received another food prior to receiving breastmilk or
during their first month after birth Table 21: Percentajem bebe foin moris ne’ebe hemu buat ruma antes de simu susuben inan nian ka
hemu buat seluk durante fulan primero depois de moris
Program Area Gave other foods prior to
breastfeeding Total
Women Provided substance other than breastmilk during first month
Total Women
Program Area Fo hahan ruma ba bebe antes
de fo susuben inan nian Inan Total
Fo hahan ruman durante fulan primero depois de moris
Total Women
Alas 15% 72 18% 72
Fatuberliu 27% 72 26% 72
Same 17% 71 24% 72
Turiscai 31% 74 7% 75
Manufahi District 20% 289 21% 291
Ainaro 19% 72 25% 72
Hatu Udo 23% 70 7% 69
Hatubuilico 41% 71 3% 71
Maubisse 17% 70 10% 70
Ainaro District 24% 283 12% 282
Combined District Totals
22% 572 17% 573

36
Table 22: Women who received a postpartum visit within two days of delivery Table 22: Inan sira ne’ebe simu vizita postpartum iha loron rua nia laran husi partus
Program Area Postpartum Visit
within 2 days Postpartum Visit
after 2 days No Post Partum Care
Total Women
Area Programa Visita postpartum
iha loron 2 nia laran Visita postpartum depois de loron 2
La hetan kuidadus postpartum
Inan total
Alas 19% 56% 25% 72
Fatuberliu 22% 44% 34% 72
Same 31% 36% 33% 72
Turiscai 9% 42% 49% 77
Manufahi District 26% 40% 34% 293
Ainaro 61% 15% 24% 72
Hatu Udo 32% 40% 28% 72
Hatubuilico 44% 1% 55% 71
Maubisse 22% 46% 32% 72
Ainaro District 38% 28% 34% 287
Combined District Total
32% 34% 34% 580
Table 23: Percent of babies that received a postnatal visit from a trained health worker within two days
of birth Table 23: Persentajen bebe ne’ebe simu vizita postnatal husi pesoal saúde treinado iha loron rua nia laran
husi moris
Area Newborn Check
within 2 days Newborn Check after
2 days No Newborn Check
Total Women
Area Vizita postnatal
Iha loron 2 nia laran Vizita postnatald epois de loron 2
La hetan kuidadus postnatal
Inan total
Alas 13% 57% 31% 72 Fatuberliu 18% 21% 62% 72
Same 24% 28% 49% 72 Turiscai 8% 68% 25% 77
Manufahi District 20% 37% 44% 293
Ainaro 63% 15% 22% 72 Hatu Udo 31% 33% 36% 72
Hatubuilico 18% 40% 42% 72 Maubisse 18% 64% 18% 72
Ainaro District 32% 43% 25% 288
Combined District Totals
25% 38% 36% 581

37
Table 24: Knowledge of danger signs danger signs during delivery and in newborns Table 24: Inan sira ne’ebe hatene sinal perigu durante partus no iha ba bebe foin moris
Program Area Knows 2 or more
danger signs during delivery
Knows 2 or more danger signs in
newborns
Knows 2 or more
danger signs for
women postpartum
Total women
Area Programa Hatene sinal perigo
durante partus 2 ka liu
Hatene sinal perigo bebe foin moris 2
ka liu
Hatene sinal perigu ba inan depois de
partus 2 ka liu
Total inan
Alas 36% 56% 50% 72 Fatuberliu 37% 75% 38% 72
Same 29% 32% 39% 72 Turiscai 35% 48% 51% 77
Manufahi District Total
32% 42% 42% 293
Ainaro 51% 40% 75% 72 Hatu Udo 36% 36% 60% 72
Hatubuilico 26% 11% 65% 72 Maubisse 24% 50% 42% 72
Ainaro District Total
33% 37% 58% 288
Combined District Total
32% 40% 50% 581

38
Tables of Results on Family Planning
Table 25: Reported ideal birth interval among women with children 0-23 months of age Table 25: Relatorio kona ba espaso oan ideal husi inan ne’ebe ho oan idade fulan 0-23
Program Area
Number of years women reported was best to space between children: Total
Women One Year Two Years Three or more
years Don’t Know
Area Programa
Numeru tinan katak inan sira hanoin apropriadu atu espasu entre oan: Inan Total
Tinan ida Tinan rua Tinan tolu ka
liu La Hatene
Alas 19% 31% 43% 7% 72 Fatuberliu 15% 36% 46% 4% 72
Same 17% 38% 44% 1% 72 Turiscai 17% 44% 35% 4% 77
Manufahi District Total
17% 37% 43% 3% 292
Ainaro 22% 49% 26% 3% 72 Hatu Udo 19% 56% 24% 1% 72
Hatubuilico 19% 67% 14% 0% 72 Maubisse 13% 65% 22% 0% 72
Ainaro District Total
18% 60% 22% 1% 288
Combined District Total
17% 48% 33% 2% 580

39
Table 26: Reported risks of getting pregnant too soon after the birth of a child* Table 26: Relata risko husi hetan isin rua fali iha tempu badak nia laran depois partus
Program Area
Baby born too small
Baby born too early
Mother can die
Mother can
miscarry
Mother can suffer
anemia
Bad for health of mother and/or baby
Mother cannot work
between pregnancies
Other Total
Women
Area Programa
Bebe moris kik
liu
Bebe moris
sedu liu
Inan bele mate
Ina bele abortus
Inan bele sofre
anemia
Ladiak ba inan ka
bebe nia saúde
Laiha tempo atu
halo servico Seluk
Inan Total
Alas 10% 0% 15% 4% 17% 33% 35% 1% 72 Fatuberliu 4% 0% 13% 6% 0% 55% 46% 4% 72
Same 18% 0% 24% 4% 22% 22% 26% 11% 72 Turiscai 2% 5% 9% 6% 3% 36% 58% 7% 77
Manufahi District
13% 1% 20% 5% 16% 29% 34% 8% 293
Ainaro 29% 0% 3% 0% 3% 74% 15% 18% 72 Hatu Udo 7% 1% 11% 0% 1% 43% 40% 4% 72
Hatubuilico 21% 3% 7% 1% 0% 79% 21% 11% 72 Maubisse 1% 0% 4% 0% 4% 44% 71% 4% 72
Ainaro District
13% 1% 6% 0% 3% 59% 42% 9% 288
Combined District Totals
13% 1% 13% 2% 10% 44% 38% 9% 581
*This table displays the proportion of total responses. Women could report more than one answer. *Tabela ne’e hatudu proporsionalidade husi total resposta. Inan bele reporta liu tan husi resposta ida.

40
Table 27: Women who could spontaneously name a contraceptive method Table 27: Inan ne’ebe bele identifika naran methodu contraceptive ruma
Program Area Any Method Any modern
method No method
known Total
Women
Area Programa
Identifika methodu 1 ka
liu
Identifika methodu
modernu 1 ka liu
La hatene methodu ida
Inan Total
Alas 83% 82% 17% 72 Fatuberliu 79% 76% 21% 72
Same 81% 79% 19% 72 Turiscai 70% 69% 30% 77
Manufahi District
80% 78% 20% 293
Ainaro 79% 75% 21% 72 Hatu Udo 90% 89% 10% 72
Hatubuilico 83% 81% 17% 72 Maubisse 57% 47% 43% 72
Ainaro District 70% 64% 30% 288
Combined District Totals
75% 72% 25% 581

41
Table 28: Knowledge of contraceptive methods by women as determined by spontaneous recall * Table 28: Koinesimentu kona ba methodu kontraseptivu husi inan sira ne’ebe sira identifika rasik
Program Area
Fem
ale
Ster
iliza
tio
n
Mal
e St
erili
zati
on
Pill
IUD
Inje
ctab
les
Imp
lan
ts
Co
nd
om
LAM
Cyc
leb
ead
s
Rh
yth
m
Met
ho
d
Oth
er
Tota
l Wo
men
Alas 14% 0% 46% 36% 78% 40% 14% 1% 17% 11% 1% 72
Fatuberliu 4% 0% 63% 26% 73% 55% 23% 4% 16% 14% 0% 72
Same 1% 0% 25% 15% 74% 31% 6% 3% 1% 3% 4% 72
Turiscai 2% 2% 52% 6% 64% 8% 0% 0% 2% 7% 5% 77
Manufahi District Total
3% 0% 36% 18% 73% 32% 8% 2% 5% 6% 3% 293
Ainaro 11% 1% 46% 21% 65% 33% 8% 12% 18% 18% 4% 72
Hatu Udo 6% 0% 50% 32% 82% 51% 3% 0% 3% 6% 1% 72
Hatubuilico 11% 0% 50% 15% 76% 36% 1% 0% 4% 3% 1% 72
Maubisse 8% 3% 28% 10% 40% 18% 10% 8% 6% 14% 10% 72
Ainaro District Total
9% 1% 41% 17% 61% 31% 7% 6% 8% 11% 5% 288
Combined District Totals
6% 1% 38% 18% 67% 32% 7% 4% 7% 9% 4% 581
*This table displays the proportion of total responses. Women could report more than one answer. *Tabela ne’e hatudu proporsionalidade husi total resposta. Inan bele reporta liu tan husi resposta ida.

42
Table 29: Women with children 0-23 months of age who are currently using any family planning method, by whether it is a modern or traditional method
Table 29: Inan ne’ebe ho oan idade fulan 0-23 mak agora dadaun uza metode planeamentu familiar modernu ka tradisional
Program Area Any Modern
Method Other Method
Not Using Contraception
Total Women
Area programa Usa methodu
modernu Usa methodu
seluk La usa methodu Inan Total
Alas 50% 1% 49% 72 Fatuberliu 39% 4% 57% 72
Same 61% 0% 39% 72 Turiscai 36% 8% 56% 77
Manufahi District Total
54% 2% 45% 293
Ainaro 27% 8% 65% 72 Hatu Udo 42% 1% 57% 72
Hatubuilico 17% 3% 80% 72 Maubisse 25% 6% 69% 72
Ainaro District Total
23% 6% 71% 288
Combined District Totals
40% 3% 57% 581

43
Table 30: Family planning methods used by women with children under 2 years of age* Table 30: Methodu planementu familiar ne’ebe uza husi inan ne’ebe iha bebe tinan 2 mai kraik
Program Area
No
t U
sin
g C
on
trac
ep
tio
n
Fem
ale
Ster
iliza
tio
n
Mal
e
Ster
iliza
tio
n
Pill
IUD
Inje
ctab
le
Imp
lan
t
Co
nd
om
LAM
Stan
dar
d
Day
s B
ead
s
Cal
end
ar
Met
ho
d
Oth
er
Tota
l W
om
en
Alas 49% 3% 0% 6% 1% 31% 8% 0% 0% 1% 1% 0% 72
Fatuberliu 57% 0% 1% 3% 0% 35% 0% 0% 0% 0% 5% 0% 72
Same 39% 0% 0% 1% 1% 52% 6% 0% 0% 0% 0% 0% 72
Turiscai 56% 0% 0% 5% 0% 31% 0% 0% 1% 0% 1% 7% 77
Manufahi District
45% 0% 0% 3% 1% 45% 5% 0% 0% 0% 1% 1% 293
Ainaro 65% 0% 0% 1% 1% 13% 6% 0% 3% 3% 8% 0% 72
Hatu Udo 57% 0% 0% 3% 0% 31% 7% 0% 1% 0% 0% 1% 72
Hatubuilico 80% 0% 0% 0% 1% 13% 1% 1% 0% 0% 3% 0% 72
Maubisse 69% 4% 1% 4% 0% 13% 0% 1% 0% 1% 3% 3% 72
Ainaro District
71% 2% 1% 2% 1% 13% 2% 1% 1% 1% 4% 1% 288
Combined District Totals
57% 1% 0% 2% 1% 30% 3% 0% 0% 1% 2% 1% 581
* Note that some rows do not add up to 100% given that these results are rounded to the nearest full number and this table includes many variables.
* Nota katak linha balu la bele aumenta tan to’o 100% tanba rezultadu sira-ne’e iha besik hela númeru kompletu (hanesan 1.13% ka 1.06%) no tabela ne’e inklui variable balu.

44
Tables of Results on Mobile Phone Ownership and Use in Manufahi and Ainaro
Table 31: Women who reported mobile phone ownership in household Table 31: Inan sira ne’ebe iha telemovel rasik iha uma
Program Area Household owns mobile
phone Household does not have mobile phone
Total women
Area Programa Iha telemovel iha uma Laiha telemovel Total Inan
Alas 36% 64% 72
Fatuberliu 60% 40% 72
Same 79% 21% 72
Turiscai 54% 46% 77
Manufahi District 69% 31% 293
Ainaro 75% 25% 72
Hatu Udo 64% 36% 72
Hatubuilico 69% 31% 72
Maubisse 58% 42% 72
Ainaro District 66% 34% 288
Combined District Total
67% 33% 581
Table 32: Number of mobile phones per household for women with any mobile phones in the home
Table 32: Numero telemovel kada uma kain husi inan ne’ebe iha telemovel ida ka liu
Program Area No phone One Two Three or more
phones Total women
Area Programa Telemovel
la iha Ida Rua
Telemovel tolu ka liu
Inan total
Alas 64% 21% 10% 5% 72
Fatuberliu 40% 32% 17% 11% 72
Same 21% 43% 25% 11% 72
Turiscai 46% 35% 12% 7% 77
Manufahi District 31% 38% 21% 10% 293
Ainaro 25% 21% 39% 15% 72
Hatu Udo 37% 37% 23% 3% 72
Hatubuilico 31% 34% 35% 0% 72
Maubisse 42% 35% 19% 4% 72
Ainaro District 34% 30% 9% 7% 288
Combined District Totals
33% 35% 24% 8% 581

45
Table 33: Percentage of women who report there is their “own” phone in the household
Table 33: Persentajen inan sira ne’ebe iha telemovel rasik
Program Area Own Phone Uses Family Phone Total Women with
Household Mobile Phone
Area Programa Telemovel rasik Uza telemovel
familia nian Total inan ho telemovel
iha uma kain
Alas 81% 19% 26
Fatuberliu 84% 14% 43 Same 68% 32% 57
Turiscai 58% 42% 46
Manufahi District 70% 30% 172
Ainaro 96% 4% 54
Hatu Udo 91% 9% 46 Hatubuilico 98% 2% 50 Maubisse 93% 7% 42
Ainaro District 95% 5% 192
Combined District Total
82% 18% 364
Table 34: Women who report using their mobile phone to send or receive text message Table 34: Inan ne’ebe iha relatori uza sira nia telemovel rasik hodi haruka no simu mensagen
Program Area Women who send or
receive SMS messages
Women who do not send or receive
messages
Women with a phone in the
household
Area Programa Inan ne’ebe simu ka haruka mensagen
Inan ne’ebe la simu ka haruka mensagen
Inan ho telemovel iha uma kain
Alas 100% 0% 26 Fatuberliu 98% 2% 43
Same 100% 0% 57 Turiscai 96% 4% 46
Manufahi District 99% 1% 172
Ainaro 98% 2% 54
Hatu Udo 96% 4% 46 Hatubuilico 94% 6% 50 Maubisse 98% 2% 42
Ainaro District 97% 3% 192
Combined District Total
98% 19% 364

46
Table 35: Frequency of text message sending among women who own mobile phones Table 35: Entre inan sira ne’ebe haruka mensagen frequentamente husi sira nia telemovel rasik
Program Area Once a day or more Once a Week Once a Month Never Women who own a
phone in their household
Area Programa Loron ida dala ida
ka liu Semana ida dala
ida Fulan ida dala ida Nunka
Inan ne’ebe iha telemovel rasik iha sira nia uma kain
Alas 77% 19% 0% 4% 26
Fatuberliu 74% 24% 0% 2% 43
Same 81% 12% 4% 4% 57
Turiscai 52% 33% 5% 10% 46
Manufahi District Total
77% 16% 3% 4% 167
Ainaro 58% 23% 8% 11% 54
Hatu Udo 76% 11% 2% 11% 46
Hatubuilico 42% 26% 0% 32% 50
Maubisse 86% 10% 2% 2% 42
Ainaro District Total
67% 17% 3% 13% 191
Combined District Total
72% 16% 3% 8% 358

47
Table 36: Methods reported by women to charge mobile phones Table 36: Relaori kona ba metode husi inan sira atu chas telemovel
Program Area Electricity at
home Solar charger
at home Battery at
home Electricity other site
Solar charger at other site
Other1 Total Women with Household Mobile
Phone
Area Programa
Eletricidade iha uma
Solar cell iha uma
Bataria iha Uma
Eletricidade iha fatin seluk
Solar cell iha fatin seluk
Seluk1 Total inan ho
telemovel iha uma
Alas 12% 38% 12% 4% 23% 12% 26
Fatuberliu 56% 7% 0% 9% 29% 0% 43
Same 51% 9% 8% 11% 15% 6% 53*
Turiscai 36% 26% 3% 8% 25% 2% 46
Manufahi District Totals
34% 10% 1% 20% 33% 2% 168
Ainaro 67% 0% 0% 19% 13% 2% 54
Hatu Udo 24% 7% 0% 26% 35% 9% 46
Hatubuilico 10% 24% 4% 2% 60% 0% 50
Maubisse 26% 12% 0% 31% 31% 0% 42
Ainaro District Totals
47% 13% 6% 10% 18% 5% 192
Combined District Total
41% 11% 4% 15% 26% 3% 360
1 Other methods include: own generator, generator in another location, another person’s generator, and the community’s office. *3 non-responses in Same 1 Métodu seluk inklui: jeradór rasik, jeradór iha fatin seluk, jeradór ema seluk nian, no komunidade nia ofísiu. *Participante nain 3 la fo resposta iha Same

48
Table 37: Reported distance to cell phone signal among women with children 0-23 months of age who have a cell phone in their household
Table 37: Relatori kona ba distancia ba signal telemovel husi inan ho oan idade fulan 0-23 ne’ebe iha telemovel rasik iha uma
Program Area Have Signal at home or within
5 minute Walk Total Women with
Household Mobile Phone
Area Programa Hetan Signal iha uma ka lao 5
minutus Total inan ho telemovel iha
uma
Alas 85% 25
Fatuberliu 96% 43
Same 96% 57
Turiscai 94% 46
Manufahi District 95% 172
Ainaro 100% 54
Hatu Udo 100% 46
Hatubuilico 100% 50
Maubisse 98% 42
Ainaro District 99% 192
Combined District Total
97% 364
Table 38: Level of Tetun language literacy reported by women with children 0-23 months of age Table 38: Nivel education iha lingua Tetun tuir relatori husi inan ne’ebe iha oan idade fulan 0-23
Program Area Cannot Speak, Read or Write
Speak Only Speak and Read Only
Speak, Read and Write
Total Women
Area Programa La koalia, le’e
ka hakerek Koalia deit
Koalia no le’e deit
Koalia, le’e no hakerek
Total Inan
Alas 18% 17% 7% 58% 72
Fatuberliu 8% 8% 0% 85% 72
Same 8% 21% 4% 67% 72
Turiscai 6% 14% 9% 71% 77
Manufahi District 9% 18% 5% 68% 293
Ainaro 0% 22% 0% 78% 72
Hatu Udo 6% 32% 1% 61% 72
Hatubuilico 1% 43% 8% 47% 72
Maubisse 0% 54% 3% 43% 72
Ainaro District 1% 40% 3% 56% 288
Combined District Total
5% 29% 4% 62% 581

49
Table 39: Available assistance in reading tetun messages by women who reported being unable to read the Tetun language themselves (multiple answers reported*)
Table 39: Iha ema ne’ebe ajuda le’e mensagen iha tetum ba inan sira ne’ebe tuir relatori labele atu le’e iha lian Tetun
Program Area
Husband Child Other Family
Member Neighbor
Area Programa Laen/Kaben Oan Membru familia
seluk Vizinho
Alas 40% 20% 28% 4% Fatuberliu 58% 26% 32% 8%
Same 29% 10% 33% 38% Turiscai 20% 61% 39% 16%
Manufahi District
32% 17% 33% 29%
Ainaro 19% 13% 69% 13% Hatu Udo 41% 15% 41% 0%
Hatubuilico 31% 19% 47% 6% Maubisse 54% 33% 21% 5%
Ainaro District 42% 25% 36% 6%
Combined District Total
38% 21% 35% 15%
*This table displays the proportion of total response. Women could report more than one person.
*Tabela ne’e hatudu proporsaun totál resposta. Feto sira bele relata liu hosi ema ida.

50
Tables on Results of SMS Message Preferences in Manufahi District
Table 40: Preferred language for text messages among women in Manufahi District Table 40: Lingua ne’ebe prefere liu ba texto mensagen nian husi inan iha Distritu Manufahi
Program Area Tetun Bahasa Mambae Other1 Total
women
Area Programa
Tetun Bahasa Mambae Seluk1 Total inan
Alas 100% 0% 0% 0% 72
Fatuberliu 95% 1% 0% 4% 72
Same 99% 0% 0% 1% 72
Turiscai 97% 0% 3% 0% 77
Manufahi District Total
98% 0% 0% 1% 293
1 Other responses included Tetun Terik and no preference. Portuguese and English were other options, but no women reported either language.
1 Resposta seluk inklui Tetun Terik no laiha preferénsia. Portugés no Inglés hanesan opsaun seluk, maibé laiha feto ida mak relata prefere dalen dalen sira-ne’e.
Table 41: Preferred time of day to receive health-related text messages in Manufahi District Table 41: Tempu iha loron ne’ebe prefere liu atu simu mensagen saúde nian iha Distrito Manufahi
Program Area
Morning Afternoon Evening No Preference Total
women
Area Programa
Dader Lokraik Kalan Laiha
preferensia Total inan
Alas 51% 27% 14% 7% 72
Fatuberliu 72% 16% 10% 2% 72
Same 28% 44% 14% 14% 72
Turiscai 18% 27% 16% 40% 77
Manufahi District Total
36% 36% 14% 15% 293

Health Alliance International
Maternal and Newborn Health
and Mobile Phone Utilization in Manufahi and Ainaro
Districts
A Final Knowledge, Practices and Coverage Survey
for the Mobile Moms/Liga Inan Program
April 2016
Annex 4: 2015 Final KPC Survey Data Tables

1
Tables for Results on Participant Demographics
Table 1: Demographics of study population*
Tabela 1: Estudu demográfiku populasaun*
Area Average age of Woman
(Years)
Average Years of School
Average Number of Children per Woman
Number of Women
interviewed
Area Medida idade
inan (Tinan)
Medida tinan
eskola
Medida númeru oan husi kada inan
Númeru inan tuir intervista
Alas 28.0 7.4 3.2 72
Fatuberliu 26.0 9.5 2.6 72
Same 26.6 9.4 2.7 72 Turiscai 29.0 8.4 3.7 72
Manufahi District Total
27.0 9 2.9 288
Ainaro 27.9 8.5 3.2 72
HatuUdo 26.9 8.7 2.8 72
Hatubuilico 31.0 4.3 4.8 72
Maubisse 26.6 6.4 3.6 72
Ainaro District Total
27.9 6.9 3.6 288
Combined District Total
27.4 8 3.2 576
*The data presented in this and all following tables are weighted with respect to variations at the sample level, the subdistrict population, and district population as follows:
at the subdistrict level: the data is weighted with respect to variations in sample size only Subdistrict weight was used in baseline analysis but it is not needed in the follow-up analysis because all enumeration areas (EA) have 9 women (households) while there were different counts of women per EA at baseline.
at the district level: the data is weighted with respect to variations in sample size and the variations in population of the subdistrict
at the combined district level: the data is weighted with respect to variations in sample size, the variations in population of the subdistrict, and variations in the population of the district

2
Histograms for Distribution of Women’s Age, Years of Schooling and Number of Children
Figure 1: Distribution of participants’s age in 2 year increments from Manufahi and Ainaro Figura 1: Distribusaun partisipante nia idade iha grupu tinan rua husi Manufahi no Ainaro
Figure 2: Distribution of years of school attended by participants from Manufahi and Ainaro Figura 2: Númeru tinan partisipante atende eskola husi Manufahi no Ainaro
Figure 3: Distribution of number of children per woman from Manufahi and Ainaro Figura 3: Distribusaun númeru oan kada inan husi Manufahi no Ainaro
05
10
15
Pe
rcen
t
10 20 30 40 50
Participant Age
01
02
03
0
Pe
rcen
t
0 5 10 15 20
Years of school attended
05
10
15
20
25
Pe
rcen
t
0 5 10 15
Number of childern per woman

3
Table 2: Type of work reported by participants
Tabela 2: Tipu servisu hato’o husi partisipante sira
Area No Outside
Work Handicrafts Harvesting
Selling Foods
Shop Keeper
Household Cleaner
Salaried Worker
Total Women
Area Programa Laiha servisu
liur Artezenatu Halo toos
Faan hahan
Faan kios Hamos rai Servisu
simu salariu
Inan total
Alas 82% 1% 7% 1% 4% 0% 4% 72 Fatuberliu 79% 0% 7% 0% 7% 0% 6% 72
Same 75% 0% 15% 0% 11% 1% 4% 72 Turiscai 56% 1% 24% 0% 14% 0% 6% 72
Manufahi District Total
74% 0.3% 14% 0.2% 10% 1% 5% 288
Ainaro 75% 3% 4% 0% 3% 0% 17% 72 Hatu Udo 79% 3% 8% 0% 6% 0% 6% 72
Hatubuilico 42% 0% 61% 0% 3% 0% 3% 72 Maubisse 79% 0% 29% 1% 3% 0% 3% 72
Ainaro District Total
70% 1% 26% 0.5% 3% 0% 6% 288
Combined District Totals
72% 0.7% 20% 0.4% 7% 0.5% 6% 576
Women could report more than one answer. Inan bele reporta liu tan husi resposta ida

4
Table 3: Floor and roofing materials used among survey participants
Tabela 3: Materia ne’ebé uza ba uma kakuluk no rai (Uma Laran) husi partisipante
Program Area
Roof Material Floor Material Total
Women Palm Leaves
Sheet Iron Other Earth Concrete Wood/
Bamboo Other
Area Programa
Uma Kakuluk Rai iha Uma Laran
Inan total Tali
Tahan Kalen Seluk Rai Semente
Ai ou Fafulu ka Au
Seluk
Alas 49% 51% 0% 38% 38% 24% 1% 72
Fatuberliu 7% 93% 0% 33% 64% 1% 1% 72
Same 10% 85% 6% 46% 49% 3% 3% 72
Turiscai 1% 97% 1% 58% 42% 0% 0% 72
Manufahi District Total
14% 83% 4% 45% 48% 5% 2% 288
Ainaro 10% 90% 0% 60% 35% 0% 6% 72
HatuUdo 35% 64% 1% 44% 53% 3% 0% 72
Hatubuilico 1% 89% 10% 64% 36% 0% 0% 72
Maubisse 14% 86% 0% 64% 36% 0% 0% 72
Ainaro District Total
14% 84% 2% 60% 39% 0.5% 1% 288
Combined District Totals
13% 84% 3% 52% 43% 3% 2% 576

5
Table 4: Women who report having specific household commodities*
Tabela 4: Inan ne’ebé relata iha sasan uma laran espesífiku
Program Area Electricity Radio Television Bicycle Motor bike Car/ Truck Solar Cell Generator Total
Women
Area Programa Eletrisidade Radio Televizaun Bisikleta Motor Kareta ka
trek Sólar Jeneradór
Inan total
Alas 51% 38% 24% 31% 49% 1% 88% 7% 72 Fatuberliu 88% 29% 35% 44% 44% 8% 53% 7% 72
Same 60% 46% 44% 21% 43% 3% 35% 4% 72 Turiscai 61% 29% 26% 11% 32% 0% 79% 7% 72
Manufahi District Total
62% 41% 39% 24% 43% 3% 49% 5% 288
Ainaro 78% 39% 47% 19% 39% 11% 13% 10% 72 Hatu Udo 69% 28% 38% 17% 43% 1% 46% 6% 72
Hatubuilico 21% 38% 13% 13% 14% 1% 74% 11% 72 Maubisse 64% 46% 24% 4% 35% 6% 50% 11% 72
Ainaro District Total
60% 40% 30% 12% 33% 5% 45% 10% 288
Combined District Totals
61% 40% 34% 18% 38% 4% 47% 8% 576
*Women could report more than one answer.

6
Table 5: Percent of women who reported having difficulty with vision, hearing, concentration, communication or activities of daily living
Tabela 5: Persentajen ba feto ne’ebé hato’o katak sira iha difikuldade haree, rona, konsentrasaun, komunikasaun ka atividade ba moris lor-loron
Area Vision Hearing Walking/ Climbing
Remembering/ Concentrating
Self-Care Communi
cating
Women who report having a lot of difficulty
or could not perform one or more actions
Area Programa Haree Rona La’o/ Sa’e
Foho Lembra/
konsentra Kuidadu
aan Komunika
Inan ne’ebé hatoo katak sira iha difikuldade
barak no labele halo aksaun ida ka rua
Alas 1% 0% 0% 0% 0% 0% 1% Fatuberliu 1% 0% 3% 0% 0% 0% 4%
Same 1% 0% 1% 1% 0% 0% 3% Turiscai 1% 1% 0% 0% 0% 0% 3%
Manufahi District Total
1% 0.2% 1% 0.9% 0% 0% 3%
Ainaro 1% 0% 0% 3% 0% 0% 4% Hatu Udo 0% 0% 0% 1% 0% 0% 1%
Hatubuilico 0% 0% 1% 3% 0% 0% 4% Maubisse 0% 0% 0% 0% 0% 0% 0%
Ainaro District Total
0.4% 0% 0.3% 1% 0% 0% 2%
Combined District Totals
0.9% 0.1% 0.8% 1% 0% 0% 2.5%
*Women could report more than one answer.

7
Tables for Results on Maternal and Newborn Health
Table 6: Percent of women who received antenatal care (ANC) from a skilled health provider Tabela 6: Persentajen inan ne’ebé simu konsulta isin rua (ANC) husi pesoál saúde
Program Area Percent women who
received at least 1 ANC visit
Percent women who received 4 or more
ANC visits No ANC visits
Area Programa
Persentajen husi inan ne’ebé simu visita ANC
dala 1 ka liu
Persentajen husi inan ne’ebé simu visita ANC
dala 4 ka liu
Persentajen husi inan ne’ebé la
simu ANC
Alas 99% 93% 1% Fatuberliu 100% 83% 0%
Same 93% 82% 7% Turiscai 86% 81% 14%
Manufahi District Total
94% 85% 6%
Ainaro 97% 84% 3% Hatu Udo 97% 94% 3%
Hatubuilico 85% 69% 15% Maubisse 93% 78% 7%
Ainaro District Total
93% 81% 7%
Combined District Totals
93% 82% 7%
Table 7: Type of health care provider women saw for antenatal care Tabela 7: Tipu kuidadu saúde husu pesoál saúde sira ne’ebé inan sira buka ba ANC
Program Area Doctor Nurse Midwife Traditional
Birth Attendant
Other
Area Programa Doutór Enfermeira Parteira Dayang Seluk
Alas 62% 18% 79% 3% 0% Fatuberliu 36% 6% 89% 1% 0%
Same 55% 13% 75% 2% 0% Turiscai 26% 13% 90% 0% 0%
Manufahi District Total
51% 13% 79% 2% 0%
Ainaro 36% 14% 86% 0% 0% HatuUdo 36% 10% 80% 0% 0%
Hatubuilico 31% 20% 85% 0% 0% Maubisse 82% 22% 51% 0% 5%*
Ainaro District Total
52% 18% 71% 0% 2%
Combined District Totals
51% 15% 75% 1% 1%
**Women could have seen multiple types of health care providers during their pregnancy

8
Table 8: Reported sites of antenatal care among women who reported they attended at least one ANC visit* Tabela 8: Reporta Fatin nebe’e inan uja atu hetan konsulta isin rua entre inan nebe’e reporta katak sira atende Visita ANC maizumenus dala ida.
Program Area Home Hospital Maternity/
Community Health Center (CHC)
Health Post
SISCA Outreach
Event Private Clinic
Number of Women who received at least 1 ANC
Area Programa Uma Ospitál Maternidade/CHC Postu Saúde
SISCa Eventu
komunidade
Klinika privadu
Inan ne’ebé simu ANC dala
1 ka liu
Alas 1% 1% 41% 52% 48% 0% 0% 71 Fatuberliu 0% 1% 81% 17% 7% 0% 1% 72
Same 0% 3% 81% 25% 9% 0% 0% 67 Turiscai 0% 3% 94% 2% 5% 0% 2% 62
Manufahi District Total
0% 3% 77% 25% 13% 0% 0% 272
Ainaro 1% 11% 60% 26% 4% 1% 0% 70 HatuUdo 0% 1% 51% 47% 1% 0% 1% 70
Hatubuilico 2% 5% 49% 33% 5% 0% 15% 61 Maubisse 0% 72% 13% 16% 9% 3% 5% 67
Ainaro District Total
1% 31% 39% 27% 6% 2% 5% 268
Combined District Totals
0% 17% 58% 26% 10% 1% 3% 540
*Women could report more than one answer. *Inan bele reporta liu tan husi resposta ida
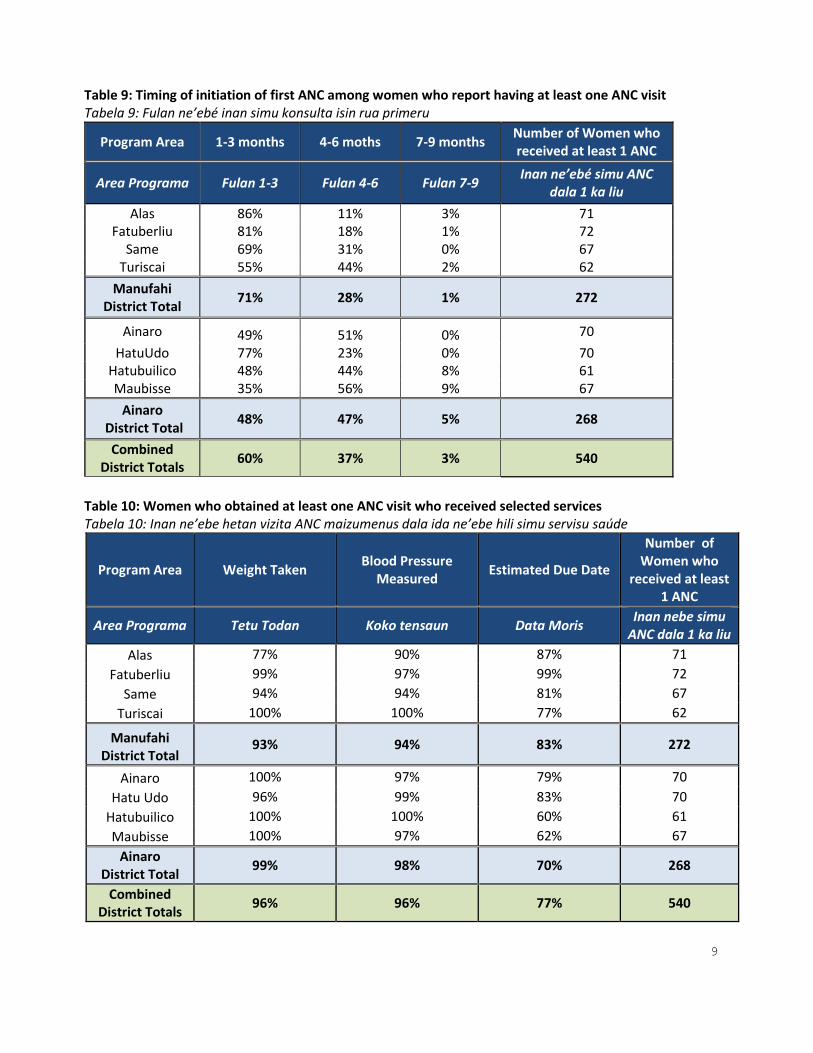
9
Table 9: Timing of initiation of first ANC among women who report having at least one ANC visit Tabela 9: Fulan ne’ebé inan simu konsulta isin rua primeru
Program Area 1-3 months 4-6 moths 7-9 months Number of Women who received at least 1 ANC
Area Programa Fulan 1-3 Fulan 4-6 Fulan 7-9 Inan ne’ebé simu ANC
dala 1 ka liu
Alas 86% 11% 3% 71 Fatuberliu 81% 18% 1% 72
Same 69% 31% 0% 67 Turiscai 55% 44% 2% 62
Manufahi District Total
71% 28% 1% 272
Ainaro 49% 51% 0% 70
HatuUdo 77% 23% 0% 70 Hatubuilico 48% 44% 8% 61 Maubisse 35% 56% 9% 67
Ainaro District Total
48% 47% 5% 268
Combined District Totals
60% 37% 3% 540
Table 10: Women who obtained at least one ANC visit who received selected services Tabela 10: Inan ne’ebe hetan vizita ANC maizumenus dala ida ne’ebe hili simu servisu saúde
Program Area Weight Taken Blood Pressure
Measured Estimated Due Date
Number of Women who
received at least 1 ANC
Area Programa Tetu Todan Koko tensaun Data Moris Inan nebe simu
ANC dala 1 ka liu
Alas 77% 90% 87% 71
Fatuberliu 99% 97% 99% 72
Same 94% 94% 81% 67
Turiscai 100% 100% 77% 62
Manufahi District Total
93% 94% 83% 272
Ainaro 100% 97% 79% 70
Hatu Udo 96% 99% 83% 70
Hatubuilico 100% 100% 60% 61
Maubisse 100% 97% 62% 67
Ainaro District Total
99% 98% 70% 268
Combined District Totals
96% 96% 77% 540

10
Table 11: Where women learn about danger signs of pregnancy Tabela 11: Inan ne’ebé mak inan aprende kona-ba sinál perigu durante isin rua
Program Area
Personal knowledge,
experience, or observation
Health Worker
In Lisio (maternal booklet)
On a Poster/ Banner
Liga Inan Message/Cell Phone
Radio Film PSF
(CHW)
Women who recognized at least one danger sign
Area Programa
Koñesimentu pesoál,
esperiensia, ka observasaun
Pesoál saúde
Iha Lision (booklet ba inan
sira sira)
Iha poster/ banner
Mensajen Liga
Inan/Telfone
Radio Filme PSF
Inan ne’ebé hatene de’it pelumenuz sinál perigu
ida
Alas 57% 60% 13% 0% 5% 0% 3% 2% 60 Fatuberliu 54% 34% 7% 0% 0% 0% 0% 2% 59
Same 50% 33% 3% 2% 2% 2% 0% 0% 60 Turiscai 47% 49% 2% 0% 0% 0% 0% 0% 53
Manufahi District Total
51% 38% 5% 1% 2% 1% 0.4% 0.4% 232
Ainaro 66% 26% 3% 2% 0% 3% 3% 0% 61 HatuUdo 49% 51% 9% 6% 0% 0% 4% 2% 53
Hatubuilico 64% 19% 8% 0% 2% 0% 2% 0% 53 Maubisse 66% 29% 2% 2% 0% 4% 0% 0% 56
Ainaro District Total
63% 30% 5% 2% 0.4% 2% 2% 0.3% 223
Combined District Totals
57% 34% 5% 2% 1% 2% 1% 0.4% 455
*Women could report more than one answer. *Inan bele reporta liu tan husi resposta ida.

11
Table 12: Women who received tetanus toxoid (TT) vaccinations during their last pregnancy and over their lifetime Tabela 12: Inan ne’ebé simu vasina tetanus toxoid (TT) durante isin rua ba sira nia oan ida ikus (kiik) ka
inan nebee simu durante moris tomak
Program Area Last pregnancy Lifetime
Any TT 2+ TT 2+ TT Never
Area Programa Isin rua ikus Durante moris tomak
Dala 1 ka liu 2+ TT 2+ TT Nunka
Alas 68% 65% 85% 6%
Fatuberliu 76% 60% 81% 3%
Same 78% 65% 82% 4%
Turiscai 63% 47% 72% 6%
Manufahi District Total
75% 63% 81% 4%
Ainaro 67% 58% 82% 4%
Hatu Udo 74% 59% 74% 6%
Hatubuilico 57% 61% 60% 21%
Maubisse 66% 60% 72% 6%
Ainaro District Total
66% 59% 72% 8%
Combined District Totals
70% 61% 77% 6%
Table 13: Percent of women who received iron supplementation during their last pregnancy Tabela 13: Persentajen inan ne’ebé hemu aimoruk aumenta ran durante isin rua ikus
Program Area Women who received
any iron tablets Women who took 90
tablets or more
Area Programa Inan ne’ebé hemu
tableta aumenta ran Inan ne’ebé hemu
tablet 90 ka liu
Alas 99% 86%
Fatuberliu 100% 75%
Same 93% 50%
Turiscai 89% 50%
Manufahi District Total
94% 57%
Ainaro 94% 74%
Hatu Udo 97% 60%
Hatubuilico 89% 38%
Maubisse 93% 56%
Ainaro District Total
93% 57%
Combined District Totals
94% 57%
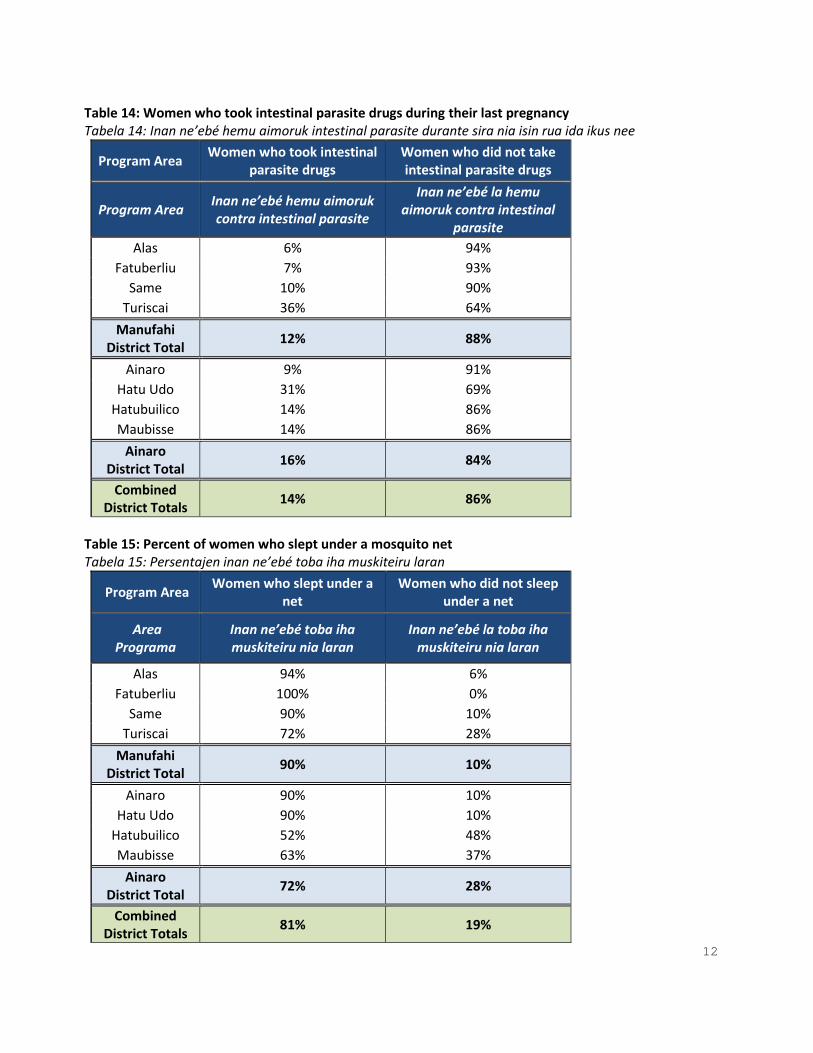
12
Table 14: Women who took intestinal parasite drugs during their last pregnancy Tabela 14: Inan ne’ebé hemu aimoruk intestinal parasite durante sira nia isin rua ida ikus nee
Program Area Women who took intestinal
parasite drugs Women who did not take intestinal parasite drugs
Program Area Inan ne’ebé hemu aimoruk contra intestinal parasite
Inan ne’ebé la hemu aimoruk contra intestinal
parasite
Alas 6% 94%
Fatuberliu 7% 93%
Same 10% 90%
Turiscai 36% 64%
Manufahi District Total
12% 88%
Ainaro 9% 91%
Hatu Udo 31% 69%
Hatubuilico 14% 86%
Maubisse 14% 86%
Ainaro District Total
16% 84%
Combined District Totals
14% 86%
Table 15: Percent of women who slept under a mosquito net Tabela 15: Persentajen inan ne’ebé toba iha muskiteiru laran
Program Area Women who slept under a
net Women who did not sleep
under a net
Area Programa
Inan ne’ebé toba iha muskiteiru nia laran
Inan ne’ebé la toba iha muskiteiru nia laran
Alas 94% 6%
Fatuberliu 100% 0%
Same 90% 10%
Turiscai 72% 28%
Manufahi District Total
90% 10%
Ainaro 90% 10%
Hatu Udo 90% 10%
Hatubuilico 52% 48%
Maubisse 63% 37%
Ainaro District Total
72% 28%
Combined District Totals
81% 19%

13
Table 16: Reported methods available for women to contact midwives around the time of birth* Tabela 16: Relatoriu ba metodu sira ne’ebé iha ba inan sira hodi kontakto parteira iha tempu nebee atu partus*
Program Area Go directly to meet health
provider
By household phone
By other phone Send messenger Not able to
contact midwife
Area Programa Ba hasoru
pesoal saude Husi telefone
uma Husi telefone
seluk Haruka
mensajen
La bele kontaktu parteira
Alas 20% 84% 4% 15% 6%
Fatuberliu 13% 79% 3% 28% 1%
Same 11% 84% 3% 5% 1%
Turiscai 15% 81% 3% 39% 6%
Manufahi District Total
13% 83% 3% 13% 2%
Ainaro 13% 72% 1% 16% 4%
HatuUdo 3% 75% 0% 54% 4%
Hatubuilico 18% 18% 7% 33% 19%
Maubisse 22% 56% 8% 24% 11%
Ainaro District Total
16% 57% 5% 29% 10%
Combined District Totals
14% 70% 4% 21% 6%
* Women could respond to more than one method. *Inan ne’ebé fo resposta liu tan metod

14
Table 17: Percent of women who reported planning for delivery Tabela 17: Persentajen inan ne’ebé halo planeamentu ba partus
Program Area Women who
said they saved money
Women who said they arranged
transport
Women who decided on a
place to deliver
Women who reported they did at least one of
the key planning actions
Area Programa
Inan ne’ebé hatete katak sira rai osan
Inan ne’ebé hatete katak sira aranja transporte
Inan ne’ebé deside fatin atu
tuur ahi
Inan ne’ebe hatoo sira halo pelumenuz ida ba aksaun planeamentu
importante
Alas 90% 57% 92% 100% Fatuberliu 93% 70% 92% 99%
Same 90% 67% 94% 99% Turiscai 83% 46% 83% 96%
Manufahi District Total
90% 63% 93% 98%
Ainaro 83% 64% 69% 96% HatuUdo 82% 61% 93% 99%
Hatubuilico 53% 17% 69% 87% Maubisse 78% 42% 82% 94%
Ainaro District Total
75% 45% 78% 94%
Combined District Totals
82% 54% 85% 96%
Table 18: Highest skilled attendant at birth Tabela 18: Persentajen inan ne’ebé simu suporta husi pesoál saúde treinado durante partus ida ikus nee
Program Area Skilled birth attendant
present (Doctor, Nurse, Midwife)
Traditional Birth Attendant
Other (Family,
Friends, PSF) No One
Area Programa Prezensa pesáal saude
treinado (Doutór, Infermeiro, Parteira)
Parteira tradisionál Seluk
(Familia, Kolega, PSF)
Laiha ema ida
Alas 63% 29% 5% 3% Fatuberliu 72% 19% 9% 0%
Same 67% 24% 8% 1% Turiscai 26% 19% 49% 6%
Manufahi District Total
62% 23% 13% 2%
Ainaro 53% 22% 25% 0% Hatu Udo 42% 29% 29% 0%
Hatubuilico 22% 22% 46% 10% Maubisse 31% 6% 55% 8%
Ainaro District Total
36% 17% 42% 5%
Combined District Totals
49% 20% 27% 4%

15
Table 19: Attendants at women’s most recent deliver Tabela 19: Ema ne’ebé asiste inan durante partus
Program Area
Doctor Nurse Midwife Traditional
Birth Attendant
PSF Husband
Other
Relative/
Friend
No One
Area Programa
Doutór Enfermei
ru Parteira Dayang PSF Laen
Familia
seluk/
Kolega
Laiha
ema ida
Alas 35% 7% 49% 29% 0% 29% 39% 3% Fatuberliu 8% 1% 72% 19% 1% 40% 63% 0%
Same 15% 4% 58% 24% 1% 39% 46% 1% Turiscai 8% 0% 24% 19% 1% 50% 65% 6%
Manufahi District Total
16% 4% 55% 23% 1% 39% 49% 2%
Ainaro 21% 4% 44% 22% 0% 38% 54% 0% HatuUdo 19% 3% 33% 29% 0% 65% 58% 0%
Hatubuilico 3% 0% 21% 22% 1% 44% 32% 10% Maubisse 19% 3% 22% 6% 4% 38% 43% 8%
Ainaro District Total
16% 3% 29% 17% 2% 44% 46% 5%
Combined District Totals
16% 3% 42% 20% 2% 41% 48% 4%

16
Table 20: Place of last delivery for women with a child 0-23 months of age Tabela 20: Fatin partu ida ikus nian ba inan ho oan idade fulan 0-23
Program Area At Home Health facility
(Hospital, CHC, or health post)
Area Programa Iha uma Fasilidade Suade
(Ospitál, CHC, ka postu saude)
Alas 74% 26%
Fatuberliu 53% 47%
Same 39% 61%
Turiscai 89% 11%
Manufahi District Total
51% 49%
Ainaro 51% 49%
HatuUdo 67% 33%
Hatubuilico 92% 8%
Maubisse 76% 24%
Ainaro District Total
72% 28%
Combined District Totals
61% 39%

17
Table 21: Method of transportation used to reach health facility among women who delivered at a health facility Tabela 21: Metode uza transporte atu ba to iha fasilidade saúde ba inan sira ne’ebé partus iha fasilidade saúde
Program Area Walk Private Car Public Ambulance or MOH vehicle
Other* Women who delivered in a health facility
Area Programa Lao Kareta Privadu Transporte
públiko Ambulansia ka
kareta MdS Seluk*
Inan ne’ebé partus iha
fasilidade saúde
Alas 0% 0% 0% 100% 0% 18
Fatuberliu 6% 6% 3% 77% 9% 34
Same 0% 5% 0% 89% 7% 44
Turiscai 0% 13% 0% 50% 38% 8
Manufahi District Total
1% 5% 0% 87% 8% 104
Ainaro 11% 11% 6% 60% 11% 35
HatuUdo 13% 0% 4% 58% 25% 24
Hatubuilico 29% 0% 0% 57% 14% 7
Maubisse 12% 6% 6% 47% 29% 17
Ainaro District Total
13% 7% 5% 55% 20% 83
Combined District Totals
5% 5% 2% 75% 12% 187
*Other methods of transport included: motorbike, paid transport (angguna), and government vehicle (police and firefighter). *Metodu transporte seluk inklui: motor, selu transporte (angguna), no kareta governu (polisia no bombeirus)

18
Table 22: Reported travel time to nearest health facility where a woman could deliver Tabela 22: Relatoriu kona-ba tempu viajen ba besik fasilidade saúde atu hodi partus
Program Area 30 minutes or
less 30-60
minutes 60-90
minutes 90-120
minutes 120-150 minutes
150-180 minutes
Greater than 180 minutes
Area Programa
Minutu 30 ka menus Minutu 30-60
Minutu 60-90
Minutu 90-120 Minutu 120-
150 Minutu 150-
180 Liu tan minutu
180
Alas 31% 22% 0% 36% 2% 8% 2%
Fatuberliu 56% 19% 2% 12% 7% 3% 2%
Same 54% 24% 5% 12% 2% 5% 0%
Turiscai 26% 22% 11% 14% 10% 10% 7%
Manufahi District Total
48% 23% 5% 15% 3% 5% 1%
Ainaro 46% 33% 6% 8% 1% 3% 3%
HatuUdo 54% 24% 13% 10% 0% 0% 0%
Hatubuilico 22% 22% 17% 12% 7% 1% 19%
Maubisse 24% 27% 11% 27% 3% 5% 5%
Ainaro District Total
34% 27% 11% 16% 3% 3% 6%
Combined District Totals
41% 25% 8% 15% 3% 4% 4%

19
Table 23: Women’s experiences during delivery in a health facility Tabela 23: Inan ne’ebé esperiensia durante partus iha fasilidade saúde inan
Program Area
Were you left alone by staff?
Were you yelled at?
Did you deliver in a private area?
Was a bed sheet provided? Women who
delivered at a health facility Yes No Yes No Yes No Yes No
Area Programa
Husik mesak hela husi pesoál saúde?
Hakilar ba itaboot? Ita boot partus iha
fatin privadu ka la’e? Fo lensól ba ita
boot? Inan ne’ebé partus iha fasilidade
saúde Los La’e Los La’e Los La’e Los La’e
Alas 0% 100% 16% 84% 90% 10% 84% 16% 19
Fatuberliu 3% 97% 9% 91% 91% 9% 88% 12% 34
Same 2% 98% 9% 91% 91% 9% 89% 11% 44
Turiscai 13% 87% 0% 100% 100% 0% 100% 0% 8
Manufahi District Total
2% 97% 9% 91% 91% 9% 89% 11% 105
Ainaro 6% 94% 6% 94% 77% 23% 77% 23% 35
Hatu Udo 8% 92% 4% 96% 92% 8% 96% 4% 24
Hatubuilico 20% 80% 0% 100% 100% 0% 100% 0% 6
Maubisse 6% 94% 18% 82% 88% 12% 82% 18% 17
Ainaro District Total
7% 93% 9% 91% 85% 15% 84% 16% 82
Combined District Totals
4% 96% 9% 91% 89% 11% 87% 13% 187

20
Table 24: Experiences women had heard about delivering in a health facility among women who delivered their last child at home Tabela 24: Inan rona ona esperiensia oinsá partus iha fasilidade saúde kona-ba inan ne’ebé partus sira nia oan iha uma
Program Area Woman was left alone Woman was yelled at
Yes No Yes No
Area Programa Inan ne’ebé husi mesak Inan ne’ebé hakilar ba
Los La’e Los La’e
Alas 17% 83% 40% 60% Fatuberliu 4% 96% 17% 83%
Same 13% 87% 28% 72% Turiscai 7% 93% 25% 75%
Manufahi District Total 11% 89% 28% 72%
Ainaro 17% 83% 32% 68% Hatu Udo 19% 81% 35% 65%
Hatubuilico 14% 86% 18% 82% Maubisse 17% 83% 47% 53%
Ainaro District Total 17% 83% 35% 65%
Combined District Totals 14% 86% 31% 69%
Table 25: Percentage of children 0-23 months of age who were placed on mother’s bare chest immediately after birth Tabela25: Persentajen bebé ne’ebé idade fulan 0 – 23 rai iha inan nia hirus matan kedas depois de partus
Program Area Percentage of children who were placed
on mother’s bare chest immediately Percentage of children
who were not
Area Programa Persentajen labarik ne’ebé tau iha inan
nia hirus matan kedas
Persentajen labarik ne’ebé lae tau iha inan nia hirus
matan
Alas 84% 16% Fatuberliu 75% 25%
Same 76% 24% Turiscai 29% 71%
Manufahi District Total 71% 29%
Ainaro 69% 31% HatuUdo 56% 44%
Hatubuilico 22% 78% Maubisse 49% 51%
Ainaro District Total 50% 50%
Combined District Totals
61% 39%

21
Table 26: Percentage of children 0-23 months of age whose first bath was delayed 6 or more hours after delivery Tabela 26: Persentajen bebé ne’ebé fulan 0 – 23 haris tarde iha oras 6 ka liu tan depois de partus
Program Area Percentage of children bathed
0-5 hours Percentage of children whose bath was
delayed 6 or more hours
Area Programa Persentajen labarik ne’ebé
haris iha oras 0-5 Persentajen labarik ne’ebé haris tarde iha
oras 6 ka liu
Alas 22% 78% Fatuberliu 18% 82%
Same 25% 75% Turiscai 43% 57%
Manufahi District Total
26% 74%
Ainaro 24% 76% Hatu Udo 15% 85%
Hatubuilico 61% 39% Maubisse 56% 44%
Ainaro District Total
42% 58%
Combined District Totals
34% 66%
Table 27: Percent of women who breastfed Tabela 27: Persetajen inan ne’ebé fo susu
Program Area Child received breastmilk Child never received breastmilk
Area Bebé ne’ebé simu susu been Bebé ne’ebé nungka simu susu
been
Alas 96% 4% Fatuberliu 99% 1%
Same 92% 8% Turiscai 99% 1%
Manufahi District Total
94% 6%
Ainaro 96% 4% Hatu Udo 96% 4%
Hatubuilico 96% 4% Maubisse 100% 0%
Ainaro District Total
97% 3%
Combined District Totals
96% 4%

22
Table 28: Percentage of children 0-23 months of age who received skin-to-skin contact after birth Tabela 28: Persentajen bebé ne’ebé fulan 0 – 23 ne’ebé tau iha inan nia hirus matan iha oras ida nia laran depois de partu
Program Area
Children who were put on the bare chest
within 1 hour
Children who were put on the bare chest more than 1 hour after birth
Children who were never placed on bare
chest after birth
Alas 71% 9% 20% Fatuberliu 65% 8% 27%
Same 68% 8% 24%
Turiscai 29% 0% 71%
Manufahi District Total
64% 7% 29%
Ainaro 58% 11% 31% Hatu Udo 44% 11% 45%
Hatubuilico 18% 3% 79% Maubisse 39% 10% 51%
Ainaro District Total
40% 9% 51%
Combined District Totals
52% 8% 40%
Table 29: Percentage of children 0-23 months of age who were put to the breast within one hour after delivery and percentage who were given colostrum Tabela 29: Persentajen husi oan idade fulan 0-23 ne’ebé simu susu ona iha oras ida nia laran depois
the partus no simu susuben kinur
Program Area Percentage of children who received
breastmilk within one hour of delivery Percentage of children
who received colostrum
Total children who were breastfed
Area Programa Persentajen husi oan ne’ebé tau kedas
ba inan atu fo susu iha oras ida nia laran depois de moris
Persentajen husi oan ne’ebé simu susuben
kinur
Total oan ne’ebé simu
susuben
Alas 91% 97% 69 Fatuberliu 87% 94% 71
Same 86% 94% 66 Turiscai 73% 91% 71
Manufahi District Total
85% 94% 277
Ainaro 91% 91% 69 Hatu-Udo 94% 97% 69
Hatubuilico 80% 84% 69 Maubisse 93% 90% 72
Ainaro District Total
90% 90% 279
Combined District Totals
88% 92% 556

23
Table 30: Percentage of newborns who received another food prior to receiving breastmilk or during their first month after birth Tabela 30: Persentajen bebé foin moris ne’ebé hemu buat ruma antes de simu susuben inan nian ka
hemu buat seluk durante fulan primeru depois de moris
Program Area
Gave other foods prior to first breastfeeding
Provided substance other than breastmilk during first month
Yes No Yes No
Area Programa
Fo hahan ruma ba bebé antes de fo susuben inan nian
Fo hahan ruman durante fulan primeru depois de moris
Los La’e Los La’e
Alas 16% 84% 28% 72% Fatuberliu 23% 77% 17% 83%
Same 23% 77% 37% 63% Turiscai 39% 61% 14% 86%
Manufahi District 24% 76% 30% 70%
Ainaro 19% 81% 13% 87% Hatu Udo 26% 74% 12% 88%
Hatubuilico 41% 59% 26% 74% Maubisse 12% 88% 10% 90%
Ainaro District 22% 78% 14% 86%
Combined District Totals
23% 77% 22% 78%

24
Table 31: Percent of newborns given food before first breastmilk by type of drink/food given among newborns who were breastfed Tabela 31: Persentajen fo hahan ba bebe antes fo susuben primeiru liu husi tipu hemu/hemu ne’ebé fo ba bebe ne’ebé fo susu
Program Area
Plain Water
Sugar or Glucose Water
Porridge/ Gruel
Infant Formula
Other Breastmilk
(Family/ Neighbor)
Milk (Other than
breastmilk) Other
Number of Children Who Received Prelactal Feeds
Area Pgrama Bee
tasak
Masin midar ka bebé ho glukosa
Sasoro/ hahan mamar
Susubeen bebé nian
Inan nia susuben seluk
(Familia/Viziñu)
Susuben (Seluk husi
inan nia susuben)
Seluk Numero bebé ne’ebe simu
hahan antes sira simu susuben inan nian
Alas 50% 40% 0% 10% 0% 0% 0% 11
Fatuberliu 56% 19% 0% 13% 19% 0% 0% 16
Same 80% 0% 0% 13% 0% 0% 7% 15
Turiscai 57% 4% 0% 11% 39% 0% 4% 28
Manufahi District Total
70% 6% 0% 12% 10% 0% 5% 70
Ainaro 54% 31% 0% 77% 0% 0% 0% 13
Hatu Udo 33% 56% 0% 11% 0% 0% 6% 18
Hatubuilico 50% 39% 0% 0% 11% 0% 0% 28
Maubisse 67% 22% 0% 11% 0% 0% 0% 9
Ainaro District
Total 51% 37% 0% 10% 4% 0% 1% 68
Combined District Totals
61% 21% 0% 11% 7% 0% 3% 138

25
Table 32: Percent of infants under 6 months who were exclusively breastfed in the last 24 hours Tabela 32: Persentajen bebé fulan neen mai kraik ne’ebé fo inan nia susbeen iha oras 24 nia laran
Program Area Infants under 6 months who
received no other foods during the last 24 hours
Infants under 6 months who received other foods
Total infants under 6 months
Area Programa Bebé kiik liu fulan 6 ne’ebe
simu susuben deit durante oras 24 nia laran
Bebe kiik liu fulan 6 ne’ebé simu hahan seluk
Total bebé kiik liu fulan 6
Alas 65% 35% 26
Fatuberliu 57% 43% 21
Same 56% 44% 27
Turiscai 77% 23% 26
Manufahi District Total
59% 33% 100
Ainaro 76% 24% 21
Hatu Udo 68% 32% 22
Hatubuilico 70% 30% 23
Maubisse 83% 17% 24
Ainaro District Total
76% 24% 90
Combined District Totals
67% 33% 190
Table 33: Women who received a postpartum visit within two days of delivery Tabela 33: Inan sira ne’ebé simu visita postpartum iha loron rua nia laran husi partus
Program Area Postpartum Visit within
2 days Postpartum Visit after 2
days No Postpartum Visit
Area Programa Vizita postpartum iha
loron 2 nia laran Vizita postpartum depois
de loron 2
Alas 46% 23% 31% Fatuberliu 55% 14% 31%
Same 56% 14% 30% Turiscai 29% 31% 40%
Manufahi District Total
51% 17% 32%
Ainaro 18% 36% 46% Hatu Udo 45% 16% 39%
Hatubuilico 17% 7% 76%
Maubisse 26% 14% 60%
Ainaro District Total
25% 18% 56%
Combined District Totals
38% 18% 44%

26
Table 34: Health provider present at postpartum visit Tabela 34: Pesoál saúde sira marka prezensa vizita postpartum
Program Area Doctor Midwife Nurse Traditional
Birth Attendant
PSF
Women who
received postpartum
care
Area Programa
Doutór Parteira Enfermeiru Dayang PSF
Inan ne’ebé simu
kuidadu postpartum
Alas 68% 64% 18% 2% 0% 50 Fatuberliu 28% 80% 2% 0% 0% 50
Same 68% 58% 4% 0% 0% 50 Turiscai 37% 74% 12% 0% 0% 43
Manufahi District Total
60% 63% 6% 0% 0% 193
Ainaro 46% 62% 10% 0% 0% 39 Hatu Udo 43% 61% 9% 2% 0% 44
Hatubuilico 11% 79% 0% 0% 0% 18 Maubisse 76% 24% 17% 0% 0% 29
Ainaro District Total
51% 51% 11% 1% 0% 130
Combined District Totals
57% 58% 8% 0% 0% 323
Table 35: Percent of babies that received a postnatal visit from a trained health worker within two days of birth Tabela 35: Persentajen bebé ne’ebé simu vizita postnatal husi pesoál saúde treinadu iha loron rua nia laran husi moris
Area Newborn Check within 2
days Newborn Check after 2 days No Newborn check
Area Vizita postnatal
Iha loron 2 nia laran Vizita postnatald depois de
loron 2 Laiha vizita hodi haree
bebe foin moris
Alas 38% 43% 19% Fatuberliu 49% 38% 13%
Same 39% 34% 27% Turiscai 28% 43% 29%
Manufahi District Total
39% 37% 25%
Ainaro 25% 49% 26% Hatu Udo 42% 37% 21%
Hatubuilico 14% 24% 62% Maubisse 15% 61% 24%
Ainaro District Total
22% 46% 32%
Combined District Totals
31% 41% 28%

27
Table 36: Health provider present at postnatal visit Tabela 36: Pesoál saúde ne’ebé marka prezensa iha vizita postnatal
Program Area Doctor Midwife Nurse Traditional
Birth Attendant
PSF Children who
received postnatal care
Area Programa Doutór Parteira Enfermeira Dayang PSF Bebé simu kuidadu
postnatal
Alas 71% 48% 29% 3% 0% 58 Fatuberliu 25% 65% 17% 0% 0% 63
Same 53% 64% 9% 0% 2% 53 Turiscai 35% 73% 15% 0% 0% 51
Manufahi District Total
49% 63% 14% 0% 1% 225
Ainaro 45% 55% 13% 0% 0% 53 Hatu Udo 42% 46% 23% 0% 0% 57
Hatubuilico 17% 72% 21% 0% 0% 28 Maubisse 55% 20% 45% 0% 4% 55
Ainaro District Total
45% 41% 29% 0% 2% 193
Combined District Totals
47% 52% 21% 0% 1% 418

28
Table 37: Knowledge of danger signs during delivery, the postpartum period and in newborns Tabela 37: Inan sira ne’ebé hatene sinál perigu durante partus no iha ba bebé foin moris
Program Area Knows 2 or more signs
during pregnancy Knows 2 or more danger
signs during delivery Knows 2 or more danger
signs for women postpartum
Knows 2 or more danger
signs in newborns
Area Programa Hatene sinál perigu 2 ka
liu husi isin rua Hatene sinál perigu
durante partus 2 ka liu Hatene sinál perigu ba inan
depois de partus 2 ka liu Hatene sinál perigu bebé
foin moris 2 ka liu
Alas 50% 49% 47% 61%
Fatuberliu 32% 24% 29% 44%
Same 38% 24% 35% 39%
Turiscai 39% 29% 33% 29%
Manufahi District Total
39% 27% 35% 40%
Ainaro 43% 36% 43% 46%
Hatu Udo 39% 40% 44% 42%
Hatubuilico 24% 17% 24% 15%
Maubisse 29% 35% 26% 47%
Ainaro District Total
33% 32% 33% 39%
Combined District Totals
36% 30% 34% 40%

29
Tables of Results on Family Planning
Table 38: Reported ideal birth interval among women with children 0-23 months of age (Number of years women reported was best to space between children) Tabela 38: Relatoriu kona-ba espasu oan ideal husi inan ne’ebé ho oan idade fulan 0-23
Program Area One Year Two Years Three or More
Area programa
Tinan ida Tinan rua Tinan tolu ka liu
Alas 7% 41% 52%
Fatuberliu 9% 38% 53%
Same 7% 32% 61%
Turiscai 18% 42% 40%
Manufahi District Total
9% 35% 56%
Ainaro 7% 40% 53%
Hatu Udo 13% 43% 44%
Hatubuilico 32% 45% 23%
Maubisse 13% 53% 34%
Ainaro District Total
15% 47% 38%
Combined District Totals
12% 41% 47%

Table 39: Reported risks of getting pregnant too soon after the birth of a child* Tabela 39: Relata risku husi hetan isin rua fali iha tempu badak nia laran depois partus
Program Area
Baby born too
small
Baby born too
early
Mother can die
Mother can
miscarry
Mother can suffer
anemia
Bad for health of mother
and/or baby
Mother cannot work between
pregnancies Other
Area Programa
Bebé moris kiik
liu
Bebé moris
sedu liu
Inan bele mate
Inan bele abortus
Inan bele sofre
anemia
Ladiak ba inan ka bebé nia
saude
Laiha tempu atu halo servisu
Seluk
Alas 14% 1% 21% 8% 6% 44% 38% 11%
Fatuberliu 1% 0% 1% 7% 6% 38% 40% 24%
Same 11% 1% 3% 0% 0% 32% 31% 22%
Turiscai 6% 0% 15% 3% 4% 29% 46% 14%
Manufahi District Total
10% 1% 6% 2% 2% 33% 35% 20%
Ainaro 6% 1% 7% 3% 4% 42% 44% 6%
Hatu Udo 7% 0% 8% 1% 3% 51% 71% 15%
Hatubuilico 6% 0% 3% 4% 1% 13% 21% 21%
Maubisse 6% 1% 13% 4% 7% 40% 46% 10%
Ainaro District Total
6% 1% 8% 3% 4% 37% 45% 12%
Combined District Totals
8% 1% 7% 3% 3% 35% 40% 16%
* Women could report more than one answer. * Inan bele reporta liu tan husi resposta ida

31
Table 40: Average of actual number of months between deliveries of last two children Tabela 40: Mediu númeru fulan atual entre partus ba oan rua ikus
Program Area Average number of months between deliveries of last two children Women with
at least two children 12 months or less 12-24 months More than 24 months
Area Programa
Mediu númeru fulan atual entre partus ba oan rua ikus Inan ho pelumenuz
oan rua Fulan 12 ka menus Fulan 12 – 24 Liu fulan 24
Alas 0% 18% 82% 56
Fatuberliu 8% 18% 74% 50
Same 0% 26% 74% 49
Turiscai 2% 24% 74% 55
Manufahi District Total
1% 24% 75% 210
Ainaro 2% 29% 69% 55
HatuUdo 0% 23% 77% 48
Hatubuilico 9% 27% 64% 63
Maubisse 3% 45% 52% 58
Ainaro District Total
4% 34% 62% 224
Combined District Totals
3% 29% 68% 434
Table 41: Women who could spontaneously name a contraceptive method Tabela 41: Inan ne’ebé bele identifika naran metodu kontraseptivu balu ho lalais
Program Area Any Method Any modern
method No method known
Area Programa
Identifika metodu 1 ka liu
Identifika metodu modernu 1 ka liu
La hatene metodu ida
Alas 93% 93% 7%
Fatuberliu 81% 81% 19%
Same 69% 69% 31%
Turiscai 82% 82% 18%
Manufahi District Total
75% 75% 25%
Ainaro 71% 69% 29%
Hatu Udo 92% 90% 8%
Hatubuilico 69% 69% 31%
Maubisse 56% 54% 44%
Ainaro District Total
68% 67% 32%
Combined District Totals
72% 71% 28%

32
Table 42: Knowledge of contraceptive methods by women as determined by spontaneous recall * Tabela 42: Koñesimetu kona-ba metodu kontraseptivu husi inan sira ne’ebé sira identifika rasik
Program Area
Fem
ale
St
eri
lizat
ion
Mal
e
Ste
riliz
atio
n
Pill
IUD
Inje
ctab
les
Imp
lan
ts
Co
nd
om
LAM
Cyc
leb
ead
s
Rh
yth
m
Me
tho
d
Area programa
Este
riliz
asau
n
ba
Feto
Este
riliz
asau
n
ba
man
e
Pill
IUD
Son
a
Imp
lan
t
Ko
nd
om
LAM
Sura
loro
n
me
nst
ruas
aun
Sura
ai m
usa
n
Alas 14% 1% 61% 26% 90% 72% 6% 4% 26% 13%
Fatuberliu 3% 0% 68% 21% 79% 74% 6% 1% 8% 11%
Same 12% 2% 50% 26% 54% 56% 3% 0% 7% 3%
Turiscai 1% 0% 61% 21% 79% 61% 4% 1% 4% 1%
Manufahi District Total
10% 1% 55% 25% 65% 60% 4% 1% 9% 5%
Ainaro 7% 3% 39% 22% 61% 39% 10% 21% 6% 10%
Hatu Udo 3% 0% 63% 39% 85% 85% 9% 9% 18% 16%
Hatubuilico 4% 1% 35% 27% 63% 63% 1% 3% 10% 3%
Maubisse 3% 0% 35% 11% 47% 47% 0% 0% 8% 8%
Ainaro District Total
4% 1% 40% 22% 60% 38% 4% 7% 10% 9%
Combined District Totals
7% 1% 48% 23% 62% 49% 4% 4% 9% 7%
* Women could report more than one answer. *Inan bele reporta liu tan husi resposta ida.

33
Table 43: Percent of women who could identify a specific contraceptive method by spontaneous recall or when prompted Tabela 43: Persentajen inan ne’ebé bele identifika metodu konstraseptivu espesifiku liu husi hanoin lalaihs ka bainhira pronto
Program Area
Fem
ale
St
eri
lizat
ion
Mal
e St
eri
lizat
ion
Pill
IUD
Inje
ctab
les
Imp
lan
ts
Co
nd
om
LAM
Cyc
le b
ead
s
Rh
yth
m
Me
tho
d
Area programa
Este
riliz
asau
n
ba
Feto
Este
riliz
asau
n
ba
man
e
Pill
IUD
Son
a
Imp
lan
t
Ko
nd
om
LAM
Sura
loro
n
me
nst
ruas
aun
Sura
ai m
usa
n
Alas 76% 28% 85% 65% 100% 94% 80% 92% 76% 80%
Fatuberliu 40% 3% 85% 54% 92% 92% 69% 69% 51% 64%
Same 52% 10% 85% 56% 93% 93% 67% 69% 39% 53%
Turiscai 46% 15% 79% 49% 85% 72% 46% 47% 44% 57%
Manufahi District Total
53% 12% 84% 56% 93% 91% 66% 70% 46% 58%
Ainaro 53% 13% 74% 49% 82% 65% 38% 60% 29% 39%
Hatu Udo 42% 4% 86% 54% 96% 96% 59% 69% 51% 55%
Hatubuilico 39% 10% 62% 42% 86% 51% 35% 54% 31% 27%
Maubisse 69% 18% 63% 42% 81% 69% 53% 57% 58% 65%
Ainaro District Total
55% 13% 69% 46% 84% 69% 46% 59% 44% 49%
Combined District Totals
54% 12% 77% 51% 89% 80% 56% 64% 45% 54%

34
Table 44: Women who are currently using any family planning method, by whether it is a modern method Tabela 44: Inan ne’ebé ho oan idade fulan 0-23 mak agora dadaun uza metodu planeamentu familiar
modernu ka tradisionál
Program Area Modern Method Other Method Not Using
Contraception Total
Women
Area programa Usa metodu modernu Usa metodu seluk La usa metodu Inan Total
Alas 68% 3% 29% 72
Fatuberliu 54% 3% 43% 72
Same 57% 1% 42% 72
Turiscai 29% 0% 71% 72
Manufahi District Total
55% 1% 44% 288
Ainaro 31% 7% 62% 72
Hatu Udo 57% 6% 37% 72
Hatubuilico 30% 10% 60% 72
Maubisse 22% 4% 74% 72
Ainaro District Total
32% 6% 62% 288
Combined District Totals
43% 4% 53% 576

35
Table 45: Contraceptive method use by specific method * Tabela 45: Metodu kontraseptivu uza husi metodu espesifiku
Program Area
No
t U
sin
g C
on
trac
ep
tio
n
Fem
ale
St
eri
lizat
ion
Pill
IUD
Inje
ctab
le
Imp
lan
t
LAM
Cal
en
dar
M
eth
od
Oth
er
Tota
l W
om
en
wh
o
rep
ort
ed
usi
ng
a
con
trac
ep
tive
m
eth
od
Area Programa
La u
za
kon
tras
ep
sau
n
Este
reliz
asau
n
ba
feto
Pil
IUD
Son
a
Inp
lan
t
LAM
Me
tod
u
Kal
end
ariu
Selu
k
Inan
to
tal
Alas 29% 4% 6% 4% 64% 20% 0% 2% 0% 50
Fatuberliu 43% 0% 15% 2% 54% 24% 0% 2% 2% 41
Same 42% 2% 10% 0% 71% 14% 2% 0% 0% 42
Turiscai 71% 0% 5% 0% 91% 5% 0% 0% 0% 21
Manufahi District Total
44% 2% 9% 1% 69% 16% 2% 1% 0% 154
Ainaro 62% 0% 4% 0% 76% 8% 0% 12% 0% 25
Hatu Udo 37% 0% 9% 2% 66% 16% 2% 5% 0% 44
Hatubuilico 60% 3% 14% 0% 52% 7% 0% 0% 24% 29
Maubisse 74% 5% 11% 5% 58% 5% 0% 5% 11% 19
Ainaro District Total 62% 2% 9% 2% 62% 9% 3% 5% 8% 117
Combined District Totals
53% 2% 9% 1% 66% 13% 2% 3% 4% 271

Tables of Results on Mobile Phone Ownership and Use in Manufahi and Ainaro
Table 46: Women who reported mobile phone ownership in household Table 46: Inan sira ne’ebé iha telemovel rasik iha uma
Program Area Mobile phone in the
household at the time of pregnancy
Household currently owns mobile phone
Household does not currently have mobile
phone
Area Programa Iha telemovél iha uma durante isin rua ikus
Iha telemovél iha uma durante survey
Laiha telemovél
Alas 93% 97% 3% Fatuberliu 96% 96% 4%
Same 89% 97% 3%
Turiscai 83% 92% 8%
Manufahi District Total
90% 96% 4%
Ainaro 85% 86% 14% Hatu Udo 85% 99% 1%
Hatubuilico 46% 78% 22% Maubisse 72% 83% 17%
Ainaro District Total
72% 85% 15%
Combined District Totals
81% 91% 9%
Table 47: Number of mobile phones per household for women with any mobile phones in the home
Tabela 47: Número telemovél kada uma kain husi inan ne’ebe iha telemovel ida ka liu
Program Area No phone One Two Three or more
phones
Area Programa Telemovél
la iha Ida Rua
Telemovél tolu ka liu
Alas 3% 21% 44% 32%
Fatuberliu 4% 18% 29% 49%
Same 3% 23% 39% 35%
Turiscai 8% 39% 24% 29%
Manufahi District Total
4% 24% 37% 35%
Ainaro 14% 32% 33% 21%
Hatu Udo 2% 25% 33% 40% Hatubuilico 23% 27% 34% 16%
Maubisse 16% 35% 35% 14%
Ainaro District Total
15% 31% 34% 20%
Combined District Totals
9% 28% 35% 28%
Table 48: Percentage of women who report there is their “own” phone in the household

37
Tabela 48: Persentajem inan sira ne’ebé iha telemovél rasik
Program Area Own Phone Uses Family Phone Don’t Use Phone
Area Programa Telemovél rasik Uza telemovél
familia nian La uza telemovél
Alas 94% 3% 3%
Fatuberliu 93% 7% 0%
Same 84% 16% 0%
Turiscai 73% 24% 3%
Manufahi District Total
85% 14% 1%
Ainaro 97% 3% 0%
HatuUdo 86% 14% 0%
Hatubuilico 48% 43% 9%
Maubisse 90% 10% 0%
Ainaro District Total
83% 15% 2%
Combined District Totals
84% 15% 1%
Table 49: Percent of women who own “smart” or simple phones Tabela 49: Persentajen inan ne’ebé iha telemovél smart phone no telemovel simplés
Program Area Simple Smart Women who have a phone in the home
Area Programa Simplés Smart phone
Inan ne’ebé iha telemovél
iha uma
Alas 90% 10% 70
Fatuberliu 84% 16% 69
Same 80% 20% 70
Turiscai 95% 5% 66
Manufahi District
83% 17% 275
Ainaro 79% 21% 62
Hatu Udo 93% 7% 71
Hatubuilico 94% 6% 56
Maubisse 88% 12% 60
Ainaro District 88% 12% 249
Combined District Totals
85% 15% 524
Table 50: Type of mobile network operator used by women
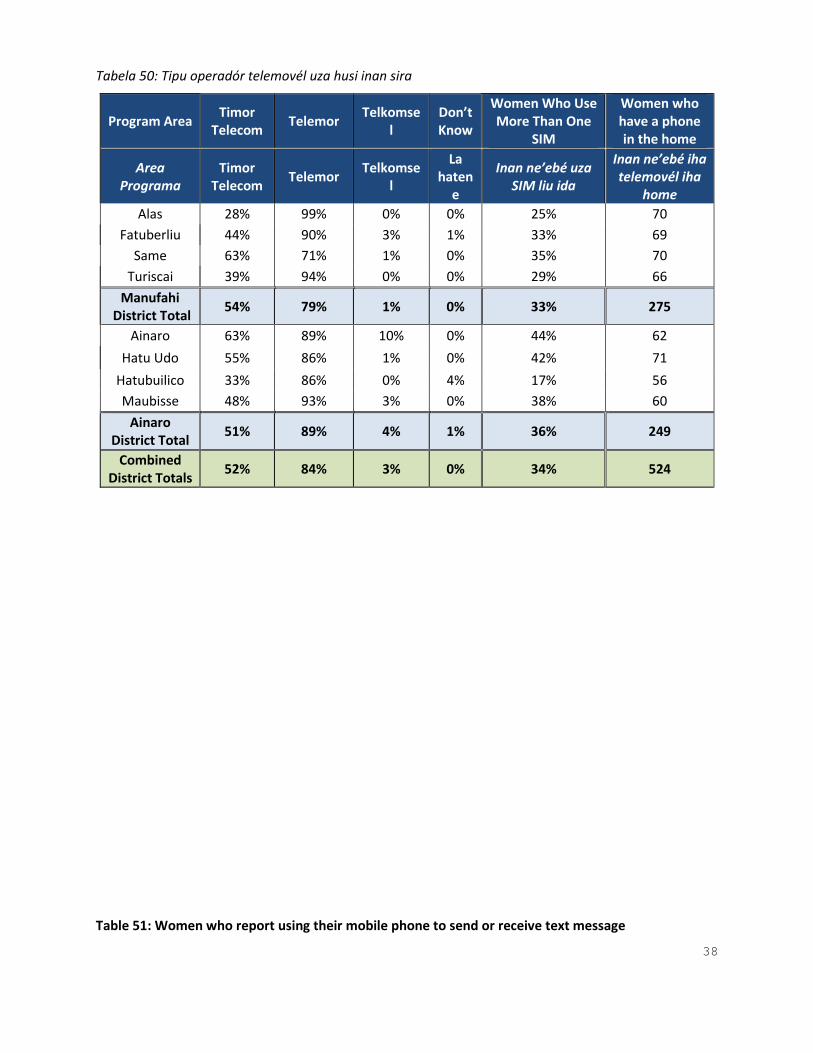
38
Tabela 50: Tipu operadór telemovél uza husi inan sira
Table 51: Women who report using their mobile phone to send or receive text message
Program Area Timor
Telecom Telemor
Telkomsel
Don’t Know
Women Who Use More Than One
SIM
Women who have a phone in the home
Area Programa
Timor Telecom
Telemor Telkomse
l
La haten
e
Inan ne’ebé uza SIM liu ida
Inan ne’ebé iha telemovél iha
home
Alas 28% 99% 0% 0% 25% 70
Fatuberliu 44% 90% 3% 1% 33% 69
Same 63% 71% 1% 0% 35% 70
Turiscai 39% 94% 0% 0% 29% 66
Manufahi District Total
54% 79% 1% 0% 33% 275
Ainaro 63% 89% 10% 0% 44% 62
Hatu Udo 55% 86% 1% 0% 42% 71
Hatubuilico 33% 86% 0% 4% 17% 56
Maubisse 48% 93% 3% 0% 38% 60
Ainaro District Total
51% 89% 4% 1% 36% 249
Combined District Totals
52% 84% 3% 0% 34% 524

39
Tabela 51: Inan ne’ebé iha relatoriu uza sira nia telemovél rasik hodi haruka no simu mensajen
Program Area Women who send or
receive SMS messages Women who do not send
or receive messages Women who have a phone in the home
Area Programa Inan ne’ebé simu ka
haruka mensajen Inan ne’ebé la simu ka
haruka mensajen Inan ne’ebé iha
telemovél iha uma
Alas 91% 9% 70 Fatuberliu 88% 12% 69
Same 88% 12% 70 Turiscai 81% 19% 66
Manufahi District Total
88% 12% 275
Ainaro 95% 5% 62 HatuUdo 88% 12% 71
Hatubuilico 55% 45% 56 Maubisse 59% 41% 60
Ainaro District Total
73% 27% 249
Combined District Totals
81% 19% 524
Table 52: Frequency of text message sending among women who own mobile phones Tabela 52: Entre inan sira ne’ebe haruka mensajen frequentamente husi sira nia telemovél rasik
Program Area Once a day
or more Once a week
Once a month
Never Women who have a phone in the home
Area Programa Loron ida
dala ida ka liu
Semana ida dala
ida
Fulan ida dala ida
Nunka Inan ne’ebé
iha telemovél ida iha uma
Alas 68% 9% 14% 9% 70
Fatuberliu 71% 13% 4% 12% 69
Same 67% 20% 2% 11% 70
Turiscai 39% 28% 14% 19% 66
Manufahi District Total
65% 19% 5% 12% 275
Ainaro 89% 3% 3% 5% 62
Hatu Udo 57% 17% 14% 12% 71
Hatubuilico 21% 10% 21% 48% 56
Maubisse 48% 5% 5% 42% 60
Ainaro District Total
56% 8% 9% 27% 249
Combined District Totals
61% 14% 6% 19% 524
Table 53: Reported distance to cell phone signal among women with children 0-23 months of age who have a cell phone in their household

40
Tabela 53: Relatoriu kona-ba distansia ba rede telemovél husi inan ho oan idade fulan 0-23 ne’ebé iha telemovél rasik iha uma
Program Area Have signal at home or within 5
minute walk More than a 5 minute walk
Area Programa Hetan rede iha uma ka lao 5
minutus Lao liu minutu 5
Alas 100% 0%
Fatuberliu 100% 0%
Same 100% 0%
Turiscai 99% 1%
Manufahi District Total
100% 0%
Ainaro 100% 0%
Hatu Udo 96% 4%
Hatubuilico 100% 0%
Maubisse 97% 3%
Ainaro District Total
98% 2%
Combined District Totals
99% 1%
Table 54: Percent women able to read the Tetun language Tabela 54: Persentajen inan ne’ebé bele lee Lian Tetun
Program Area Women that
can read Tetun
Women that can’t read
Tetun
Area Programa Inan ne’ebé
bele lee Tetun
Inan ne’ebé labele lee
Tetun
Alas 83% 17% Fatuberliu 94% 6%
Same 88% 13% Turiscai 76% 24%
Manufahi District Total
86% 14%
Ainaro 71% 21% Hatu Udo 82% 18%
Hatubuilico 53% 47% Maubisse 69% 31%
Ainaro District Total
71% 29%
Combined District Totals
79% 21%
Table 55: Available assistance in reading tetun messages by women who reported being unable to
read the Tetun language themselves*

41
Tabela 55: Iha ema ne’ebé ajuda lee mensajen iha Tetun ba inan sira tuir relatoriu labele atu lee iha lian Tetun
Program Area
Husband Child Other Family
Member Neighbor
Number of women who
could not read Tetun
Area Programa Laen/ Kaben
Oan Membru familia
seluk Vizinho
Númeru inan ne’ebé labele
lee Tetun
Alas 42% 33% 50% 25% 12
Fatuberliu 100% 0% 0% 0% 4
Same 44% 33% 22% 0% 9
Turiscai 65% 35% 35% 0% 17
Manufahi District Total
51% 32% 28% 4% 42
Ainaro 53% 13% 20% 27% 15
HatuUdo 62% 31% 15% 31% 13
Hatubuilico 29% 65% 18% 6% 34
Maubisse 45% 32% 27% 0% 22
Ainaro District Total
43% 39% 22% 10% 84
Combined District Totals
46% 37% 24% 8% 126
* Women could report more than one person * Inan bele hatoo liu ema ida

42
Table Results for Knowledge of and Participation in Liga Inan in Manufahi District
Table 56: Percent of women who recognized the name of the Liga Inan program Tabela 56: Persentajen inan ne’ebé hatene naran ba Programa Liga Inan
Program Area
Recognized the name of the Liga Inan program
Did not recogn ize the name of the Liga Inan
program
Area Programa
Alas 47% 53%
Fatuberliu 29% 71%
Same 27% 73%
Turiscai 25% 75%
Manufahi District
29% 71%
Table 57: Sources of knowledge where women heard about the Liga Inan program among women who reported hearing about the program
Tabela 57: Rekursu koñesimentu inan rona kona-ba programa Liga Inan iha inan balu ne’ebé hatoo rona kona-ba programa
Program Area
Fro
m a
He
alth
C
are
Wo
rker
In L
isio
On
a P
ost
er/
B
ann
er/
B
illb
oar
d
Ce
ll P
ho
ne
M
ess
age
Rad
io
Me
ssag
e
In a
Film
or
Vid
eo
Co
mm
un
ity
Hea
lth
W
ork
er (
PSF
)
Co
mm
un
ity
Me
eti
ng
SISC
a P
ost
Oth
er
Wo
me
n w
ho
he
ard
ab
ou
t
Liga
Inan
Area Programa
Hu
si p
eso
ál
saú
de
Iha
Lisi
o
Iha
po
ste
r/b
ann
er/
bill
bo
ard
M
en
saje
n
tele
fon
e
Me
nsa
jen
R
adio
Iha
film
e k
a
vid
eo
Serv
isu
Saú
de
Ko
mu
nid
ade
(PSF
)
Enko
ntr
u
Ko
mu
nid
ade
Po
stu
SIS
Ca
Selu
k
Inan
ne’
eb
é
ron
a ko
na-
ba
Liga
Inan
Alas 78% 7% 4% 11% 6% 6% 3% 10% 15%
6% 29
Fatuberliu 70% 0% 3% 4% 1% 0% 0% 7% 7% 6% 19
Same 68% 0% 4% 3% 3% 0% 1% 4% 3% 7% 19
Turiscai 63% 3% 3% 0% 1% 0% 0% 4% 0% 1% 18
Manufahi District Total
69% 1% 4% 4% 3% 1% 1% 5% 5% 6% 85
Table 58: Where women report hearing about the Liga Inan Program
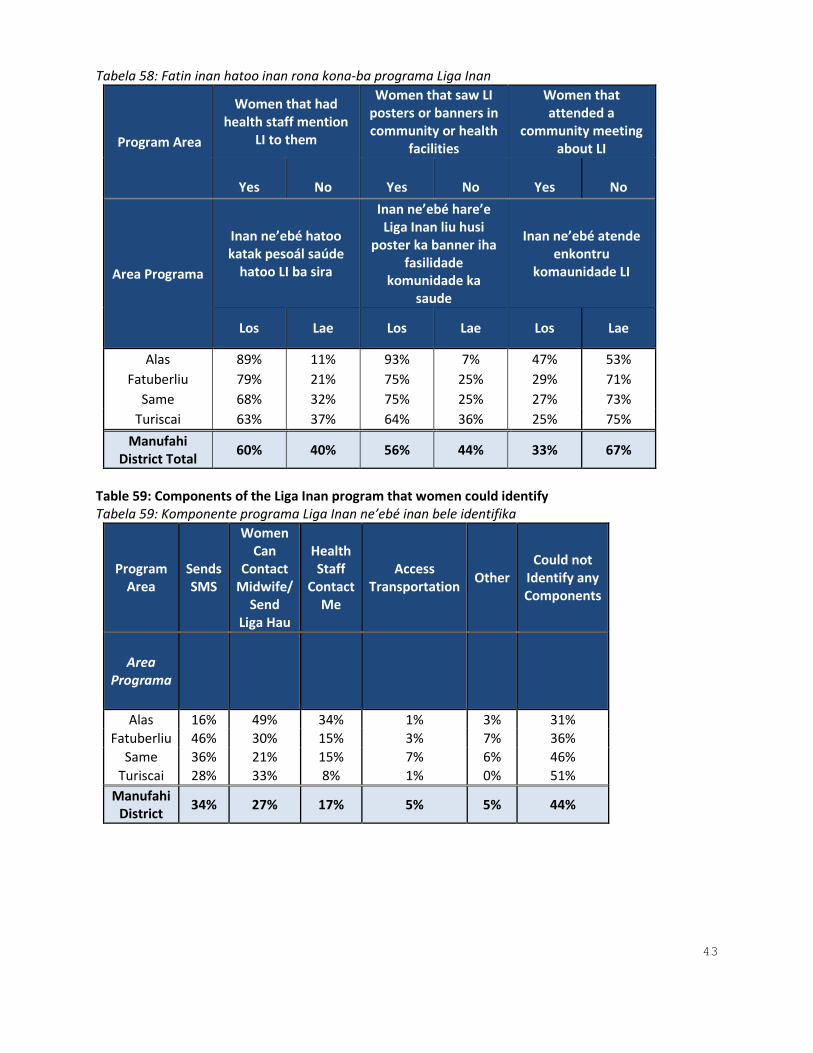
43
Tabela 58: Fatin inan hatoo inan rona kona-ba programa Liga Inan
Program Area
Women that had health staff mention
LI to them
Women that saw LI posters or banners in community or health
facilities
Women that attended a
community meeting about LI
Yes
No
Yes
No
Yes
No
Area Programa
Inan ne’ebé hatoo katak pesoál saúde
hatoo LI ba sira
Inan ne’ebé hare’e Liga Inan liu husi
poster ka banner iha fasilidade
komunidade ka saude
Inan ne’ebé atende enkontru
komaunidade LI
Los Lae Los Lae Los Lae
Alas 89% 11% 93% 7% 47% 53%
Fatuberliu 79% 21% 75% 25% 29% 71%
Same 68% 32% 75% 25% 27% 73%
Turiscai 63% 37% 64% 36% 25% 75%
Manufahi District Total
60% 40% 56% 44% 33% 67%
Table 59: Components of the Liga Inan program that women could identify Tabela 59: Komponente programa Liga Inan ne’ebé inan bele identifika
Program Area
Sends SMS
Women Can
Contact Midwife/
Send Liga Hau
Health Staff
Contact Me
Access Transportation
Other Could not
Identify any Components
Area Programa
Alas 16% 49% 34% 1% 3% 31%
Fatuberliu 46% 30% 15% 3% 7% 36%
Same 36% 21% 15% 7% 6% 46%
Turiscai 28% 33% 8% 1% 0% 51%
Manufahi District
34% 27% 17% 5% 5% 44%

44
Table 60a: Percent of all women who had participated in Liga Inan Tabela 60a: Persentajen ba inan hothotu ne’ebé partisipa ona Liga Inan
Program Area
Participated in Liga Inan
Did Not Participate in Liga Inan
Total Women
Area Programa
Partisipa iha Liga Inan
La partisipa iha Liga Inan
Total Inan
Alas 68% 32% 72
Fatuberliu 79% 21% 72
Same 71% 29% 72
Turiscai 60% 40% 72
Manufahi District
70% 30% 288
Table 60b: Percent of women that had both a cell phone and at least one ANC visit with a skilled provider during their pregnancy and were enrolled in Liga Inan Table 60b: Persentajen inan ne’ebé iha telefone no pelumenuz iha vizita ANC ho pesoál saúde durante sira nia isin rua no rejistu ba programa Liga Inan
Program Area
Participated in Liga Inan
Did Not Participate in Liga Inan
Total Eligible Women
Area Programa
Partisipa iha Liga Inan
La partisipa iha Liga Inan
Total inan ne’ebé
kualifikadu
Alas 71% 29% 66
Fatuberliu 81% 19% 69
Same 78% 22% 59
Turiscai 70% 30% 53
Manufahi District
77% 23% 247
Table 61: Length of participation in Liga Inan before delivery (Average weeks of confirmed participation per subdistrict) Tabela 61: Durasaun partisipasaun Liga Inan antes partus (mediu semana konfirmadu partisipasaun kada postu administrativu)
Program Area
Average weeks of participation before delivery
Women whose participation was confirmed
Area Programa
Mediu semana partisipasaun antes partus
Inan ne’ebé konfirma nia partisipasaun
Alas 14 35 Fatuberliu 18 51
Same 17 36 Turiscai 18 27
Manufahi District
17 149
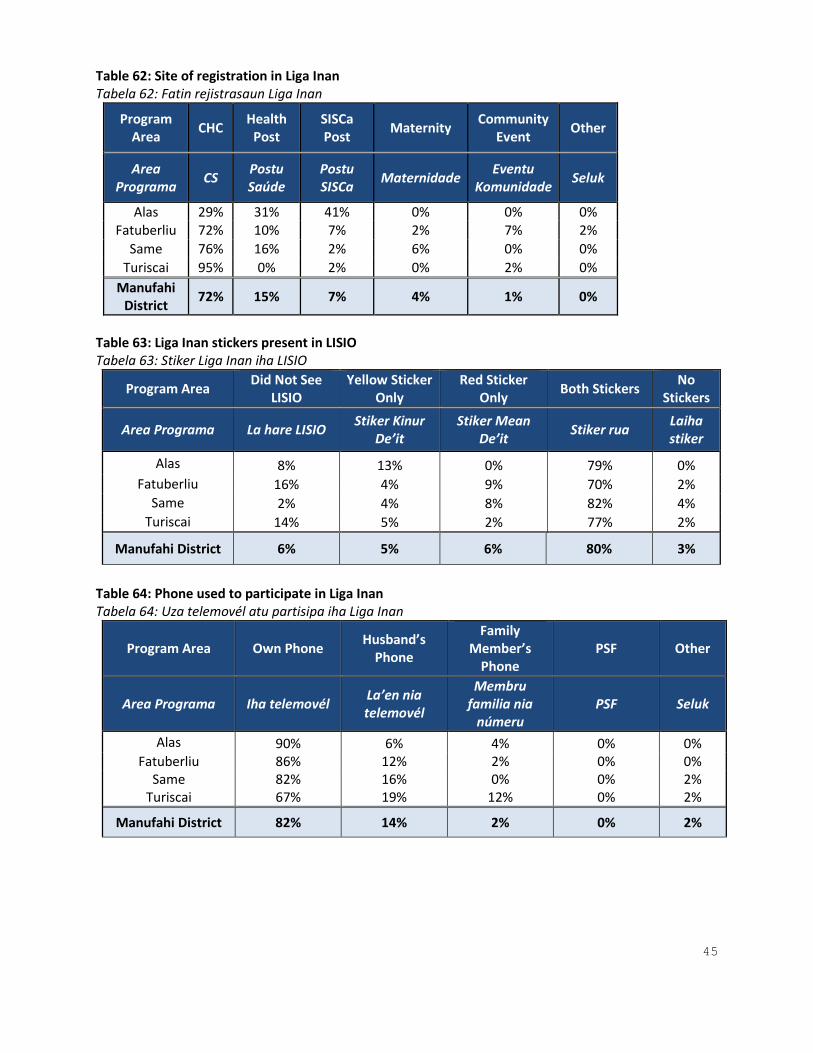
45
Table 62: Site of registration in Liga Inan Tabela 62: Fatin rejistrasaun Liga Inan
Program Area
CHC Health
Post SISCa Post
Maternity Community
Event Other
Area Programa
CS Postu Saúde
Postu SISCa
Maternidade Eventu
Komunidade Seluk
Alas 29% 31% 41% 0% 0% 0% Fatuberliu 72% 10% 7% 2% 7% 2%
Same 76% 16% 2% 6% 0% 0%
Turiscai 95% 0% 2% 0% 2% 0%
Manufahi District
72% 15% 7% 4% 1% 0%
Table 63: Liga Inan stickers present in LISIO Tabela 63: Stiker Liga Inan iha LISIO
Program Area Did Not See
LISIO Yellow Sticker
Only Red Sticker
Only Both Stickers
No Stickers
Area Programa La hare LISIO Stiker Kinur
De’it Stiker Mean
De’it Stiker rua
Laiha stiker
Alas 8% 13% 0% 79% 0%
Fatuberliu 16% 4% 9% 70% 2% Same 2% 4% 8% 82% 4%
Turiscai 14% 5% 2% 77% 2%
Manufahi District 6% 5% 6% 80% 3%
Table 64: Phone used to participate in Liga Inan Tabela 64: Uza telemovél atu partisipa iha Liga Inan
Program Area Own Phone Husband’s
Phone
Family Member’s
Phone PSF Other
Area Programa Iha telemovél La’en nia telemovél
Membru familia nia
númeru PSF Seluk
Alas 90% 6% 4% 0% 0% Fatuberliu 86% 12% 2% 0% 0%
Same 82% 16% 0% 0% 2% Turiscai 67% 19% 12% 0% 2%
Manufahi District 82% 14% 2% 0% 2%

46
Table 65a: Frequency of SMS message delivery (if received on own phone) Tabela 65a: Simu mensajen SMS dala hira ( sekarik simu iha sira nia telemovél rasik ka membru familia nia telemovél
Table 65b: Frequency of SMS message delivery (if received on a family member’s phone) Table 65b:
Table 66: Liga Inan message comprehension (Were the messages sent to women easy to understand?) Tabela 66: Komprensaun ba mensajen Liga Inan (mensajen hirak ne’ebé haruka ba inan sira fasil atu komprende ka la’e?)
Program Area
Twice a Week
Once a Week
Sometimes
Area Programa
Semana dala rua
Semana ida dala rua
Dalaruma
Alas 56% 36% 8% Fatuberliu 60% 38% 2%
Same 55% 37% 8% Turiscai 58% 38% 4%
Manufahi District
56% 37% 7%
Program Area
Twice a Week
Once a Week
Sometimes
Area Programa
Semana dala rua
Semana ida dala rua
Dalaruma
Alas 81% 13% 6% Fatuberliu 78% 0% 22%
Same 38% 62% 0% Turiscai 67% 27% 6%
Manufahi District
56% 40% 4%
Program Area Yes Somewhat or
Not Quite No
Area Programa Los Dalaruma ka
Ladun komprende
La’e
Alas 100% 0% 0% Fatuberliu 98% 0% 2%
Same 98% 2% 0% Turiscai 90% 8% 2%
Manufahi District
97% 2% 1%
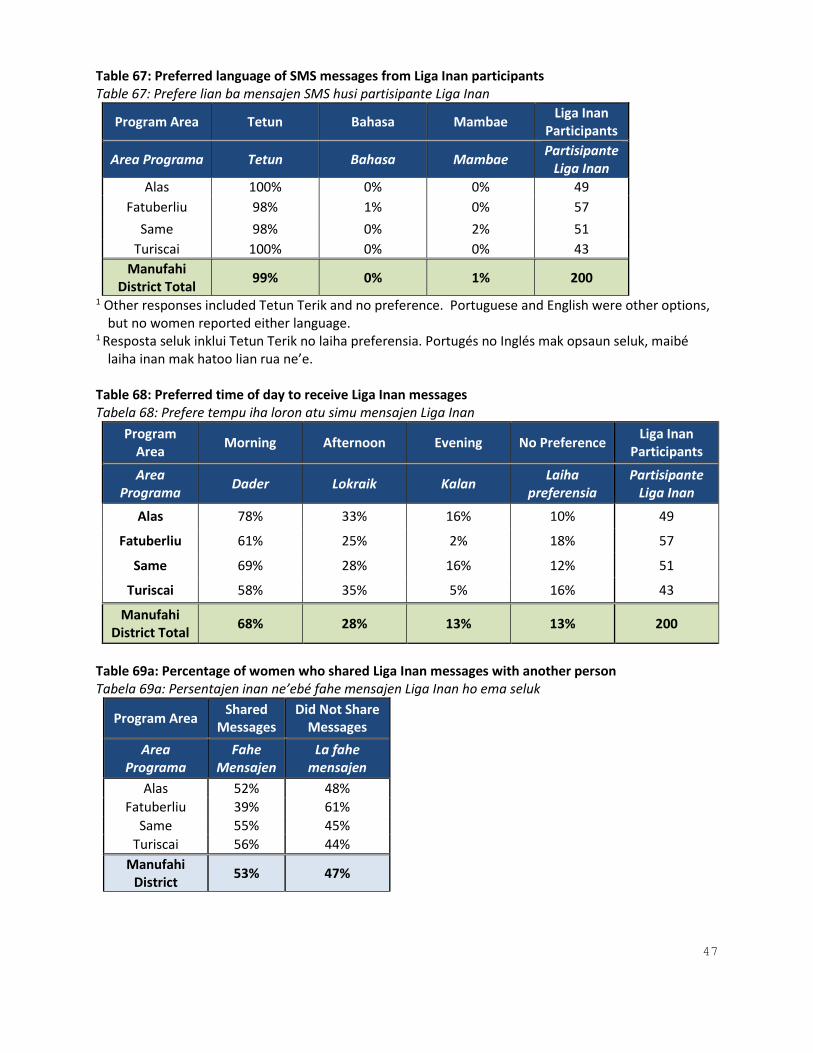
47
Table 67: Preferred language of SMS messages from Liga Inan participants Table 67: Prefere lian ba mensajen SMS husi partisipante Liga Inan
Program Area Tetun Bahasa Mambae Liga Inan
Participants
Area Programa Tetun Bahasa Mambae Partisipante
Liga Inan
Alas 100% 0% 0% 49
Fatuberliu 98% 1% 0% 57
Same 98% 0% 2% 51
Turiscai 100% 0% 0% 43
Manufahi District Total
99% 0% 1% 200
1 Other responses included Tetun Terik and no preference. Portuguese and English were other options, but no women reported either language.
1 Resposta seluk inklui Tetun Terik no laiha preferensia. Portugés no Inglés mak opsaun seluk, maibé laiha inan mak hatoo lian rua ne’e.
Table 68: Preferred time of day to receive Liga Inan messages Tabela 68: Prefere tempu iha loron atu simu mensajen Liga Inan
Program Area
Morning Afternoon Evening No Preference Liga Inan
Participants
Area Programa
Dader Lokraik Kalan Laiha
preferensia Partisipante
Liga Inan
Alas 78% 33% 16% 10% 49
Fatuberliu 61% 25% 2% 18% 57
Same 69% 28% 16% 12% 51
Turiscai 58% 35% 5% 16% 43
Manufahi District Total
68% 28% 13% 13% 200
Table 69a: Percentage of women who shared Liga Inan messages with another person Tabela 69a: Persentajen inan ne’ebé fahe mensajen Liga Inan ho ema seluk
Program Area Shared
Messages Did Not Share
Messages
Area Programa
Fahe Mensajen
La fahe mensajen
Alas 52% 48%
Fatuberliu 39% 61%
Same 55% 45%
Turiscai 56% 44%
Manufahi District
53% 47%

48
Table 69b: Percentage of women who shared Liga Inan messages by the person they shared them with Tabela 69b: Persentajen inan ne’ebé fahe mensajen Liga Inan husi ema ne’ebé sira fahe ba
Program Area
Health Staff
Husband Sibling In-Law PSF Friend or Neighbor
Other
Area Programa
Pesoál saúde
La’en Membr
u familia
Banin PSF Kolega ka
viziñu Seluk
Alas 7% 52% 56% 0% 0% 22% 4%
Fatuberliu 9% 57% 13% 9% 0% 48% 0%
Same 7% 20% 22% 4% 0% 36% 11%
Turiscai 6% 28% 32% 11% 0% 11% 0%
Manufahi District
7% 26% 26% 5% 0% 32% 8%
Table 70a: Percentage of Liga Inan participants who believe it would be helpful to have another person also receive Liga Inan messages Table 70a: Persentajen partisipante Liga Inan ne’ebé fiar katak ida ne’e ajuda duni atu iha ema seluk mos simu mensajen Liga Inan
Program Area
Women who would like another person to also participate in Liga Inan
with them
Women who do not think another person
should participate in Liga Inan with them
Area Programa Inan ne’ebé hakarak ema seluk mos partisipa Liga
Inan ho sira
Inan ne’ebé hanoin ema seluk mos la partisipa
Liga Inan ho sira
Alas 98% 2%
Fatuberliu 96% 4%
Same 88% 12%
Turiscai 74% 26%
Manufahi District
89% 11%

49
Table 70b: Percentage of Liga Inan participants who identified people they would want to receive Liga Inan messages Tabela 70b: Persentajen partisipante Liga inan ne’ebé identifika ema ne’ebé sira
Program Area
Pregnant Women
Only Husband Sibling
In-Law
PSF Neighbor Other
Do Not Know or
No Response
Area Programa
Inan isin rua de’it
La’en Feton naan
Banin PSF Viziñu Seluk Lahatene ka laiha resposta
Alas 30% 58% 40% 2% 0% 2% 6% 8%
Fatuberliu 36% 63% 11% 2% 0% 2% 2% 7%
Same 19% 42% 27% 3% 0% 2% 6% 5%
Turiscai 20% 41% 27% 4% 0% 0% 0% 0%
Manufahi District
22% 46% 27% 3% 0% 1% 5% 5%
Table 71: Percentage of Liga Inan participants who attempted to contact health staff during pregnancy or delivery (by method) Tabela 71: Persentajen partisipante ne’ebe tenta atu kontaktu pesoál saúde durante isin rua ka partus ( liu husi metodu)
Program Area
Liga Hau
Miss Call Call Directly Other Phone
PSF Other Did Not Contact
Area Programa
Liga Hau
Telefone perdida
Telefone diretamentu
Telefone seluk
PSF Seluk La
kontaku
Alas 47% 0% 56% 2% 2% 0% 16%
Fatuberliu 36% 5% 55% 0% 0% 2% 28%
Same 24% 4% 44% 0% 0% 0% 25%
Turiscai 9% 7% 36% 0% 0% 0% 51%
Manufahi District
26% 4% 45% 0% 0% 0% 30%
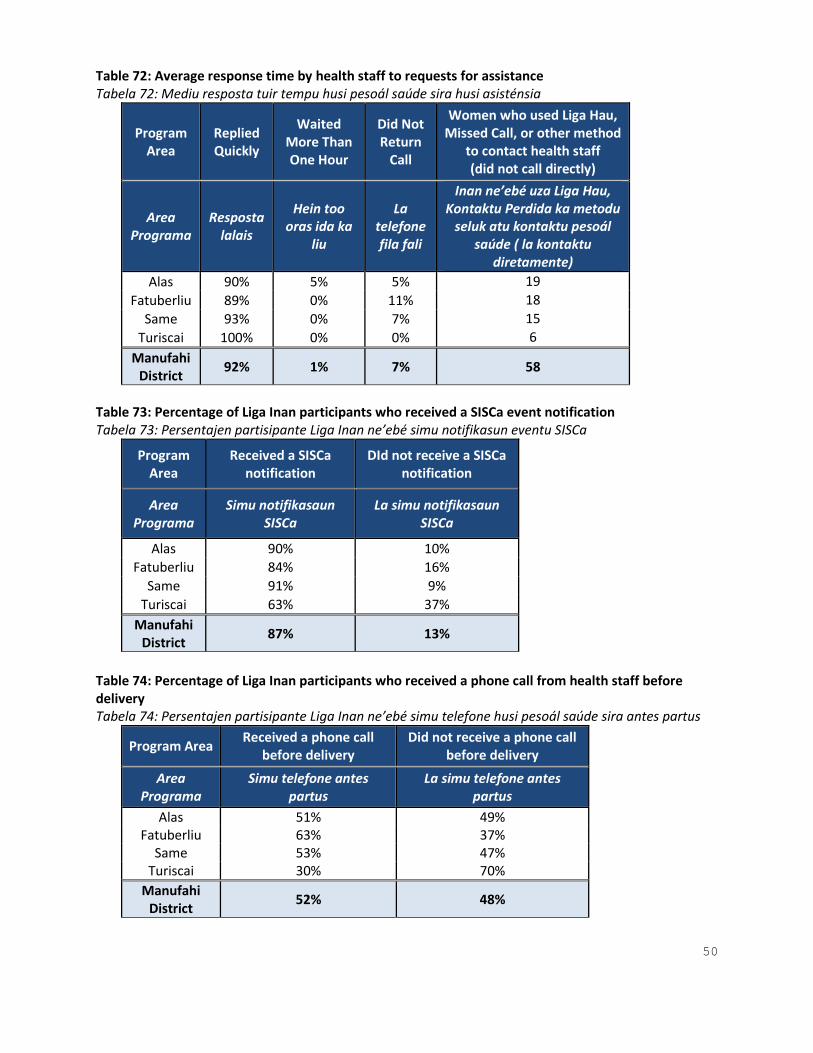
50
Table 72: Average response time by health staff to requests for assistance Tabela 72: Mediu resposta tuir tempu husi pesoál saúde sira husi asisténsia
Program Area
Replied Quickly
Waited More Than One Hour
Did Not Return
Call
Women who used Liga Hau, Missed Call, or other method
to contact health staff (did not call directly)
Area Programa
Resposta lalais
Hein too oras ida ka
liu
La telefone fila fali
Inan ne’ebé uza Liga Hau, Kontaktu Perdida ka metodu
seluk atu kontaktu pesoál saúde ( la kontaktu
diretamente)
Alas 90% 5% 5% 19
Fatuberliu 89% 0% 11% 18
Same 93% 0% 7% 15
Turiscai 100% 0% 0% 6
Manufahi District
92% 1% 7% 58
Table 73: Percentage of Liga Inan participants who received a SISCa event notification Tabela 73: Persentajen partisipante Liga Inan ne’ebé simu notifikasun eventu SISCa
Program Area
Received a SISCa notification
DId not receive a SISCa notification
Area Programa
Simu notifikasaun SISCa
La simu notifikasaun SISCa
Alas 90% 10%
Fatuberliu 84% 16%
Same 91% 9%
Turiscai 63% 37%
Manufahi District
87% 13%
Table 74: Percentage of Liga Inan participants who received a phone call from health staff before delivery Tabela 74: Persentajen partisipante Liga Inan ne’ebé simu telefone husi pesoál saúde sira antes partus
Program Area Received a phone call
before delivery Did not receive a phone call
before delivery
Area Programa
Simu telefone antes partus
La simu telefone antes partus
Alas 51% 49% Fatuberliu 63% 37%
Same 53% 47% Turiscai 30% 70%
Manufahi District
52% 48%

51
Table 75: Percentage of Liga Inan participants who had a “bebe” delivery confirmation Tabela 75: Persentajen partisipante Liga Inan hetan partus “bebe”
Program Area
Health staff confirmed birth
Health staff did not confirm birth
Women who participated in
Liga Inan*
Area Programa
Pesoál saúde sira konfirma partus
Pesoál saúde sira la konfirma partus
Inan ne’ebé partisipa konfirma
Alas 68% 32% 34
Fatuberliu 70% 30% 50
Same 81% 19% 36
Turiscai 56% 44% 27
Manufahi District
75% 25% 147
*Missing data equals 53 women
Table 76: Percentage of Liga Inan participants who have changed their phone number since participation (reported) Tabela 76: Persentajen partisipante Liga Inan ne’ebé troka sira nia númeru telemovél desde partipasau tuir relatoriu)
Program Area
Changed phone number
Did Not Change phone number
Area Programa
Troka númeru telemovel
La troka sira númeru
telemovél
Alas 35% 65%
Fatuberliu 50% 50%
Same 42% 58%
Turiscai 28% 72%
Manufahi District
41% 59%

52
Table Results for Liga Inan Message Preferences in Ainaro District
Table 77: Preferred language of SMS messages among women in Ainaro Tabela 77: Prefere lian mensajen SMS entre inan sira iha Ainaro
Program Area
Tetun Bahasa Portuguese Mambae English Other
Area Programa
Tetun Bahasa Portugés Mambae Inglés Seluk
Ainaro 99% 6% 4% 1% 1% 0%
Hatu-Udo 100% 3% 1% 3% 0% 0%
Hatubuilico 94% 0% 0% 13% 0% 1%
Maubisse 99% 1% 3% 0% 0% 3%
Ainaro District Total
98% 2% 2% 3% 0%
1%
Table 78: Preferred time of day to receive Liga Inan messages among women in Ainaro Tabela 83 prefere tempu atu simu mensajen Liga Inan inan sira iha Ainaro
Program Area Morning Afternoon Evening No Preference
Area Programa
Dader Lokraik Kalan Laiha
preferensia
Ainaro 81% 10% 7% 4%
Hatu-Udo 38% 21% 4% 40%
Hatubuilico 22% 21% 8% 56%
Maubisse 51% 19% 7% 22%
Ainaro District Total
50% 18% 7% 28%







