1
Management of Common Management of Common Inpatient Infections:Inpatient Infections:
MRSA, C diff, VRE, and more…MRSA, C diff, VRE, and more…
Bradley A. Sharpe, M.D.Associate Professor Medicine
Department of MedicineUCSF
Common Inpatient Infections
RoadmapRoadmap
• Background
• MRSA
• Clostridium difficile
• VRE
• More…
Common Inpatient Infections
Specific Goals:Specific Goals:
• Appreciate the morbidity and mortality associated with hospital-acquired infections (HAIs).
• Describe optimal therapy for MRSA infections.
• List key principles in the management of Clostridium difficile infection.
• Understand evidence for preventing HAIs.
CaveatsCaveats
• Will discuss hospital-acquired infections + community-acquired
• Cannot cover all in-depth
• Often complex patients (ID consult?)
• Highlight key principles, what you need to know
Common Inpatient Infections
2
RoadmapRoadmap
• Background
• MRSA
• Clostridium difficile
• VRE
• More…
Common Inpatient Infections
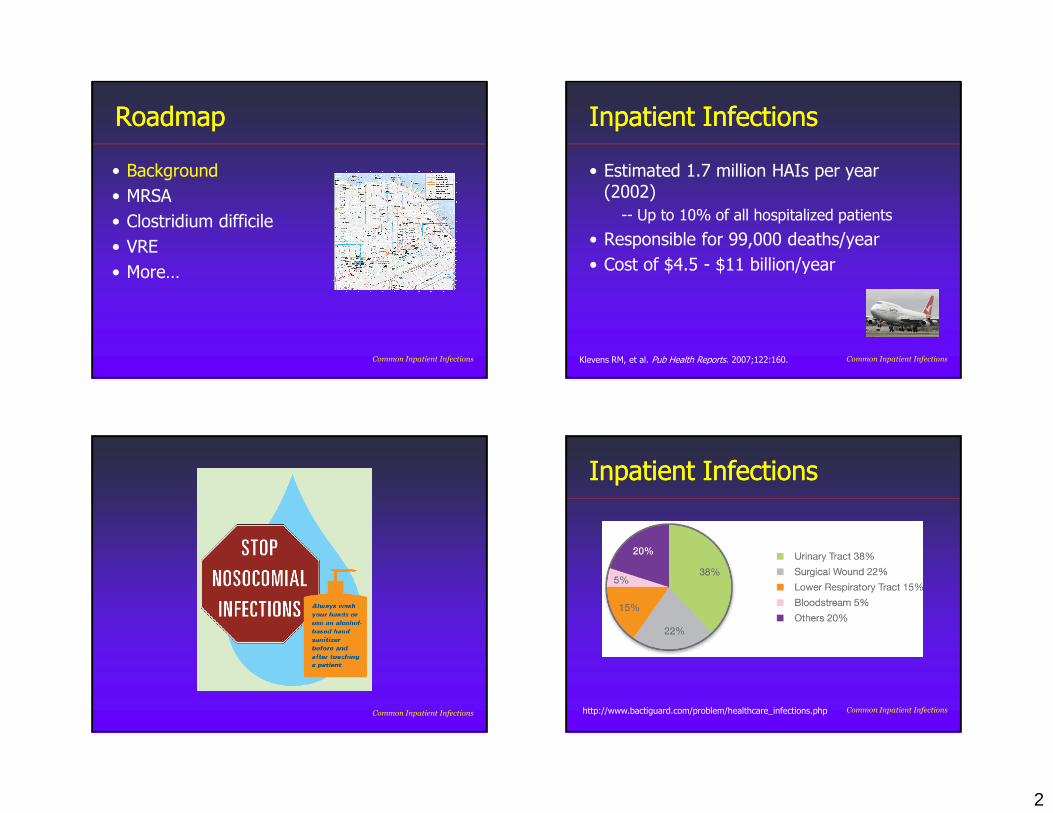
Inpatient InfectionsInpatient Infections
• Estimated 1.7 million HAIs per year (2002)
-- Up to 10% of all hospitalized patients
• Responsible for 99,000 deaths/year
• Cost of $4.5 - $11 billion/year
Klevens RM, et al. Pub Health Reports. 2007;122:160. Common Inpatient Infections
Common Inpatient Infections
Inpatient InfectionsInpatient Infections
http://www.bactiguard.com/problem/healthcare_infections.php Common Inpatient Infections
3
RoadmapRoadmap
• Background
• MRSA
• Clostridium difficile
• VRE
• More…
Common Inpatient Infections
MRSA EpidemiologyMRSA Epidemiology
• Facultative gram-positive
• Colonizer in humans (mainly nares)-- 20% persistent, 30% intermittent
• Transmitted in the hospital (your hands)
Ammerlaan HS, et al. CID. 2009;49:922. Solberg, CO. Scand J Infect Dis. 2000;32:587.
Common Inpatient Infections
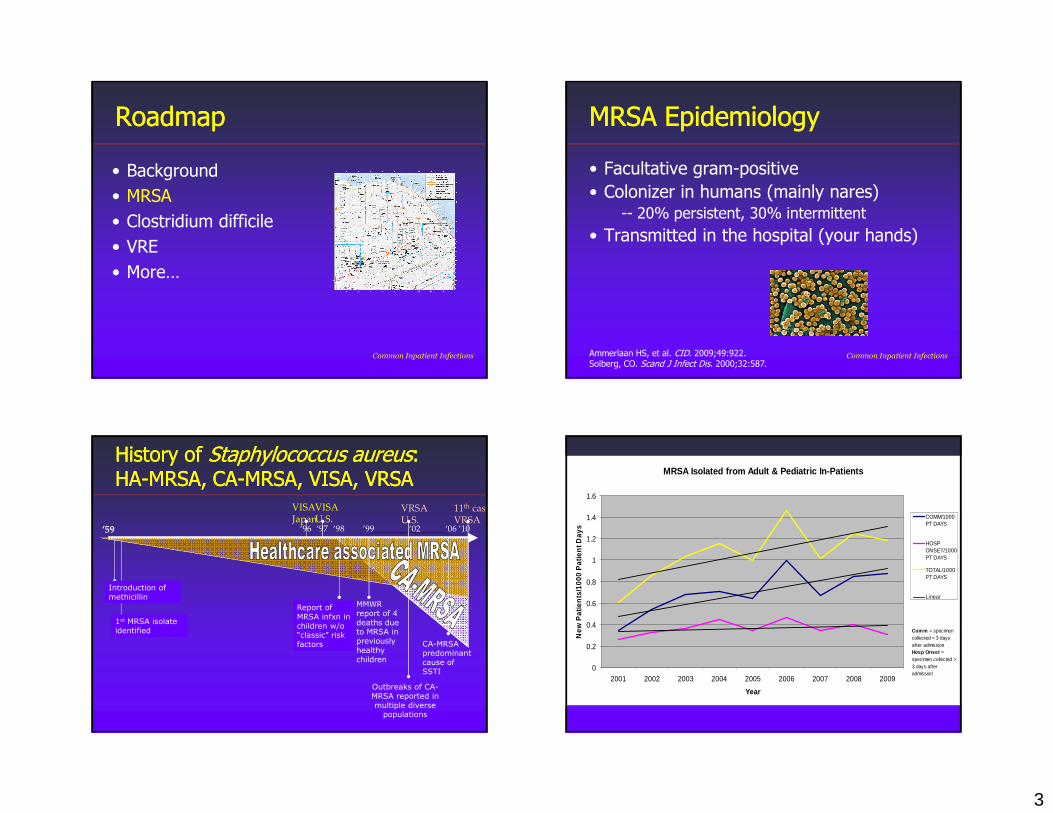
History of History of Staphylococcus Staphylococcus aureusaureus: : HAHA--MRSA, CAMRSA, CA--MRSA, VISA, VRSAMRSA, VISA, VRSA
‘59
Introduction of
methicillin
1st MRSA isolate
identified
‘98
Report of
MRSA infxn in
children w/o “classic” risk
factors
’99
MMWR
report of 4
deaths due to MRSA in
previously
healthy
children
‘06
CA-MRSA
predominant
cause of SSTI
‘97
VISAJapan
‘96
VISAU.S.
‘02
VRSAU.S.
‘10
11th case VRSA
Outbreaks of CA-
MRSA reported in
multiple diverse populations
MRSA Isolated from Adult & Pediatric In-Patients
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
2001 2002 2003 2004 2005 2006 2007 2008 2009
Year
New
Pat
ien
ts/1
000
Pat
ien
t Day
s
COMM/1000PT DAYS
HOSPONSET/1000PT DAYS
TOTAL/1000PT DAYS
Linear
Comm = specimen collected < 3 days after admissionHosp Onset = specimen collected > 3 days after admission
Moffitt-Long/ Mt.Zion
4
MRSA InfectionsMRSA Infections
• Skin and soft-tissue infections (SSTIs)
• Pneumonia (CAP, HCAP, HAP, VAP)
• Bacteremia/endocarditis
• Bone and joint infections
• Other (epidural abscess, etc.)
Common Inpatient Infections
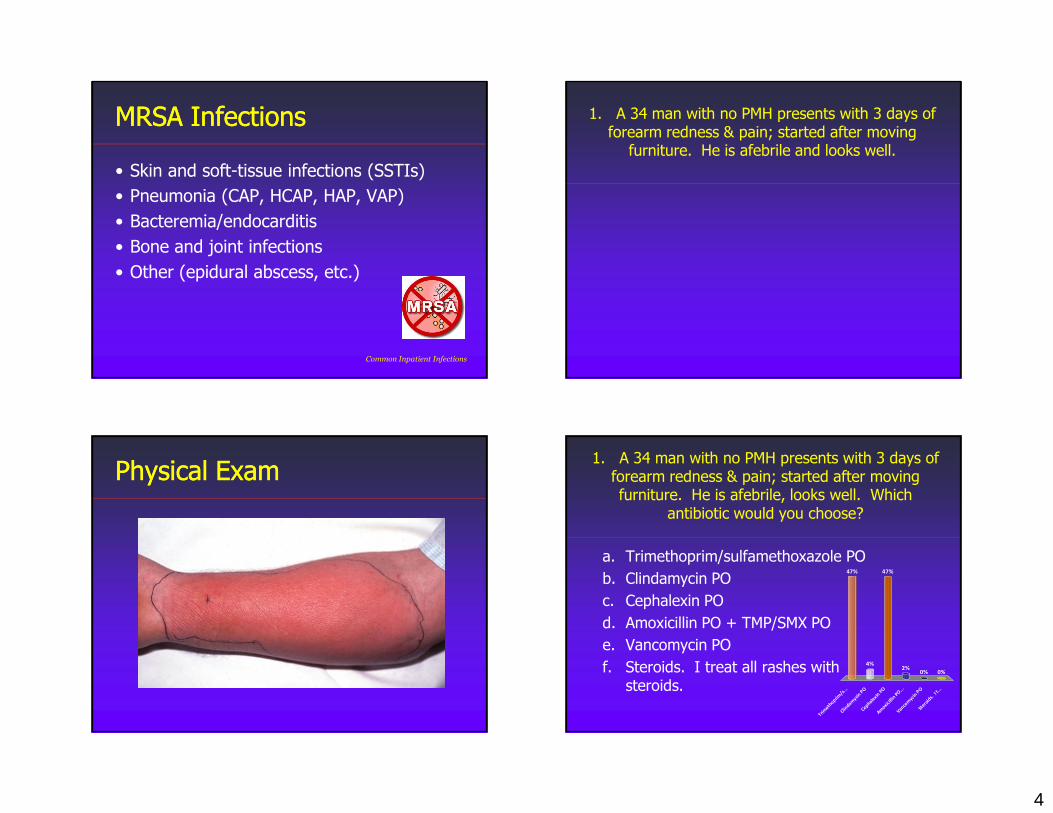
1. A 34 man with no PMH presents with 3 days of forearm redness & pain; started after moving furniture. He is afebrile and looks well.
Physical ExamPhysical Exam1. A 34 man with no PMH presents with 3 days of forearm redness & pain; started after moving furniture. He is afebrile, looks well. Which
antibiotic would you choose?
Trim
ethoprim
/s...
Clin
damycin
PO
Cephale
xin P
O A
moxi
cilli
n PO
... V
ancom
ycin
PO
Ste
roid
s. I
t...
47%
4%
0%0%2%
47%
a. Trimethoprim/sulfamethoxazole PO
b. Clindamycin PO
c. Cephalexin PO
d. Amoxicillin PO + TMP/SMX PO
e. Vancomycin PO
f. Steroids. I treat all rashes with steroids.
5
Skin & SoftSkin & Soft--tissue Infectionstissue Infections
• Most common Staphyloccocus Aureus and streptococcal species (GAS)
• Depends on purulent vs. non-purulent infection
Common Inpatient Infections
Purulent SSTIsPurulent SSTIs
• Furuncle
• Carbuncle
• Abscess
• Cellulitis with purulence
Common Inpatient Infections
Common Inpatient Infections
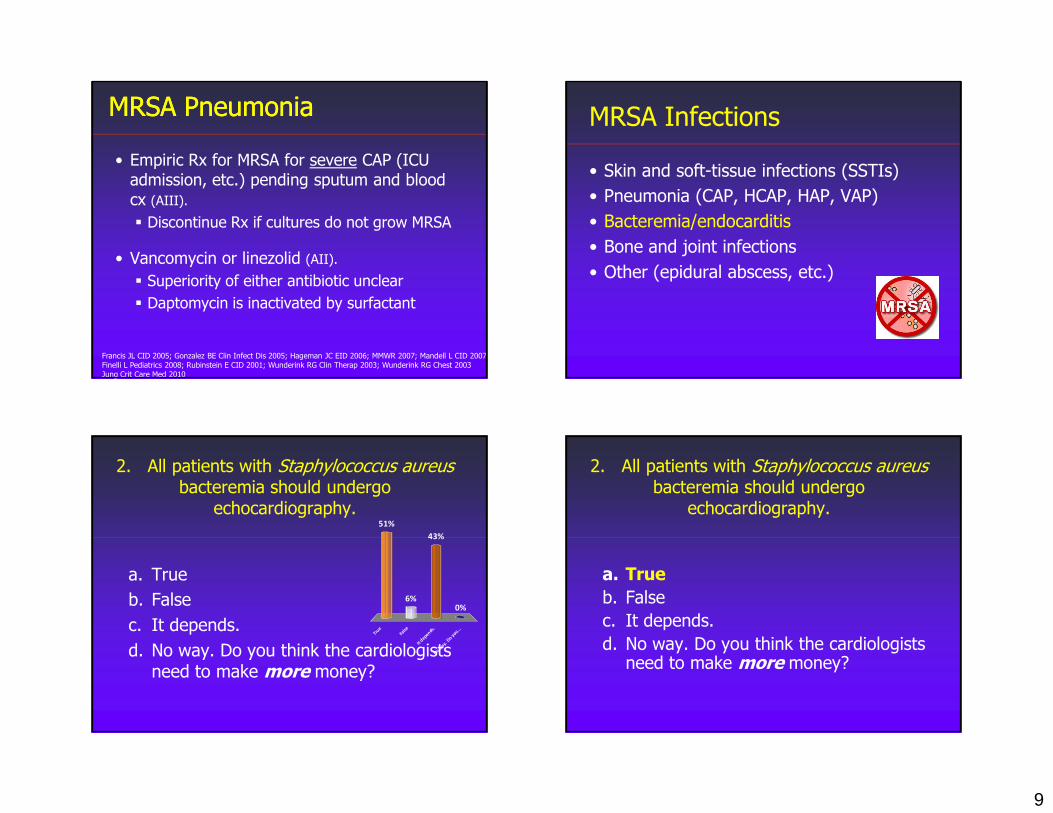
Microbiology of Purulent SSTIMicrobiology of Purulent SSTI
59.0%17.0%
2.6%
4.5%8.1%
9.0%
MRSA MSSA
B-hemolytic strep non-B hemolytic strep
other unknown
Moran NEJM 2006

6
CACA--MRSA SusceptibilitiesMRSA Susceptibilities
Antimicrobials % susceptible
TMP/SMX 100%
Rifampin 100%
Clindamycin 95%
Tetracycline 92%
Fluoroquinolones 60%
Erythromycin 6%
Moran GJ. NEJM. 2006
Purulent SSTIs Purulent SSTIs -- TreatmentTreatment
Outpatient (PO)
• Clindamycin
• Trimethoprim-sulfamethoxazole
• Tetracycline (doxycycline)
Inpatient (IV)
• Vancomycin
Common Inpatient Infections
CAP: A Practical Approach
NonNon--Purulent SSTIsPurulent SSTIs
• Erisypelas
-- Raised above skin
-- Clear borders
• Cellulitis
-- Poorly defined borders
Common Inpatient Infections
7
NonNon--Purulent SSTIsPurulent SSTIs
• Probably β-hemolytic streptoccal (group A strep) in most cases
-- Likely > 70%
• Unclear how often CA-MRSA in non-purulent SSTIs
-- “Role of CA-MRSA is unknown”
Liu C, et al. CID. 2011;52:285.Jeng A, et al. Medicine. 2010;89:217. Common Inpatient Infections
Treat MRSA in nonTreat MRSA in non--purulent SSTIpurulent SSTI
• Risk factors:
-- Hemodialysis, IVDU, SNF, recent abx
• Known prior MRSA
• (Possibly) MRSA rates > 30%
• Systemic illness
-- Fever, appearing ill, etc.
Stevens DL, et al. CID. 2005;41:1373. Common Inpatient Infections
NonNon--Purulent SSTIs Purulent SSTIs -- TreatmentTreatment
NO MRSA Risk*
Outpatient (PO)
• Dicloxacillin
• Cephalexin
Inpatient (IV)
• Cephazolin (?)
MRSA Risk
Outpatient (PO)
• Clindamycin
• Amoxicillin/TMP-SMX
• Linezolid
Inpatient (IV)
• Vancomycin
* If worse after 2nd day of treatment, consider change
Skin & softSkin & soft--tissue, MRSAtissue, MRSA
• Likely cause of purulent SSTIs.
• May or may not be involved with non-purulent SSTIs.
• If the patient is sick, treat for MRSA.
• Duration: 5-10 days.
Liu C, et al. CID. 2011;52:285.
8
1. A 34 man with no PMH presents with 3 days of forearm redness & pain; started after moving furniture. He is afebrile, looks well. Which
antibiotic would you choose?
a. Trimethoprim/sulfamethoxazole PO
b. Clindamycin PO
c. Cephalexin PO
d. Amoxicillin PO + TMP/SMX PO
e. Vancomycin PO
f. Steroids. I treat all rashes with steroids.
NonNon--Purulent SSTIs Purulent SSTIs -- TreatmentTreatment
NO MRSA Risk*
Outpatient (PO)
• Dicloxacillin
• Cephalexin
Inpatient (IV)
• Cephazolin (?)
MRSA Risk
Outpatient (PO)
• Clindamycin
• Amoxicillin/TMP-SMX
• Linezolid
Inpatient (IV)
• Vancomycin
* If worse after 2nd day of treatment, consider change
1. A 34 man with no PMH presents with 3 days of forearm redness & pain; started after moving furniture. He is afebrile, looks well. Which
antibiotic would you choose?
a. Trimethoprim/sulfamethoxazole PO
b. Clindamycin PO
c. Cephalexin PO
d. Amoxicillin PO + TMP/SMX PO
e. Vancomycin PO
f. Steroids. I treat all rashes with steroids.
MRSA Infections
• Skin and soft-tissue infections (SSTIs)
• Pneumonia (CAP, HCAP, HAP, VAP)
• Bacteremia/endocarditis
• Bone and joint infections
• Other (epidural abscess, etc.)
9
MRSA PneumoniaMRSA Pneumonia
• Empiric Rx for MRSA for severe CAP (ICU admission, etc.) pending sputum and blood cx (AIII).
� Discontinue Rx if cultures do not grow MRSA
• Vancomycin or linezolid (AII).
� Superiority of either antibiotic unclear
� Daptomycin is inactivated by surfactant
Francis JL CID 2005; Gonzalez BE Clin Infect Dis 2005; Hageman JC EID 2006; MMWR 2007; Mandell L CID 2007; Finelli L Pediatrics 2008; Rubinstein E CID 2001; Wunderink RG Clin Therap 2003; Wunderink RG Chest 2003 Jung Crit Care Med 2010
MRSA Infections
• Skin and soft-tissue infections (SSTIs)
• Pneumonia (CAP, HCAP, HAP, VAP)
• Bacteremia/endocarditis
• Bone and joint infections
• Other (epidural abscess, etc.)
2. All patients with Staphylococcus aureusbacteremia should undergo
echocardiography.
Tru
e
False
It d
epends. N
o way. D
o you...
51%
0%
43%
6%
a. True
b. False
c. It depends.
d. No way. Do you think the cardiologists need to make more money?
2. All patients with Staphylococcus aureusbacteremia should undergo
echocardiography.
a. True
b. False
c. It depends.
d. No way. Do you think the cardiologists need to make more money?
10
MRSA Bacteremia and Endocarditis
• All patients need echocardiography
� TEE preferred; can start with TTE
• For uncomplicated bacteremia, treat with 2 weeks of IV antibiotics
� No endocarditis, repeat cx negative, better in 3 days, no implanted prostheses
• For complicated bacteremia, treat with 4-6 weeks of IV antibiotics
Liu C, et al. CID. 2011;52:285.. Common Inpatient Infections
MRSA Bacteremia and Endocarditis
• Vancomycin or daptomycin (AII)
• Addition of gentamicin (AII) or rifampin (AI) to vancomycin is not recommended for bacteremia or native-valve endocarditis
� No clear evidence of benefit for either drug1
� Increased risk of nephrotoxicity2 with gentamicin
� Increased risk of drug interactions and development of rifampin resistance3
1Levine D Annals of Intern Med 1991; Riedel DJ AAC 2008; 2Rybak MJ AAC 1990; Goetz, MJ JAC 1993; Rybak MJ AAC 1999; Cosgrove SE CID 2009 3Riedel DJ AAC 2008
ID Consult & Staph ID Consult & Staph bacteremiabacteremia????
• Complex disease, high mortality
• Infectious diseases consultation associated with improved outcomes
-- Improved adherence to standards of care
-- Decreased mortality by 40-60%
Lahey T, et al. Medicine. 2009;88:263. Rieg S, et al. J Infect. 2009;59:232. Jenkins TC, et al. CID. 2008;46:1000. Honda H, et al. Am J Med. 2010;123:631. Common Inpatient Infections
Infection ControlInfection Control
Common Inpatient Infections
11
MRSA Control: What’s the Data?
• MRSA screening (active surveillance testing)-- Observational study over 3 consecutive time periods ↓ MRSA infections1
-- Cluster randomized trial of surgical patients – no benefit2
• Contact isolation-- Systematic review -- ↓ MRSA but many confounding interventions3
-- Prospective study – no change MRSA transmission4
-- Potential adverse consequences: pressure ulcers, falls, depression5
1Robicsek Ann Intern Med 2008; 2Harbarth JAMA 2008; 3Cooper BMJ
2004; 4Cepeda Lancet 2005; 5Stelfox JAMA 2003;
MRSA Control: What’s the Data?
• Hand hygiene-- Alcohol hand rub ↓ HA-MRSA (20%) and VRE
(40%), not C. diff4
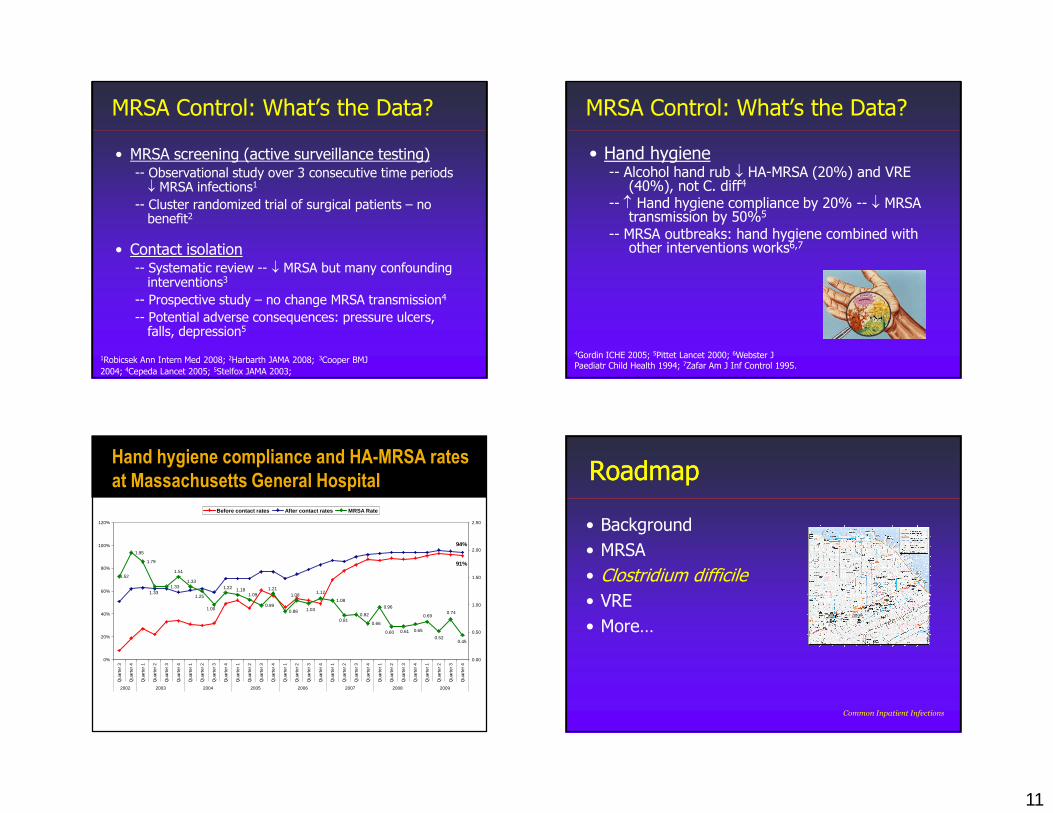
-- ↑ Hand hygiene compliance by 20% -- ↓ MRSA transmission by 50%5
-- MRSA outbreaks: hand hygiene combined with other interventions works6,7
4Gordin ICHE 2005; 5Pittet Lancet 2000; 6Webster J Paediatr Child Health 1994; 7Zafar Am J Inf Control 1995.
Hand hygiene compliance and HA-MRSA rates
at Massachusetts General HospitalHH and MRSA Rates
91%
94%1.95
1.79
1.33
0.990.88
1.08
0.82
0.66
0.960.74
1.03
1.091.25
0.52
0.69
0.650.61
1.52
1.00
1.33
0.81
1.121.08
1.211.181.22
1.51
1.33
0.60
0.45
0%
20%
40%
60%
80%
100%
120%
Qua
rter
3
Qua
rter
4
Qua
rter
1
Qua
rter
2
Qua
rter
3
Qua
rter
4
Qua
rter
1
Qua
rter
2
Qua
rter
3
Qua
rter
4
Qua
rter
1
Qua
rter
2
Qua
rter
3
Qua
rter
4
Qua
rter
1
Qua
rter
2
Qua
rter
3
Qua
rter
4
Qua
rter
1
Qua
rter
2
Qua
rter
3
Qua
rter
4
Qua
rter
1
Qua
rter
2
Qua
rter
3
Qua
rter
4
Qua
rter
1
Qua
rter
2
Qua
rter
3
Qua
rter
4
2002 2003 2004 2005 2006 2007 2008 2009
0.00
0.50
1.00
1.50
2.00
2.50
Before contact rates After contact rates MRSA Rate
RoadmapRoadmap
• Background
• MRSA
• Clostridium difficile
• VRE
• More…
Common Inpatient Infections
12
C. Diff MicrobiologyC. Diff Microbiology
• First isolated in 1935 (stool of a healthy infant)
• Named for difficulty in culture and isolation
• Association with disease recognized in 1978
• Now leading cause of hospital-acquired diarrhea
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247.
C. Diff EpidemiologyC. Diff Epidemiology
• Since 2001, ↑ incidence AND ↑ severity & mortality (Especially ≥ 65 year olds)
• Multiple outbreaks in US between 2001-2006
• Due to a virulent BI/NAP1/027 strain:
-- ↑↑↑↑ toxin A and B production
-- Production of a binary toxin
-- Deletion of tcdC gene (negative regulator of toxin prod)
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
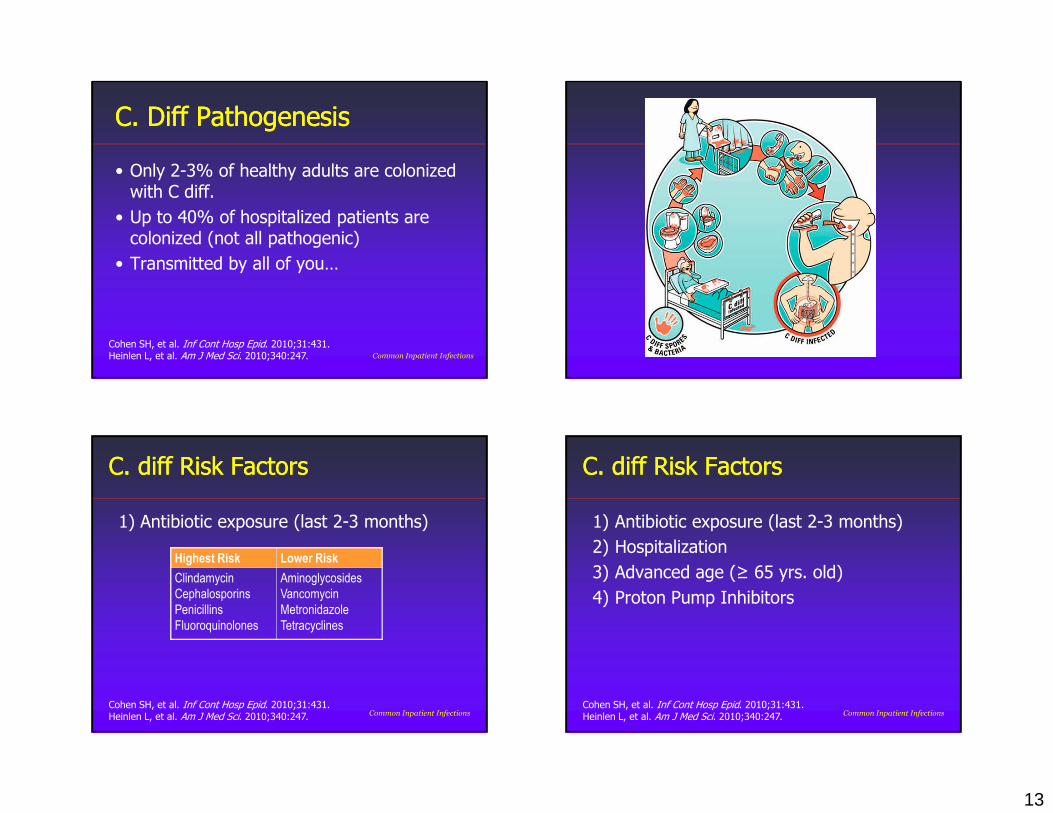
3. There are 80 people at the conference. What percentage of all of you are colonized with C diff (assume none have been hospitalized recently)?
90%
50%
10% 2% 0% I
can’t
believ.
..18%
25%
6%6%
25%
20%
a. 90%
b. 50%
c. 10%
d. 2%
e. 0%
f. I can’t believe I just licked my fingers…
3. There are 80 people at the conference. What percentage of all of you are colonized with C diff (assume none have been hospitalized recently)?
a. 90%
b. 50%
c. 10%
d. 2%
e. 0%
f. I can’t believe I just licked my fingers…
13
C. Diff PathogenesisC. Diff Pathogenesis
• Only 2-3% of healthy adults are colonized with C diff.
• Up to 40% of hospitalized patients are colonized (not all pathogenic)
• Transmitted by all of you…
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
C. diff Risk FactorsC. diff Risk Factors
1) Antibiotic exposure (last 2-3 months)
Highest Risk Lower Risk
Clindamycin
Cephalosporins
Penicillins
Fluoroquinolones
Aminoglycosides
Vancomycin
Metronidazole
Tetracyclines
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
C. diff Risk FactorsC. diff Risk Factors
1) Antibiotic exposure (last 2-3 months)
2) Hospitalization
3) Advanced age (≥ 65 yrs. old)
4) Proton Pump Inhibitors
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections

14
C. Diff DiagnosisC. Diff Diagnosis
“If the stool is not loose, the test is no use.”
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
C. Diff DiagnosisC. Diff Diagnosis
• Perform testing only on diarrheal (unformed) stool (B-II)
-- Only ~1% have ileus from severe colitis
-- Usually ≥ 3 times/day
• Do not test asymptomatic patients; no role for “test of cure.” (B-III)
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
C. Diff DiagnosisC. Diff Diagnosis
• Many different tests available
• Most are ELISA for toxin or for cell membrane proteins
• Find out your local testing – most have very high sensitivity
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
C. Diff TreatmentC. Diff Treatment
• Stop inciting antibiotic if possible! (A-II)
• Treat empirically if suspect severe or complicated C. difficile (C-III)
• Consider colectomy for severely ill patients (B-II) – consult surgery early!
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
15
4. A 65 yo man hospitalized 5 days prior for CAP now has fever, abdominal pain, and diarrhea (yes, loose). He appears ill and has a wbc of 22,000 and new acute renal failure (creatinine 2.2 mg/dL). A C diff test comes back positive. What is the optimal initial treatment?
Common Inpatient Infections Clin
damycin
PO
Vanco
myc
in P
O M
etronid
azole
...
Vanco
myc
in IV
Sto
ol tra
nspla
...
0%
31%
4%
12%
53%a. Clindamycin PO
b. Vancomycin PO
c. Metronidazole PO
d. Vancomycin IV
e. Stool transplant.
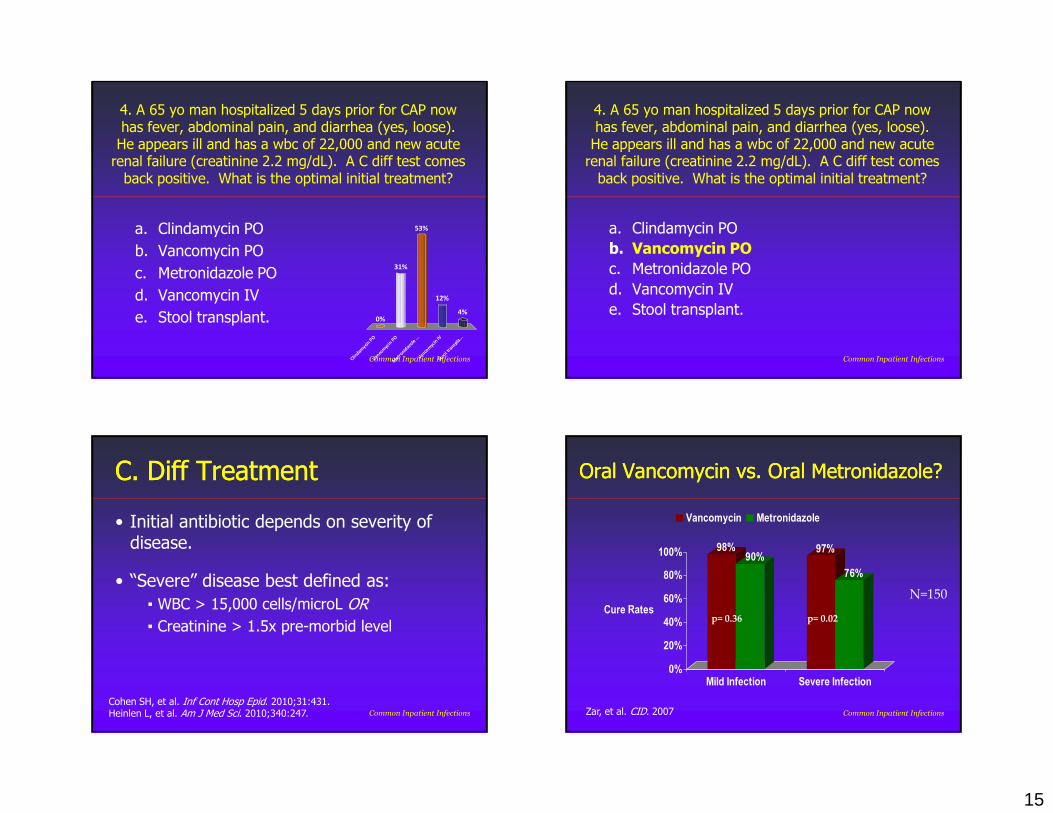
4. A 65 yo man hospitalized 5 days prior for CAP now has fever, abdominal pain, and diarrhea (yes, loose). He appears ill and has a wbc of 22,000 and new acute renal failure (creatinine 2.2 mg/dL). A C diff test comes back positive. What is the optimal initial treatment?
a. Clindamycin PO
b. Vancomycin PO
c. Metronidazole PO
d. Vancomycin IV
e. Stool transplant.
Common Inpatient Infections
C. Diff TreatmentC. Diff Treatment
• Initial antibiotic depends on severity of disease.
• “Severe” disease best defined as:
▪ WBC > 15,000 cells/microL OR
▪ Creatinine > 1.5x pre-morbid level
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247. Common Inpatient Infections
Oral Oral VancomycinVancomycin vs. Oral vs. Oral MetronidazoleMetronidazole??
98%90%
97%
76%
0%
20%
40%
60%
80%
100%
Cure Rates
Mild Infection Severe Infection
Vancomycin Metronidazole
Zar, et al. CID. 2007
p= 0.36 p= 0.02
N=150
Common Inpatient Infections
16
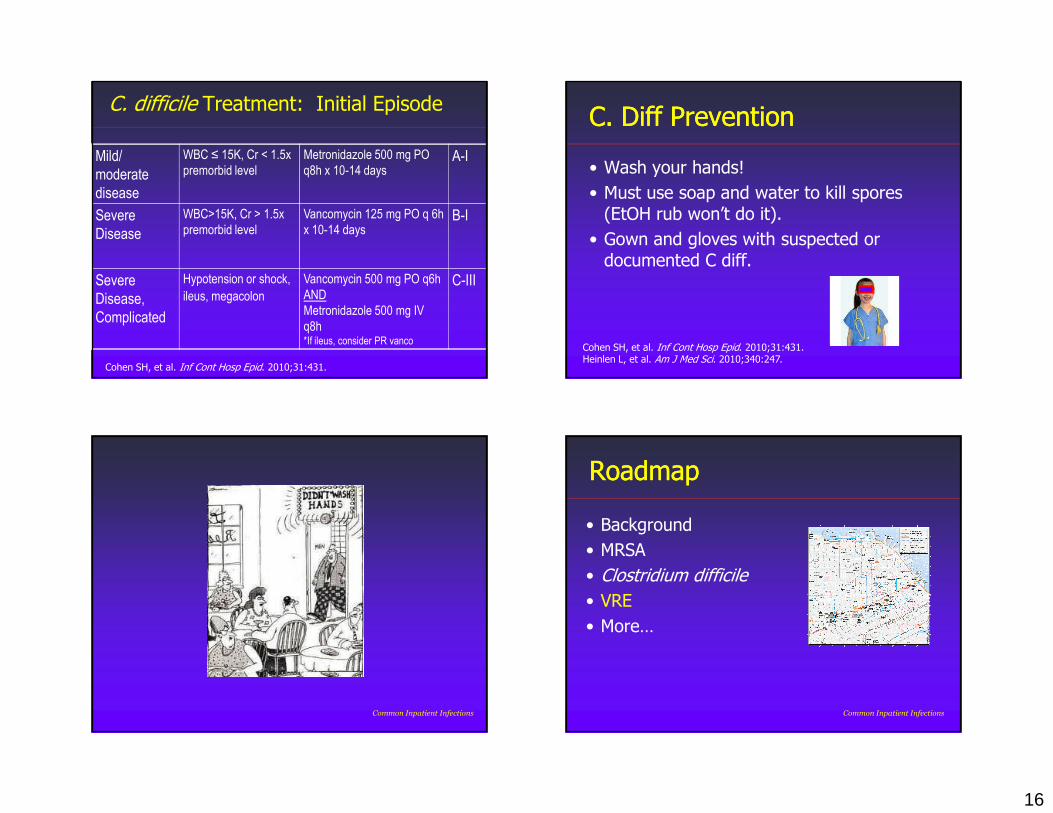
C. difficile Treatment: Initial Episode
Mild/
moderate
disease
WBC ≤ 15K, Cr < 1.5x
premorbid level
Metronidazole 500 mg PO
q8h x 10-14 daysA-I
Severe
Disease
WBC>15K, Cr > 1.5x
premorbid level
Vancomycin 125 mg PO q 6h
x 10-14 daysB-I
Severe
Disease,
Complicated
Hypotension or shock,
ileus, megacolon
Vancomycin 500 mg PO q6h
AND
Metronidazole 500 mg IV
q8h*If ileus, consider PR vanco
C-III
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431.
C. Diff PreventionC. Diff Prevention
• Wash your hands!
• Must use soap and water to kill spores (EtOH rub won’t do it).
• Gown and gloves with suspected or documented C diff.
Cohen SH, et al. Inf Cont Hosp Epid. 2010;31:431. Heinlen L, et al. Am J Med Sci. 2010;340:247.
Common Inpatient Infections
RoadmapRoadmap
• Background
• MRSA
• Clostridium difficile
• VRE
• More…
Common Inpatient Infections
17
EnterococcusEnterococcus MicrobiologyMicrobiology
• Enterococci are gram positive cocci, identified in 1980s
• Two main enterococcal species
▪ E. faecalis: 85-90% of isolates
▪ E. faecium: 5-10% of isolates
• Normal colonizer of human GI tract
Common Inpatient Infections
EnterococcusEnterococcus EpidemiologyEpidemiology
• Enterococcus causes infections in the hospital
▪ Second or third most common nosocomial infxn
• Generally fecal-oral transmission � colonization � infection
▪ Can survive in the hospital
• Risk factors for enterococcal infection:
▪ Long hospital or ICU admission
▪ Bone marrow or other transplant
▪ Urinary or vascular catheter
Noskin GA, et al. Inf Cont Hosp Epid. 1995;16:577.
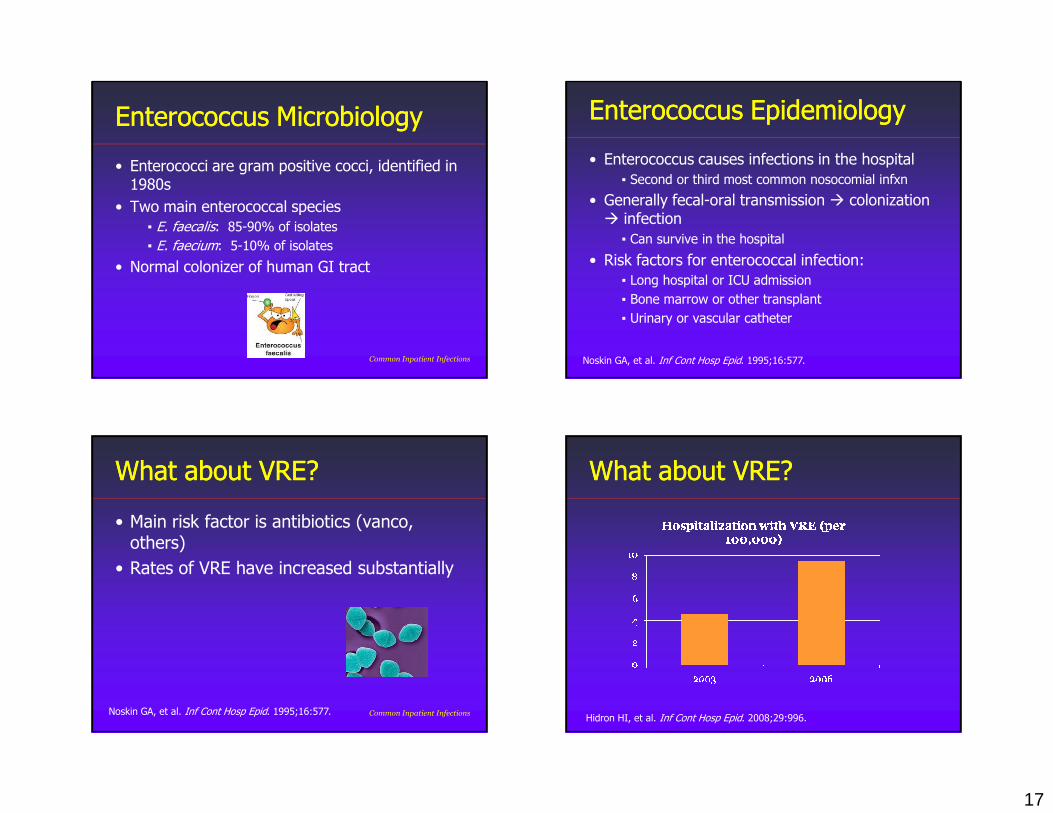
What about VRE?What about VRE?
• Main risk factor is antibiotics (vanco, others)
• Rates of VRE have increased substantially
Noskin GA, et al. Inf Cont Hosp Epid. 1995;16:577. Common Inpatient Infections
What about VRE?What about VRE?
Hidron HI, et al. Inf Cont Hosp Epid. 2008;29:996.
18
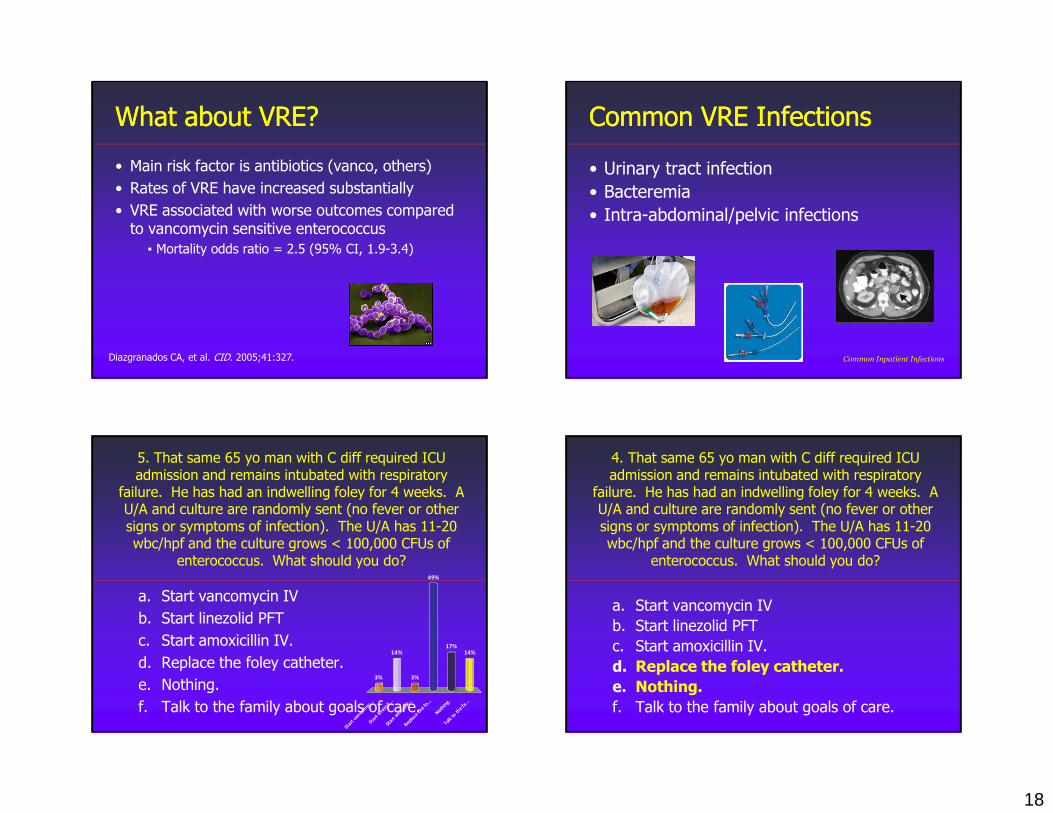
What about VRE?What about VRE?
• Main risk factor is antibiotics (vanco, others)
• Rates of VRE have increased substantially
• VRE associated with worse outcomes compared to vancomycin sensitive enterococcus
▪ Mortality odds ratio = 2.5 (95% CI, 1.9-3.4)
Diazgranados CA, et al. CID. 2005;41:327.
Common VRE InfectionsCommon VRE Infections
• Urinary tract infection
• Bacteremia
• Intra-abdominal/pelvic infections
Common Inpatient Infections
5. That same 65 yo man with C diff required ICU admission and remains intubated with respiratory
failure. He has had an indwelling foley for 4 weeks. A U/A and culture are randomly sent (no fever or other signs or symptoms of infection). The U/A has 11-20 wbc/hpf and the culture grows < 100,000 CFUs of
enterococcus. What should you do?
Sta
rt v
ancom
yc...
Sta
rt li
nezoli.
.. S
tart
am
oxici
l...
Repla
ce th
e fo...
Noth
ing.
Tal
k to th
e fa...
3%
14% 14%17%
49%
3%
a. Start vancomycin IV
b. Start linezolid PFT
c. Start amoxicillin IV.
d. Replace the foley catheter.
e. Nothing.
f. Talk to the family about goals of care.
4. That same 65 yo man with C diff required ICU admission and remains intubated with respiratory
failure. He has had an indwelling foley for 4 weeks. A U/A and culture are randomly sent (no fever or other signs or symptoms of infection). The U/A has 11-20 wbc/hpf and the culture grows < 100,000 CFUs of
enterococcus. What should you do?
a. Start vancomycin IV
b. Start linezolid PFT
c. Start amoxicillin IV.
d. Replace the foley catheter.
e. Nothing.
f. Talk to the family about goals of care.
19
VRE Urinary Tract InfectionVRE Urinary Tract Infection
• Urinary tract colonization w/ VRE common in ICU/hospital setting▪ Can stay colonized for > 1 year
• Need to differentiate between:
▪ Colonization
▪ Asymptomatic bacteriuria
▪ True infection
Byers KE, et al. Inf Cont Hosp Epid. 2002;23:207. Common Inpatient Infections
VRE Urinary Tract ColonizationVRE Urinary Tract Colonization
• Most VRE in the urine is colonization▪ In 100 pts, only 13% had true infection
▪ Others colonized or asymp. bacteriuria
▪ True infection more common in patients with cancer
Wong AH, et al. Am J Infect Cont. 2000;28:277. Common Inpatient Infections
VRE Urinary Tract InfectionVRE Urinary Tract Infection
True infection should include:
1) Symptoms (fever, confusion, malaise, flank pain, etc.)
2) Pyuria and/or leukocyte est/nitrate
3) ≥ 103 cfu/ml of enterococcus
Hooten TM, et al. CID. 2010;50:625. Common Inpatient Infections
VRE UTI TreatmentVRE UTI Treatment
• If true infection+ high-risk for VRE + ill, treat empirically for VRE▪ Linezolid pending cultures
• Replace the foley catheter▪ May help rid colonization
Heintz BH, et al. Pharmacotherapy. 2010;30:1136. Common Inpatient Infections
20
Common VRE InfectionsCommon VRE Infections
• Urinary tract infection
• Bacteremia
• Intra-abdominal/pelvic infections
Common Inpatient Infections
VRE VRE BacteremiaBacteremia
• Usually in patients with multiple morbidities
• From catheters, UTIs, GI tract
• Rarely associated with endocarditis
• Rarely associated with sepsis or severe illness▪ Consider gram-negative polymicrobial infxn
Wisplinghoff H, et al. CID. 2004;39:309. Common Inpatient Infections
VRE VRE BacteremiaBacteremia
• Treat empirically for VRE in high-risk patients
• Await sensitivities
• Duration of treatment unclear▪ Likely 1-2 weeks for bacteremia
▪ Probably 4-6 weeks for endocarditis
Common Inpatient Infections
Common VRE InfectionsCommon VRE Infections
• Urinary tract infection
• Bacteremia
• Intra-abdominal/pelvic infections
Common Inpatient Infections
21
VRE Abdominal/Pelvic InfectionVRE Abdominal/Pelvic Infection
• Usually mixed aerobic/anaerobic infection
• Not the most virulent (vs. GNRs)
• If grow it in culture, should treat it
• Duration of treatment unclear – parellel tx of other organisms
VRE PreventionVRE Prevention
• Wash your hands!
• Data on contact isolation is mixed – follow your local policy
Common Inpatient Infections
RoadmapRoadmap
• Background
• MRSA
• Clostridium difficile
• VRE
• More…
Common Inpatient Infections
GramGram--negative HAIsnegative HAIs
• MDR Pseudomonas aeruginosa
• MDR Acinetobacter baumanii
• ESBL producing E. coli and Klebsiella
• Carbapenem-resistant Enterobacteriaceae(CRE)
22
5. I always gel in and gel out (or wash) each time I see patients in the inpatient setting.
Tru
e
False
45%
55%
1. True
2. False
Common Inpatient Infections
RoadmapRoadmap
• Background
• MRSA
• Clostridium difficile
• VRE
• More…
Common Inpatient Infections Common Inpatient Infections
Specific Goals:Specific Goals:
• Appreciate the morbidity and mortality associated with hospital-acquired infections (HAIs).
• Describe optimal therapy for MRSA infections.
• List key principles in the management of Clostridium difficile infection.
• Understand evidence for preventing HAIs.
23
Common Inpatient Infections
MRSA TakeMRSA Take--home Pointshome Points
• Treat for MRSA with purulent SSTIs; consider in non-purulent SSTIs if risk factors or systemically ill
• Add vanco for patients with CAP admitted to the ICU
• Consider ID consultation in patients with S. aureus bacteremia
Common Inpatient Infections
C Diff. TakeC Diff. Take--home Pointshome Points
• “If the stool is not loose, the test is no use!”
• Treat severe disease (wbc > 15,000, Cr > 1.5x) with oral vancomycin
Common Inpatient Infections
VRE TakeVRE Take--home Pointshome Points
• VRE infections are generally in sick hospitalized patients.
• Most patients with VRE in the urine are colonized or have asymp. bacteriuria
• For true infection, need symptoms + pyuria + positive culture.
Management of Common Management of Common Inpatient Infections:Inpatient Infections:
MRSA, C diff, VRE, and more…MRSA, C diff, VRE, and more…
Bradley A. Sharpe, M.D.Associate Professor Medicine
Department of MedicineUCSF







