Finance
Eve BakerDirector of Finance
Debbie FraserDeputy Director of Finance
3 Questions
• What skills will you need at your disposal to deliver the finance management agenda?
• What can you do differently on a daily basis to deliver QIPP?
• How many Finance Directors does it take to change a light bulb?
How is the PCT Funded
PCT Allocation is based on• Responsible Population • ONS
+/- patients registered with one practice while resident in another PCT area+ All Prisoners irrespective of the time in prison+ Armed Forces+ Asylum seekers
• This is then adjusted for age, need and MFF• Add Primary Dental, Ophthalmic and
Pharmaceutical funding• Add Funding Support for Social Care
Funding per crude head of population – including Funding for Social Care
Exposition Book March 2011
Lowest - Berkshire West - £1,367
Highest - Islington - £2,350
Average allocation - £1,693
NHS Berkshire East - £1,451 - 9th Lowest
Additional allocation if avge per head £98m
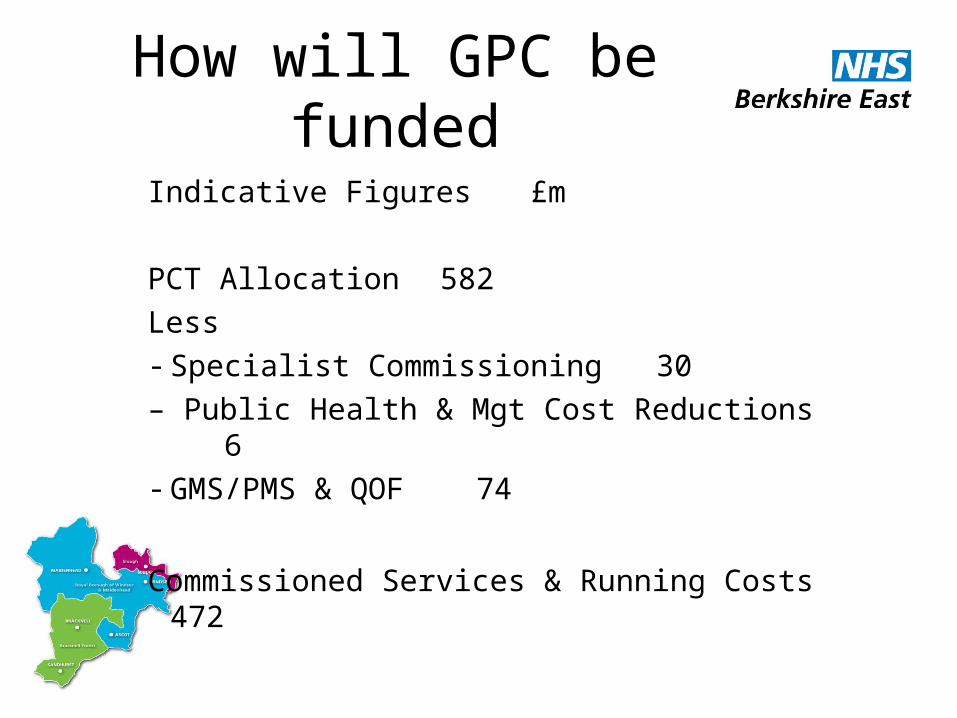
How will GPC be funded
Indicative Figures £m
PCT Allocation 582
Less- Specialist Commissioning 30
– Public Health & Mgt Cost Reductions 6- GMS/PMS & QOF 74
Commissioned Services & Running Costs 472
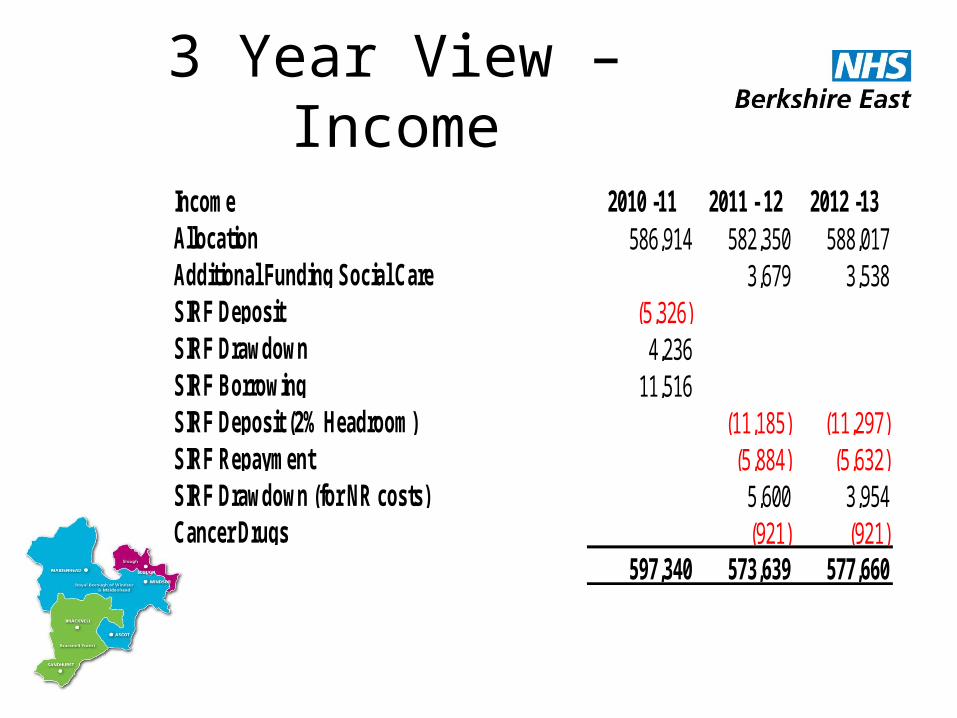
3 Year View – Income
Income 2010 -11 2011 - 12 2012 -13Allocation 586,914 582,350 588,017Additional Funding Social Care 3,679 3,538SIRF Deposit (5,326)SIRF Drawdown 4,236SIRF Borrowing 11,516SIRF Deposit (2% Headroom) (11,185) (11,297)SIRF Repayment (5,884) (5,632)SIRF Drawdown (for NR costs) 5,600 3,954Cancer Drugs (921) (921)
597,340 573,639 577,660
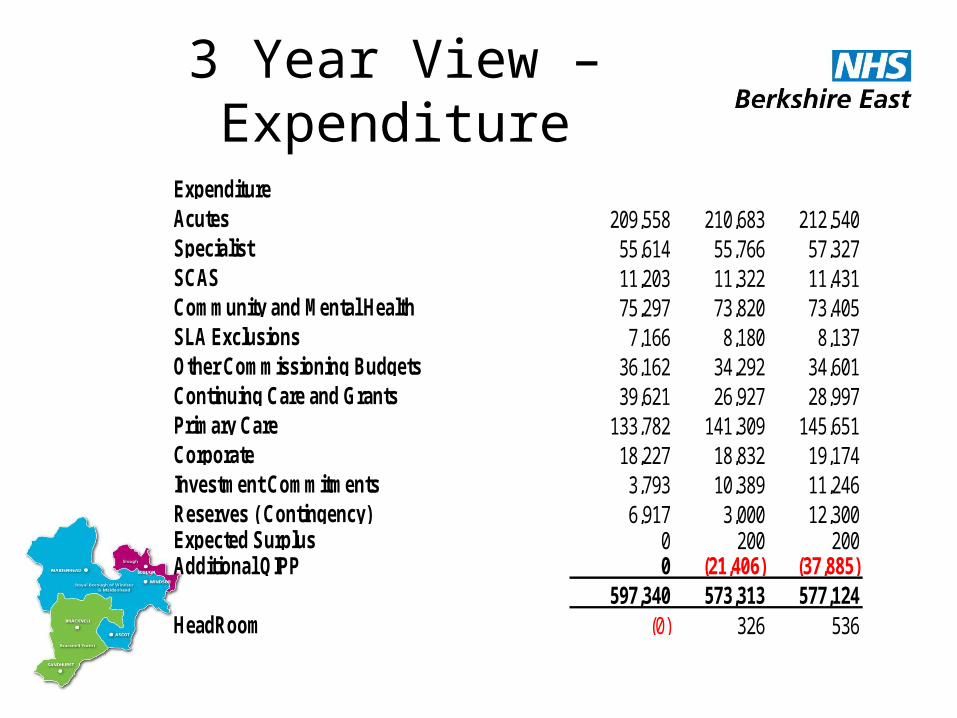
3 Year View – Expenditure
ExpenditureAcutes 209,558 210,683 212,540Specialist 55,614 55,766 57,327SCAS 11,203 11,322 11,431Community and Mental Health 75,297 73,820 73,405SLA Exclusions 7,166 8,180 8,137Other Commissioning Budgets 36,162 34,292 34,601Continuing Care and Grants 39,621 26,927 28,997Primary Care 133,782 141,309 145,651Corporate 18,227 18,832 19,174Investment Commitments 3,793 10,389 11,246Reserves ( Contingency) 6,917 3,000 12,300Expected Surplus 0 200 200Additional QIPP 0 (21,406) (37,885)
597,340 573,313 577,124HeadRoom (0) 326 536
Remaining Risks 2010/11
• With SIRF Borrowing support should break even
• Legacy Risks resolved
• Disputes with HWP over - Data Challenges- Readmission Thresholds
• Attempting a negotiated settlement
• Frimley & RBFT smaller risks
Key Risks 2011/12
• Recurrent overspend B/fwd• Repayment of support in 2011/12• Delivery of QIPP- Big Hitters
- Urgent Care - Managing the order book - PLCV - Intermediate care and EOL
• Changes in Provider Market Share• Impact of QIPP on Providers
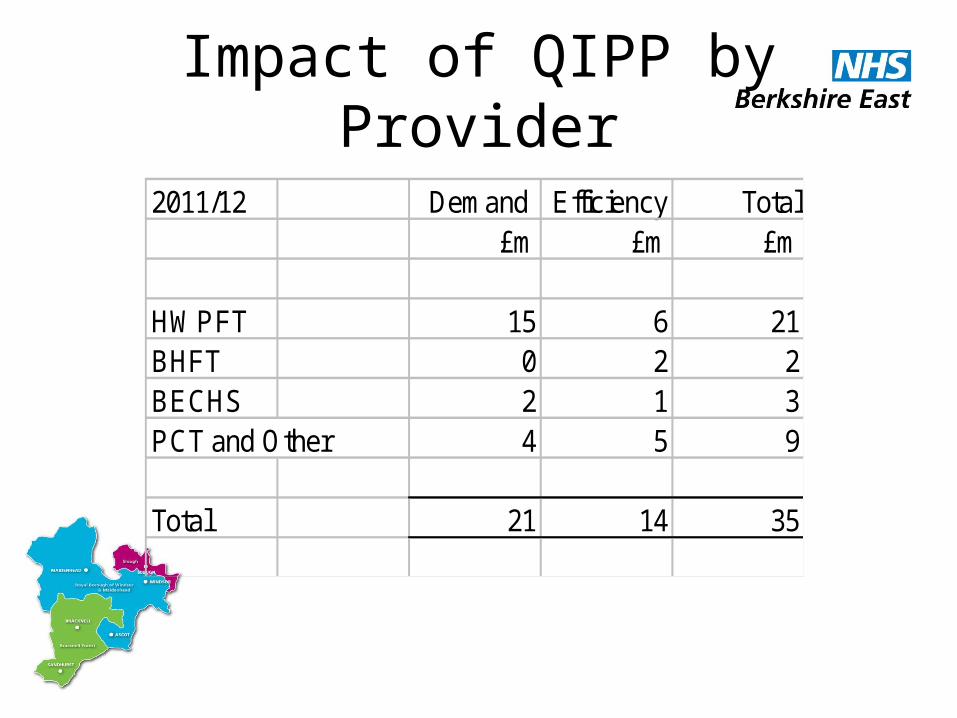
Impact of QIPP by Provider
2011/12 Demand Efficiency Total£m £m £m
HWPFT 15 6 21BHFT 0 2 2BECHS 2 1 3PCT and Other 4 5 9
Total 21 14 35
The Finance Function
What does PCT Finance currently do?
• Financial and Statutory Reporting
• Balance Sheet
• Capital Asset Accounting
• Cash and Treasury
• Raising invoices and debt collection
What does PCT Finance currently do?• Creditors (BPPC)/Procurement
• Management accounting and reporting
• Financial Planning (operating plan/medium term plans)
• QIPP
• VAT accounting
• Payroll and Staff Expenses
What finance functions are GP Consortia likely to
require?
Emerging guidance is giving indications…
• Keep Proper Accounts/Annual Audit
• In year reporting against budgetary/parliamentary controls to NHS CB (financial and other data)
• Budgeting
What finance functions are GP Consortia likely to
require?• Monitoring of budgets• Managing Revenue Resource Limit
to achieve breakeven• Managing Capital Funding
(consortium premises/IT)• Developing and delivering
operational plans• Longer term financial plans
What finance functions are GP Consortia likely to
require?• Monitoring of admin costs so not
to exceed running cost allowance
• Use prescribed banking service (Government banking system) to manage consortium’s funds– Request funds in advance– No significant month end balance
Support to GPCC in Transition
• Restructure across the Cluster – Finance, Contracts, Information
• Move to shadow CSU over time• Maintain core specialist functions and
transaction processes• Create customer facing roles so that each
consortia knows where it will access specialist support
• Draft structures for comment as soon as possible following appointment of SAO and SFO
What might a CSU include?
• Finance – Separate Consortia allocations and business entities
• Contracts – 1 Specialist team per provider to consolidate Consortia Commissioning Intentions.
• Berkshire wide Informatics framework – supporting commissioning, contracting, planning, reporting
• BSS services – CSU infrastructure, CSU Transaction processes, Procurement services, GP Premises, GP IT.
• Primary Care Agency
Discussion paper under preparation







