Evaluation of the chestEvaluation of the chest
part 1part 1
Nagy EndreNagy Endre
SZEGEDI TUDOMÁNYEGYETEM SZEGEDI TUDOMÁNYEGYETEM ÁOK, RADIOLÓGIAI KLINIKA, ÁOK, RADIOLÓGIAI KLINIKA,
SZEGEDSZEGED
Indication
In case of complaints or symptoms:
• In suspicion of lesions, diseases or injuries of the chest organs and
• On the basis of complaints, clinical signs and lab findings
Indication
If free of complaints:
• In case of such diseases of distant organs that may cause – even symptomless – lesions of the chest (e.g. metastasis)

Indication
For prevention:
• Exclusion of lung and heart diseases before operation and complex anesthesia
• In case of unconsciousness or polytrauma.

Indication
In healthy patients:for screening or evaluation of fitness
for work; before settling down or having a job.
Limited indication
• Follow-up of previously detected lesions (e.g. pneumonia)
• Thoracal diseases inducing dullness(US instead)
• Supposedly mediastinal lesions (MRI instead)
Contraindication
• Only cardiopulmonary resuscitation in progress
• (→ it can be performed in recumbent position or even on an unconscious patient!)
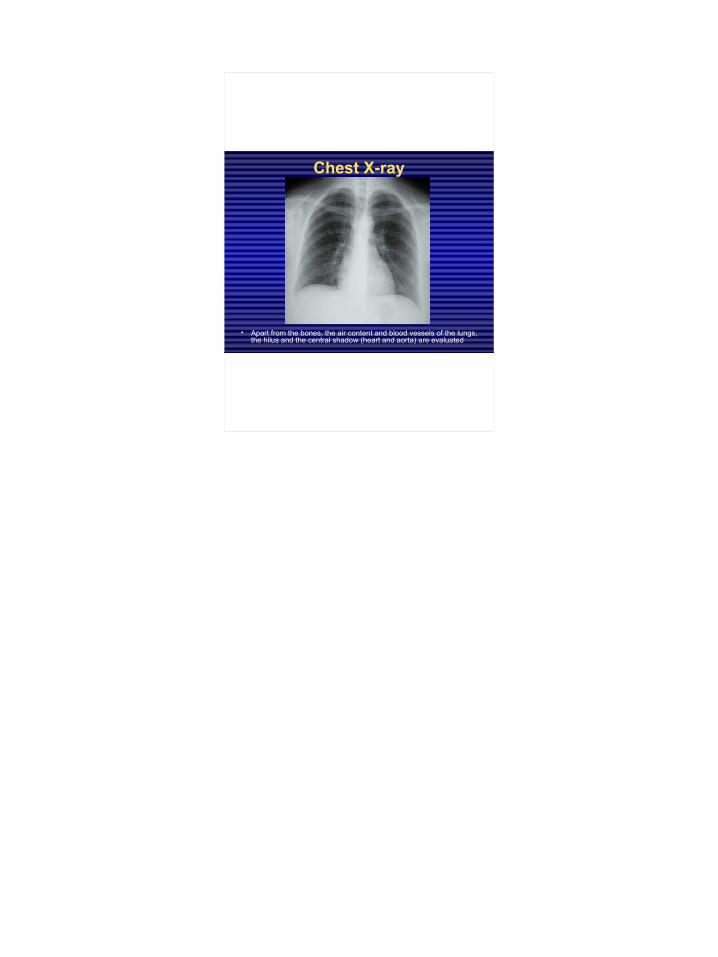
Chest X-ray
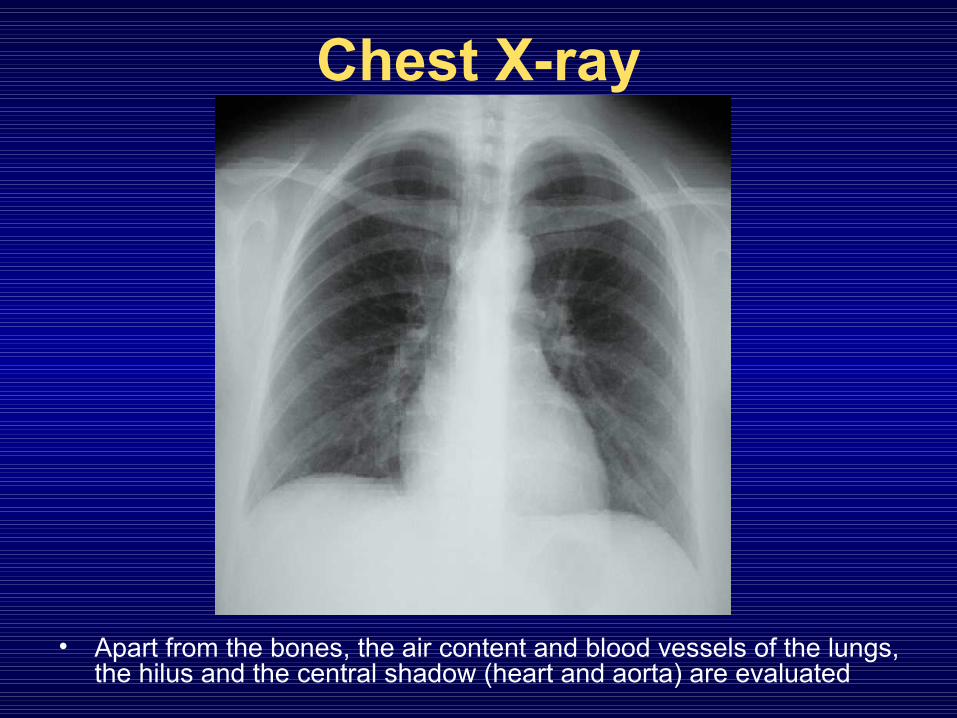
• Apart from the bones, the air content and blood vessels of the lungs, the hilus and the central shadow (heart and aorta) are evaluated
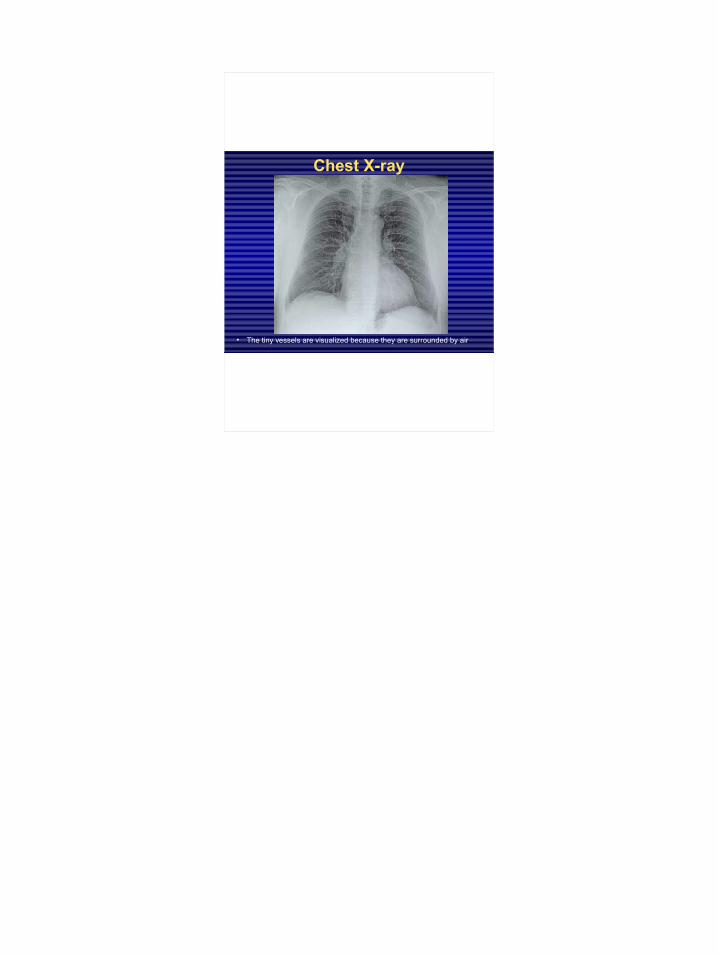
Chest X-ray
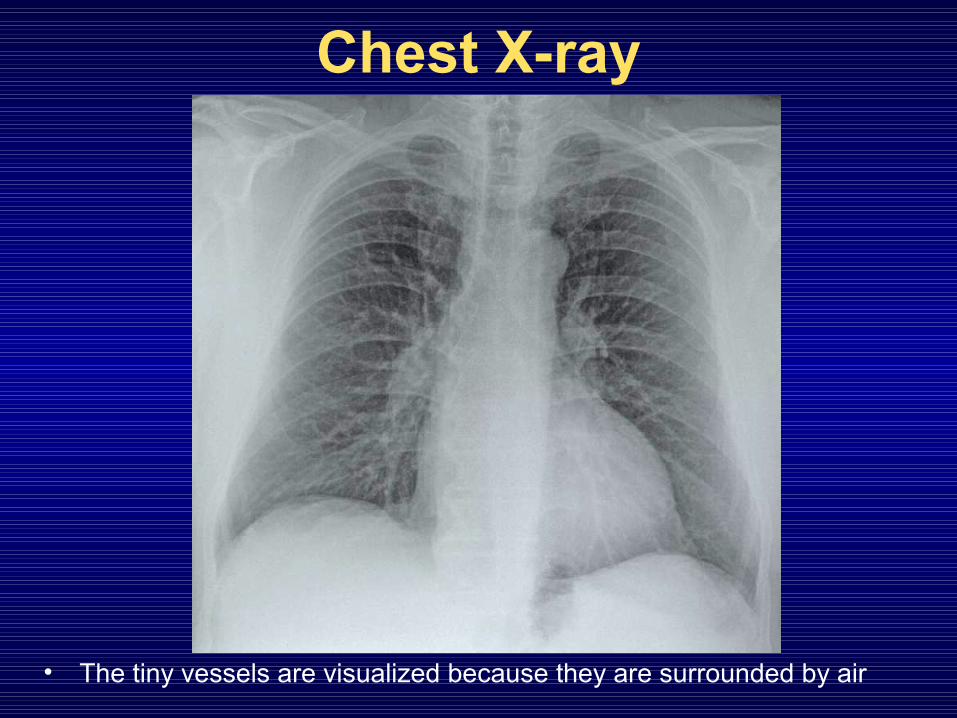
• The tiny vessels are visualized because they are surrounded by air

For the interpretation of the image it is helpful to know:
• age• sex• physical activity• occupation• smoking, alcohol, drug abuse• clinical data
Clinical background presumes
extended shadow in the lung
+ fever → pneumonia+ foreign body aspiration → atelectasis+ difficulty breathing and thrombophlebitis →
infarction+ cough, smoking → cancer+ unconsciousness, vomiting → aspiration+ penetrating injury → hematoma in the lung…
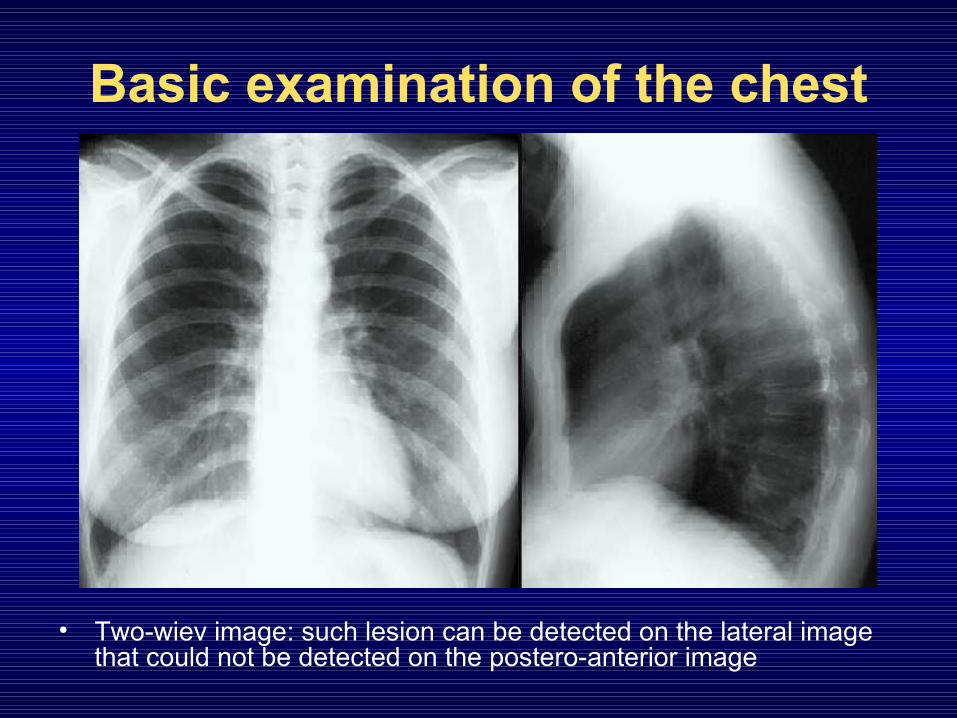
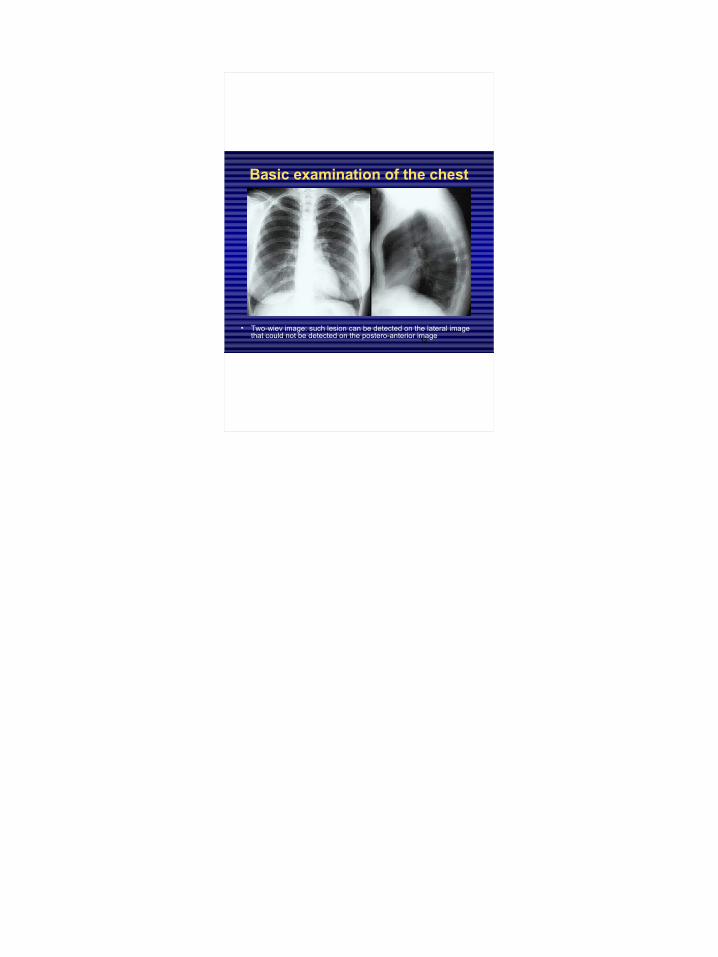
Basic examination of the chest
• Two-wiev image: such lesion can be detected on the lateral image that could not be detected on the postero-anterior image
Additional X-ray procedures• Fluoroscopy• Oblique images• Images in lateral position• Images in exspiration• fluorography• (conventional tomography)• Digital radiography• „dual energy” technique
Fluoroscopy
Visualizes motions and provides spatial information

Oblique image
For the evaluation of covered or complex structures
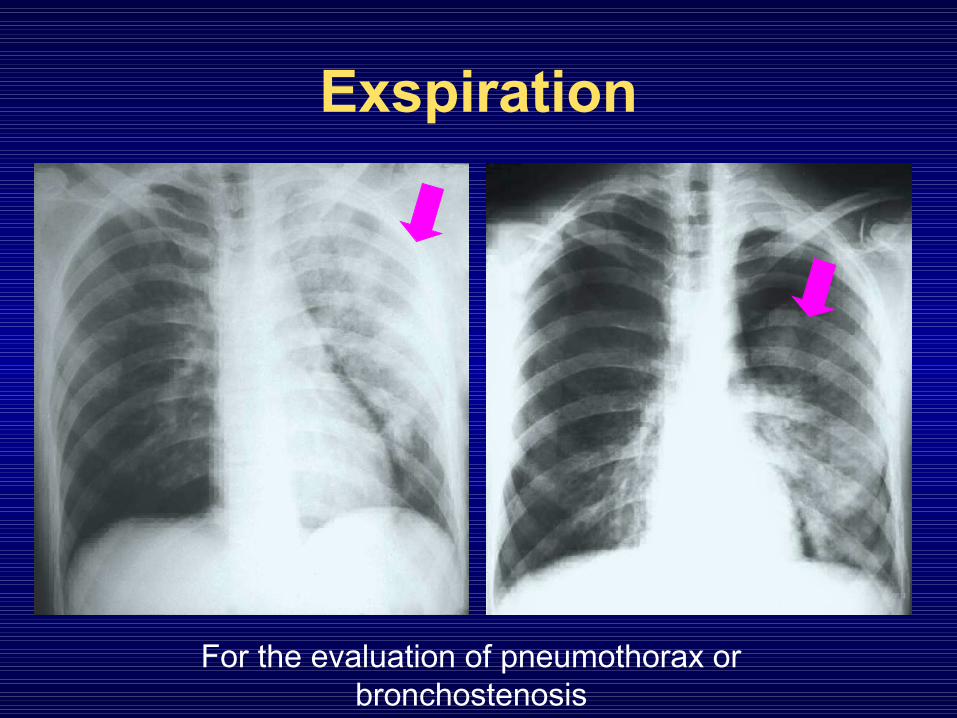
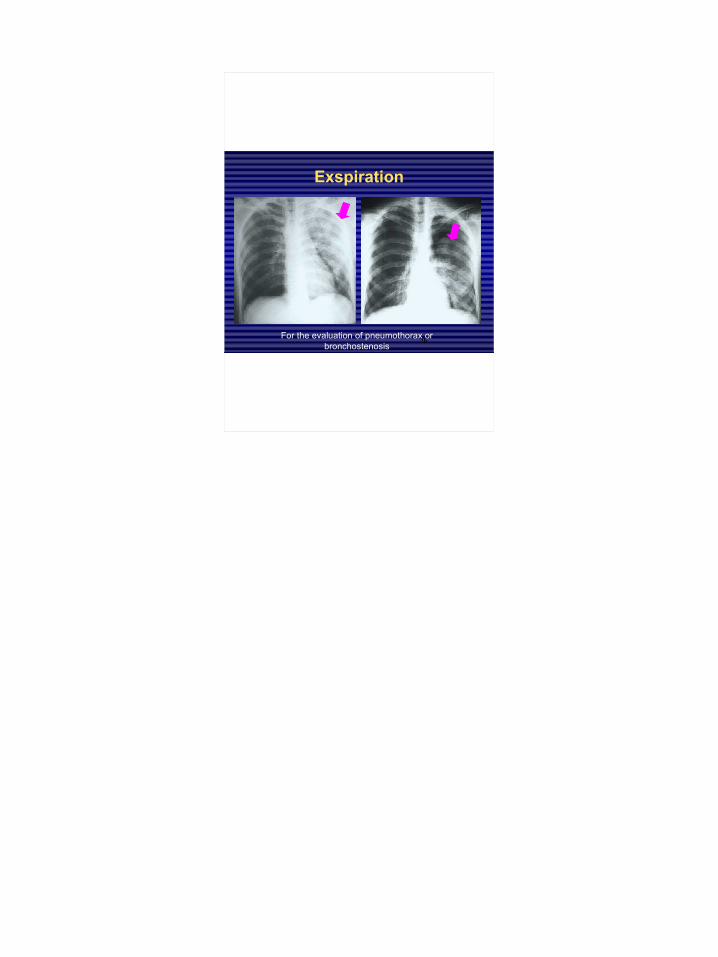
Exspiration
For the evaluation of pneumothorax or bronchostenosis
Fluorogram
small size analogous or digital picture made directly from the fluoroscope in order to screening

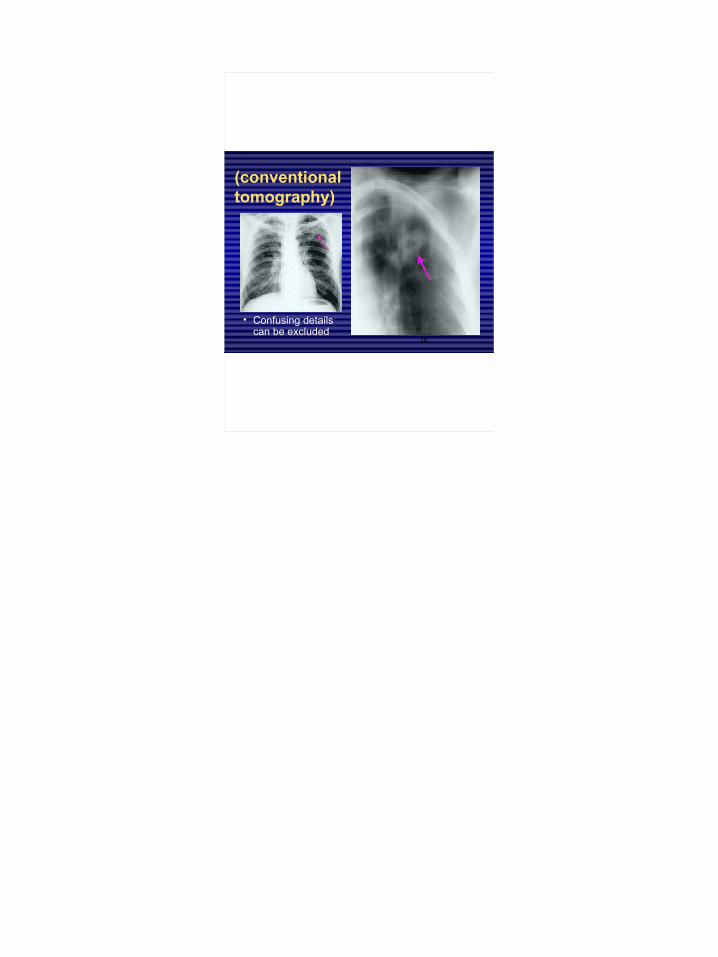
(conventional tomography)
• Confusing details can be excluded
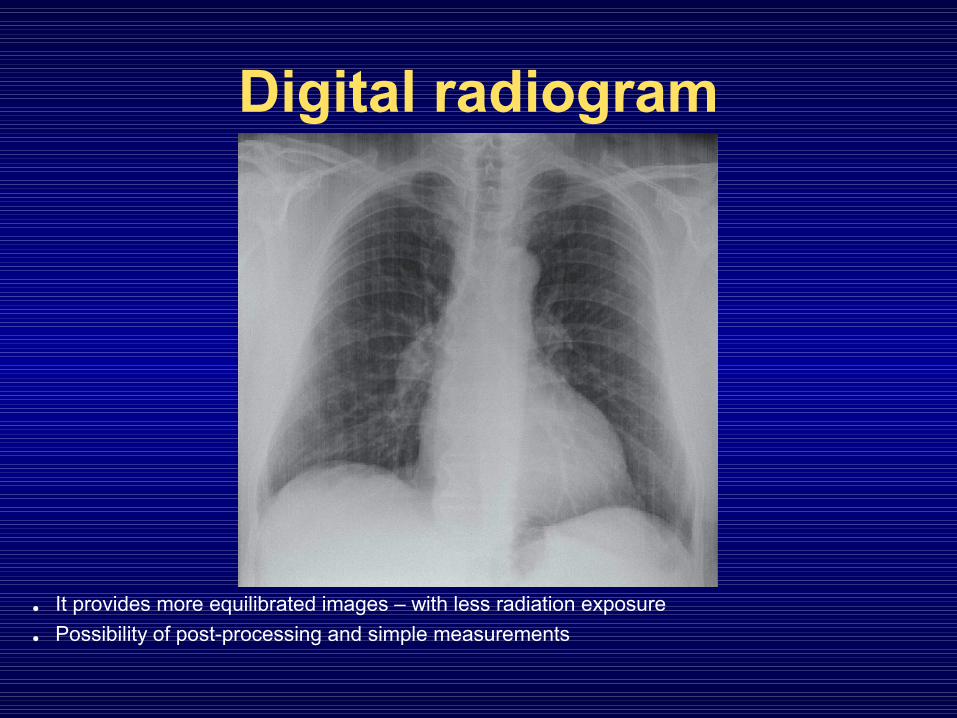
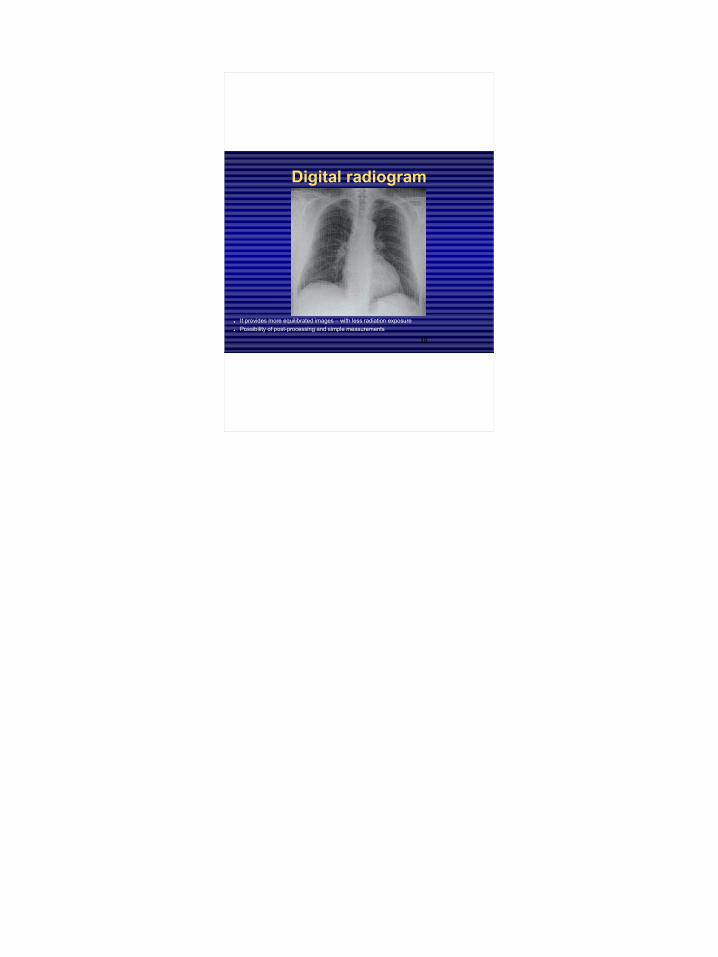
Digital radiogram
• It provides more equilibrated images – with less radiation exposure
• Possibility of post-processing and simple measurements
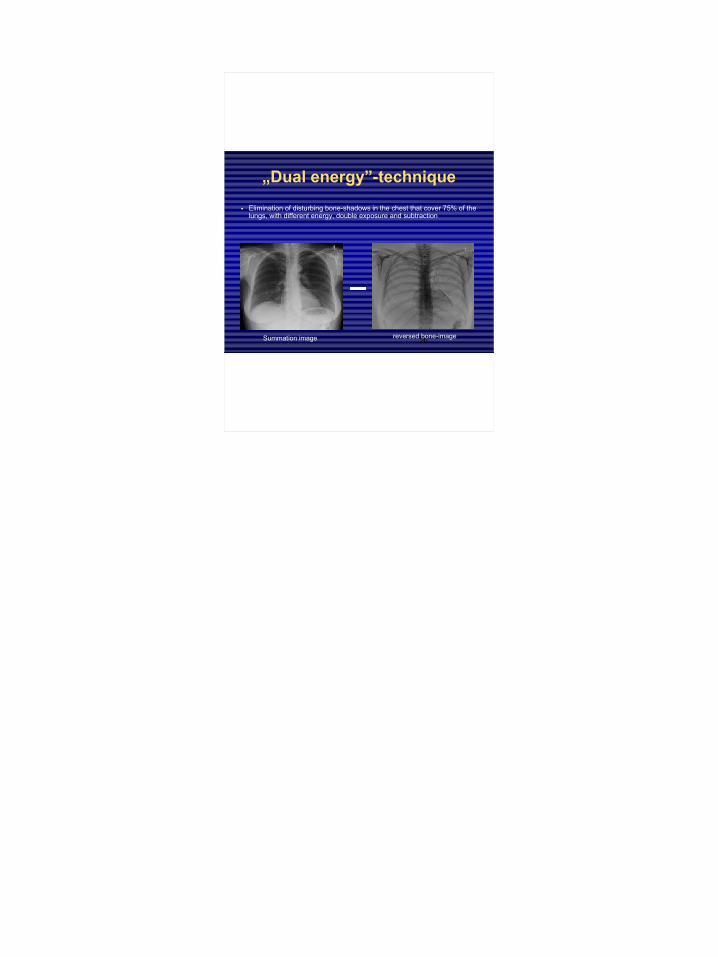
„Dual energy”-technique
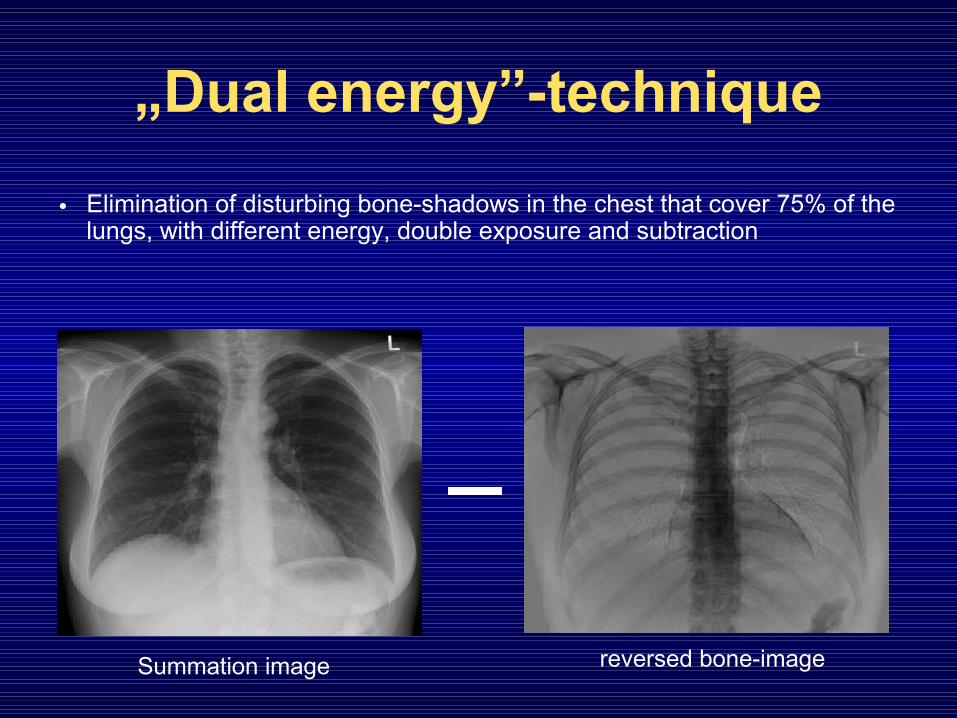
• Elimination of disturbing bone-shadows in the chest that cover 75% of the lungs, with different energy, double exposure and subtraction
Summation image reversed bone-image
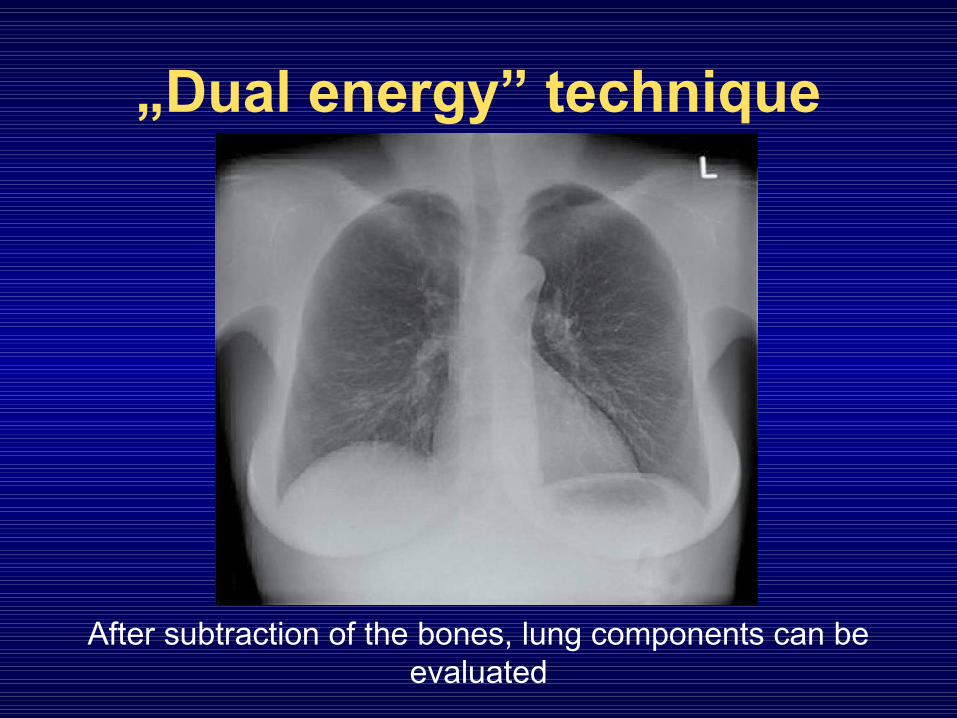
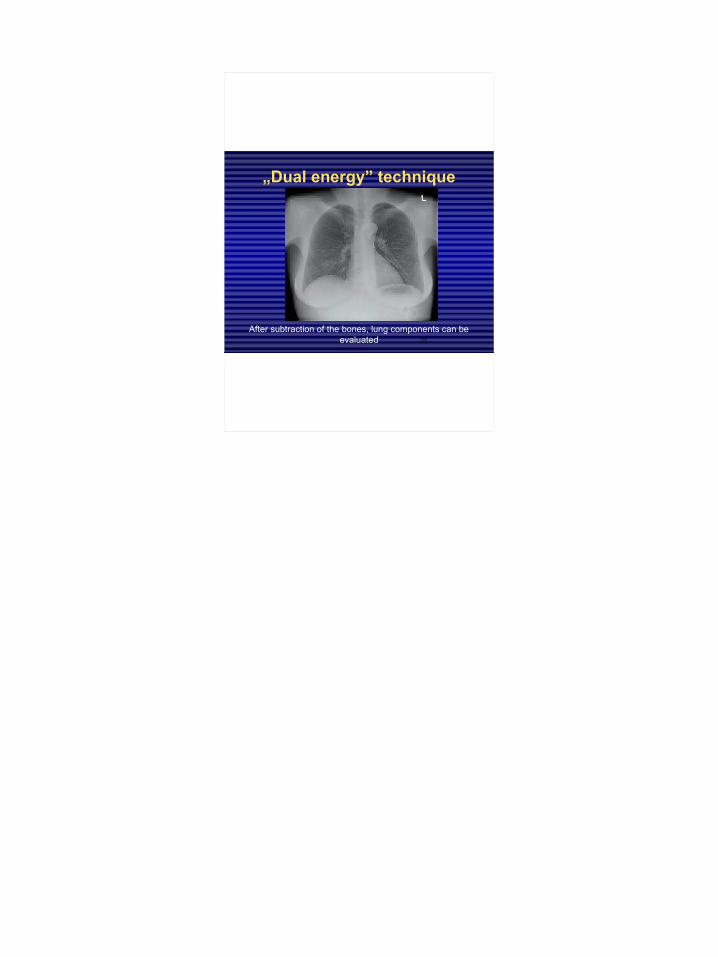
„Dual energy” technique
After subtraction of the bones, lung components can be evaluated
Application of contrast materials
• water-soluble iodinated contrast materials are used• in the bronchi:
– bronchography• blood vessels:
– arteries: pulmonary or bronchial– veins: pulmonary or systemic

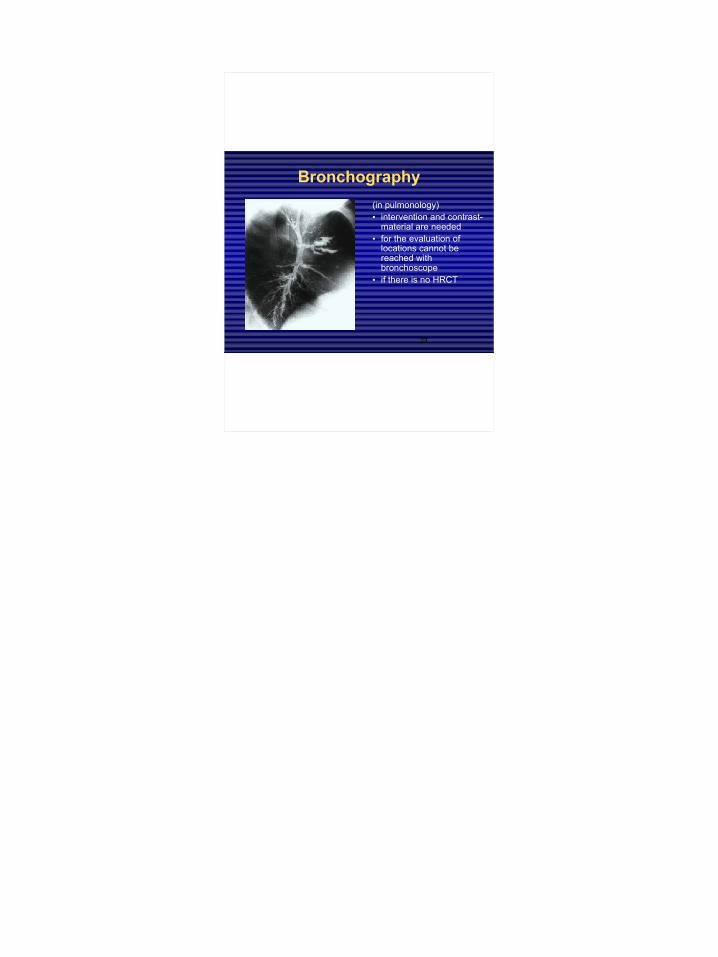
Bronchography(in pulmonology)• intervention and contrast-
material are needed• for the evaluation of
locations cannot be reached with bronchoscope
• if there is no HRCT
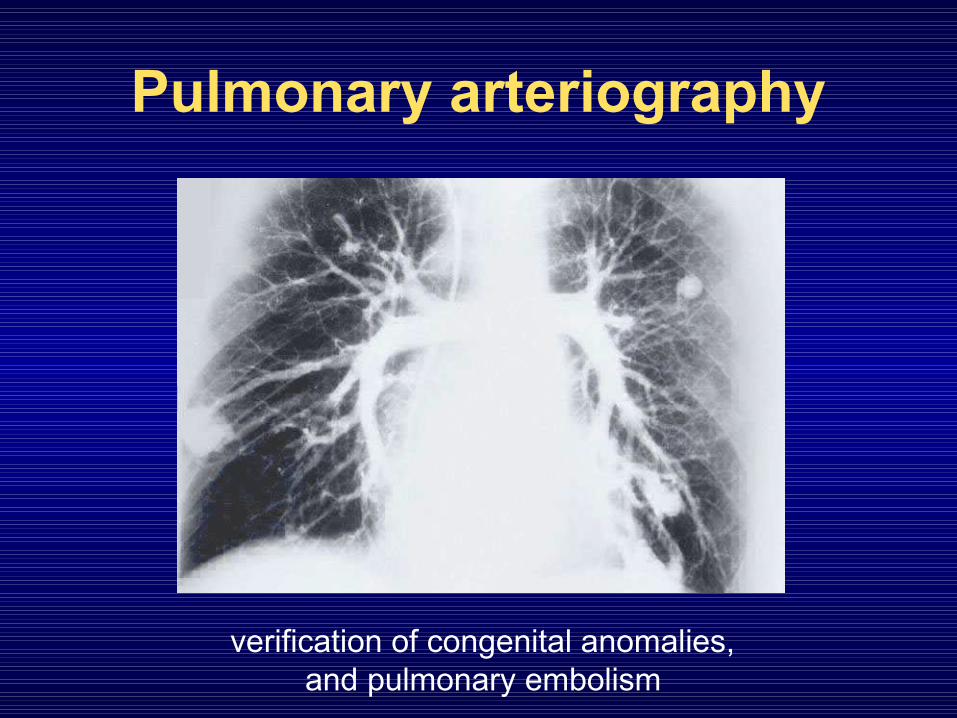
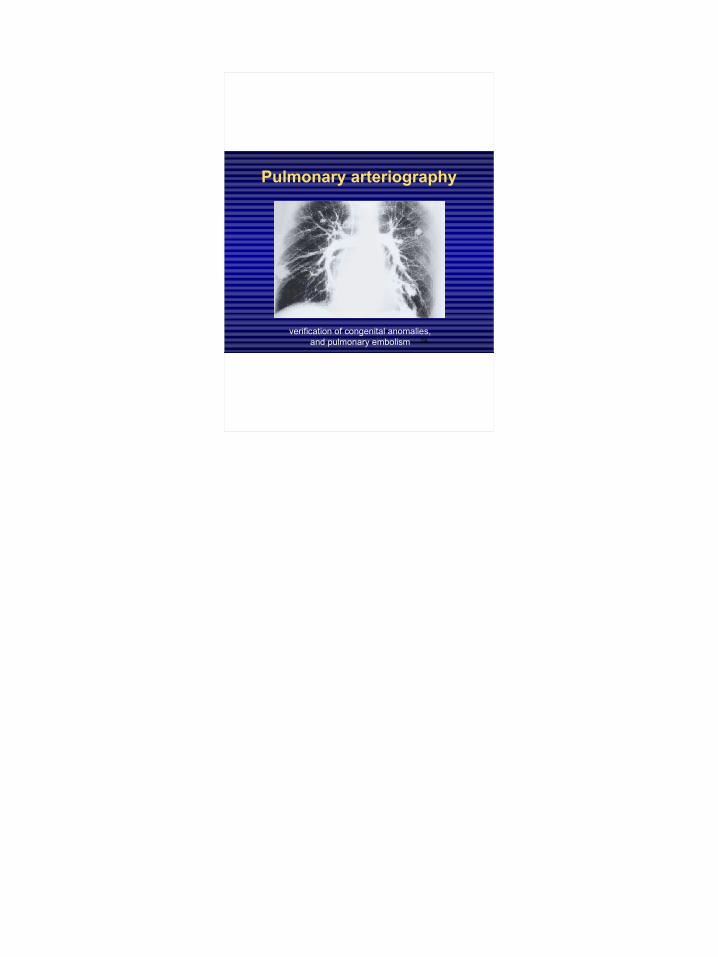
Pulmonary arteriography
verification of congenital anomalies, and pulmonary embolism
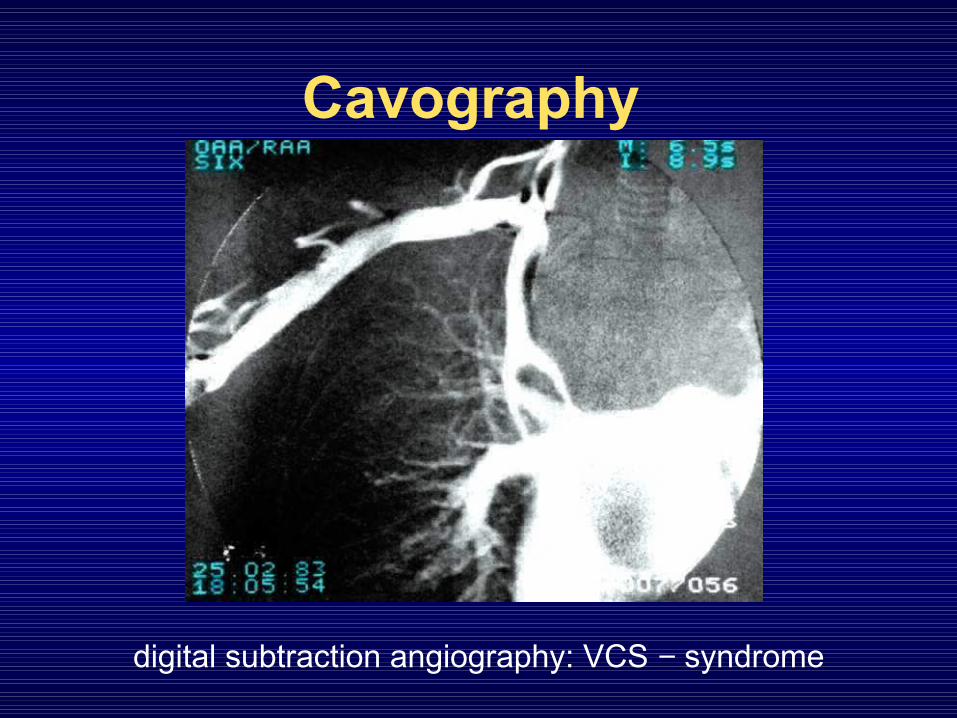
Cavography
digital subtraction angiography: VCS − syndrome
Native and contrast enhanced CT
• at first:
– axial images
– without contrast-material
• more precisely:
– reconstruction in different plains
– with iv. water-soluble iodinated contrast-material
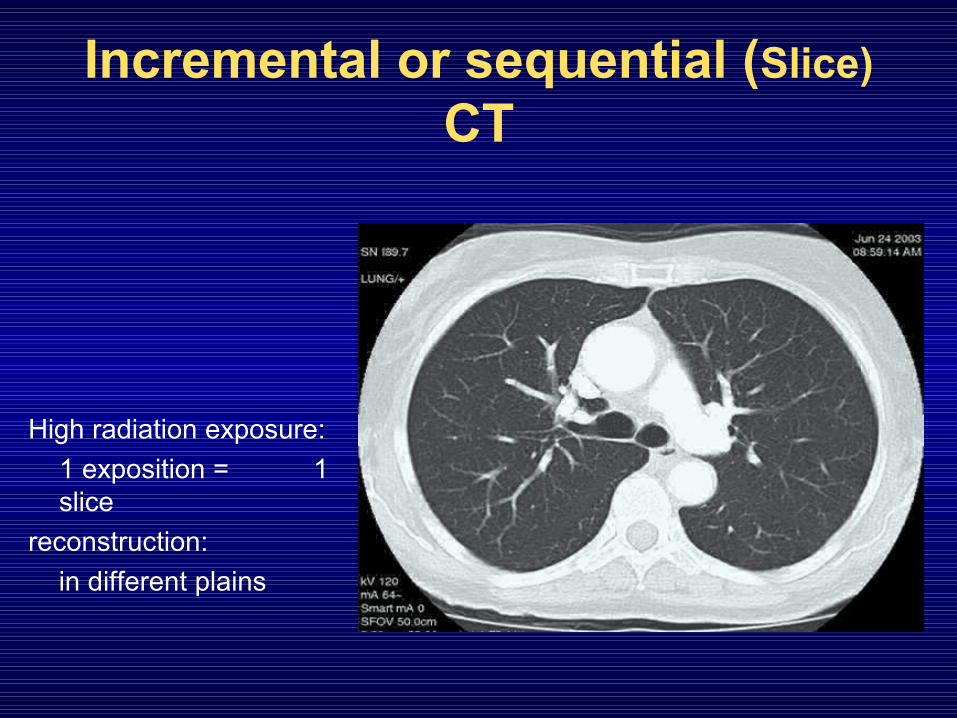
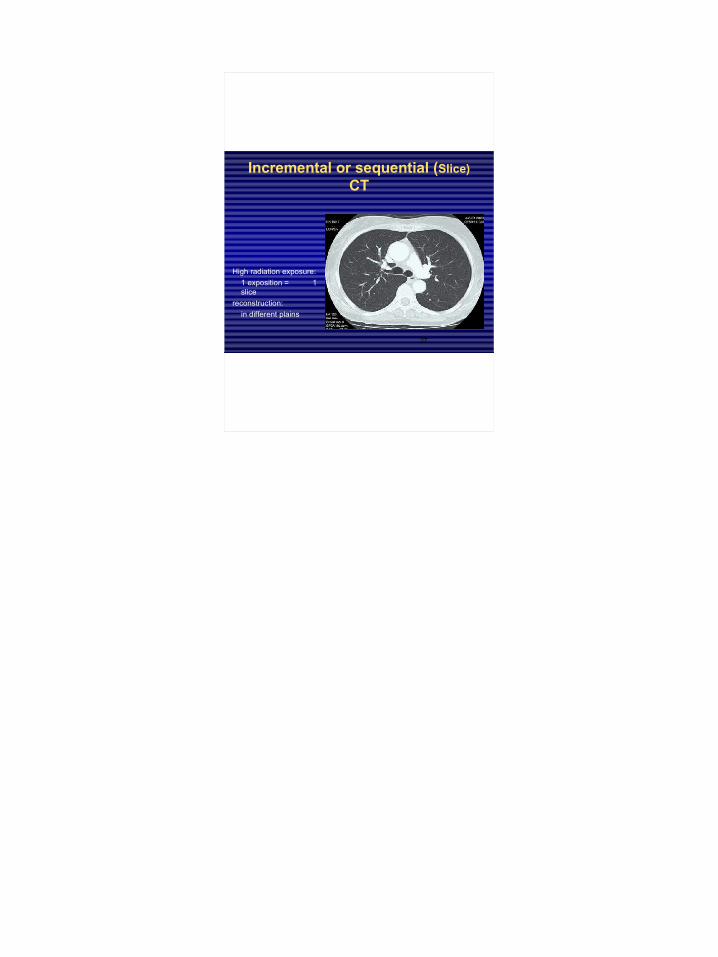
Incremental or sequential (Slice) CT
High radiation exposure:1 exposition = 1 slice
reconstruction: in different plains
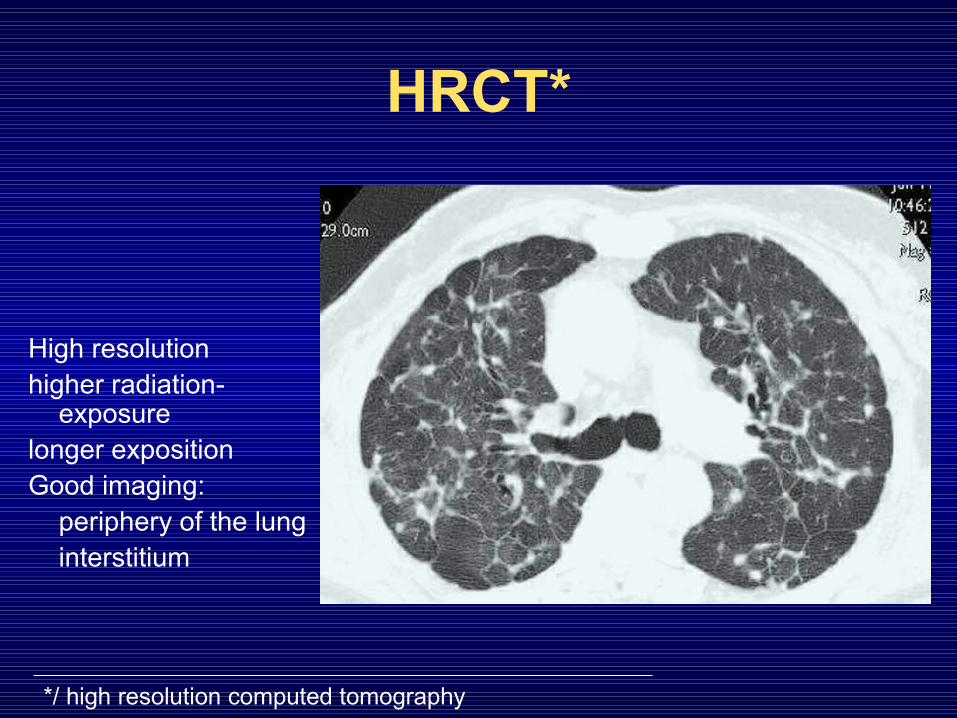
HRCT*
High resolutionhigher radiation-
exposurelonger expositionGood imaging:
periphery of the lunginterstitium
*/ high resolution computed tomography
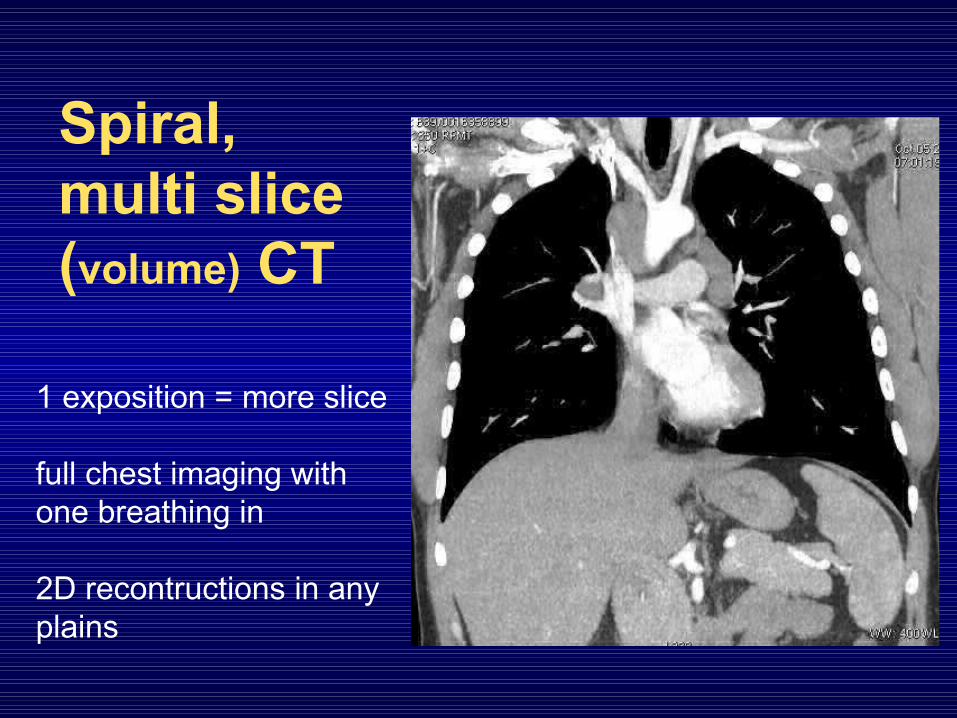
1 exposition = more slice
full chest imaging with one breathing in
2D recontructions in any plains
Spiral, multi slice (volume) CT
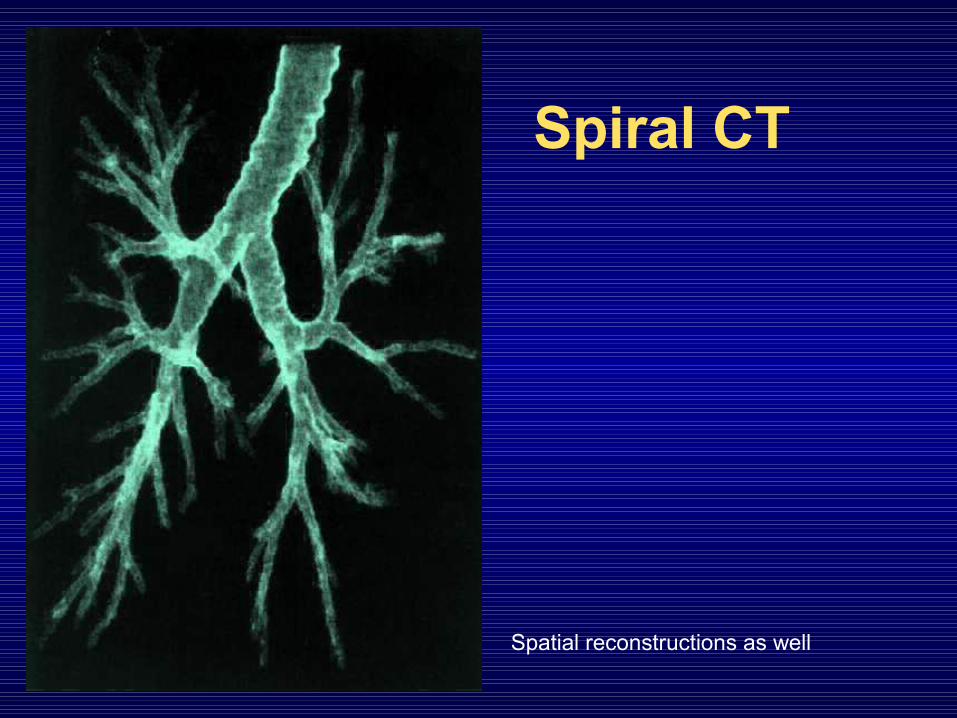
Spiral CT
Spatial reconstructions as well
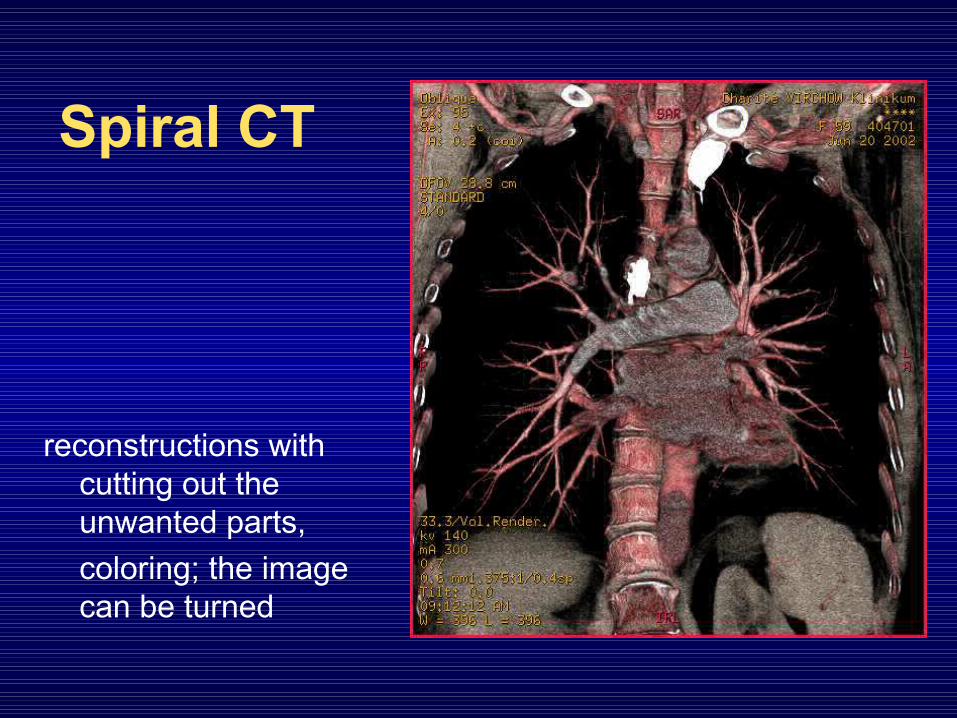
Spiral CT
reconstructions with cutting out the unwanted parts,coloring; the image can be turned

CT-angiography
i. v. iodinated contrast-material
Visualization of the blood vessel lumen
+ parenchymal visualization
3D reconstruction in any plains
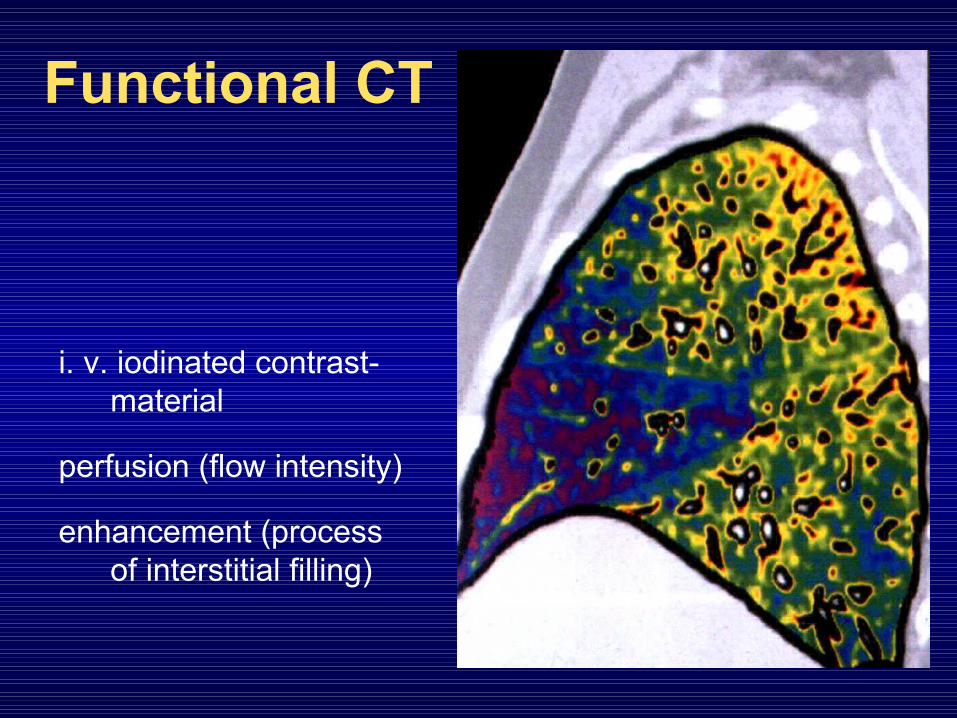
Functional CT
i. v. iodinated contrast-material
perfusion (flow intensity)
enhancement (process of interstitial filling)
Dynamic 3D CT• Visualization of physical borders of structures with
different radiation absorption• It can be evaluated from many angles, can be
rotated as a 3D model
• virtual bronchoscopy:advantage: no injury or infection disadvantage: doesn’t show the actual mucosa, bleeding etc.
Virtual bronchoscopy
Good to know for the indication of a CT scan:
• Radiation exposure of the population mostly arises from the medical applications,
• One CT examination has the radiation exposure equivalent with 400 chest X-rays
Hybrid techniques
• For the visualization of the morphology and function at the same time:
– SPECTCT (Single Photon Emission Tomography)
– PETCT (Positron Emission Tomography)
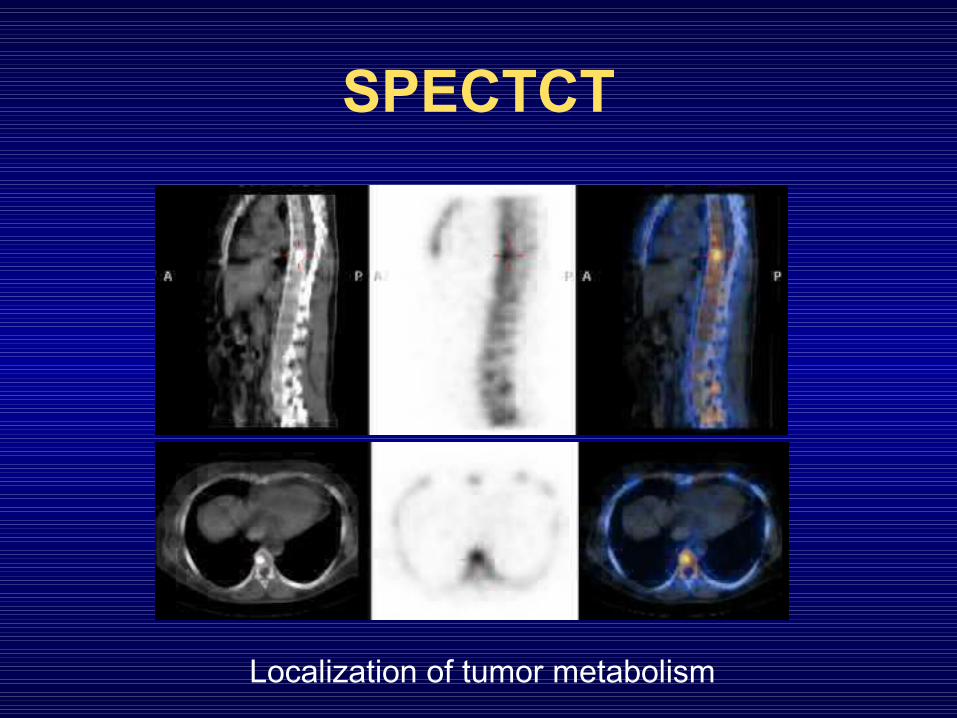
SPECTCT
Localization of tumor metabolism

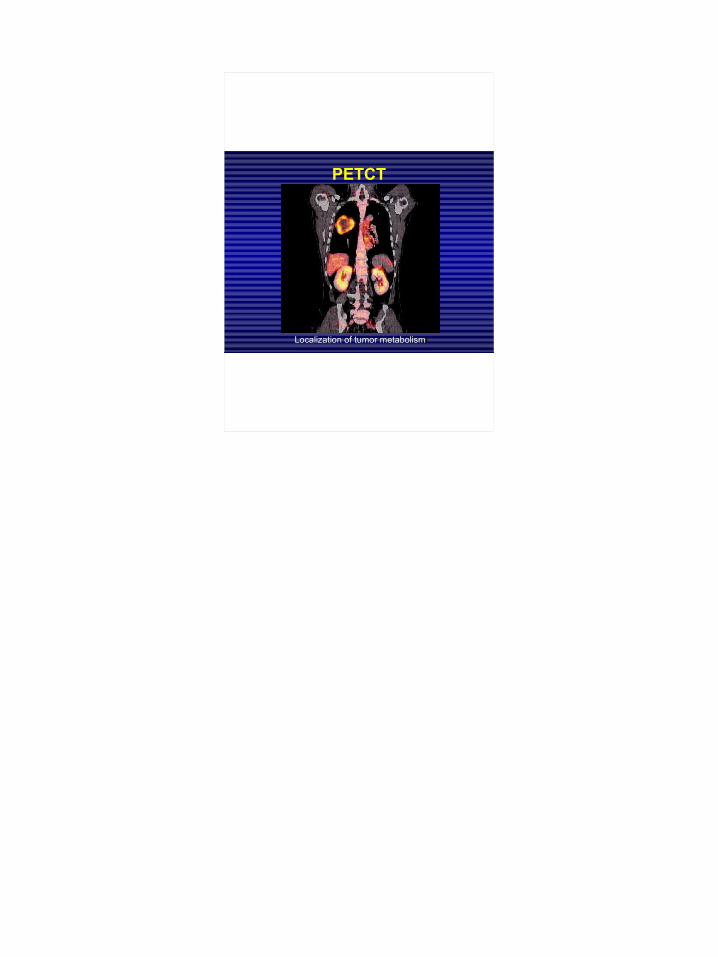
PETCT
Localization of tumor metabolism
MR-examination• Visualizes the proton (H-nuclei) density and their
relation to the surrounding structures• The water and fat are best visualized with this
method• inflammation, edema, and the fat-layers
surrounding the organs are seen• And it shows the distribution of proper contrast-
materials• Because it is sensitive to motions, the circulating
blood can also be evaluated
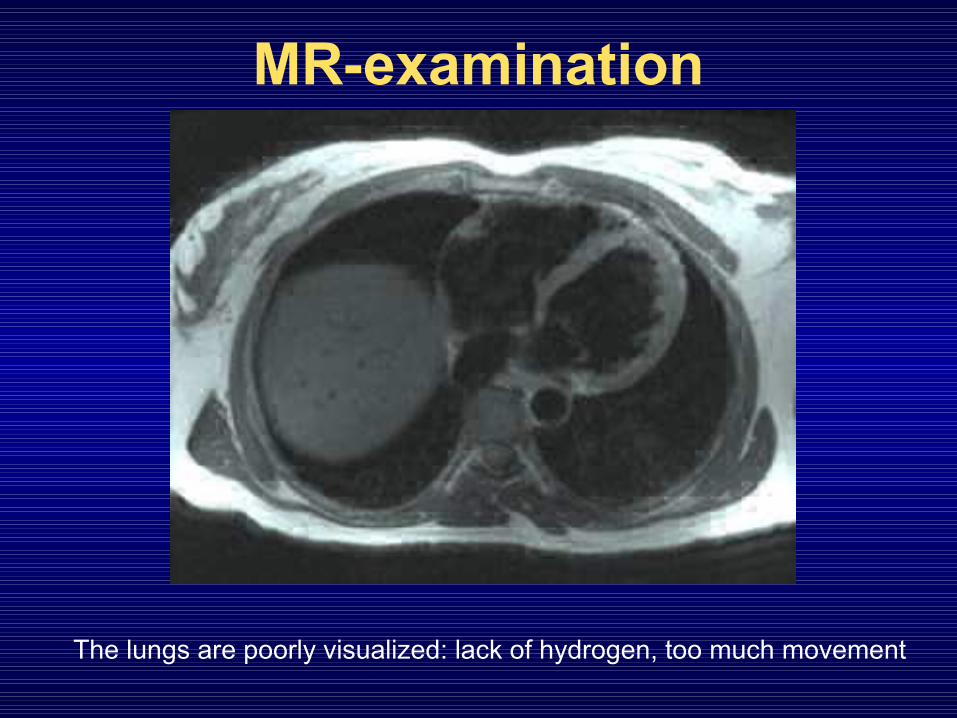
MR-examination
The lungs are poorly visualized: lack of hydrogen, too much movement
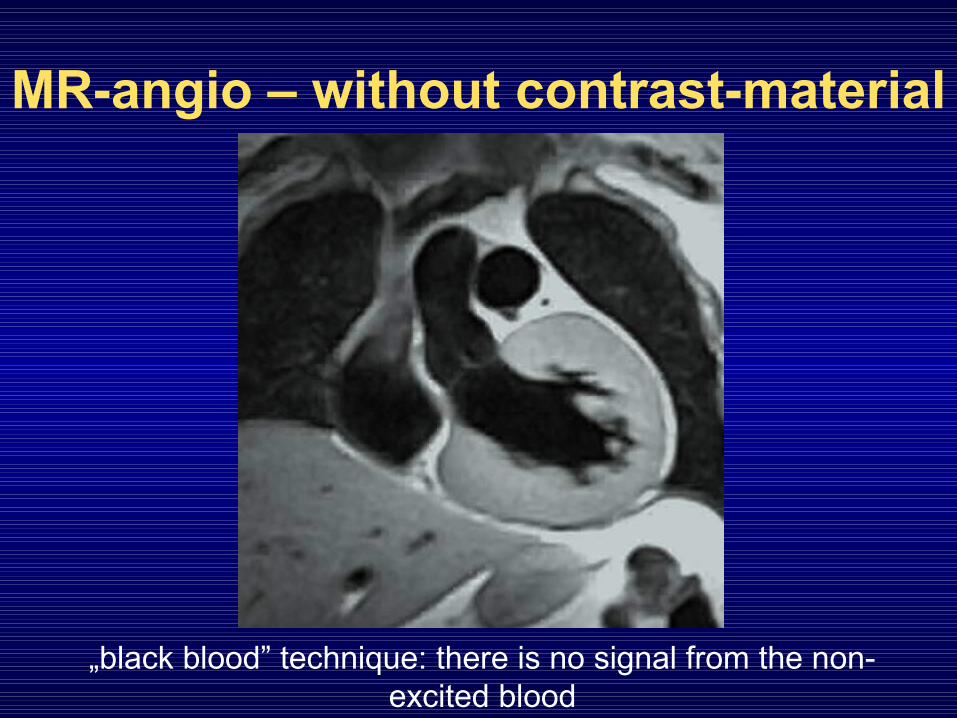
MR-angio – without contrast-material
„black blood” technique: there is no signal from the non-excited blood
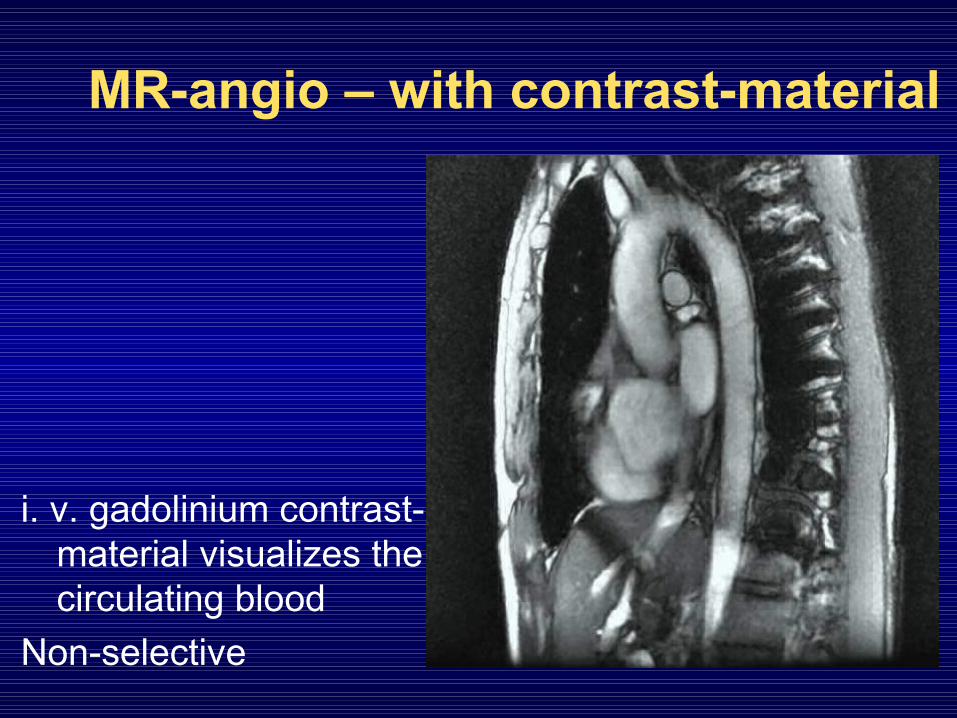
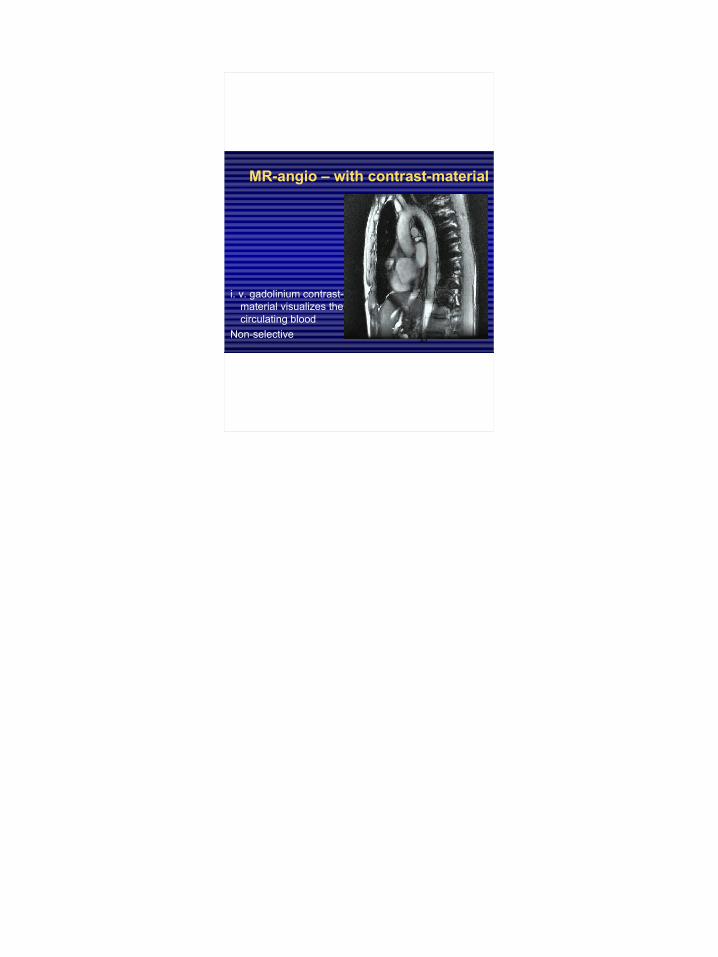
MR-angio – with contrast-material
i. v. gadolinium contrast-material visualizes the circulating blood
Non-selective
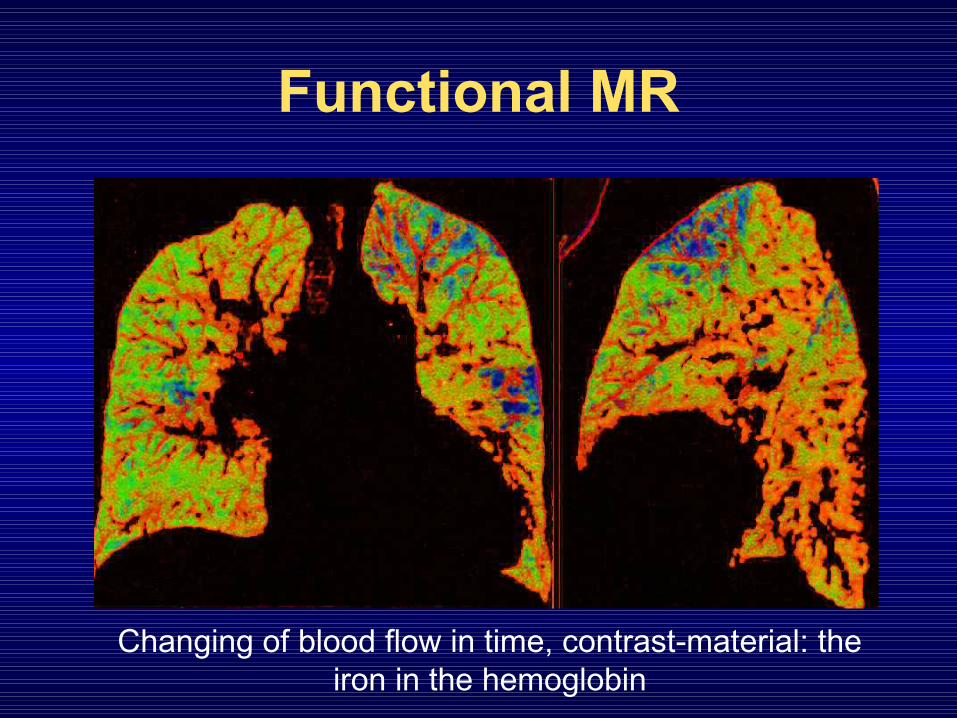
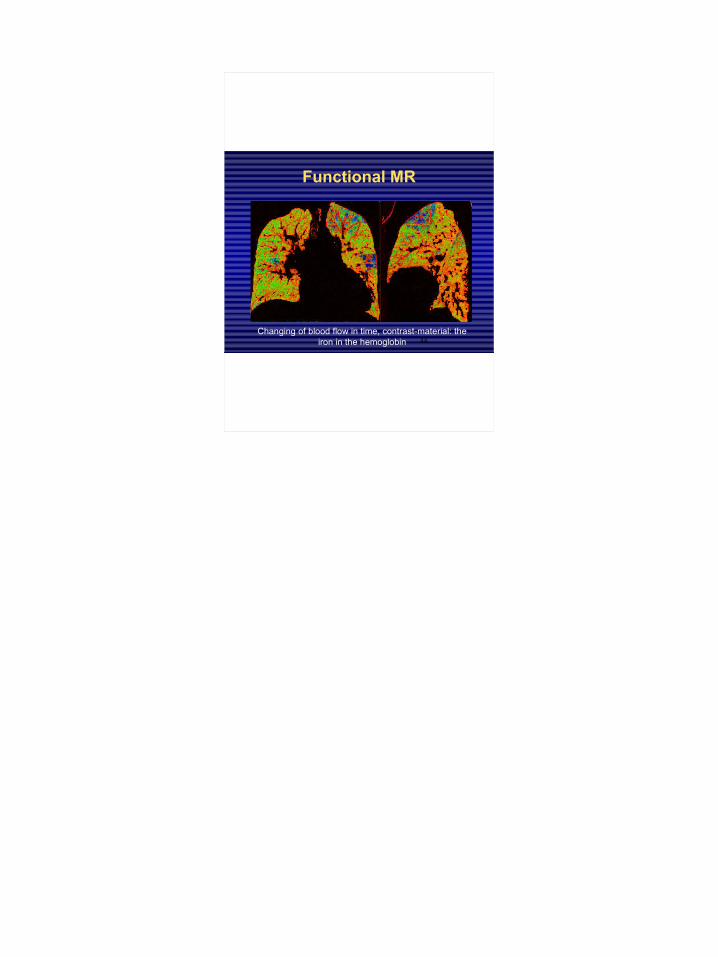
Functional MR
Changing of blood flow in time, contrast-material: the iron in the hemoglobin
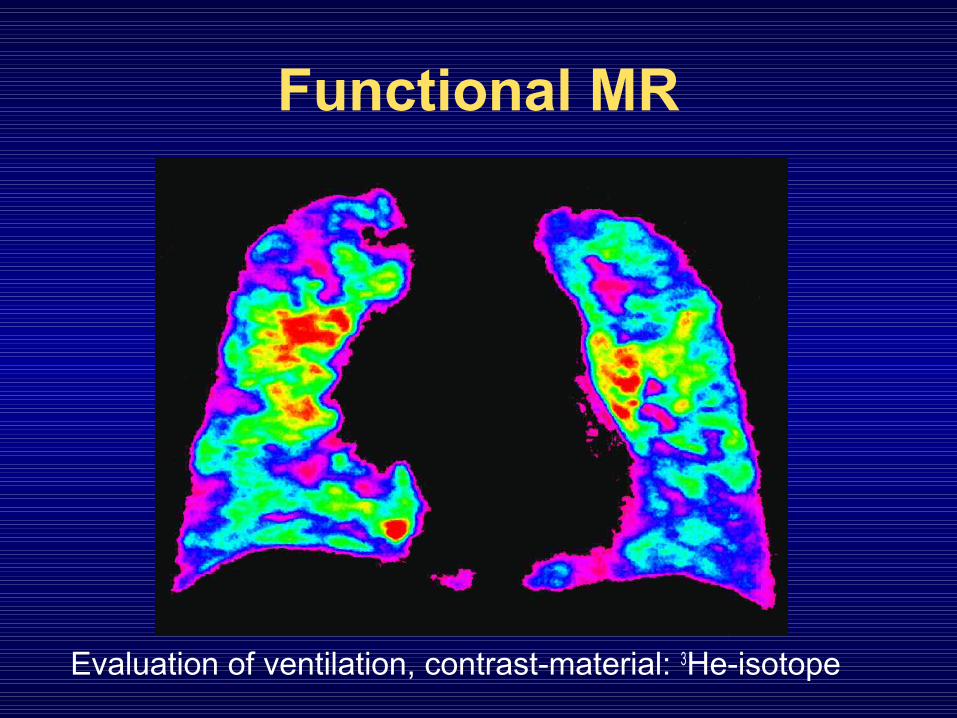
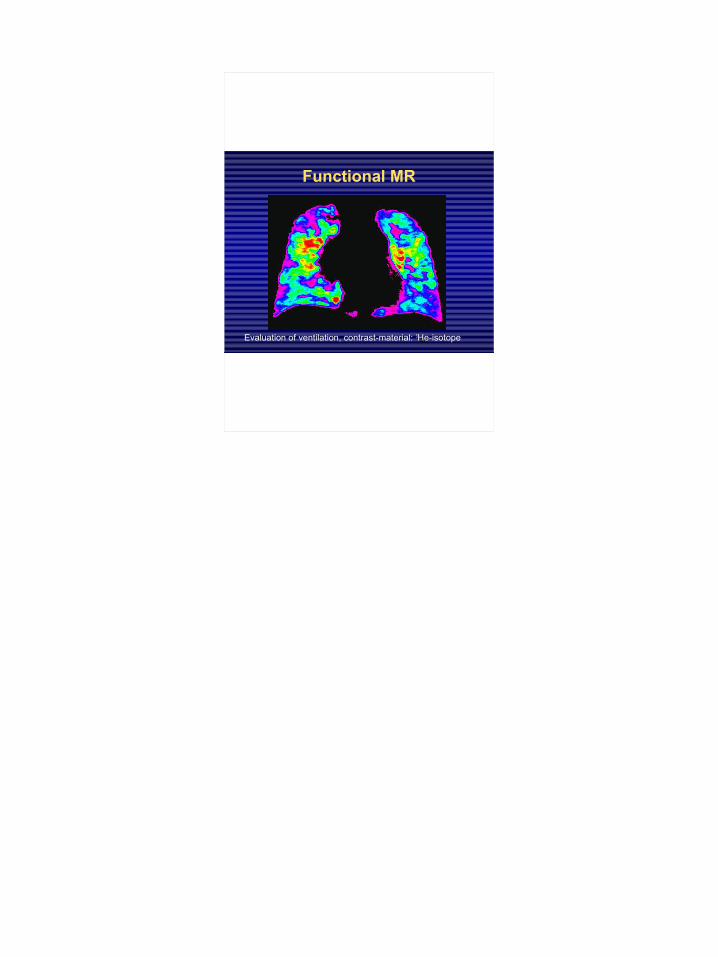
Functional MR
Evaluation of ventilation, contrast-material: 3He-isotope

Radiologic signs of diseases
There is no sign, because the lesion• is too small or too slight• is not radiopaque, reflective enough, or doesn’t
contain enough H• doesn’t provide enough contrast with the
surrounding structures • is moving too fast or too slow• cannot be detected with the given modality

Radiologic signs of diseases
• By radiation absorption:– Enhanced radiation absorption = shadow– Reduced radiation absorption = transparency-enhancement,
enlightenment, negative shadow• By tissue characteristic:
– air (accumulation or diminution)– soft tissue (accumulation or diminution)– fluid (in the interstitium, alveolus, pleural space)
Shadows in the chest X-rays
intrapulmonary:• alveolar • interstitial• Shadow of a vessel• Shadow of a
bronchusextrapulmonary• pleural• extrathoracal
Typical shadows
• As mentioned in the findings:– nodular lesion– infiltration– linear shadow– opacity
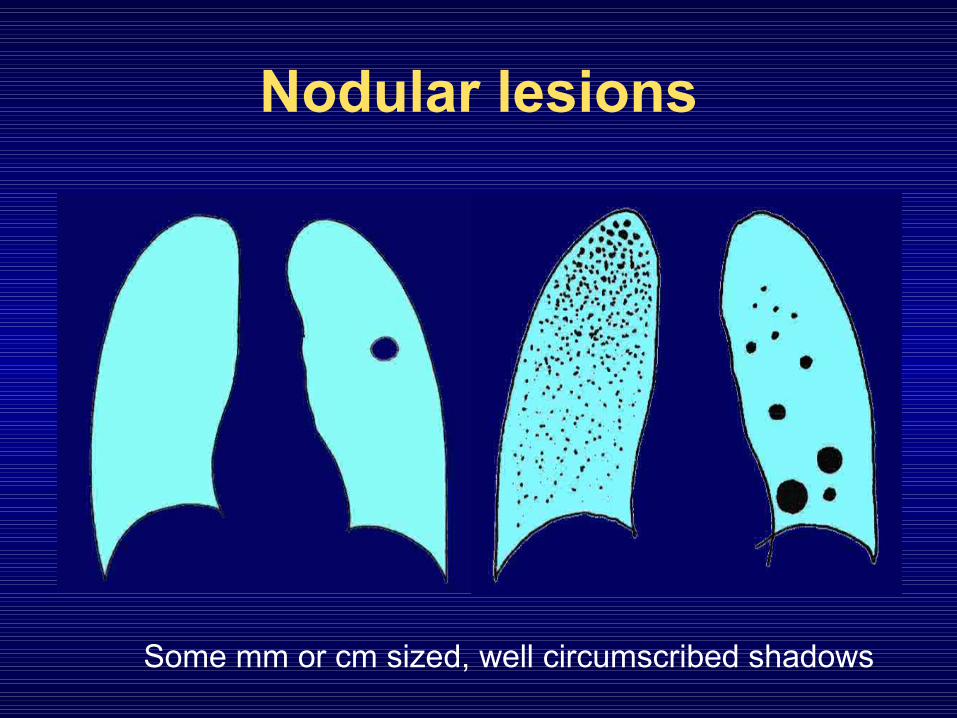
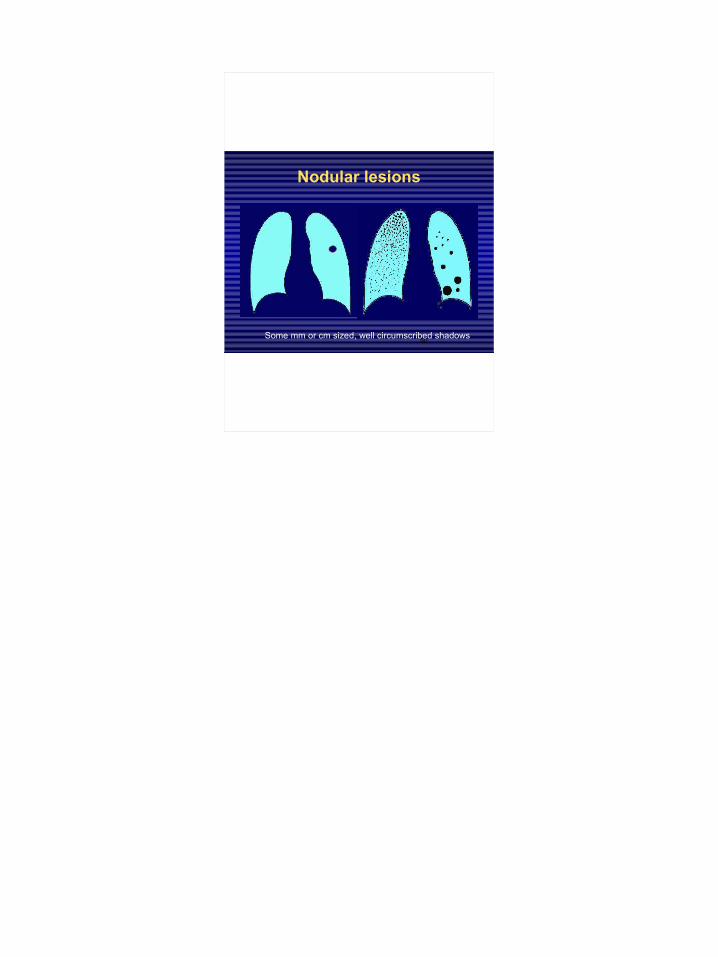
Nodular lesions
Some mm or cm sized, well circumscribed shadows
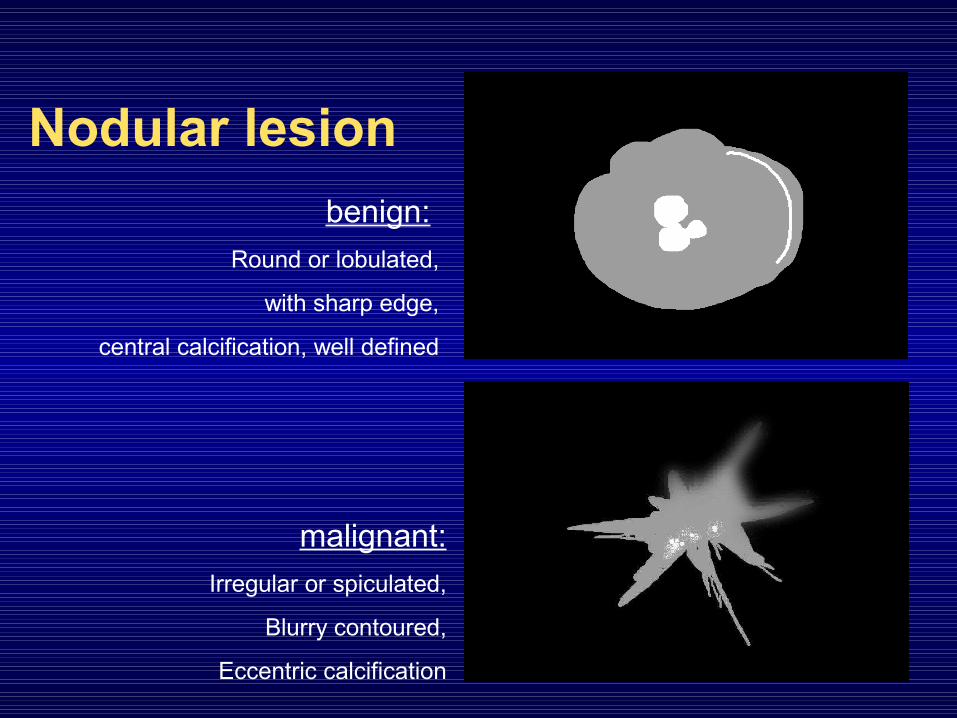
Nodular lesionbenign:
Round or lobulated,
with sharp edge,
central calcification, well defined
malignant:Irregular or spiculated,
Blurry contoured,
Eccentric calcification
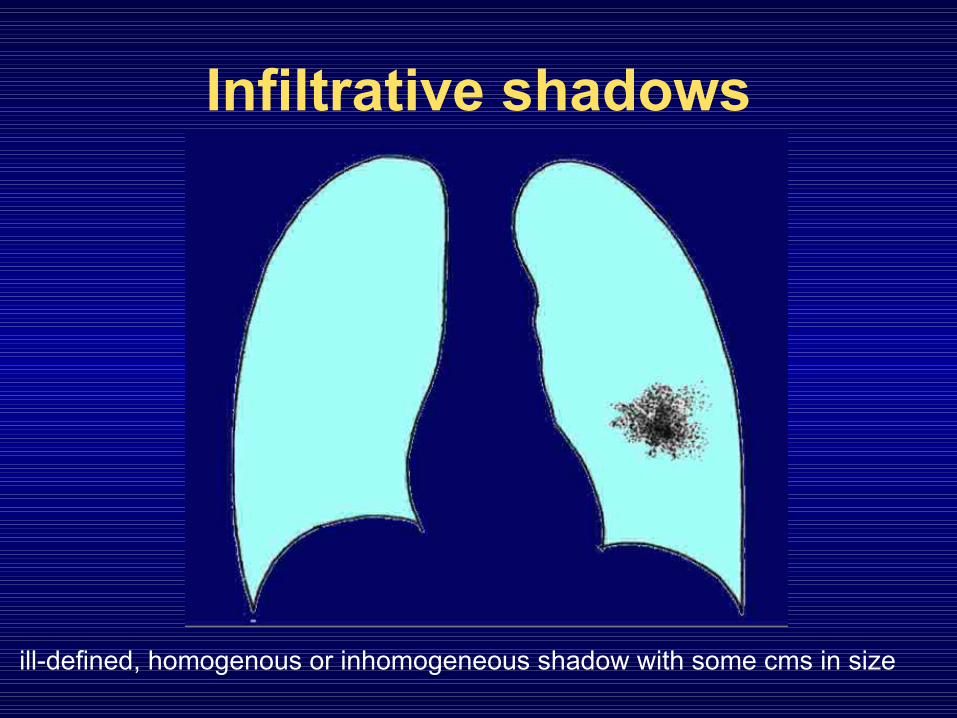
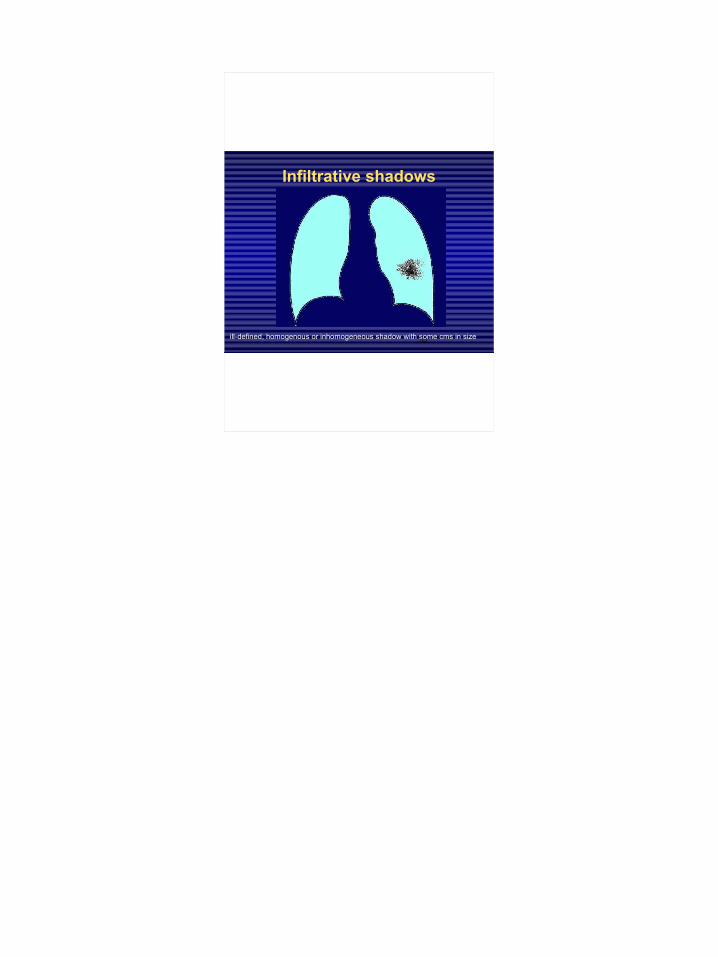
Infiltrative shadows
ill-defined, homogenous or inhomogeneous shadow with some cms in size
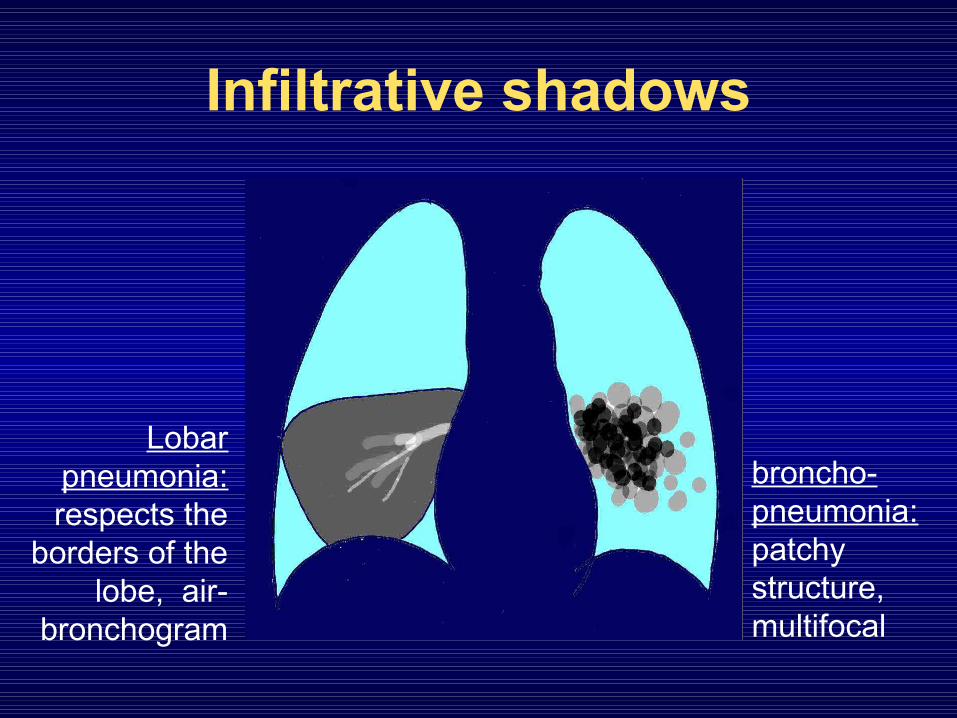
Infiltrative shadows
Lobar pneumonia: respects the
borders of the lobe, air-
bronchogram
broncho-pneumonia: patchy structure, multifocal
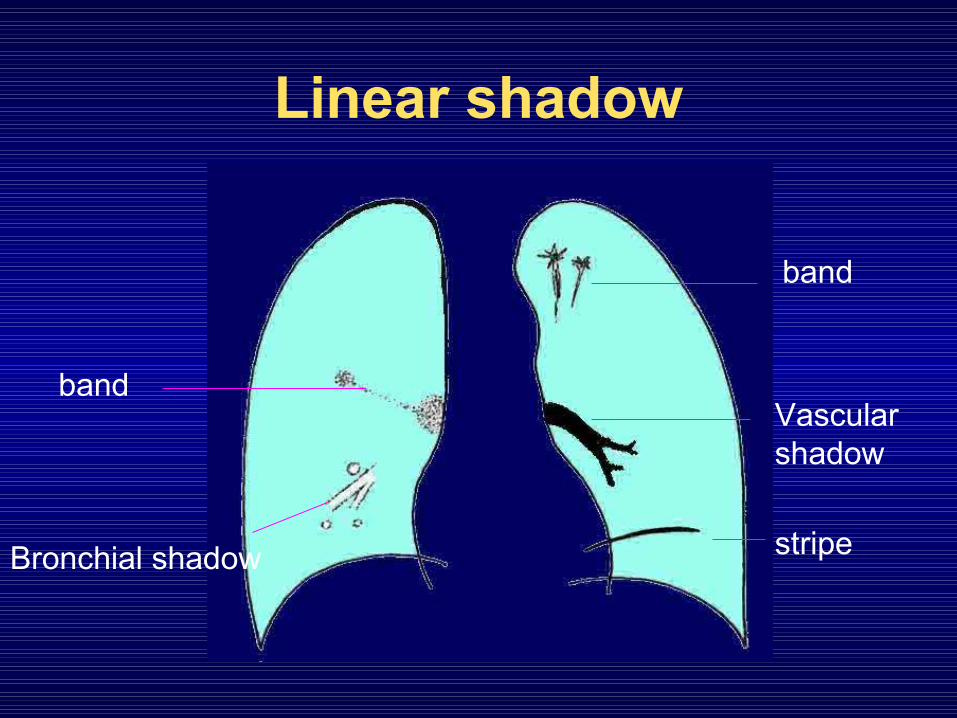
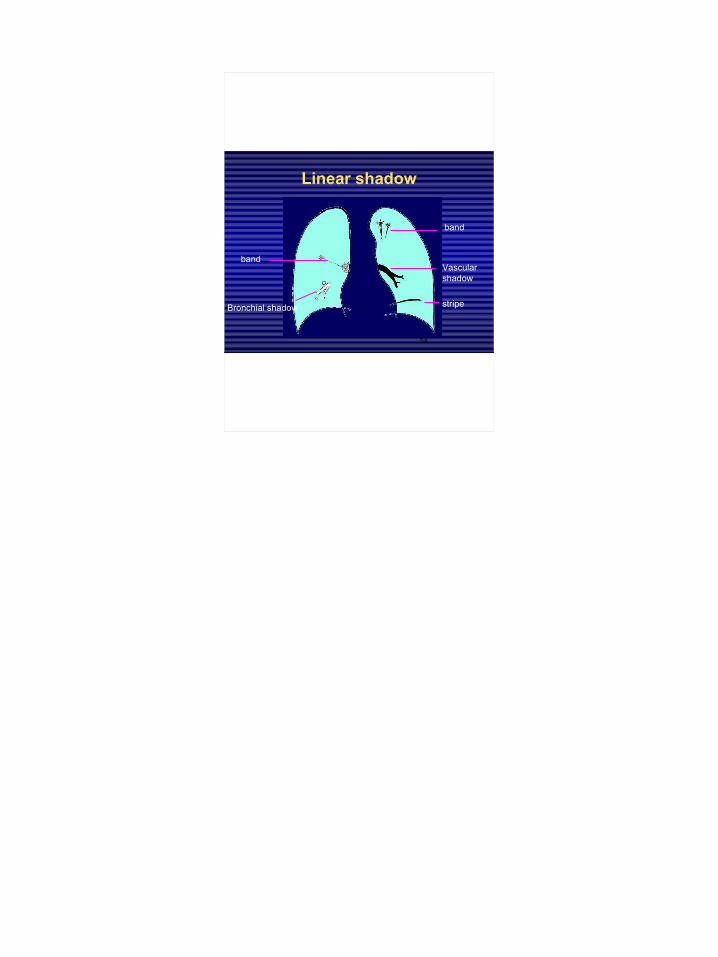
Linear shadow
band
stripe
bandVascular shadow
Bronchial shadow
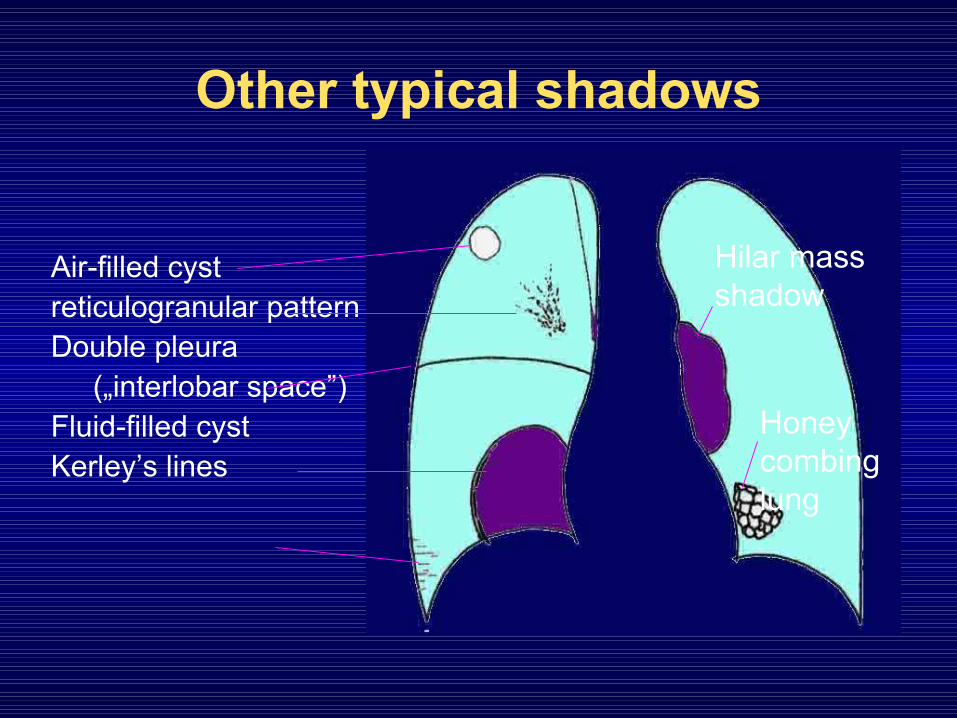
Other typical shadows
Air-filled cystreticulogranular patternDouble pleura
(„interlobar space”)Fluid-filled cystKerley’s lines
Hilar mass shadow
Honey combing lung
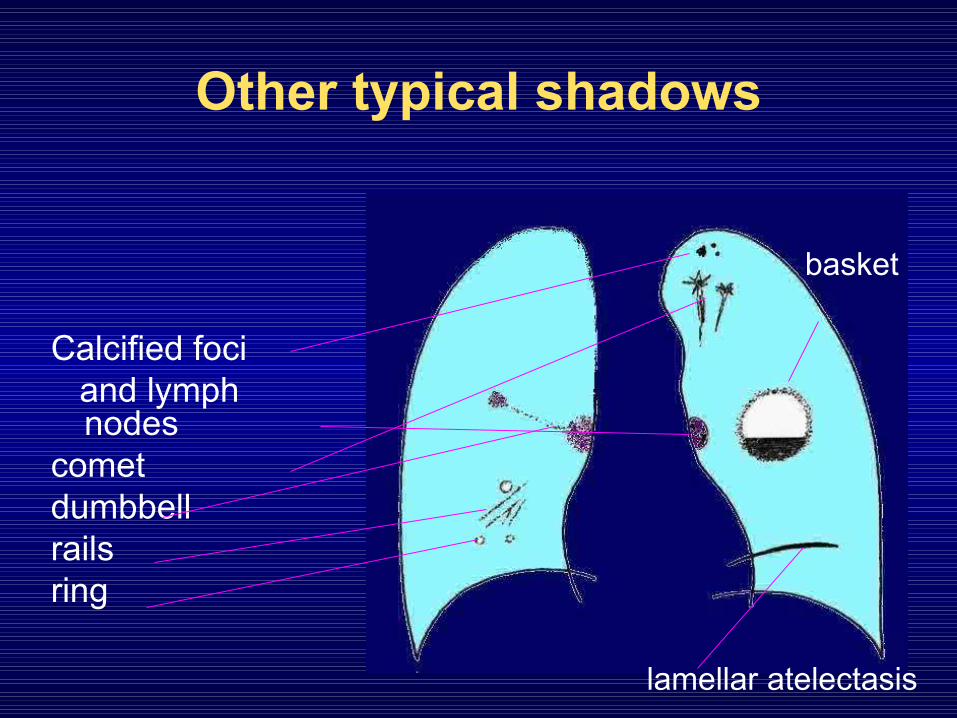
Other typical shadows
Calcified foci and lymph
nodescometdumbbellrailsring
lamellar atelectasis
basket
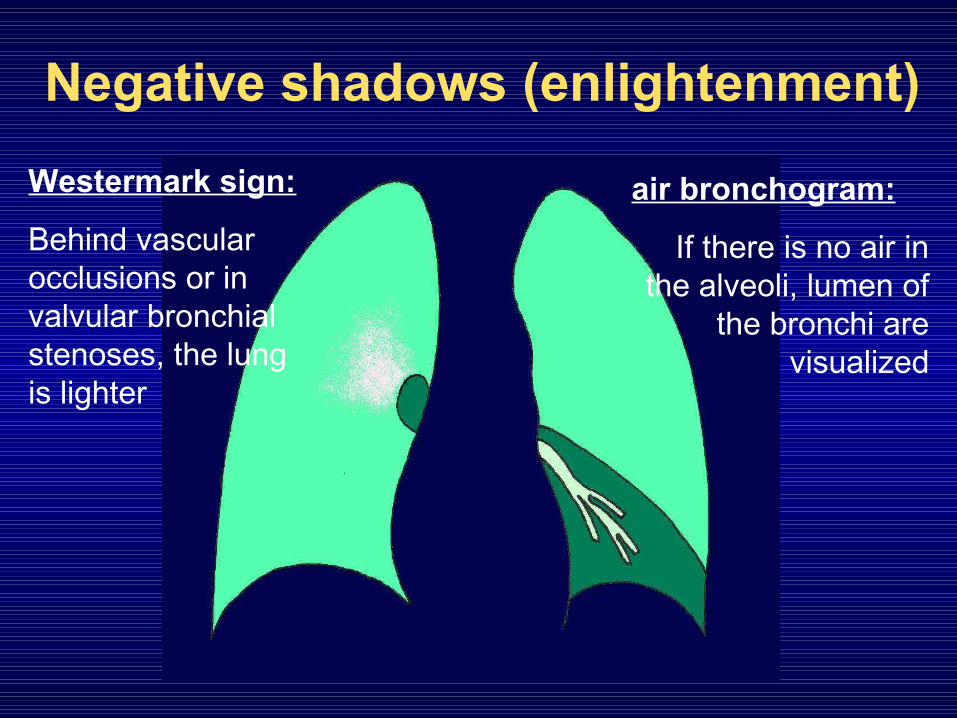
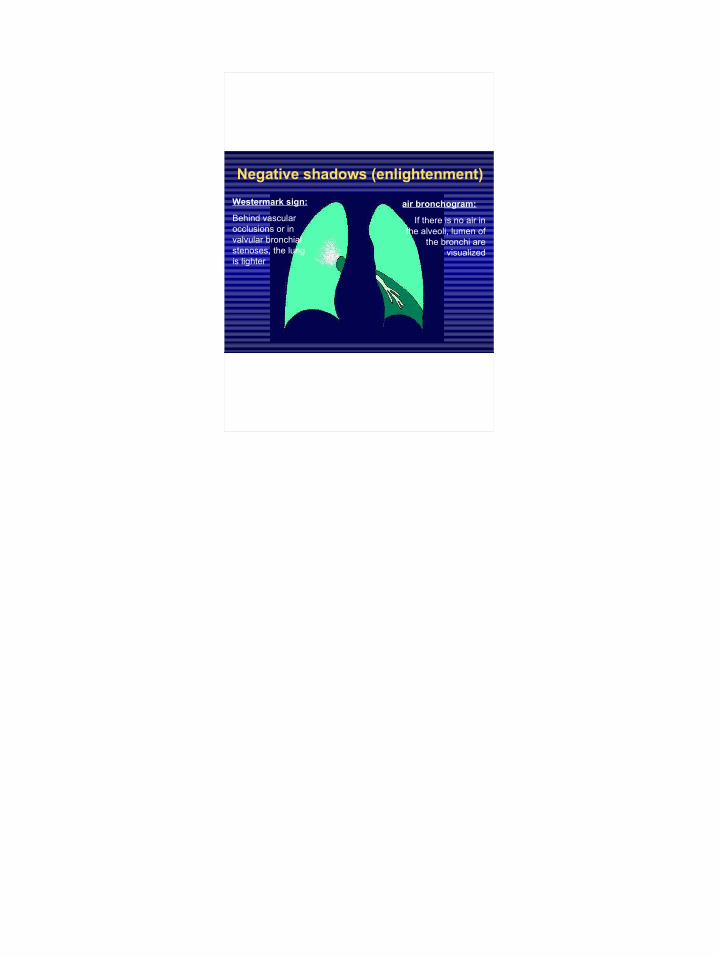
Negative shadows (enlightenment)
air bronchogram:
If there is no air in the alveoli, lumen of
the bronchi are visualized
Westermark sign:
Behind vascular occlusions or in valvular bronchial stenoses, the lung is lighter

Covering, blur
The extrapulmonary shadows won’t make the vascular pattern disappear
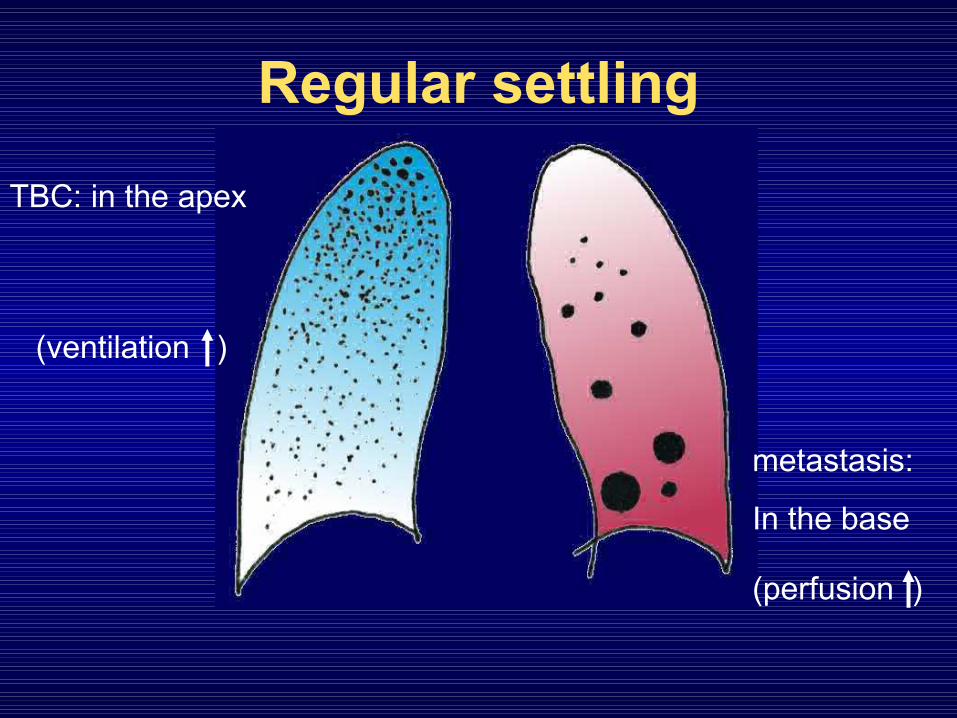
Regular settling
(ventilation )
(perfusion )
TBC: in the apex
metastasis:
In the base
Changing of the volume
• the intrapulmonary inflammation, haemorrhage, or the pleural fluid- or blood accumulation, ptx needs more space than usual
• atelectasis, shrinking processes occupy less space

Inflammation and atelectasis
Volume is increasing Volume is decreasing

Pushing and pulling
fluid accumulation is pushing atelectasis is pulling

Typical shapesFree pleural fluid accumulation
hydro- pneumothorax
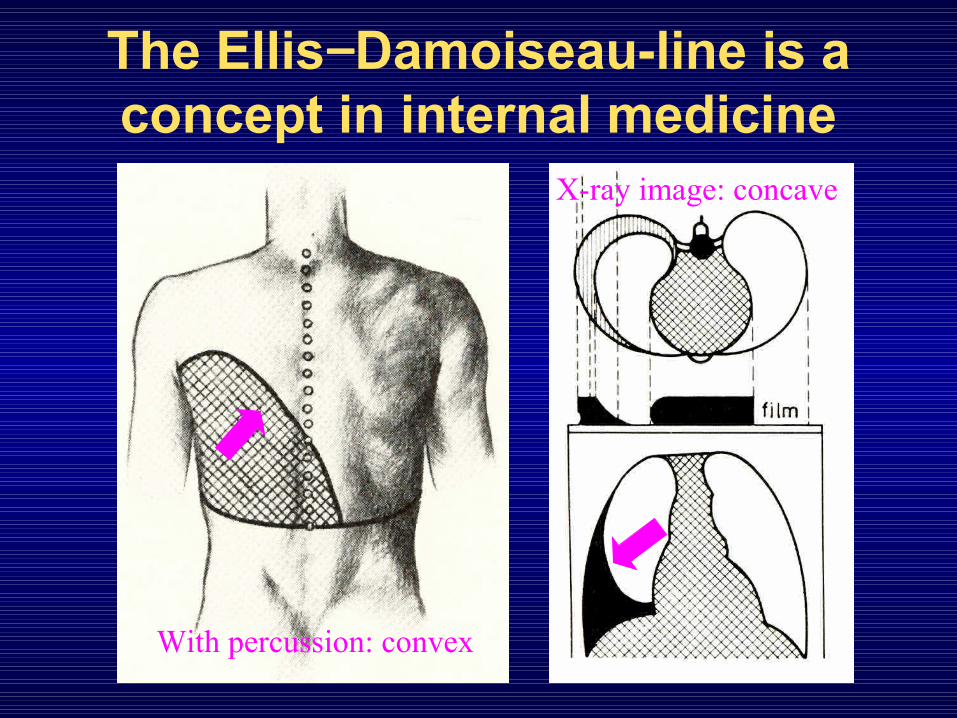
The Ellis−Damoiseau-line is a concept in internal medicine
With percussion: convex
X-ray image: concave
o f T h e o f T h e
f i r s t f i r s t p a r tp a r t

1
Evaluation of the chestEvaluation of the chest
part 1part 1
Nagy EndreNagy Endre
SZEGEDI TUDOMÁNYEGYETEM SZEGEDI TUDOMÁNYEGYETEM ÁOK, RADIOLÓGIAI KLINIKA, ÁOK, RADIOLÓGIAI KLINIKA,
SZEGEDSZEGED
2
Indication
In case of complaints or symptoms:
• In suspicion of lesions, diseases or injuries of the chest organs and
• On the basis of complaints, clinical signs and lab findings
3
Indication
If free of complaints:
• In case of such diseases of distant organs that may cause – even symptomless – lesions of the chest (e.g. metastasis)
4
Indication
For prevention:
• Exclusion of lung and heart diseases before operation and complex anesthesia
• In case of unconsciousness or polytrauma.
5
Indication
In healthy patients:for screening or evaluation of fitness
for work; before settling down or having a job.

6
Limited indication
• Follow-up of previously detected lesions (e.g. pneumonia)
• Thoracal diseases inducing dullness(US instead)
• Supposedly mediastinal lesions (MRI instead)
7
Contraindication
• Only cardiopulmonary resuscitation in progress
• (→ it can be performed in recumbent position or even on an unconscious patient!)
8
Chest X-ray
• Apart from the bones, the air content and blood vessels of the lungs, the hilus and the central shadow (heart and aorta) are evaluated
9
Chest X-ray
• The tiny vessels are visualized because they are surrounded by air
10
For the interpretation of the image it is helpful to know:
• age• sex• physical activity• occupation• smoking, alcohol, drug abuse• clinical data
11
Clinical background presumes
extended shadow in the lung
+ fever → pneumonia+ foreign body aspiration → atelectasis+ difficulty breathing and thrombophlebitis →
infarction+ cough, smoking → cancer+ unconsciousness, vomiting → aspiration+ penetrating injury → hematoma in the lung…
12
Basic examination of the chest
• Two-wiev image: such lesion can be detected on the lateral image that could not be detected on the postero-anterior image
13
Additional X-ray procedures• Fluoroscopy• Oblique images• Images in lateral position• Images in exspiration• fluorography• (conventional tomography)• Digital radiography• „dual energy” technique

14
Fluoroscopy
Visualizes motions and provides spatial information

15
Oblique image
For the evaluation of covered or complex structures
16
Exspiration
For the evaluation of pneumothorax or bronchostenosis

17
Fluorogram
small size analogous or digital picture made directly from the fluoroscope in order to screening
18
(conventional tomography)
• Confusing details can be excluded
19
Digital radiogram
• It provides more equilibrated images – with less radiation exposure
• Possibility of post-processing and simple measurements
20
„Dual energy”-technique
• Elimination of disturbing bone-shadows in the chest that cover 75% of the lungs, with different energy, double exposure and subtraction
Summation image reversed bone-image
21
„Dual energy” technique
After subtraction of the bones, lung components can be evaluated

22
Application of contrast materials
• water-soluble iodinated contrast materials are used• in the bronchi:
– bronchography• blood vessels:
– arteries: pulmonary or bronchial– veins: pulmonary or systemic
23
Bronchography(in pulmonology)• intervention and contrast-
material are needed• for the evaluation of
locations cannot be reached with bronchoscope
• if there is no HRCT
24
Pulmonary arteriography
verification of congenital anomalies, and pulmonary embolism

25
Cavography
digital subtraction angiography: VCS − syndrome
26
Native and contrast enhanced CT
• at first:
– axial images
– without contrast-material
• more precisely:
– reconstruction in different plains
– with iv. water-soluble iodinated contrast-material
27
Incremental or sequential (Slice) CT
High radiation exposure:1 exposition = 1 slice
reconstruction: in different plains

28
HRCT*
High resolutionhigher radiation-
exposurelonger expositionGood imaging:
periphery of the lunginterstitium
*/ high resolution computed tomography

29
1 exposition = more slice
full chest imaging with one breathing in
2D recontructions in any plains
Spiral, multi slice (volume) CT

30
Spiral CT
Spatial reconstructions as well

31
Spiral CT
reconstructions with cutting out the unwanted parts,coloring; the image can be turned

32
CT-angiography
i. v. iodinated contrast-material
Visualization of the blood vessel lumen
+ parenchymal visualization
3D reconstruction in any plains

33
Functional CT
i. v. iodinated contrast-material
perfusion (flow intensity)
enhancement (process of interstitial filling)

34
Dynamic 3D CT• Visualization of physical borders of structures with
different radiation absorption• It can be evaluated from many angles, can be
rotated as a 3D model
• virtual bronchoscopy:advantage: no injury or infection disadvantage: doesn’t show the actual mucosa, bleeding etc.
35
Virtual bronchoscopy

36
Good to know for the indication of a CT scan:
• Radiation exposure of the population mostly arises from the medical applications,
• One CT examination has the radiation exposure equivalent with 400 chest X-rays

37
Hybrid techniques
• For the visualization of the morphology and function at the same time:
– SPECTCT (Single Photon Emission Tomography)
– PETCT (Positron Emission Tomography)

38
SPECTCT
Localization of tumor metabolism
39
PETCT
Localization of tumor metabolism
40
MR-examination• Visualizes the proton (H-nuclei) density and their
relation to the surrounding structures• The water and fat are best visualized with this
method• inflammation, edema, and the fat-layers
surrounding the organs are seen• And it shows the distribution of proper contrast-
materials• Because it is sensitive to motions, the circulating
blood can also be evaluated

41
MR-examination
The lungs are poorly visualized: lack of hydrogen, too much movement

42
MR-angio – without contrast-material
„black blood” technique: there is no signal from the non-excited blood
43
MR-angio – with contrast-material
i. v. gadolinium contrast-material visualizes the circulating blood
Non-selective
44
Functional MR
Changing of blood flow in time, contrast-material: the iron in the hemoglobin
45
Functional MR
Evaluation of ventilation, contrast-material: 3He-isotope

46
Radiologic signs of diseases
There is no sign, because the lesion• is too small or too slight• is not radiopaque, reflective enough, or doesn’t
contain enough H• doesn’t provide enough contrast with the
surrounding structures • is moving too fast or too slow• cannot be detected with the given modality
47
Radiologic signs of diseases
• By radiation absorption:– Enhanced radiation absorption = shadow– Reduced radiation absorption = transparency-enhancement,
enlightenment, negative shadow• By tissue characteristic:
– air (accumulation or diminution)– soft tissue (accumulation or diminution)– fluid (in the interstitium, alveolus, pleural space)
48
Shadows in the chest X-rays
intrapulmonary:• alveolar • interstitial• Shadow of a vessel• Shadow of a
bronchusextrapulmonary• pleural• extrathoracal
49
Typical shadows
• As mentioned in the findings:– nodular lesion– infiltration– linear shadow– opacity
50
Nodular lesions
Some mm or cm sized, well circumscribed shadows

51
Nodular lesionbenign:
Round or lobulated,
with sharp edge,
central calcification, well defined
malignant:Irregular or spiculated,
Blurry contoured,
Eccentric calcification
52
Infiltrative shadows
ill-defined, homogenous or inhomogeneous shadow with some cms in size

53
Infiltrative shadows
Lobar pneumonia: respects the
borders of the lobe, air-
bronchogram
broncho-pneumonia: patchy structure, multifocal
54
Linear shadow
band
stripe
bandVascular shadow
Bronchial shadow

55
Other typical shadows
Air-filled cystreticulogranular patternDouble pleura
(„interlobar space”)Fluid-filled cystKerley’s lines
Hilar mass shadow
Honey combing lung

56
Other typical shadows
Calcified foci and lymph
nodescometdumbbellrailsring
lamellar atelectasis
basket
57
Negative shadows (enlightenment)
air bronchogram:
If there is no air in the alveoli, lumen of
the bronchi are visualized
Westermark sign:
Behind vascular occlusions or in valvular bronchial stenoses, the lung is lighter
58
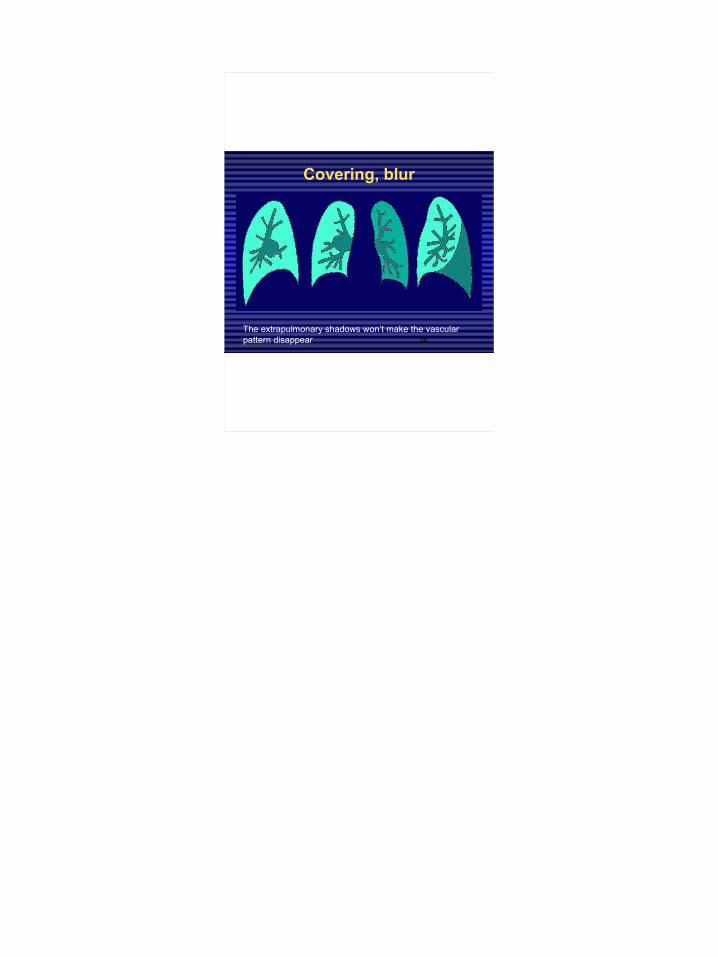
Covering, blur
The extrapulmonary shadows won’t make the vascular pattern disappear

59
Regular settling
(ventilation )
(perfusion )
TBC: in the apex
metastasis:
In the base
60
Changing of the volume
• the intrapulmonary inflammation, haemorrhage, or the pleural fluid- or blood accumulation, ptx needs more space than usual
• atelectasis, shrinking processes occupy less space
61
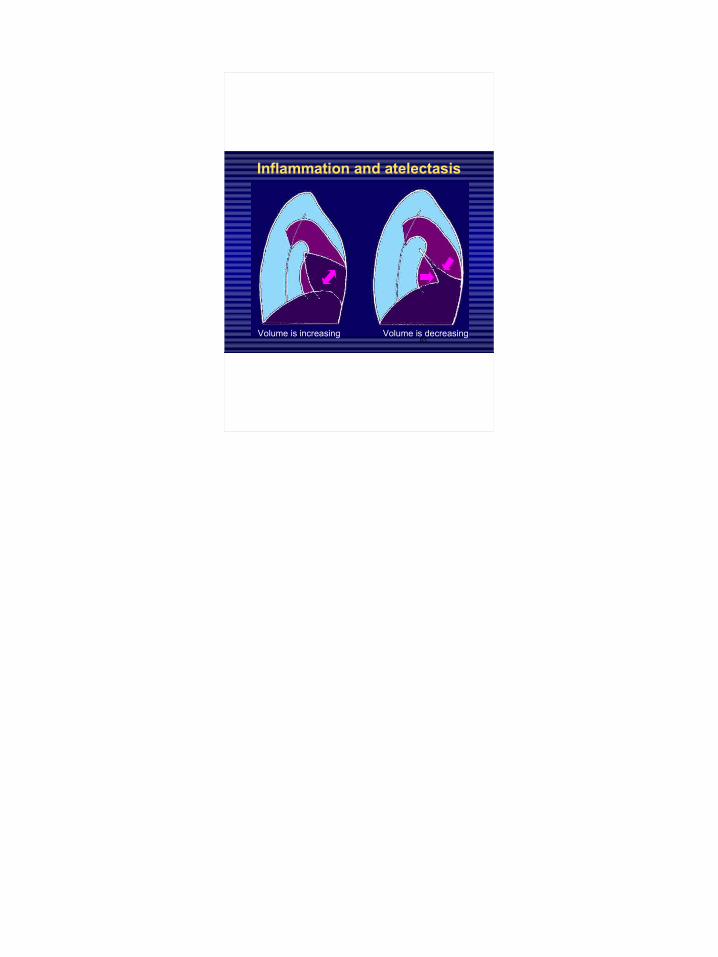
Inflammation and atelectasis
Volume is increasing Volume is decreasing

62
Pushing and pulling
fluid accumulation is pushing atelectasis is pulling
63
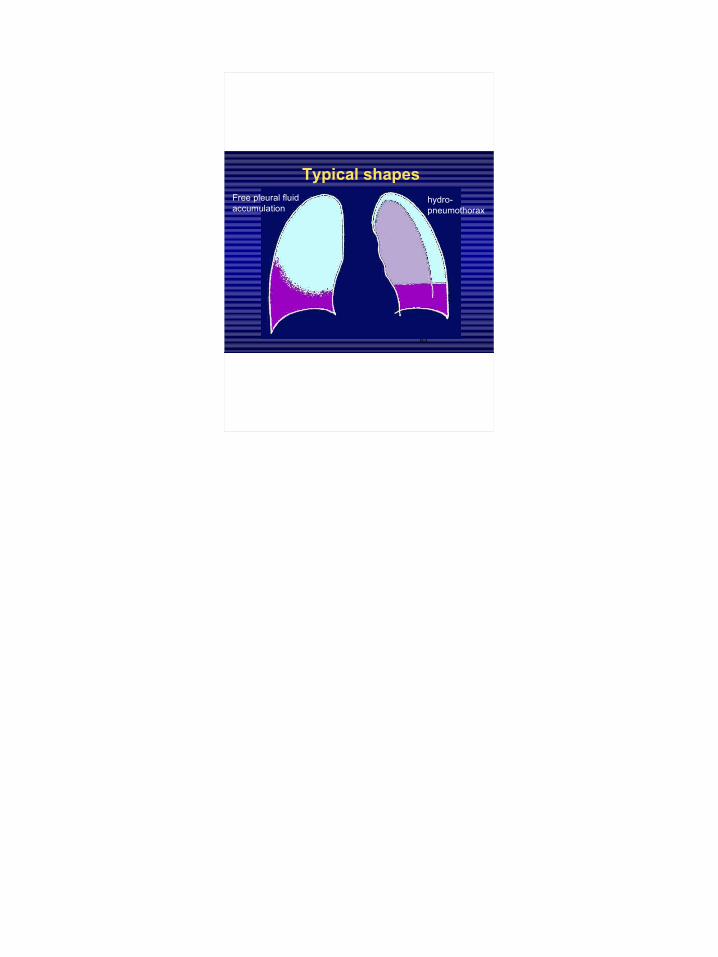
Typical shapesFree pleural fluid accumulation
hydro- pneumothorax

64
The Ellis−Damoiseau-line is a concept in internal medicine
With percussion: convex
X-ray image: concave

65o f T h e o f T h e
f i r s t f i r s t p a r tp a r t







