
Current and future burden
of HCV infection
in Russia
St. Petersburg, 05 May, 2015
Olga Sagalova
Clinic of South Ural State Medical University of
Ministry of Healthcare of Russian Federation
1

Disclosures
• Consultant: MSD, Gilead
• Sponsored Lectures (National or International): BMS,
MSD, Janssen, AbbVie, Gilead
2

Current Disease Burden
-Gower, E., et al., Global epidemiology and genotype distribution of the hepatitis C virus, J Hepatol (2014)
Prevalence(Viremic)
0.0%-0.6%
0.6%-0.8%
0.8%-1.3%
1.3%-2.9%
2.9%-7.8%
Total Infected (Viremic)
200K-650K
650K-1.9M
0-200K
1.9M-3.5M
3.5M-9.2M
3

Current Disease Burden
• The number of chronic HCV cases per 100,000 increased from
12.9 in 1999 to a peak of 40.9 in 2009. In 2012 there were 39.1
cases per 100,000 individuals (1)
1Viral hepatitis in Russian Federation. Analytical review. 9 ed. 2013; 113.
4
0
5
10
15
20
25
30
35
40
45
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
ХГС
12.9
39.4
pe
r 1
00
00
0
39.1

Current Disease Burden
2010 anti-HCV Prevalence Total Cases
Russia 4.10% 5,861,500
2010 Viremic Prevalence Total Viremic Cases
Russia 2.91% 4,161,700
• The estimate for anrti-HCV prevalence in the general Russian
population derives from a general consensus of 4.1% in 2010, reported
in multiple sources (VHPB 2011, Lavanchy 2011, Pimenov 2012)
• Applying a viremic rate of 71% (Iashina 1993), the viremic prevalence in
2010 was estimated at 2.9%, corresponding to 4.2 million infections
-Viral Hepatitis Prevention Board. Russia: Burden of disease. January 2011.
http://www.vhpb.org/files/html/Meetings_and_publications/Viral_Hepatitis_Newsletters/vhv19n1.pdf
-Lavanchy D. Evolving epidemiology of hepatitis C virus. Clin Microbiol Infec 2011 Feb; 17(2):107-15.
-Pimenov NN, Vdovin AV, Komarova SV, Mamonova NA, Chulanov VP, Pokrovskii VI. [The relevance and prospeсts of introducing a uniform federal register
of patients with viral hepatitis B and C in Russia.] Ter Arkh 2012; 85(11):4-9.
-Iashina TL, Favorov MO, Shakhgil'dian IV, Iarasheva DM, Nazarova OI, Derevianko EN, Ommadova MI, Onishchenko GG, Watanabe Y, Nishioka K. [The
spread of hepatitis C markers among the population of regions of Russia and Central Asia]. Zh Mikrobiol Epidemiol Immunobiol 1993 September;(5):46-9.
5

Current Disease Burden
-Pimenov N.N, Chulanov V.P., Komarova S.V. et al. [Hepatitis C in Russia: current epidemiology and approaches to improving diagnosis and surveillance].
Epidemiology and Infectious Diseases, 2012; (4):4-10.
Prevalence Age and Gender Distribution
• The age and gender distribution was developed using the
age distribution and gender ratio of infection as presented in
Pimenov et al (2012)
6

Current Disease Burden
Genotype Distribution
• The genotype distribution was developed using data from
regional registries of more than 40,000 patients with chronic viral
hepatitis (Pimenov et al. 2012)
• G1: 54.9%
‒ G1a: 2.1%
‒ G1b: 52.8%
• G2: 8.1%
• G3: 36.3%
• Other: 0.7%
-Pimenov N.N, Chulanov V.P., Komarova S.V. et al. [Hepatitis C in Russia: current epidemiology and approaches to improving diagnosis and surveillance].
Epidemiology and Infectious Diseases, 2012; (4):4-10.
7
52,8%
8,1%
36,3%
1a
1b
2a
3a

39%
25%
16%
9%
11%
F0
F1
F2
F3
F4
Federal register of patients with viral hepatitis (2014)
n=9851
F0-F1 64%
F2-F4 36%
Distribution of fibrosis
Current Disease Burden
8

Current Disease Burden
Diagnosed
• According to the National Reference Center for Viral Hepatitis
the number of previously diagnosed (viremic) in 2012
was1,789,500 individuals
• The number of newly diagnosed (viremic) in 2012 was 55,900
patients (National Reference Center for Viral Hepatitis)
• According to an analysis of regional registries conducted by the
Russian National Reference Center for Viral Hepatitis,
approximately 43% of the infected population in 2012 had
received anti-HCV testing
9

Current Disease Burden
Treated Patients
• 2011: 5,500 patients were on treatment (regional registries),
corresponding to a 0.1% treatment rate
Year 2004 2005 2006 2007 2008 2009 2010
2011-
2030
Tx Pts 666 1,662 2,254 3,010 2,735 3,807 5,500 5,500
10

Current Disease Burden
Incidence
• Using the known number of total HCV infections in 2010, a
mathematical model was used to calculate the annual number of
all-cause mortality, liver-related deaths and cured cases as
described by Razavi et al. According to this calculation, there
were an estimated 236,000 new cases of HCV in Russia in 2013
- Razavi H, Waked I, Sarrazin C, et al. The present and future disease burden of hepatitis C virus (HCV) infection with today's treatment paradigm. J Viral Hepat
2014; 21 Suppl 1: 34-59
11

Current Disease Burden
• A progression model constructed to quantify the size of the
HCV infected population, by stages of liver disease until 2030
-Razavi H, et al. J Viral Hepat. 2014;Suppl 1:34-59;
12
Количество в 2013
Total ~ 4 500 000
Treated 5 500
Compensated cirrhosis ~ 145 500
Decompensated cirrhosis ~ 17 000
HCC ~ 5 000
Total living with the diagnosis ~ 1 800 000
Annual newly diagnosed 55 900

Future Disease Burden Continue Current Treatment Program
0
1 000 000
2 000 000
3 000 000
4 000 000
5 000 000
6 000 000
7 000 000
2013 2030
Total Infected
0
5 000
10 000
15 000
20 000
2013 2030
LRD
0
10 000
20 000
30 000
40 000
50 000
60 000
2013 2030
Decompensated Cirrhosis
0
5 000
10 000
15 000
20 000
2013 2030
HCC
13
2013 2030
Treated (annual) 5,500
SVR by Genotype (G)G1 50% and G4 and
75% G2 and 60% G3%
Impact
# Total infected 4,525,000 6,164,000
% change +36%
# Liver-related deaths 5,110 16,100
% Change +215%
# Decompensated
cirrhosis 17,140 52,000
% change +203%
# HCC 5,170 16,530
% change +220%

Future Disease Burden Can we control the disease? What needs be done?
0
20 000
40 000
60 000
80 000
100 000
120 000
140 000
201
32
01
62
01
72
01
92
02
22
02
5
Treated
0
100 000
200 000
300 000
400 000
500 000
600 000
700 000
201
32
01
62
01
72
01
92
02
22
02
5
Newly diagnosed
0
50 000
100 000
150 000
200 000
250 000
201
3
201
6
201
7
201
9
202
2
202
5
New infections
• 40% reduction in viremic individuals
by 2030
• 68% drop in HCV-related mortality by
2030
• We need to:
– Increase annual number
of treated patients to 123,800 with
high SVR therapies
– Increase diagnosed
patients accordingly
– Reduce new infections by 20%
annually starting in 2017
14

Future Disease Burden Impact of Disease Control Strategy
4 500 000
6 200 000
3 700 000
01 000 0002 000 0003 000 0004 000 0005 000 0006 000 0007 000 000
Today 2030CurrentStrategy
2030ControlStrategy
Total Infected
-40%
150 000
400 000
100 000
0100 000200 000300 000400 000500 000
Today 2030CurrentStrategy
2030ControlStrategy
# Compensated Cirrhosis
-75%
Impact
# Total infected 4,500,000 6,200,000 3,700,000
Change (%) +27% -40%
Today
2030
Current Strategy
Control Strategy
Treated (Annual) 5,500 5,500 123,800
Treatment rate 0.1% 0.1% 3%
SVR by genotype
G1 50% and
G4 and 75%
G2 and 60%
G3%
G1 50% and
G4 and 75%
G2 and 60%
G3%
90% for all genotypes
Total diagnosed 1,800,000 2,200,000 4,100,000
Common treatment age 15 - 64 15- 64 15-69Treated Stages ≥ F1 ≥ F1 ≥ F2
# Compensated cirrhosis 150,000 400,000 100,000
Change (%) +63% -75%
15

• Adopting this scenario will result in 2,490,000 fewer viremic
individuals in 2030 vs the base case, a 40% reduction
• Between 2015 and 2030
– 1,610,000 new infections avoided
– 67,000 HCV-related mortalities prevented
– 1,500,000 patients cured
– 300,000 cirrhotic cases averted
Future Disease Burden Impact of Disease Control Strategy
16
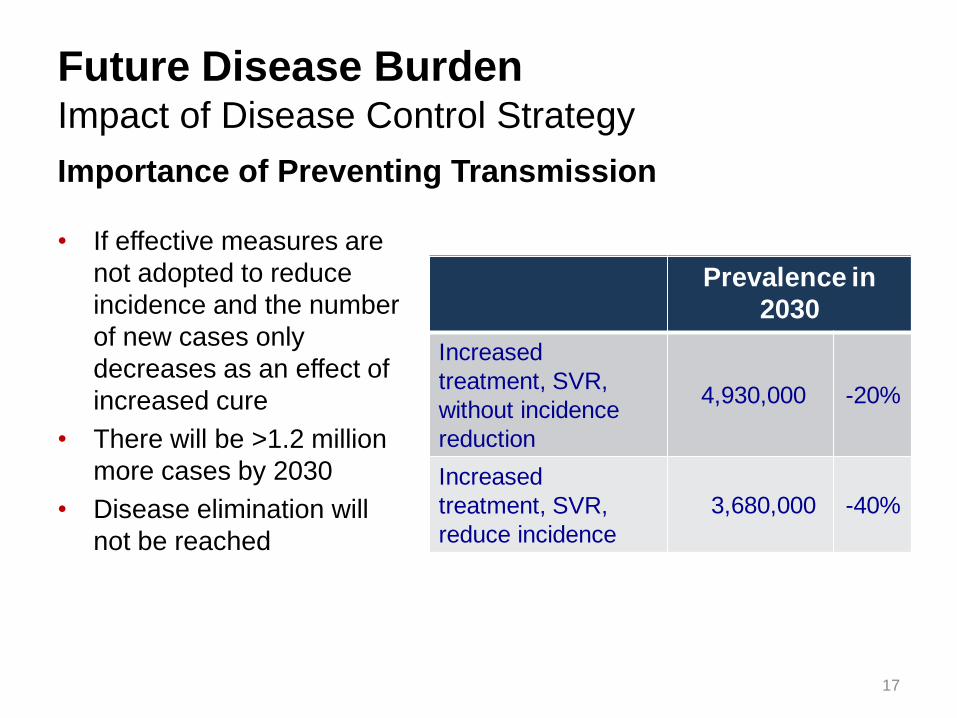
Future Disease Burden Impact of Disease Control Strategy
Importance of Preventing Transmission
• If effective measures are
not adopted to reduce
incidence and the number
of new cases only
decreases as an effect of
increased cure
• There will be >1.2 million
more cases by 2030
• Disease elimination will
not be reached
Prevalence in
2030
Increased
treatment, SVR,
without incidence
reduction
4,930,000 -20%
Increased
treatment, SVR,
reduce incidence
3,680,000 -40%
17

Conclusions
• Without significantly changing treatment strategies,
HCV infection will remain a highly prevalent problem for
the next 20–30 years
• With treatment rates of 3% and SVR 90% along with
treatment initiated at ≥F2, it will be possible to control
HCV disease burden in Russia
• The availability of highly effective therapy,
coupled with increased diagnosis and treatment,
and marked reduction in new cases, has the potential
to significantly reduce hepatitis C morbidity and mortality
in Russia within the next 15 years
18

Cпасибо
Thank you
19

References • Abdourakhmanov DT, Hasaev AS, Castro FJ, Guardia J. Epidemiological and clinical aspects of hepatitis C virus infection in the Russian Republic
of Daghestan. Eur.J.Epidemiol. 1998 Sep;14(6):549-53.
• Andreytseva O.Il, Zhao A.V. Oral presentation at Immune System and Liver Disease conference, May 16, 2009, Nakhabino
• Gautier SV, Moysyuk YG, Khomyakov SM, Ibragimova OS. Progress in organ donation and transplantation in Russian Federation in 2006-2010. 3rd reprot of national registry. Journal of Transplantation and Artificial Organs 2011;2:6-20.
• Gautier SV, Moysyuk YG, Khomyakov SM, Ibragimova OS. Organ donation and transplantation in Russian Federation in 2011. 4th report of national registry. Journal of Transplantation and Artificial Organs 2012;3:6-18.
• Gower, E., et al., Global epidemiology and genotype distribution of the hepatitis C virus, J Hepatol (2014).
• Granov A.M., Granov D.A., Zherebtsov F.K., Gerasimova O.A., Borovik V.V., Osovskikh V.V., Maystrenko D.N., Rutkin I.O., Tsurupa S.P., Tileubergenov I.I., Shapoval S.V., Mikhaylichenko T.G. Liver Transplantation. A single center experience of 100 cases. Journal of Transplantation and Artificial Organs 2012;4:11-16.
• Iashina TL, Favorov MO, Shakhgil'dian IV, Iarasheva DM, Nazarova OI, Derevianko EN, Ommadova MI, Onishchenko GG, Watanabe Y, Nishioka K. [The spread of hepatitis C markers among the population of regions of Russia and Central Asia]. Zh Mikrobiol Epidemiol Immunobiol 1993 September;(5):46-9.
• Lavanchy D. Evolving epidemiology of hepatitis C virus. Clin Microbiol Infec 2011 Feb; 17(2):107-15.
• Pimenov N.N, Chulanov V.P., Komarova S.V. et al. [Hepatitis C in Russia: current epidemiology and approaches to improving diagnosis and surveillance]. Epidemiology and Infectious Diseases, 2012; (4):4-10.
• Pimenov NN, Vdovin AV, Komarova SV, Mamonova NA, Chulanov VP, Pokrovskii VI. [The relevance and proscpets of introducing a uniform federal register of patients with viral hepatitis B and C in Russia.] Ter Arkh 2012; 85(11):4-9.
• Razavi H, Waked I, Sarrazin C, et al. The present and future disease burden of hepatitis C virus (HCV) infection with today's treatment paradigm. J Viral Hepat 2014; 21 Suppl 1: 34-59
• UC Berkeley, Max Planck Institute for Demographic Research, The Human Mortality Database (http://www.mortality.org). 2008-2031 mortality rate was calculated from historical trends and allocated to five year age cohorts.
• United Nations - Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat, World Population Prospects: The 2010 Revision and World Urbanization Prospects: The 2010 Revision, http://esa.un.org/unpd/wpp/unpp/panel_indicators.htm
• Viral hepatitis in Russian Federation. Analytical review. 9 ed. 2013; 113.
• Viral Hepatitis Prevention Board. Russia: Burden of disease. January 2011. http://www.vhpb.org/files/html/Meetings_and_publications/Viral_Hepatitis_Newsletters/vhv19n1.pdf
20

Current Disease Burden
Other Assumptions
• Population – 1950-2030 (United Nations 2010)
• Mortality – 1950-2007 (University of California Berkeley)
• Risk Factors
– Percent of the population infected through IDU- 16% in 1995
(Abdourakhmanov 1998)
– Percent of the population infected through Transfusion - 26% in
1995 (Abdourakhmanov 1998)
-UC Berkeley, Max Planck Institute for Demographic Research, The Human Mortality Database (http://www.mortality.org). 2008-2031 mortality rate was
calculated from historical trends and allocated to five year age cohorts.
-United Nations - Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat, World Population Prospects: The 2010
Revision and World Urbanization Prospects: The 2010 Revision, http://esa.un.org/unpd/wpp/unpp/panel_indicators.htm
-Abdourakhmanov DT, Hasaev AS, Castro FJ, Guardia J. Epidemiological and clinical aspects of hepatitis C virus infection in the Russian Republic of
Daghestan. Eur.J.Epidemiol. 1998 Sep;14(6):549-53.
21

Current Disease Burden
Liver Transplants • Liver transplant data for 2006-2011 was available through Gautier 2011 and
Gautier 2012. Estimates for 2004 and 2005 were trended from the available
data. The calculated weights were applied to generate the number of HCV-
Related Transplants by year
• Assumed 32% of all transplants were due to HCV (Granov 2012 and
Andreytseva 2009)
-
50
100
150
200
250
2004 2005 2006 2007 2008 2009 2010 2011
Liv
er
Tra
nsp
lan
ts
Actual Transplants HCV-Related Transplants
-Gautier SV, Moysyuk YG, Khomyakov SM, Ibragimova OS. Progress in organ donation and transplantation in Russian Federation in 2006-2010. 3rd reprot of
national registry. Journal of Transplantation and Artificial Organs 2011;2:6-20.
-Gautier SV, Moysyuk YG, Khomyakov SM, Ibragimova OS. Organ donation and transplantation in Russian Federation in 2011. 4th report of national registry.
Journal of Transplantation and Artificial Organs 2012;3:6-18.
-Granov A.M., Granov D.A., Zherebtsov F.K., Gerasimova O.A., Borovik V.V., Osovskikh V.V., Maystrenko D.N., Rutkin I.O., Tsurupa S.P., Tileubergenov I.I.,
Shapoval S.V., Mikhaylichenko T.G. Liver Transplantation. A single center experience of 100 cases. Journal of Transplantation and Artificial Organs 2012;4:11-
16.
-Andreytseva O.Il, Zhao A.V. Oral presentation at Immune System and Liver Disease conference, May 16, 2009, Nakhabino.
22







