Aplastic AnemiaAplastic Anemia
Rakesh Biswas
MD, Professor, Department of Medicine, People's College of Medical Sciences, Bhanpur,
Bhopal, India
Morphologic, Etiologic
Possible causes:
Investigations and treatment

• Definition:
– Pancytopenia with hypocellularity (Aplasia) of Bone Marrow
• One cell line may be affected more than the others
Etiology• Inherited
– Fanconi’s Anemia
• Acquired– Idiopathic (majority)-2/3rd of cases– Drug : Acetazolamide, Carbamazepine, Gold,
Hydantoin, Penicillin, Phenylbutazone,
– Chemical – Radiation exposure – Viral illness

Pathogenesis
• Immune mechanism responsible for most of the cases of Idiopathic acquired aplastic anemia
• Activated Cytotoxic T cells in Blood & Bone marrow Bone marrow failure

Clinical Features
• Signs & symptoms of :
– Anemia:……….
– Bleeding: Ecchymoses ,Bleeding gums, Epistaxis
– Infections: Fever,Mouth ulcers

Diagnosis
• Blood peripheral smear : Pancytopenia and reticulocytopenia
• Bone marrow aspiration & biopsy : Hypocellular / aplastic bone marrow with increased fat spaces
• Tests for underlying cause ( viral titers)
• Other causes of Pancytopenia:– Drugs,– Megaloblastic anemia– Bone Marrow infiltration or Replacement:
Lymphoma, Myeloma,Acute Leukemia, Secondaries
– Hyperspleenisn– SLE– Disseminated TB– PNH– Sepsis

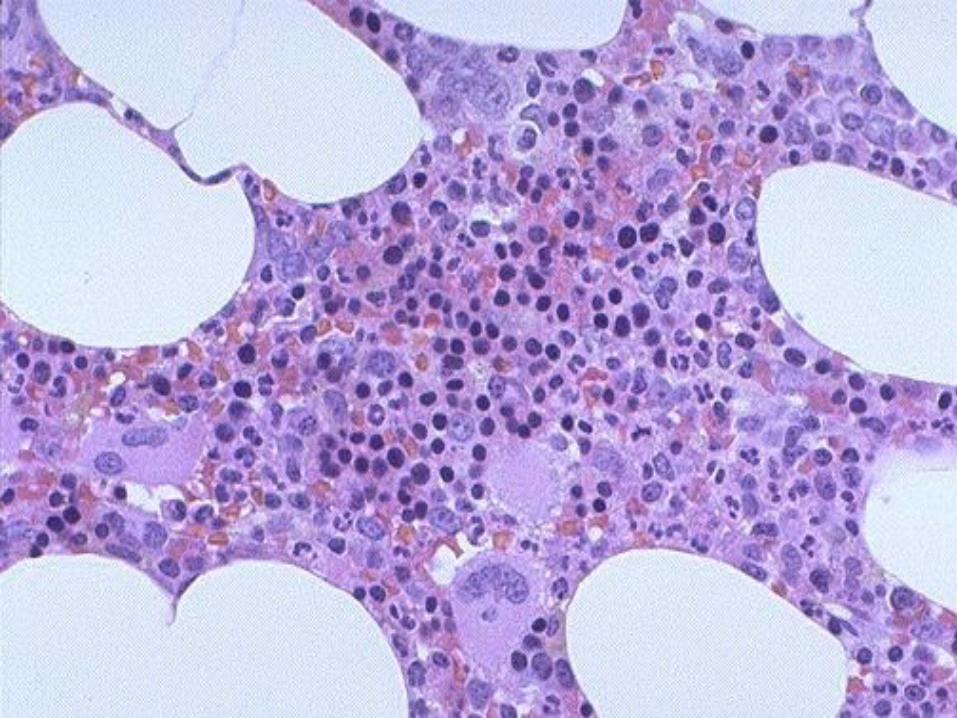
BM Aspiration BM Biopsy
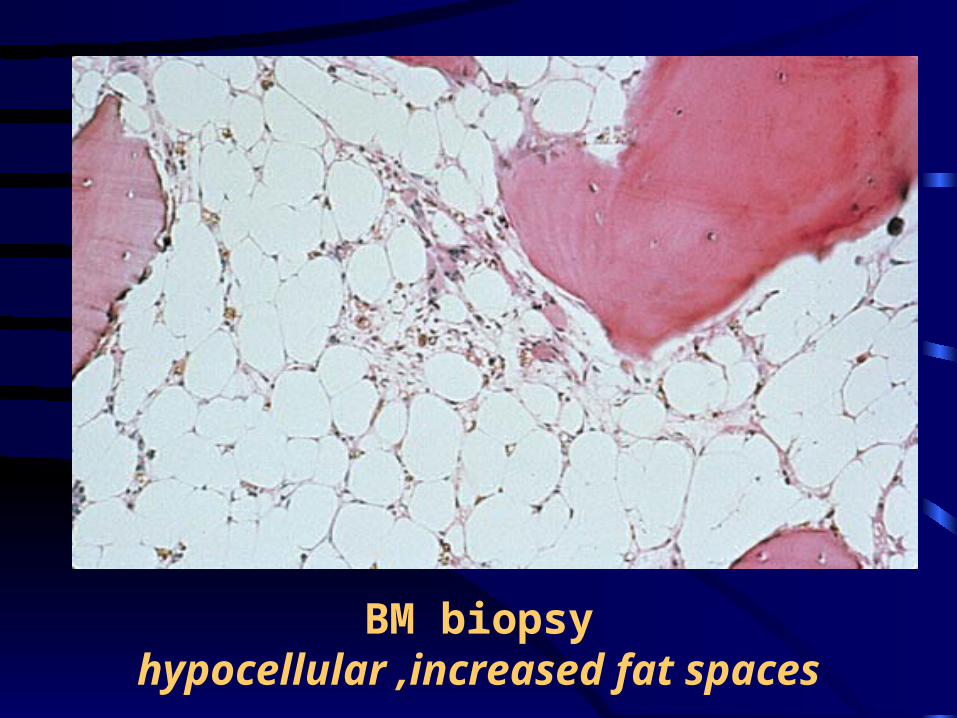
BM biopsyhypocellular ,increased fat spaces
Text book Treatment
• Treatment of underlying cause –if possible• Removal of cause• Supportive care
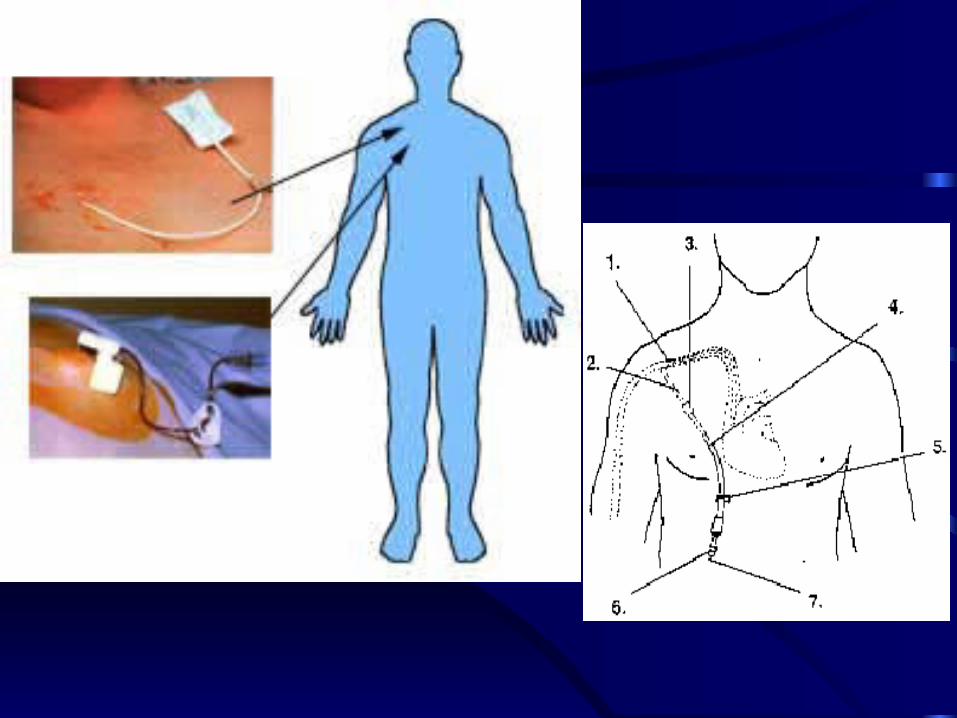
– Blood & platelet transfusion – Infection: Broad spectrum antibiotics– Asepsis
• Bone Marrow Transplant (SCT) – patient age <40yrs , availability of a HLA-
identical sibling marrow donor

• Immunosuppression:
– Cyclosporine,
– Glucocorticoids : in cong Pure Red Cell Aplasia
– Antilymphocyte or Antithymocyte globulin (ALG / ATG)
– Cyclophosphomide
• Androgens
• Thymectomy : for Adult Pure Red Cell Aplasia
Case History:My first post-Cyclophosphamide white cells appeared 10 days after treatment. I had 6. I ordered them all little party hats,
and got to know them personally:-)
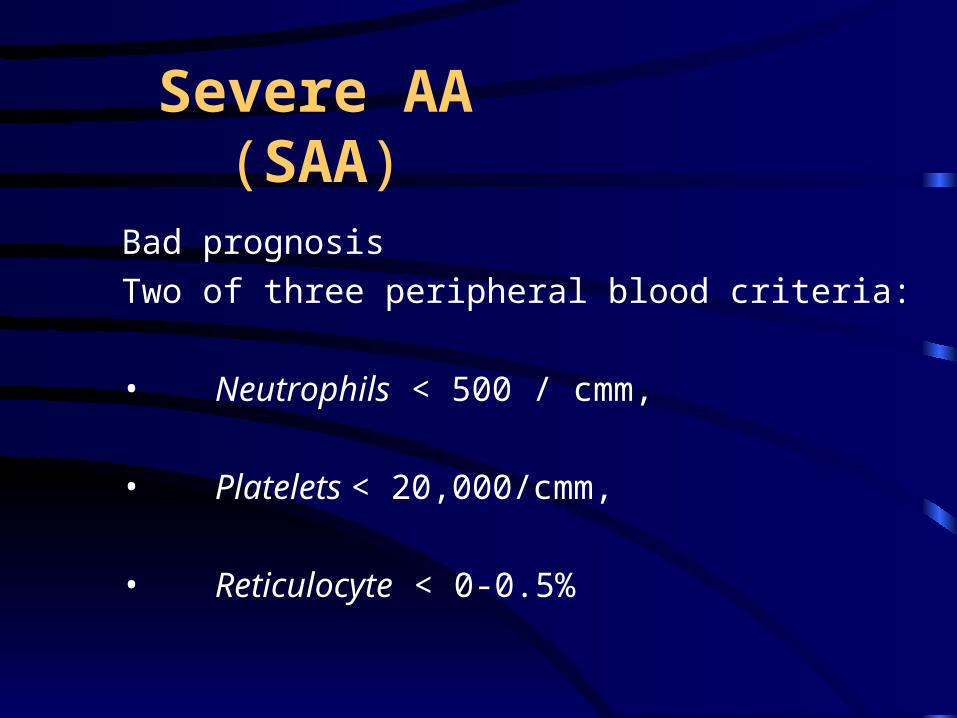
Severe AA (SAA)
Bad prognosis
Two of three peripheral blood criteria:
• Neutrophils < 500 / cmm,
• Platelets < 20,000/cmm,
• Reticulocyte < 0-0.5%
Prognosis
• Improved survival with newer treatment modalities
• Relates to severity
• Evolution to MDS, PNH, AML`
Agranulocytosis
• Leukopenia: Decrease in Total Leukocyte Count
• Neutropenia: Decrease in Neutrophil count < 1500 / micro L
• Agranulocytosis: severe neutropenia < 500 neutrophils / micro L
Causes• Congenital• Drug induced:Chloramphenicol,CBZ, Carbimazole
, Co-trimoxazole, Gold, Phenytoin, Sulfa drugs• Infections:
– Viral-Hepatitis,Influenza,HIV – Bacterial-Typhoid,Miliary TB
• Benign ( familial/racial)• Cyclical• Immune: AI, SLE,Felty’s,
Clinical Features
• Mouth infection,Sore throat ( Mucositis)• Ulcers of : Mouth & throat , Skin, Anus
• Features of Sepsis (Gm +ve &–ve):– Fever +/-– Hypotension,– MODS
• In prolonged neutropenia Fungal infections are likely to develop: Candida (Oral), Aspergillus(Pulm)
Investigations and Treatment
The peripheral blood smear shows a marked decrease or absence of neutrophils.
The bone marrow may show myeloid hypoplasia or absence of myeloid precursors.
In many cases, the bone marrow is cellular with a maturation arrest at the promyelocyte stage.
On occasion, the marrow may be hypercellular.







