aplastic anemia rakesh biswas md, professor, department of medicine, people's college of...
TRANSCRIPT
Aplastic AnemiaAplastic Anemia
Rakesh Biswas
MD, Professor, Department of Medicine, People's College of Medical Sciences, Bhanpur,
Bhopal, India
Morphologic, Etiologic
Possible causes:
Investigations and treatment

• Definition:
– Pancytopenia with hypocellularity (Aplasia) of Bone Marrow
• One cell line may be affected more than the others
Etiology• Inherited
– Fanconi’s Anemia
• Acquired– Idiopathic (majority)-2/3rd of cases– Drug : Acetazolamide, Carbamazepine, Gold,
Hydantoin, Penicillin, Phenylbutazone,
– Chemical – Radiation exposure – Viral illness

Pathogenesis
• Immune mechanism responsible for most of the cases of Idiopathic acquired aplastic anemia
• Activated Cytotoxic T cells in Blood & Bone marrow Bone marrow failure

Clinical Features
• Signs & symptoms of :
– Anemia:……….
– Bleeding: Ecchymoses ,Bleeding gums, Epistaxis
– Infections: Fever,Mouth ulcers

Diagnosis
• Blood peripheral smear : Pancytopenia and reticulocytopenia
• Bone marrow aspiration & biopsy : Hypocellular / aplastic bone marrow with increased fat spaces
• Tests for underlying cause ( viral titers)
• Other causes of Pancytopenia:– Drugs,– Megaloblastic anemia– Bone Marrow infiltration or Replacement:
Lymphoma, Myeloma,Acute Leukemia, Secondaries
– Hyperspleenisn– SLE– Disseminated TB– PNH– Sepsis

BM Aspiration BM Biopsy
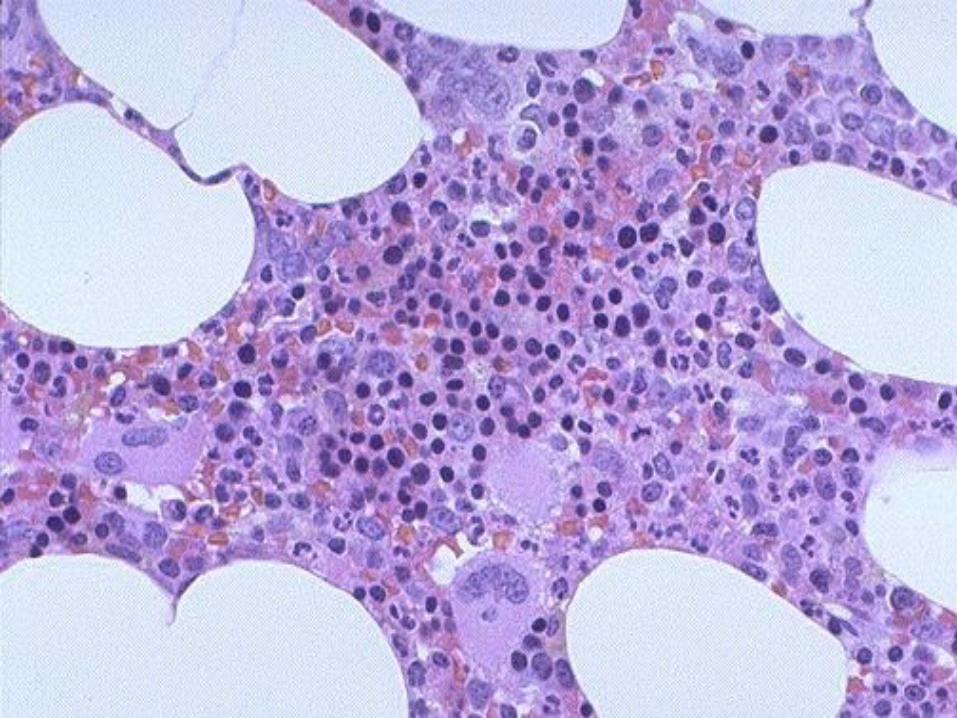
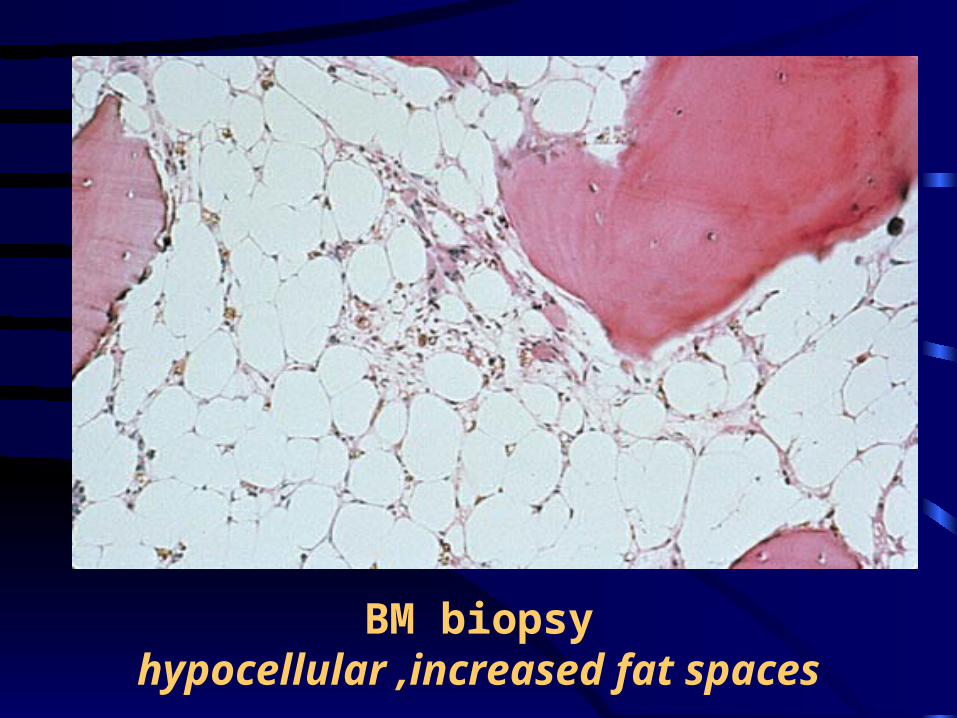
BM biopsyhypocellular ,increased fat spaces
Text book Treatment
• Treatment of underlying cause –if possible• Removal of cause• Supportive care
– Blood & platelet transfusion – Infection: Broad spectrum antibiotics– Asepsis
• Bone Marrow Transplant (SCT) – patient age <40yrs , availability of a HLA-
identical sibling marrow donor

• Immunosuppression:
– Cyclosporine,
– Glucocorticoids : in cong Pure Red Cell Aplasia
– Antilymphocyte or Antithymocyte globulin (ALG / ATG)
– Cyclophosphomide
• Androgens
• Thymectomy : for Adult Pure Red Cell Aplasia
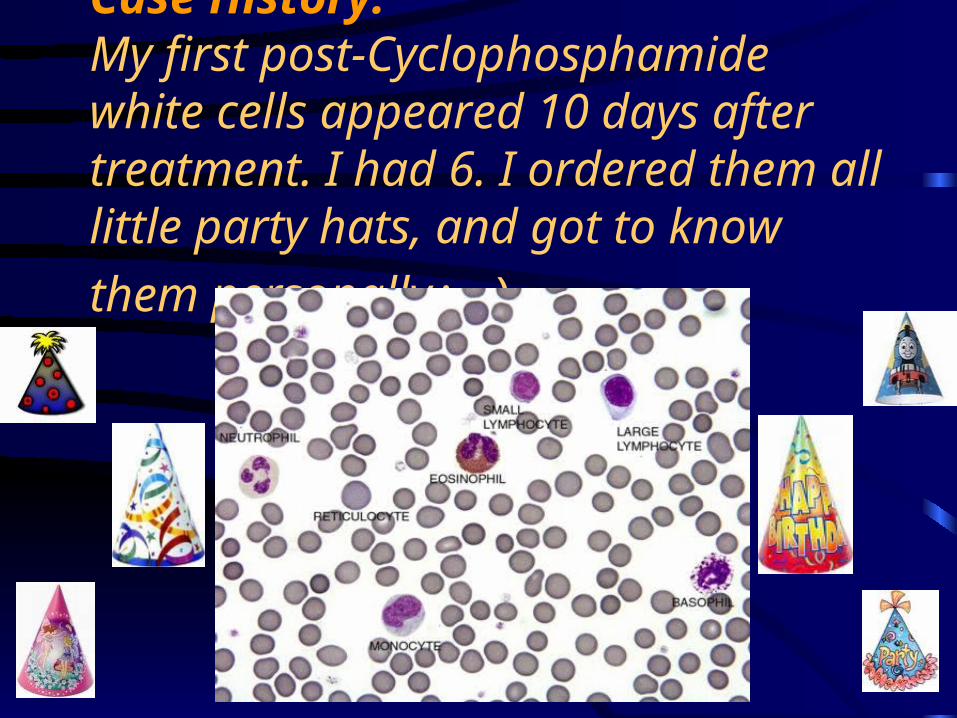
Case History:My first post-Cyclophosphamide white cells appeared 10 days after treatment. I had 6. I ordered them all little party hats,
and got to know them personally:-)
Severe AA (SAA)
Bad prognosis
Two of three peripheral blood criteria:
• Neutrophils < 500 / cmm,
• Platelets < 20,000/cmm,
• Reticulocyte < 0-0.5%
Prognosis
• Improved survival with newer treatment modalities
• Relates to severity
• Evolution to MDS, PNH, AML`
Agranulocytosis
• Leukopenia: Decrease in Total Leukocyte Count
• Neutropenia: Decrease in Neutrophil count < 1500 / micro L
• Agranulocytosis: severe neutropenia < 500 neutrophils / micro L
Causes• Congenital• Drug induced:Chloramphenicol,CBZ, Carbimazole
, Co-trimoxazole, Gold, Phenytoin, Sulfa drugs• Infections:
– Viral-Hepatitis,Influenza,HIV – Bacterial-Typhoid,Miliary TB
• Benign ( familial/racial)• Cyclical• Immune: AI, SLE,Felty’s,
Clinical Features
• Mouth infection,Sore throat ( Mucositis)• Ulcers of : Mouth & throat , Skin, Anus
• Features of Sepsis (Gm +ve &–ve):– Fever +/-– Hypotension,– MODS
• In prolonged neutropenia Fungal infections are likely to develop: Candida (Oral), Aspergillus(Pulm)
Investigations and Treatment
The peripheral blood smear shows a marked decrease or absence of neutrophils.
The bone marrow may show myeloid hypoplasia or absence of myeloid precursors.
In many cases, the bone marrow is cellular with a maturation arrest at the promyelocyte stage.
On occasion, the marrow may be hypercellular.