
2/7/2018
1
THE RED EYE Richard A. Jacobs, M.D.,PhD*
*Todd Margolis, M.D.,PhD, Prof of Ophthalmology and Director F. I. Proctor Foundation, UCSF (Now Chair of Ophthalmology at Washington University in St. Louis)Brian Schwartz, M.D., Associate Professor of Medicine, Division of Infectious Diseases
NO DISCLOSURES
2/7/2018
2
Case
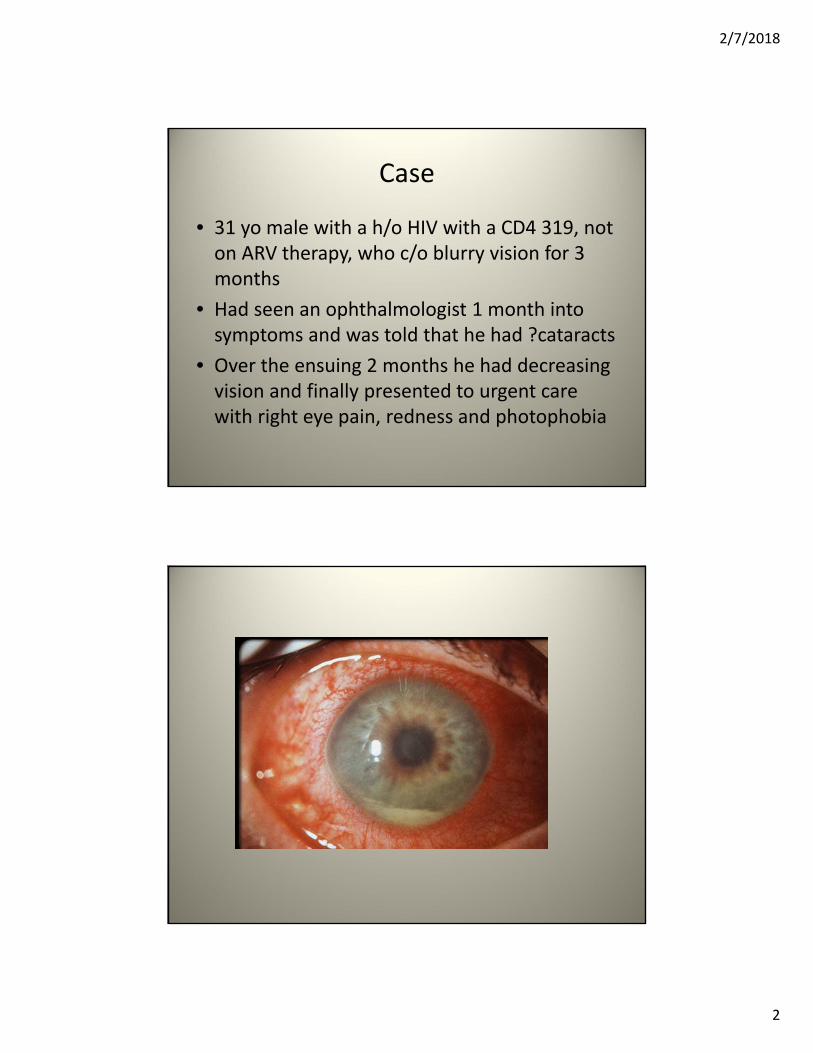
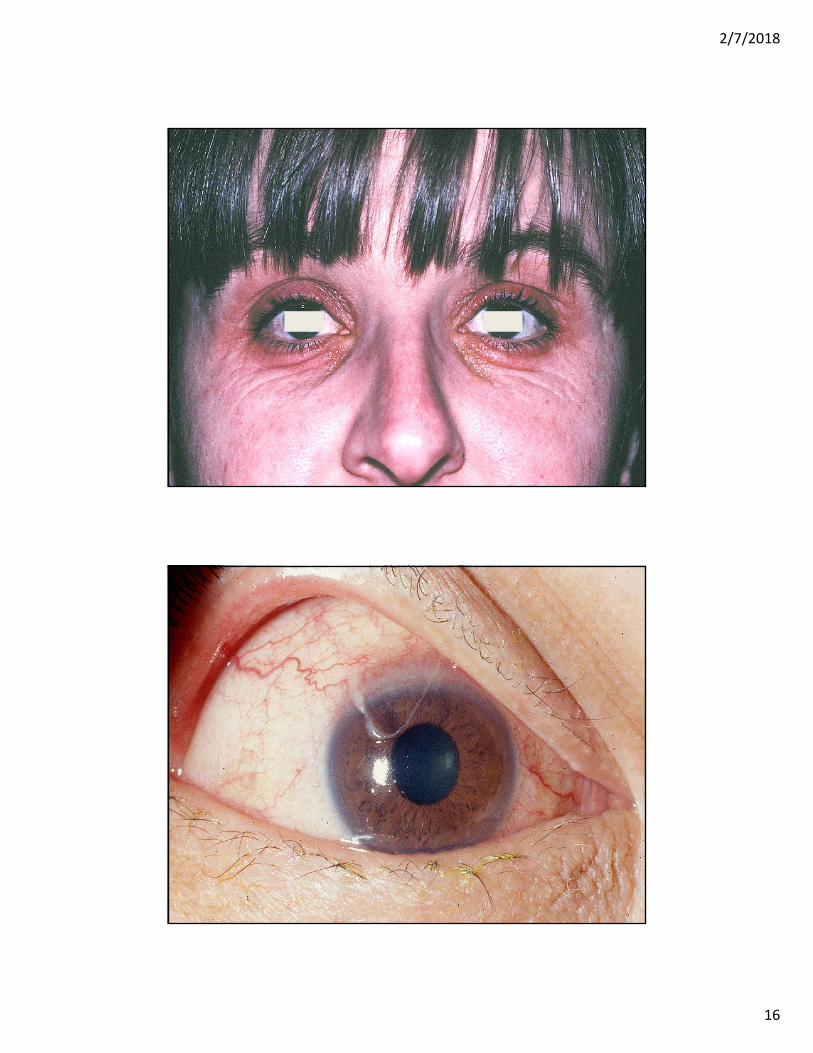
• 31 yo male with a h/o HIV with a CD4 319, not on ARV therapy, who c/o blurry vision for 3 months
• Had seen an ophthalmologist 1 month into symptoms and was told that he had ?cataracts
• Over the ensuing 2 months he had decreasing vision and finally presented to urgent care with right eye pain, redness and photophobia
2/7/2018
3
Case
• Should he be referred to an ophthalmologist?
• What is the diagnosis?
Infections of the eye• Ocular infections
– Kerititis– Conjunctivitis– Uveitis– Endopthalmitis– Retinitis
• Peri-ocular infections– Orbital infections
• Preseptal cellulitis• Orbital cellulitis• Subperiosteal abscess• Orbital abscess
– Lacrimal system infections• Dacryoadenitis• Canaliculitis• Dacryocystitis
– Eyelid infections• Hordeolum• Chalazion• Blephiritis
What the @#%&*……
2/7/2018
4
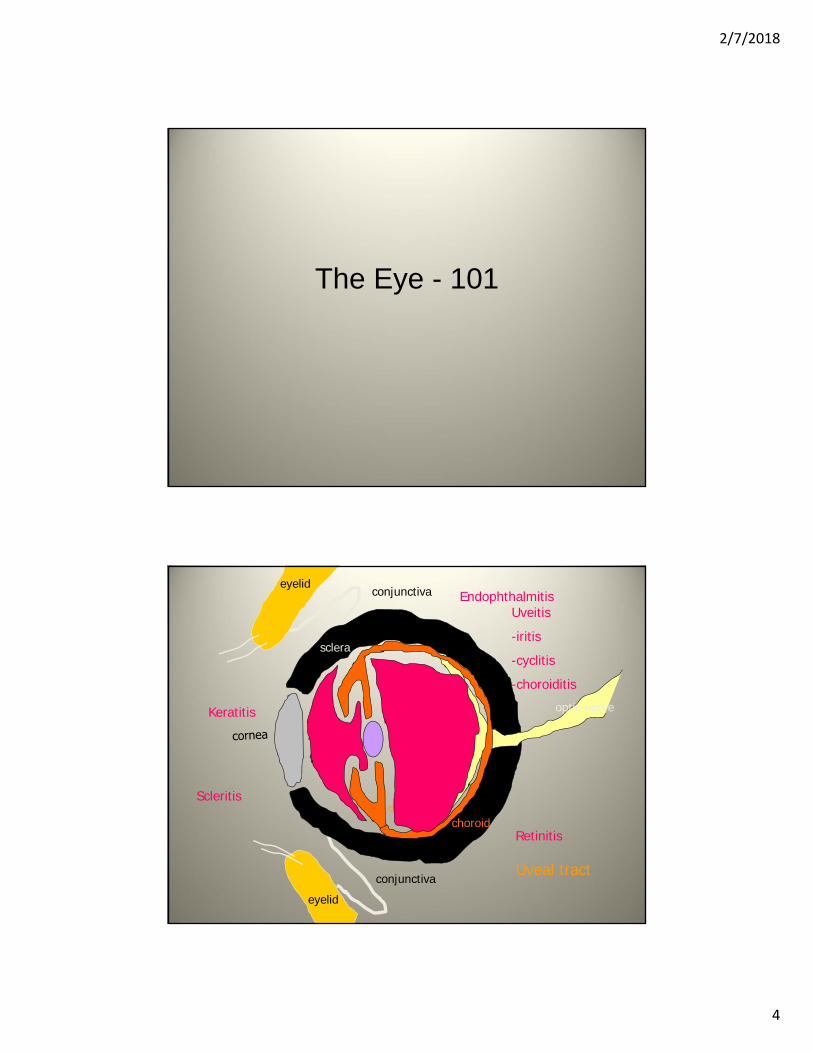
The Eye - 101
sclera
eyelidconjunctiva
eyelid
conjunctiva
optic nerveretina
choroid
lens
iris
ciliary body
EndophthalmitisUveitis
-iritis
-cyclitis
-choroiditis
Keratitis
Retinitis
Uveal tract
Scleritis
2/7/2018
5
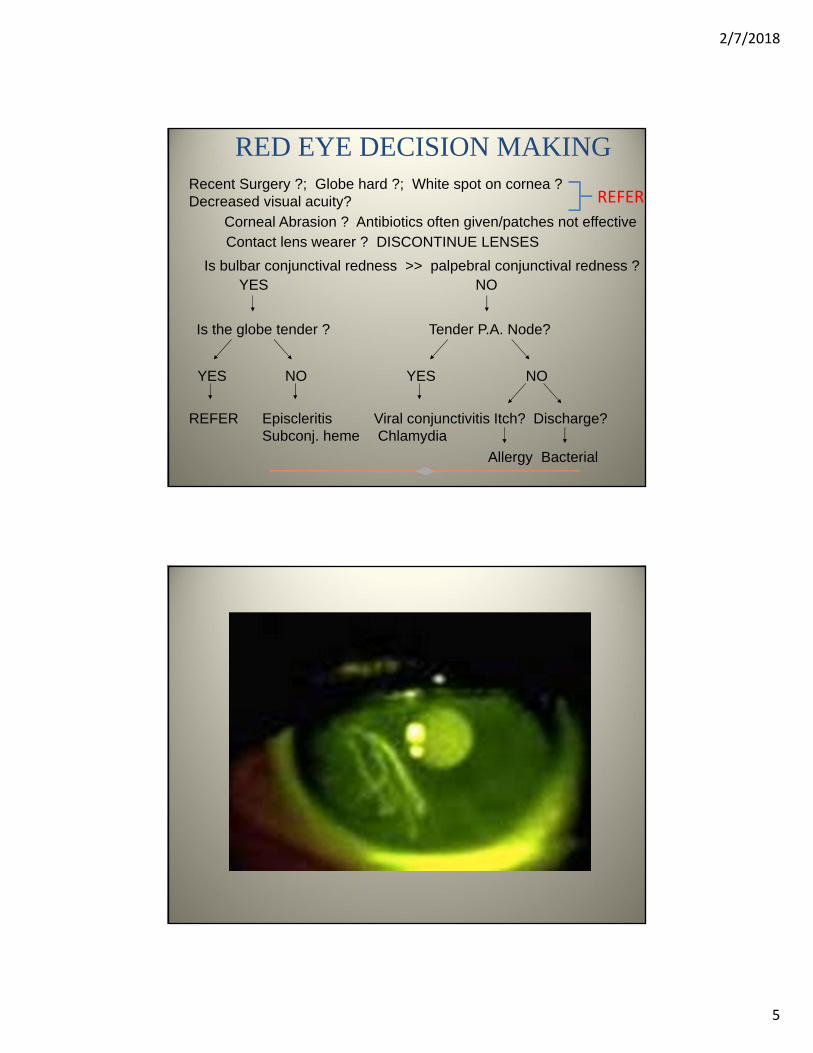
RED EYE DECISION MAKINGRecent Surgery ?; Globe hard ?; White spot on cornea ?Decreased visual acuity?
Is bulbar conjunctival redness >> palpebral conjunctival redness ?YES NO
Is the globe tender ? Tender P.A. Node?
YES NO YES NO
REFER Episcleritis Viral conjunctivitis Itch? Discharge?Subconj. heme Chlamydia
Contact lens wearer ? DISCONTINUE LENSES
Allergy Bacterial
Corneal Abrasion ? Antibiotics often given/patches not effective
REFER
2/7/2018
6
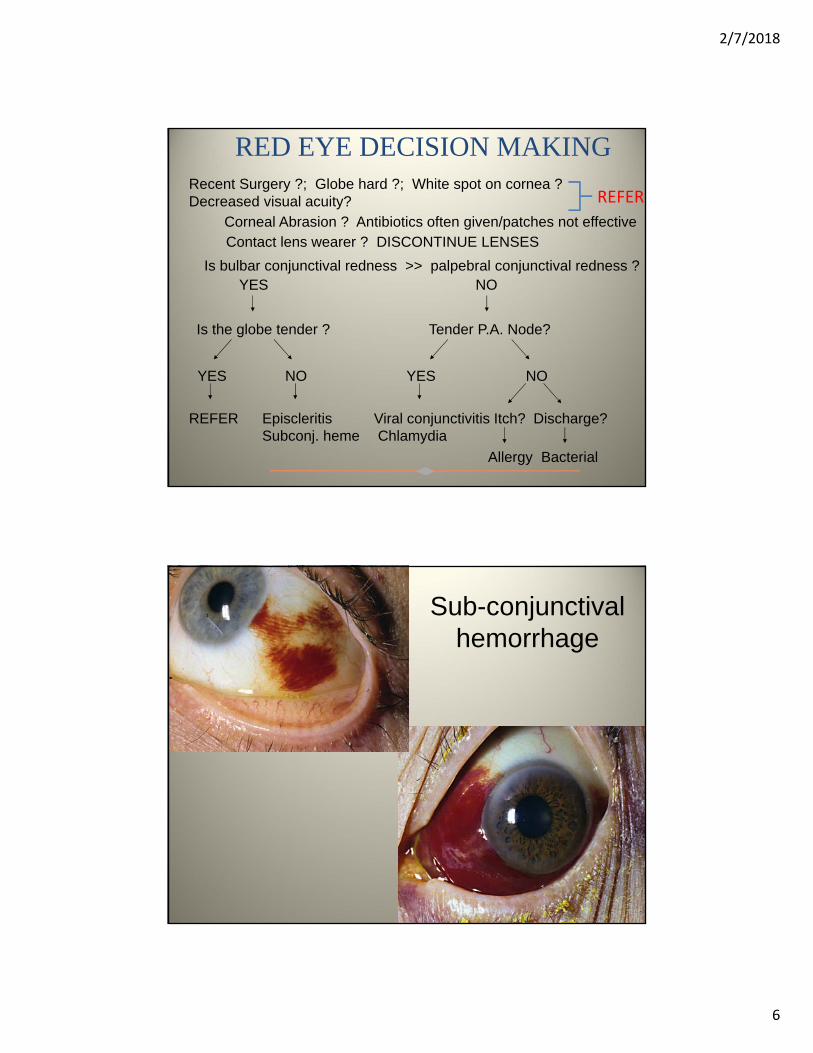
RED EYE DECISION MAKINGRecent Surgery ?; Globe hard ?; White spot on cornea ?Decreased visual acuity?
Is bulbar conjunctival redness >> palpebral conjunctival redness ?YES NO
Is the globe tender ? Tender P.A. Node?
YES NO YES NO
REFER Episcleritis Viral conjunctivitis Itch? Discharge?Subconj. heme Chlamydia
Contact lens wearer ? DISCONTINUE LENSES
Allergy Bacterial
Corneal Abrasion ? Antibiotics often given/patches not effective
REFER
Sub-conjunctival hemorrhage
2/7/2018
7
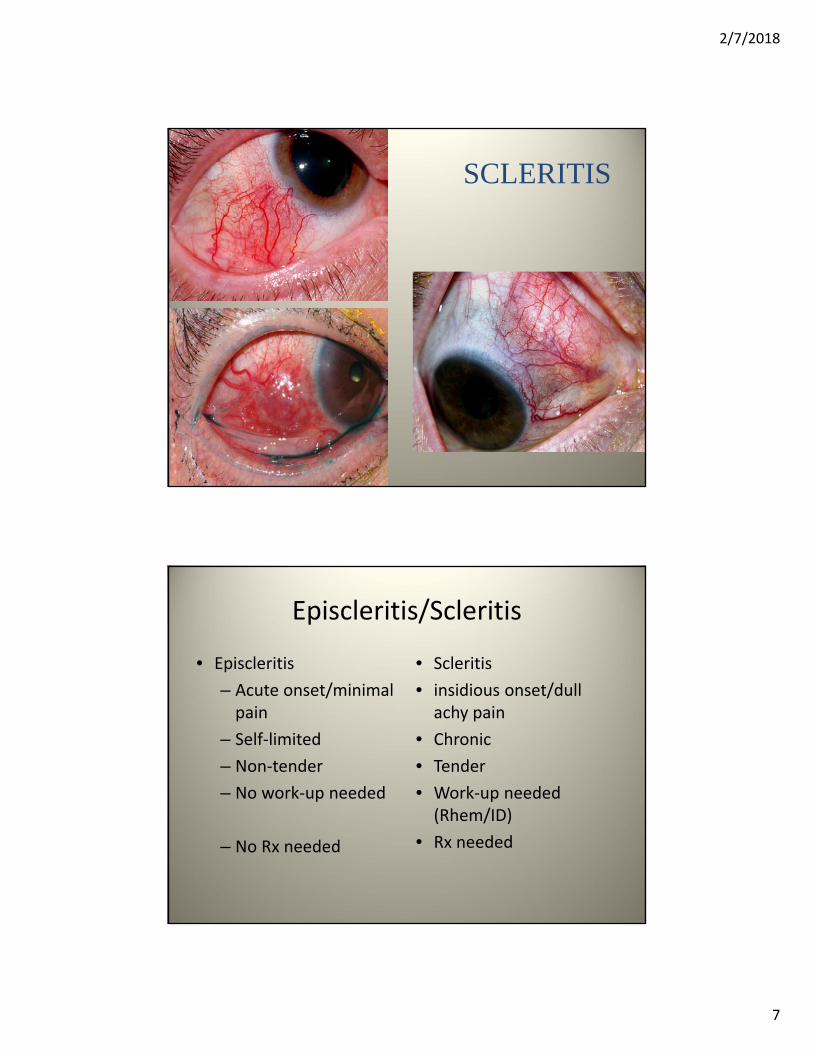
SCLERITIS
Episcleritis/Scleritis
• Episcleritis
– Acute onset/minimal pain
– Self‐limited
– Non‐tender
– No work‐up needed
– No Rx needed
• Scleritis
• insidious onset/dull achy pain
• Chronic
• Tender
• Work‐up needed (Rhem/ID)
• Rx needed
2/7/2018
8
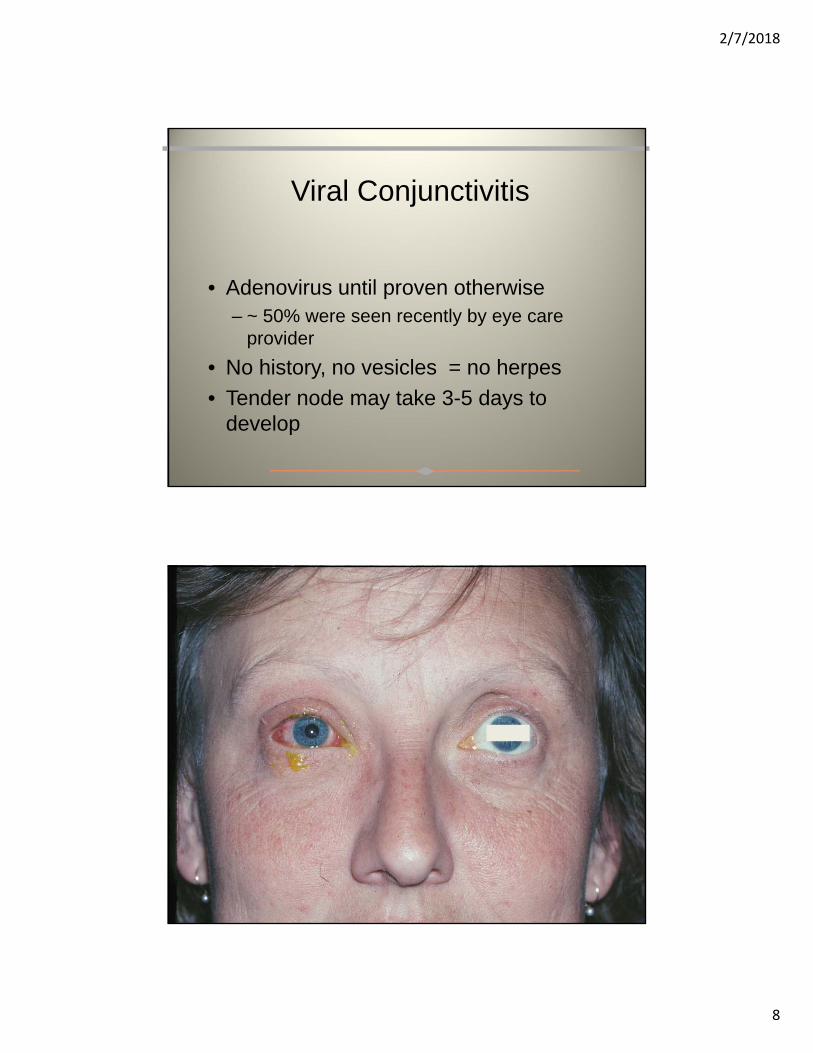
Viral Conjunctivitis
• Adenovirus until proven otherwise– ~ 50% were seen recently by eye care
provider
• No history, no vesicles = no herpes
• Tender node may take 3-5 days to develop

2/7/2018
9
Management of viral conjunctivitis
• Supportive care (cold AT, vasoconstrictors)
• Antibiotic coverage unwarranted
• Corticosteroids prolong viral shedding
ChlamydiaConjunctivits

2/7/2018
10
Chlamydia Conjunctivitis
• Less common than viral conjunctivitis
• Not an acute conjunctivitis– Chronic, indolent inclusion conjunctivitis
• Diagnosis suspected when patients fail to respond to topical antibiotic therapy
• Can confirm diagnosis by DFA, culture or PCR
• Therapy is doxycycline or azithromycin

2/7/2018
11
Management of Bacterial Conjunctivitis
• Prime suspects:– S. aureus, Strep. pneumoniae, H.
influenzae• First line drugs:
– Sulfacetamide (Bleph-10®)– Polymyxin/trimethoprim (Polytrim®)
• 72 hour rule

2/7/2018
12
Hyperacute Bacterial Conjunctivits
Hyperacute Bacterial Conjunctivits
• Due to Neisseria gonorrhoeae
• Characterized by:– Acute onset
– Copious purulent discharge
– Chemosis and eye lid swelling
– Rapid progression
• Emergency that requires systemic antibiotics

2/7/2018
13
Management of Bacterial Conjunctivitis
Drugs to avoid– Ointments: poor compliance
– Erythromycin: very high rates of resistance
• H. influenza 94%, S. epi. 70%, S. aureus 45%, Strep. pneumo 8%
– Aminoglycosides: coverage & toxicity
– Fluoroquinolones: expense. Save for resistant cases.
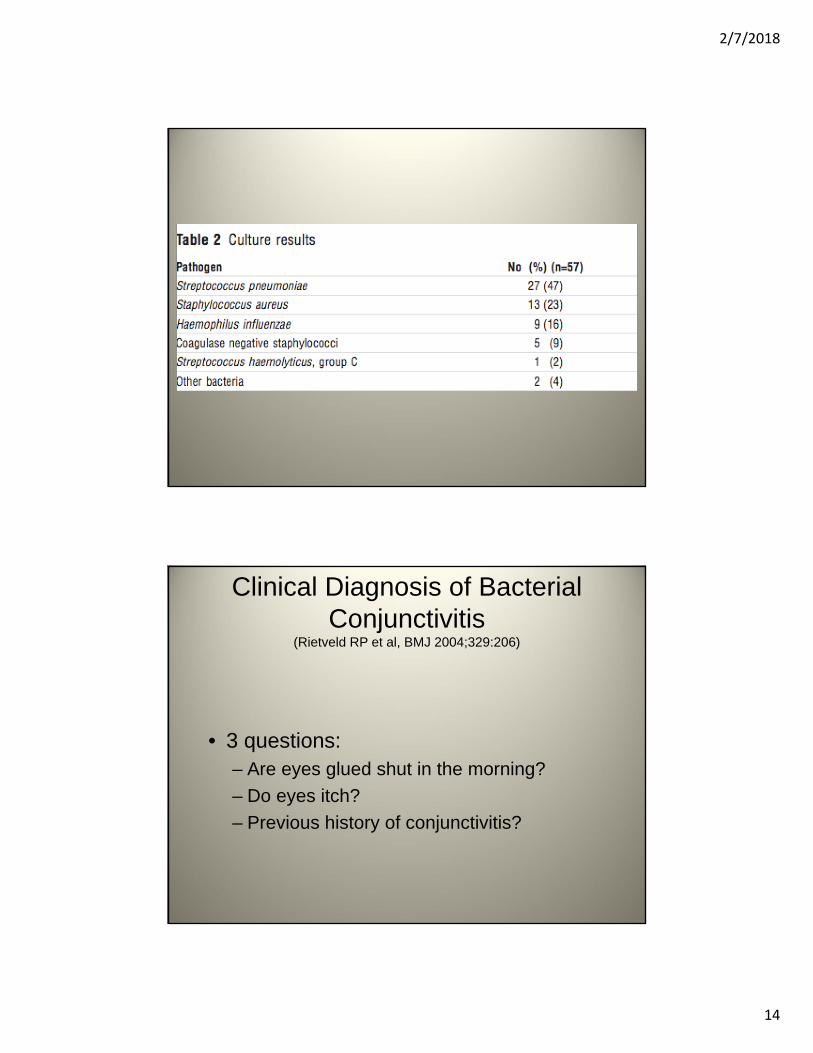
Clinical Diagnosis of Bacterial Conjunctivitis
(Rietveld RP et al, BMJ 2004;329:206)
• Dutch study of primary care physicians
• 184 adults (not contact lens wearers) presenting with a red eye and discharge
• All patients cultured– 57 with + bacterial cultures
– 120 negative cultures
2/7/2018
14
Clinical Diagnosis of Bacterial Conjunctivitis
(Rietveld RP et al, BMJ 2004;329:206)
• 3 questions:– Are eyes glued shut in the morning?
– Do eyes itch?
– Previous history of conjunctivitis?

2/7/2018
15
Clinical Diagnosis of Bacterial Conjunctivitis
(Rietveld RP et al, BMJ 2004;329:206)
Symptom Odds Ratio Probability of Bacterial Conjunctivitis
Both eyes glued shut in AM
15:1 77%
itching
previous h/o conjunctivitis
4%
Allergic Conjunctivitis
• History of allergies, rubbing or itching
• Typical periocular skin changes
• Stringy, mucoid discharge
• Eosinophils on Giemsa stain
2/7/2018
16

2/7/2018
17
Management of Allergic Conjunctivitis
• Cold compresses• Cold artificial tears• Topical antihistamines/vasoconstrictors – Visine A, Naphcon
A, Opcon A– OTC– Use < 2 weeks– Can cause rebound hyperemia
• Antihistamine + mast cell stabilizer – Patanol/Lastacaft• REFER if severe symptoms persist after 3 weeks of
antihistamine/mast cell stabilizer therapy• Topical corticosteroids/pulse steroids--leave to
ophthalmologist
Contact Lens Related Problems

2/7/2018
18
Contact Lens Related Problems
Contact Lens Related Problems
• Dirty lens• Torn lens• Lens overwear• Corneal abrasion• Drug toxicity/allergies/abuse• Infections

2/7/2018
19
Contact Lens Users Are Contact Lens Abusers
• 41 million contact lens users > 18 yrs of age
• ≈ 1/3 of wearers reported a red or painful eye requiring a doctor’s visit
• When surveyed, what % of users reported lens hygiene behavior associated with increased risk of infection?
MMWR Vol. 64, No. 32, August 21, 2015
% of Users Admitting Risky Hygiene Behavior
• 25%
• 50%
• 75%
• 100%
MMWR Vol. 64, No. 32, August 21, 2015

2/7/2018
20
% of Users Admitting Risky Hygiene Behavior
• 25%
• 50%
• 75%
• 100% (99%)
MMWR Vol. 64, No. 32, August 21, 2015
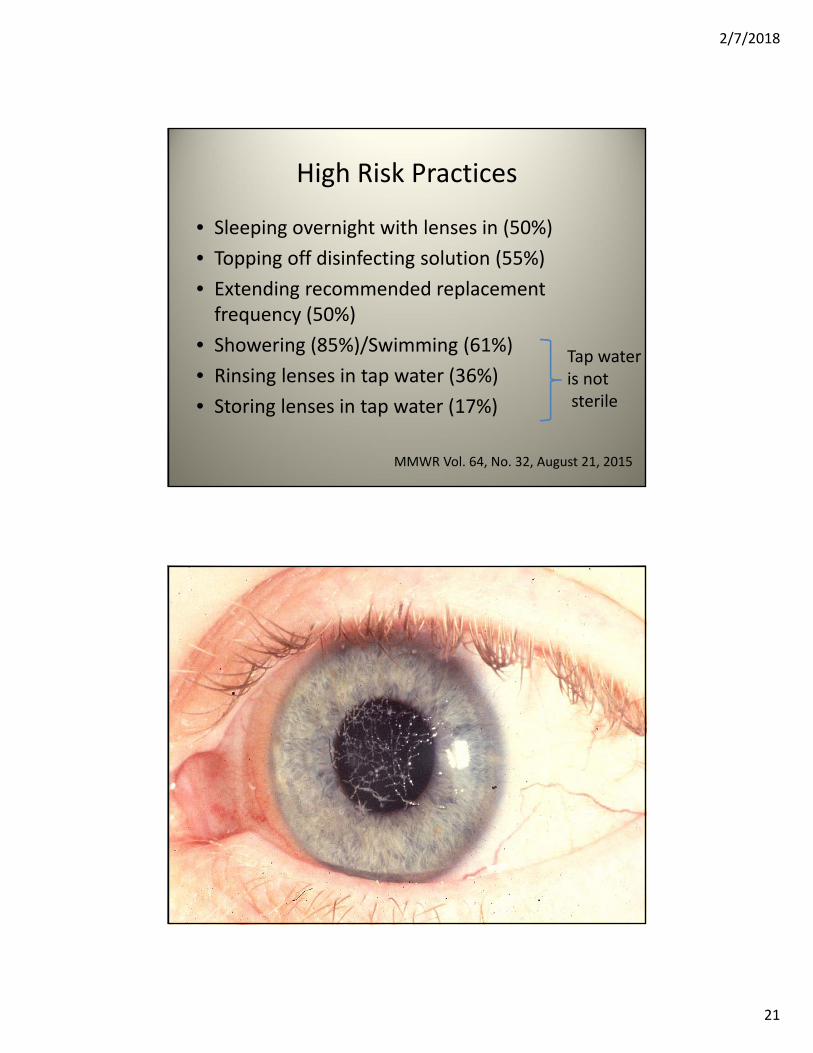
High Risk Practices
• Sleeping overnight with lenses in (50%)
• Topping off disinfecting solution (55%)
• Extending recommended replacement frequency (50%)
• Showering (85%)/Swimming (61%)
• Rinsing lenses in tap water (36%)
• Storing lenses in tap water (17%)
MMWR Vol. 64, No. 32, August 21, 2015
2/7/2018
21
High Risk Practices
• Sleeping overnight with lenses in (50%)
• Topping off disinfecting solution (55%)
• Extending recommended replacement frequency (50%)
• Showering (85%)/Swimming (61%)
• Rinsing lenses in tap water (36%)
• Storing lenses in tap water (17%)
Tap wateris notsterile
MMWR Vol. 64, No. 32, August 21, 2015

2/7/2018
22
2/7/2018
23
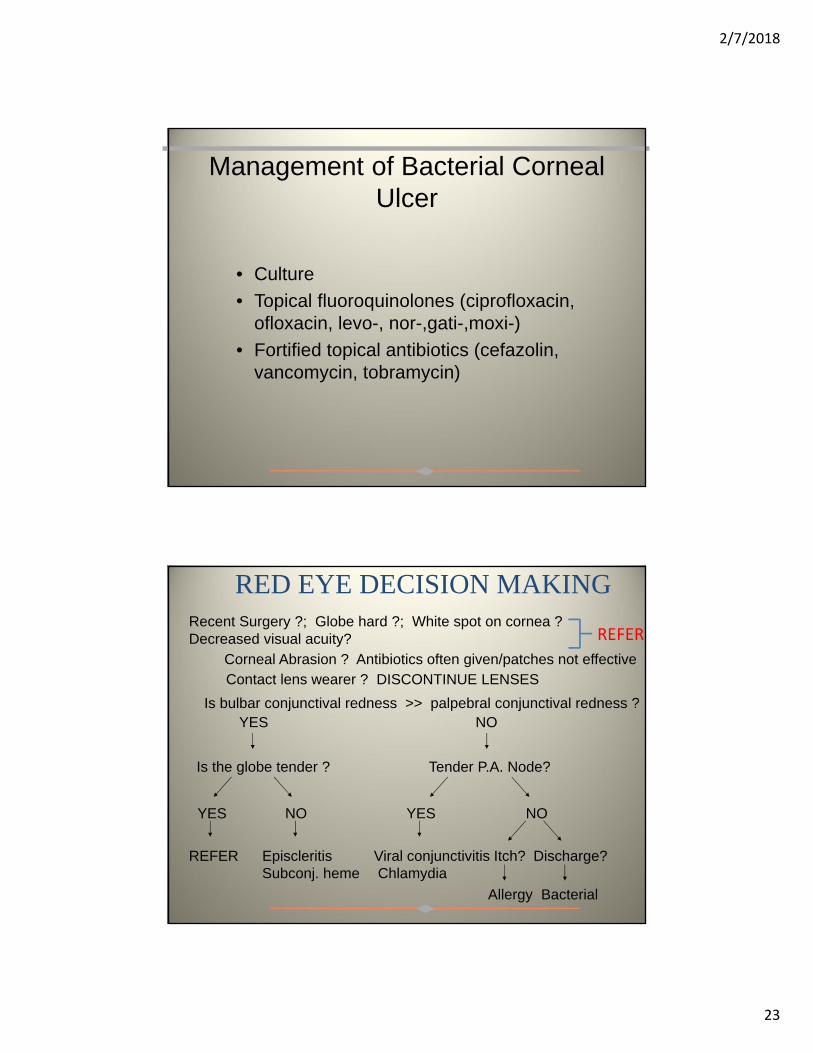
Management of Bacterial Corneal Ulcer
• Culture
• Topical fluoroquinolones (ciprofloxacin, ofloxacin, levo-, nor-,gati-,moxi-)
• Fortified topical antibiotics (cefazolin, vancomycin, tobramycin)
RED EYE DECISION MAKINGRecent Surgery ?; Globe hard ?; White spot on cornea ?Decreased visual acuity?
Is bulbar conjunctival redness >> palpebral conjunctival redness ?YES NO
Is the globe tender ? Tender P.A. Node?
YES NO YES NO
REFER Episcleritis Viral conjunctivitis Itch? Discharge?Subconj. heme Chlamydia
Contact lens wearer ? DISCONTINUE LENSES
Allergy Bacterial
Corneal Abrasion ? Antibiotics often given/patches not effective
REFER

2/7/2018
24
Back to the Case
HIV + male with decreased vision and a CD4 319
Back to the Case
• Should he be referred to an ophthalmologist?
• What is the diagnosis?
2/7/2018
25
Back to the Case
• RPR was 1:1024
• FTA‐ABS positive
Review of ocular syphilis
• Ocular syphilis may occur in secondary or tertiary syphilis
• Uveitis is the most common manifestation, but can also have a keratitis or scleritis.
• Bilateral eye involvement is seen in about 50% of patients
• All patient with presumed ocular syphilis should have a lumbar puncture to exclude concomitiant meningitis.
• Ocular syphilis is often, but not always, accompanied by syphilitic meningitis.
Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 7th ed.
2/7/2018
26
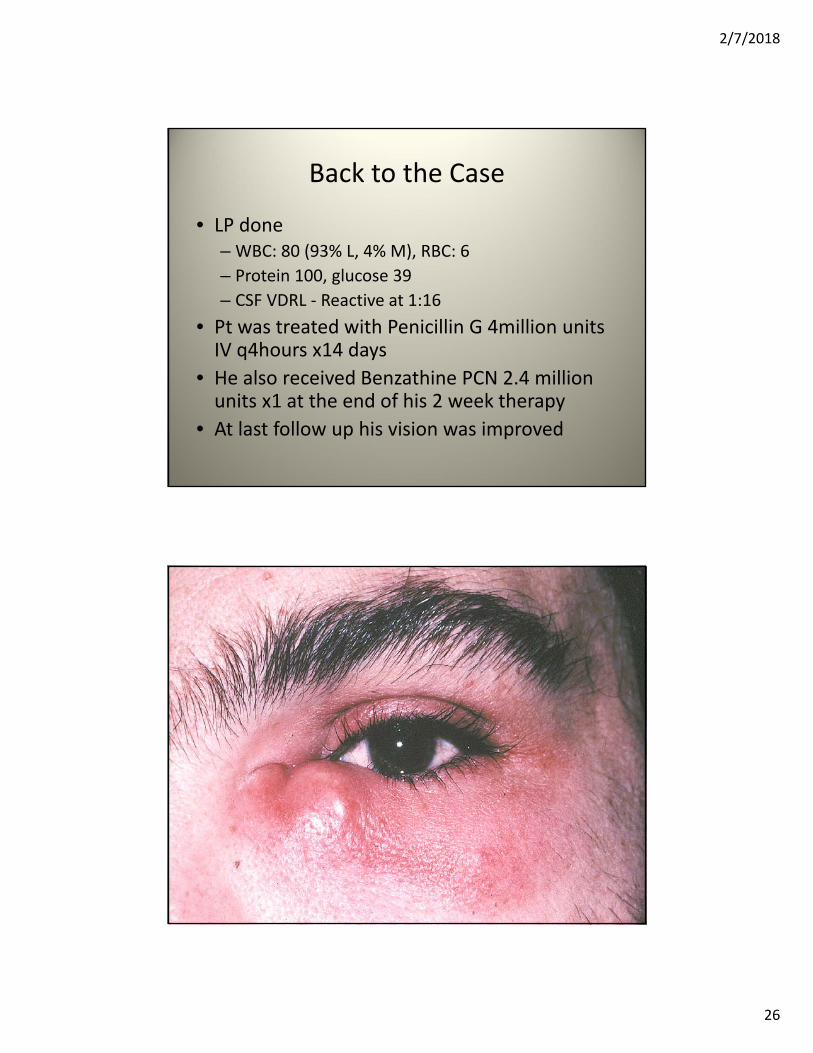
Back to the Case
• LP done– WBC: 80 (93% L, 4% M), RBC: 6
– Protein 100, glucose 39
– CSF VDRL ‐ Reactive at 1:16
• Pt was treated with Penicillin G 4million units IV q4hours x14 days
• He also received Benzathine PCN 2.4 million units x1 at the end of his 2 week therapy
• At last follow up his vision was improved

2/7/2018
27
Orbital septumPeriocular infections
Ethmoid sinus
Sphenoid sinus
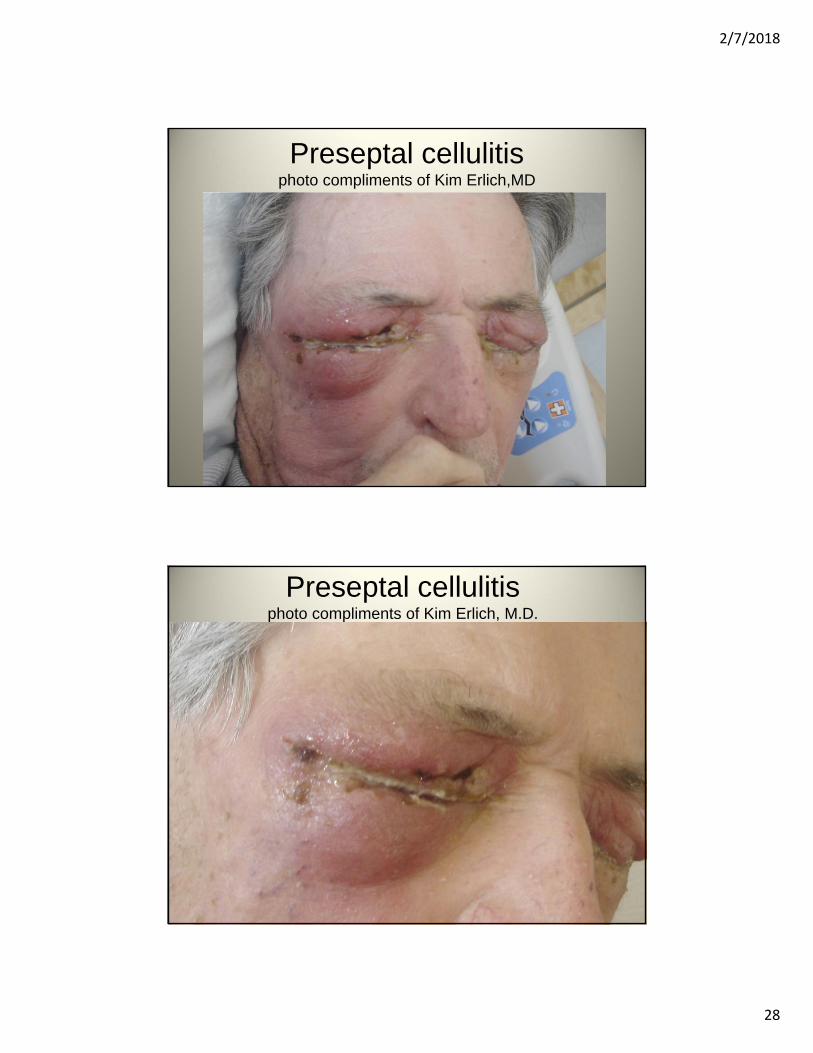
Preseptal cellulitis
• Clinical Symptoms– Lid swelling/eyrthema– EOMI, no pupillary defect– Normal vision
• Pathogens– S. aureus, S. pneumo, H. flu
• Treatment– Amoxicillin-clavulanate
(Augmentin®) +/- Septra– If not better in 48 hours, admit for
IV abxs
2/7/2018
28
Preseptal cellulitisphoto compliments of Kim Erlich,MD
Preseptal cellulitisphoto compliments of Kim Erlich, M.D.
2/7/2018
29
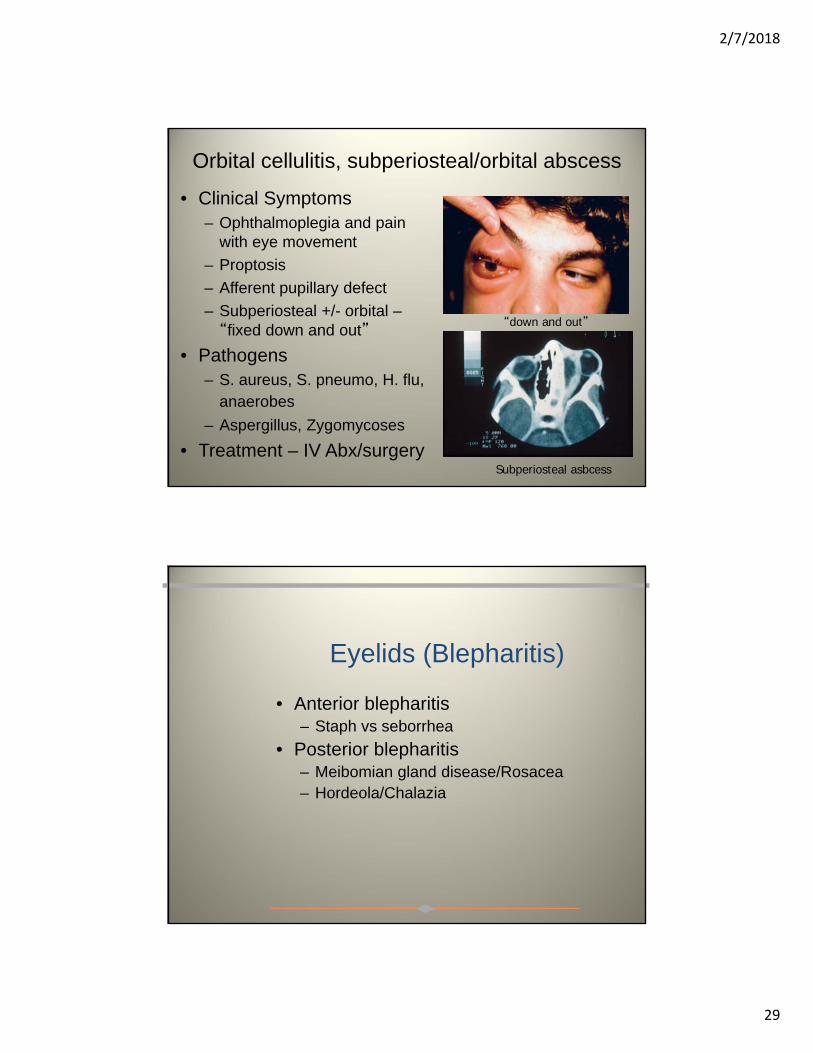
Orbital cellulitis, subperiosteal/orbital abscess
• Clinical Symptoms– Ophthalmoplegia and pain
with eye movement
– Proptosis
– Afferent pupillary defect
– Subperiosteal +/- orbital –“fixed down and out”
• Pathogens– S. aureus, S. pneumo, H. flu,
anaerobes
– Aspergillus, Zygomycoses
• Treatment – IV Abx/surgery
“down and out”
Subperiosteal asbcess
Eyelids (Blepharitis)
• Anterior blepharitis– Staph vs seborrhea
• Posterior blepharitis– Meibomian gland disease/Rosacea– Hordeola/Chalazia
2/7/2018
30
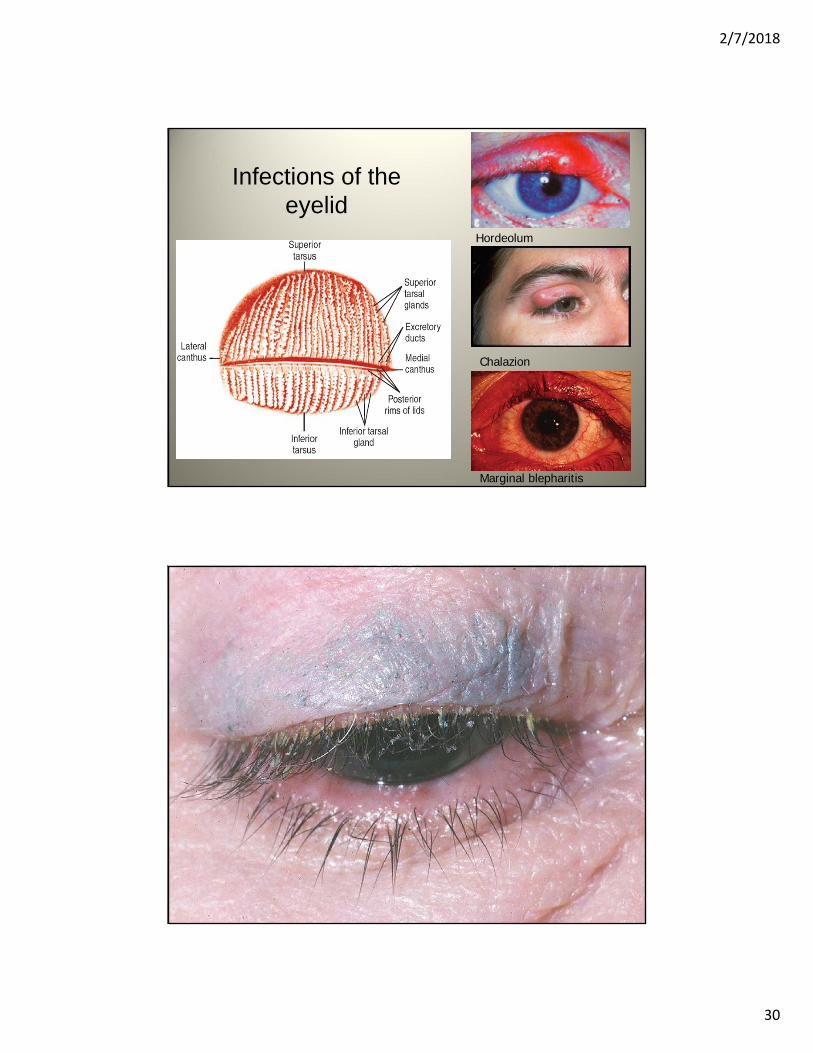
Infections of the eyelid
Hordeolum
Chalazion
Marginal blepharitis

2/7/2018
31

2/7/2018
32
Management of Blepharitis• Anterior Blepharitis
– Lid hygiene– Topical antibiotic ointment applied to lid margins
(erythromycin, bacitracin)
• Posterior Blepharitis– Lid hygiene– Warm compresses (5-10 minutes, 2-4 X/day)/lid
massage– Topical antibiotics (as above)– 1% azithromycin ophthalmic solution– Oral antibiotics (severe cases)
• Doxycycline (50 mg po bid)• “Z-Pak”
• Chalazia– I&D or steroid injection
• LOW THRESHOLD FOR REFERRAL– Chronic disease with multiple recurrences

2/7/2018
33
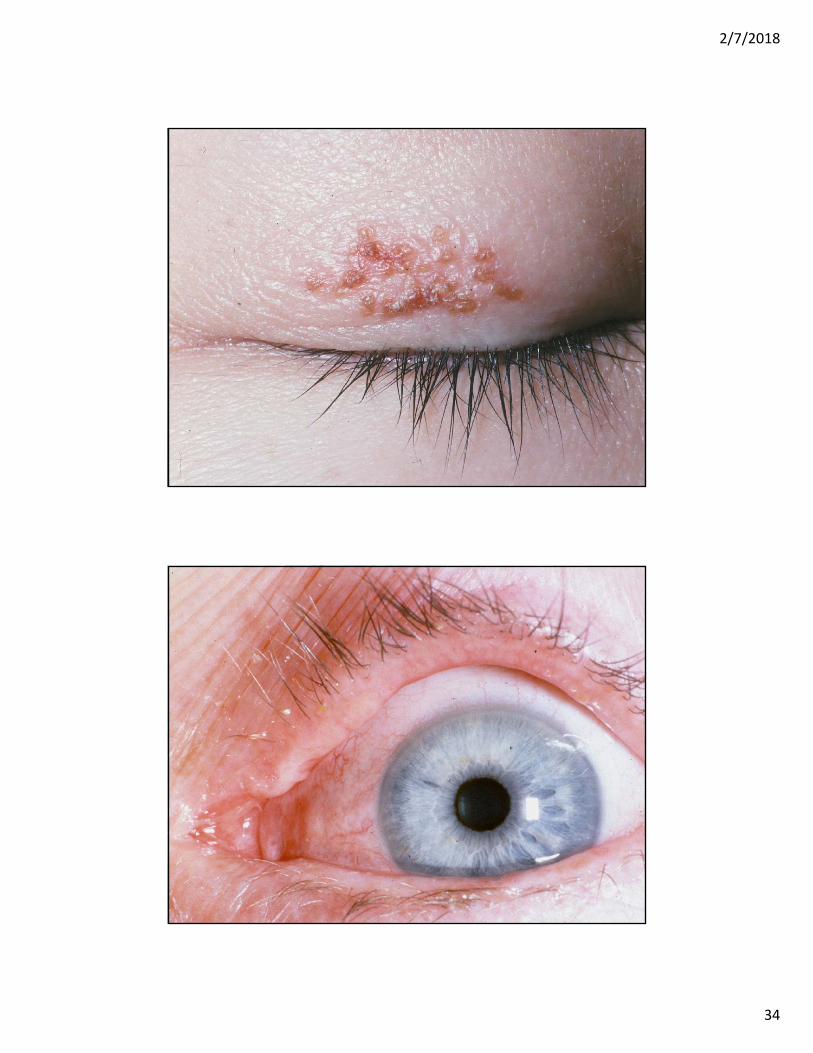
Herpes Infections
Herpes Simplex
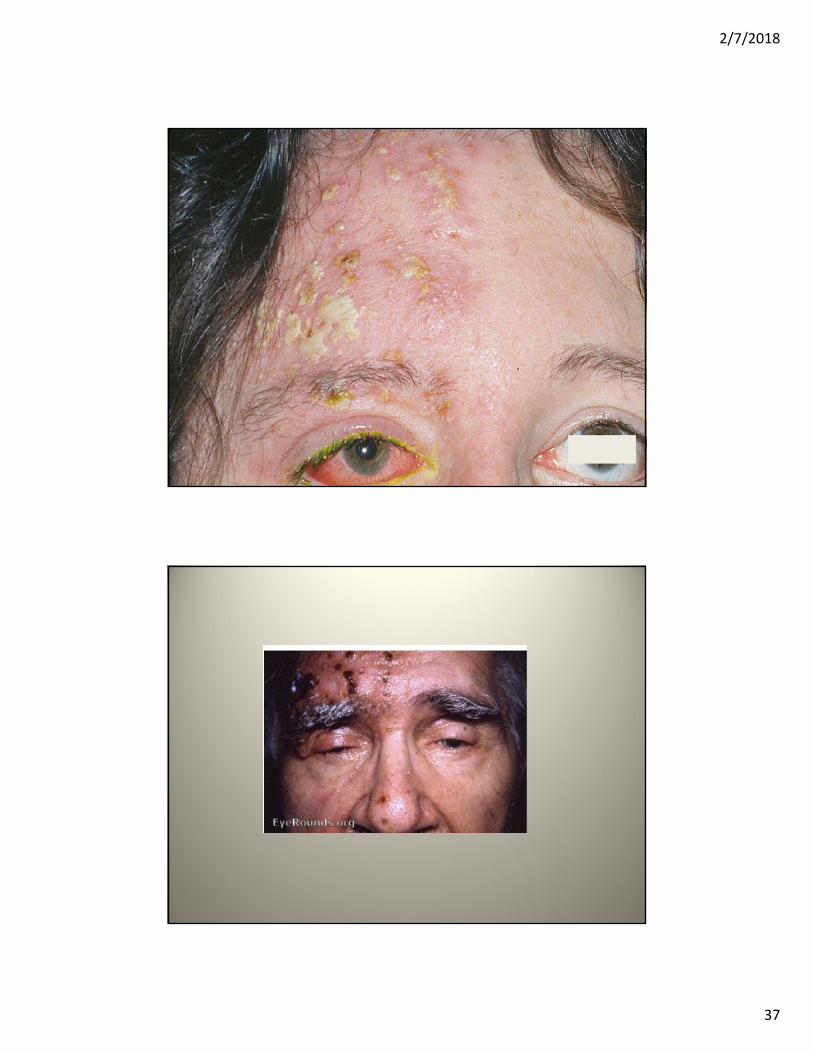
Varicella Zoster
2/7/2018
34

2/7/2018
35
2/7/2018
36
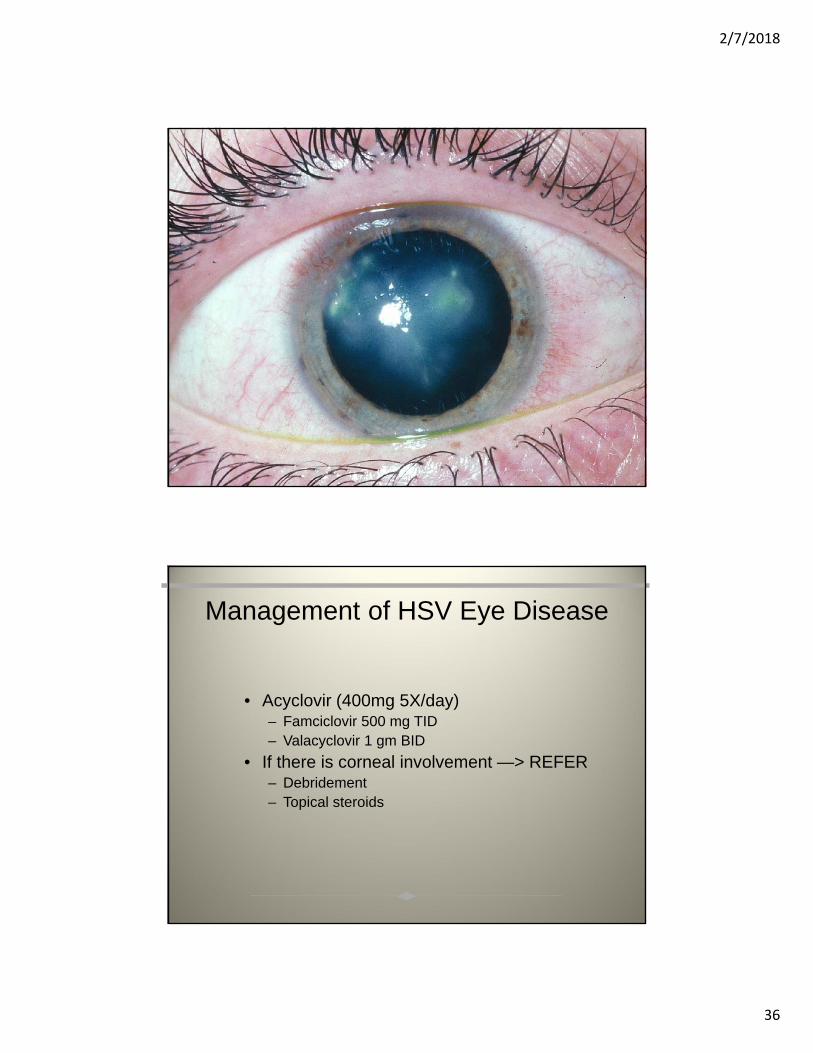
Management of HSV Eye Disease
• Acyclovir (400mg 5X/day) – Famciclovir 500 mg TID– Valacyclovir 1 gm BID
• If there is corneal involvement —> REFER– Debridement– Topical steroids
2/7/2018
37
2/7/2018
38
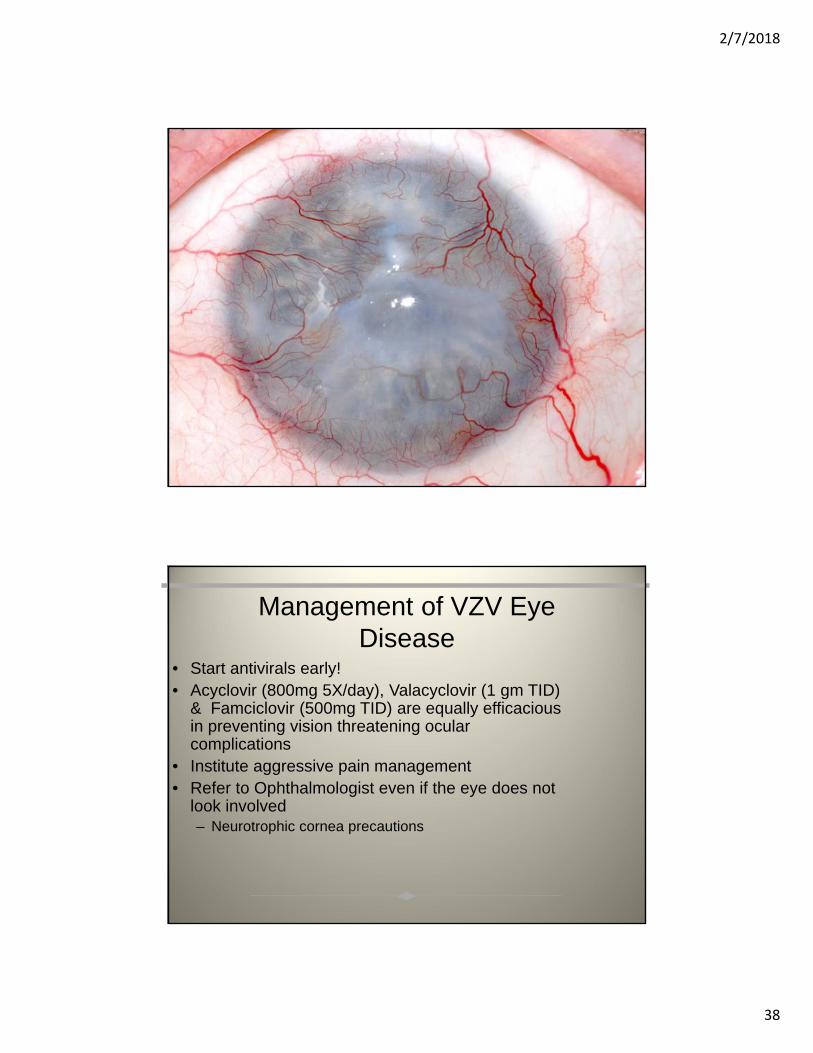
Management of VZV Eye Disease
• Start antivirals early! • Acyclovir (800mg 5X/day), Valacyclovir (1 gm TID)
& Famciclovir (500mg TID) are equally efficacious in preventing vision threatening ocular complications
• Institute aggressive pain management • Refer to Ophthalmologist even if the eye does not
look involved – Neurotrophic cornea precautions
2/7/2018
39
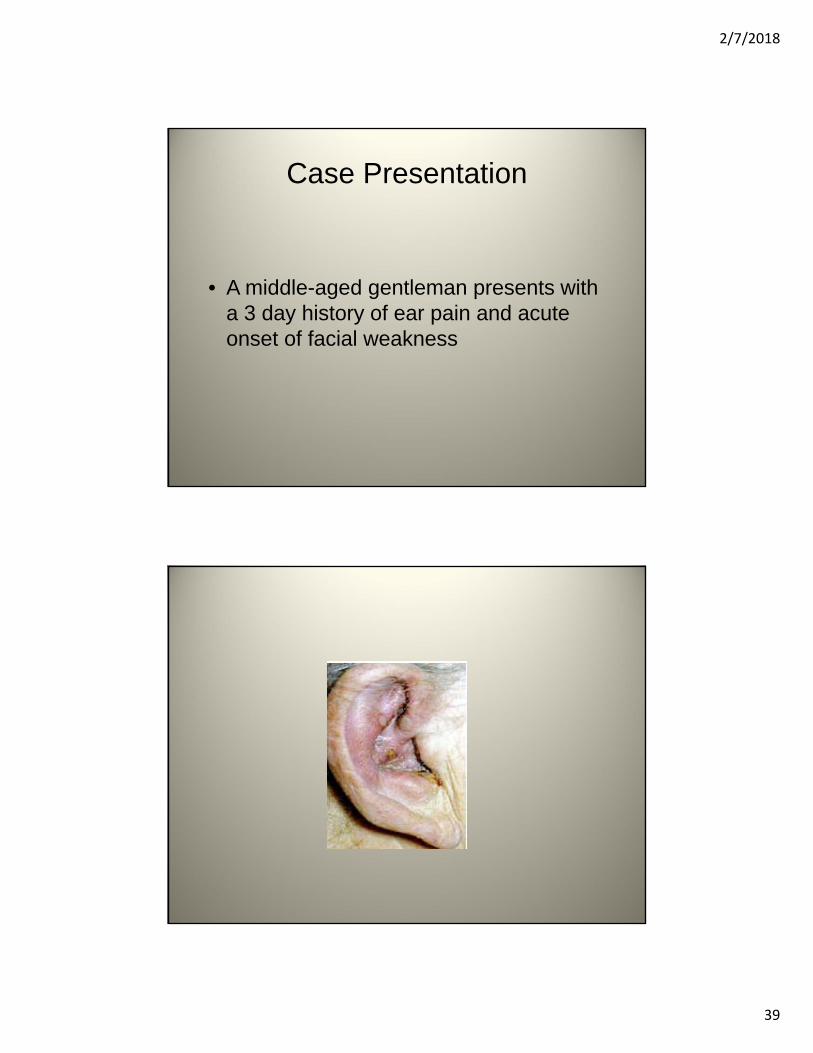
Case Presentation
• A middle-aged gentleman presents with a 3 day history of ear pain and acute onset of facial weakness
2/7/2018
40
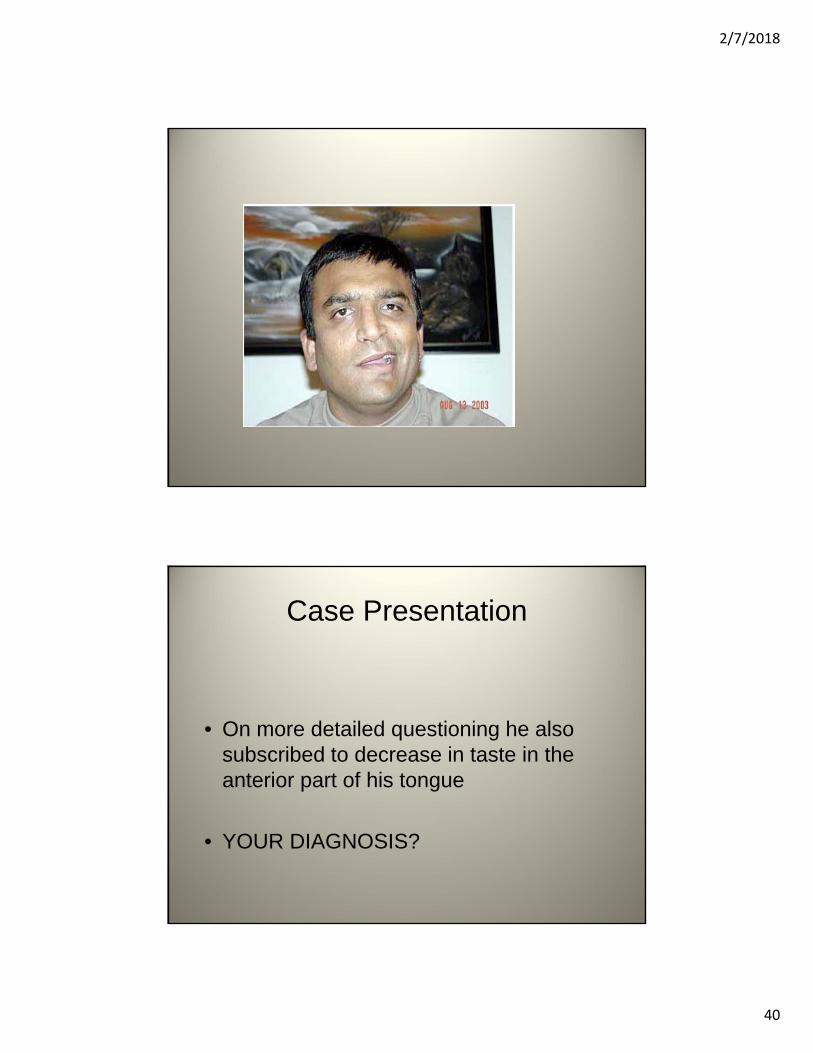
Case Presentation
• On more detailed questioning he also subscribed to decrease in taste in the anterior part of his tongue
• YOUR DIAGNOSIS?
2/7/2018
41
Ramsay Hunt Syndrome
• VZV reactivation in geniculate ganglion– Auricular vessicles
– VIIth nerve palsey
– Loss of taste in anterior two-thirds of tongue
Case Presentation
• A 10 year old girl brought in by her parents complaining of a red eye with with a foreign body sensation for 2‐3 weeks.

2/7/2018
42
Case Presentation
• A 10 year old girl brought in by her parents complaining of a red eye with with a foreign body sensation for 2‐3 weeks.
Case Presentation
• On PE she was found to have
2/7/2018
43
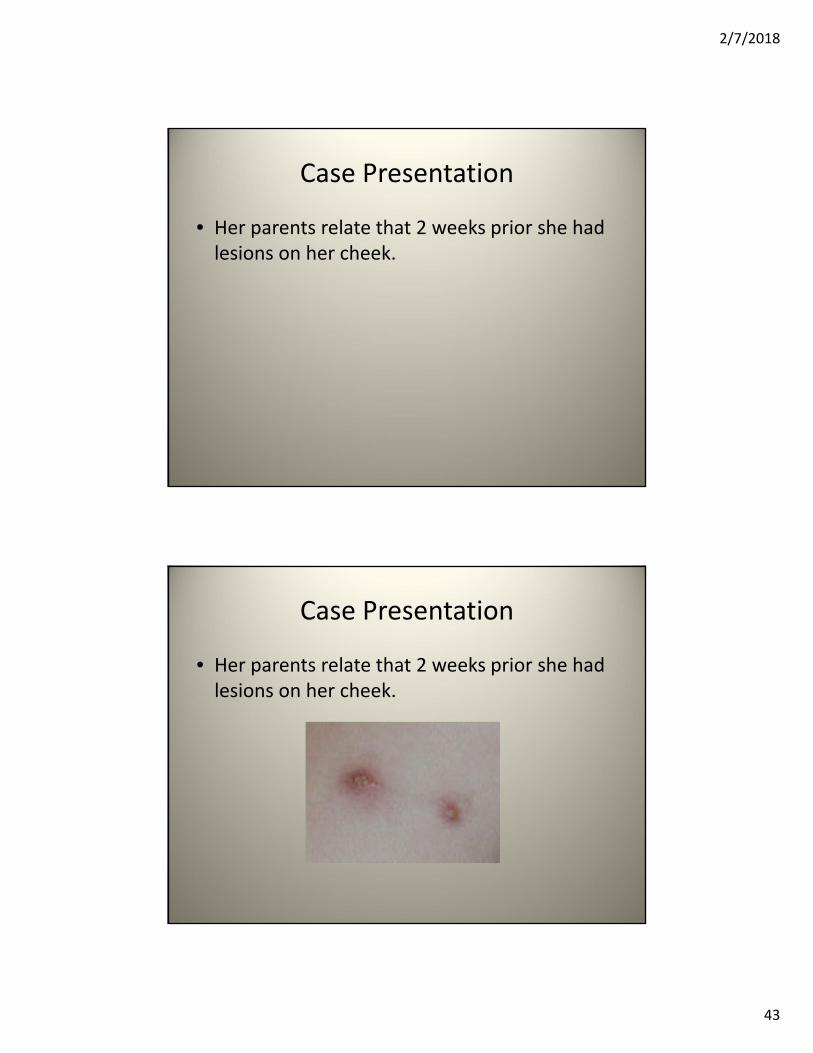
Case Presentation
• Her parents relate that 2 weeks prior she had lesions on her cheek.
Case Presentation
• Her parents relate that 2 weeks prior she had lesions on her cheek.
2/7/2018
44
Case Presentation
• 2 months earlier for her birthday ……………
Case Presentation
• 2 months earlier for her birthday ……………

2/7/2018
45
Parinaud Oculoglandular Syndrome
• Tender regional adenopathy of the preauricular, submandibular or cervical glands
• Associated with infection of the conjunctiva
• Seen in 2‐8% of cases of CSD (B. henselae)







