
11/19/2012
1
Head to Toe Psoriasis, How to Treat ?
Charoen Choonhakarn, MDDivision of Dermatology, Faculty of Medicine
Khon Kaen University
Psoriasis• Chronic inflammatory skin disease, 1-2% of populati on
• Male = female, age at onset 22.5 and 55 yrs
• Trigger: genetic and environment
• HLA association; Cw 6, B13, B17, PSORS 1 and 2
• Mother or father 8-15%, mother and father 40-50%
• Early onset ; clinical more severe, genetic influen ce
• Degree of disability and negative impact on QoL= IH D, DM, cancer
• Severe psoriasis / arthritis : increased risk of CV S disease, DM (metabolic syndrome) , depression
Elder JT, et al. Arch Dermatol 1994. Christophers E. Clin Dermatol 2007. Burden AD, et al. BMJ 2010.
Etiology• Unknown (genetic and environment)
1. Abnormal proliferation and differentiation of keratinocytes
(36 hr. VS 311 hr. of epidermal cell cycle)
2. Immune system
cell - mediated (T helper cell), cytokines, chemokines (TNF , interleukin)
3. Gene (PSORS 1-7)
Bowcock AM and Krueger JG. Nat Rev Immunol ,2005.
Precipitating factor
1. Skin trauma “Koebner phenomenon”
2. Infection
Streptoccous (URI) : guttate type (childhood),
HIV : extensive and sudden onset
3. Stress 30-40%
4. Alcohol drinking, smoking (food?)
5. Drug
chloroquine, beta-blocker, lithium, NSAIDs,
steroid withdrawal : pustular psoriasis
Clinical feature• Skin (head to toe)
Well-demarcated, silvery scale, erythematous on extensor surface
• NailsOil spot, pits, onycholysis, subungual hyperkeratosis
• Joints and enthesopathy Axial or peripheral (small or large joints)

11/19/2012
2
Variation1. Chronic plaque “psoriasis vulgaris”
2. Guttate ; papule
3. Erythrodermic ; diffuse
4. Pustular ; localized or generalized
5. Inverse ; flexural area
Chronic plaque type
Guttate type
Erythrodermic psoriasisPustular type, generalized

11/19/2012
3
Palmoplantar pustular psoriasis
Inverse psoriasis
Psoriasis treatment
• Encourage a healthy lifestyle with regular exercise, weight management, cessation of smoking, and moderation of alcohol consumption
• Encourage patients to be actively involved in their care management
• Discuss treatment options, risk, and benefit with the patients, to be involved in decision making
Psoriasis treatment
1. Mild : BSA ≤ 10%, PASI ≤ 10
Rx- topical therapy or phototherapy
2. Moderate to severe : BSA > 10 %,
PASI > 10, DLQI>10 Rx- phototherapy or systemic therapy
Foulkes AC, et al. Clin Exp Dermatol, 2011, Burden AD, et al. BMJ,2010.
11/19/2012
4
Treatment of psoriasis
• Topical therapyTopical corticosteroid* Calcipotriol*Tazarotene Tars Anthralin Salicylic acid
Immunomodulators
• Systemic therapy• Conventional:
Methotrexate Cyclosporine Acitretin
• Biologics:Etanercept Infliximab Ustekinumab
• PhototherapyNarrow-band UVB PUVA (psoralen-UVA)Excimer laser
*First-line topical therapy
Topical treatment1. Topical glucocorticoids First-line for mild to moderate psoriasis
Improvement within 2-4 wks, maintenance with interm ittent application (weekends)
Good for intertrigenous, genitalia, and pustular ty pe Long-term use increases S/E Tachyphylaxis
2. Vitamin D 3 analogue
Calcipotriol, tacalcitol, maxacalcitol: First-line for mild to moderate psoriasis
Short term: efficacy< potent topical steroids, > an thralin Efficacy not reduced with long term treatment, appl y BID>ODIncreased efficacy by combination with topical ster oidsMinimal S/E in long-term use, hypercalcemia, not ex ceed 100g/wk
Lebwohl and Ali. J Am Acad Dermatol,2001.
Topical treatment3. Tars or liquor carbonis detergents (LCD)
5-20% in cream, ointment, pasteEffective, irritation and bleach cloth and hair, u npleasant odor
4. Anthralin Effective “short contact treatment”
5. Keratolytics salicylic acid, lactic acid, ureaSynergistic effect, enhances absorption of other ag ents
6. Retinoids Tazarotene (0.05, 0.1% gel, cream): Efficacy = moderate potency topical steroids Reduce skin atrophy from topical steroidsS/E irritation, + mid to high-potency topical stero ids
7. Calcineurin inhibitors Tacrolimus (0.03, 0.1% ) Chronic plaque: not effectiveEffective for facial and inverse types psoriasis (black-box warning) Lebwohl and Ali. J Am Acad Dermatol,2001.
Plaque type treatment• Regular application of emollient to reduce scaling
and itch• Short term
- Intermittent potent TC for rapid improvement, avoid regular use of TC for prolonged periods- Combination of calcipotriol and betamethasone dipropionate OD (higher efficacy and more rapid onset of action, QoL>calcipotriol bid)
• Long term- Vitamin D analogue, calcipotriol first, but if this causes troublesome local irritation, switch to an alternative vitamin D analogue - If ineffective or not tolerated consider-coal tar, tazarotene gel, short contact dithranol
Burden AD, et al. BMJ,2010. van de Kerkhof PCM. BJD 2004. Saraceno R, et al. J Dermatol Treat 2007.
van de Kerkhof PCM. BJD 2004.
-828 patients with psoriasis vulgaris :Psoriasis Disability Index, EuroQoL 5D questionnaire and visual analogue scale (VAS)-The TCP used once or twice daily and calcipotriol used twice daily (4 wks)were found to have statistically significant beneficial effects on patients’ QoL over vehicle. -The TCP, applied once daily, was superior to calcipotriol twice daily in terms of reductions on the EuroQoL questionnaire and VAS
Combination of calcipotriol and betamethasone
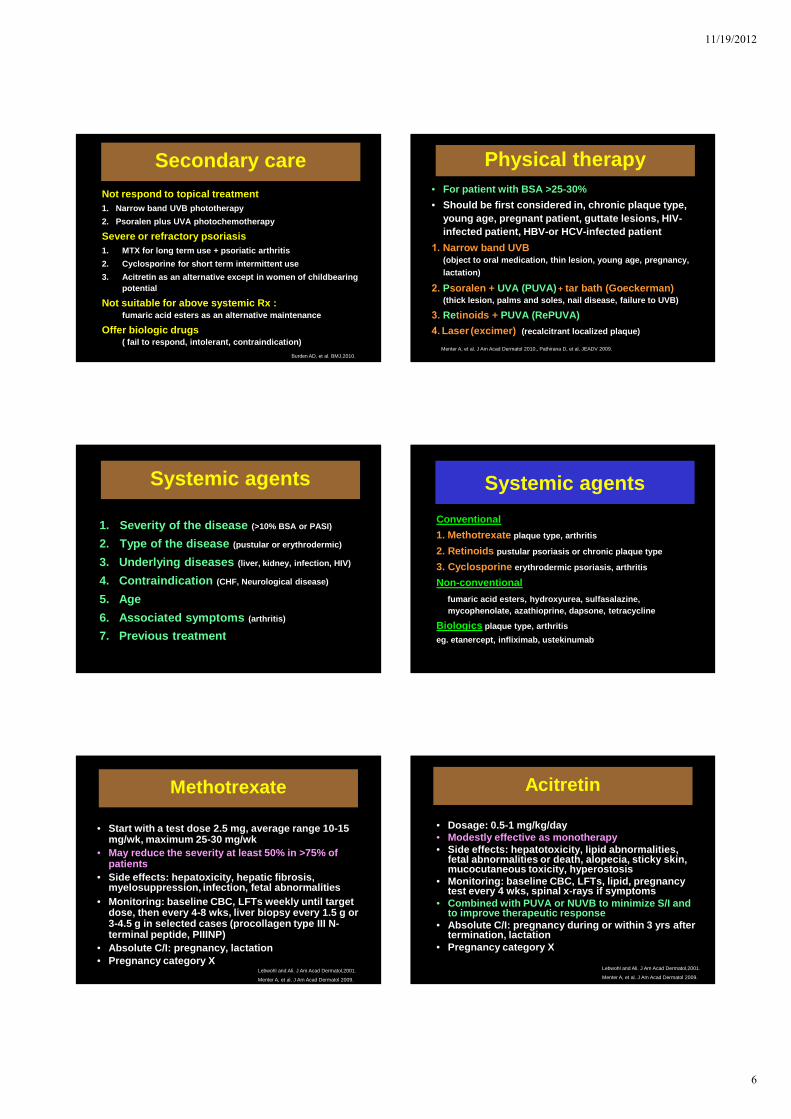
Sequential therapy
Phase Vitamin D3 analogue
Topical steroids class I
Clearance
2-4 weeks
bid od or bid
Transition1-6 months
bid weekday
bid weekend
Maintenanceuntil remission and prevent relapse
bid none
Burden AD, et al. BMJ,2010.

11/19/2012
5
Scalp treatment• Mild case :
Tar or keratolytic shampoo • Moderate to severe case :
Intermittent potent TC ( lotion, solution, foam, g el ) Combination of calcipotriol and betamethasone dipropionate OD ( improvement QoL, quick onset of improvement )
Overnight application of salicylic acid or oil preparation (olive or coconut oil) to remove thick scale
• Recalcitrant case :Phototherapy: ultraviolet comb, excimer laser (UVB 308 nm)Systemic therapy
Burden AD, et al. BMJ,2010. Ortonne JP, et al. JEADV 2009. Mrowietz U, et al. J Dtsch Dermatol Ges.2011.
Combination of calcipotriol and betamethasone, scalp preparation
• 721 patients with scalp psoriasis received calcipotriol 50 µg/g, betamethasone 0,5 mg/g topically for 4 weeks
• Severity was assessed by physician’s global assessment (PGA) and QoL by using a scalp-specific questionnaire
Results• Mean PGA improved from 4.26 to 2.49 (–41.8 %,
p < 0.0001)• QoL improved from 10.57 to 3.22 (–69.5 %,p < 0.0001)• Among patients with pretreatment 89.5 % of patients and
87.9 % of dermatologists judged treatment response to this combination as better/much better compared to previous therapy
Mrowietz U, et al. J Dtsch Dermatol Ges.2011.
Mrowietz U, et al. J Dtsch Dermatol Ges.2011.
Ortonne JP, et al. JEADV 2009.
Facial / flexural psoriasis treatment
• Moderate potency TC (1st line short term use)
• Vitamin D analogue• Tacrolimus ointment• Avoid dithranol, topical retinoids
Burden AD, et al. BMJ,2010.
Nail signs /anatomic site / treatment
Nail bed psoriasis Nail matrix psoriasisOnycholysis Splinter hemorrhagesOil drop (salmon patch)Nail bed hyperkeratosis
PittingLeukonychiaRed spots in the lunulaNail plate thickening / crumbling
Cacipotriol ointmentTopical corticosteroids (+keratolytics)Systemic therapy
Topical corticosteroidsCalcipotriol TarzaroteneSteroid injectionSystemic therapy
Burden AD, et al. BMJ,2010. Lebwohl and Ali. J Am Acad Dermatol,2001.
11/19/2012
6
Secondary care
Not respond to topical treatment1. Narrow band UVB phototherapy
2. Psoralen plus UVA photochemotherapy
Severe or refractory psoriasis1. MTX for long term use + psoriatic arthritis
2. Cyclosporine for short term intermittent use
3. Acitretin as an alternative except in women of ch ildbearing potential
Not suitable for above systemic Rx :fumaric acid esters as an alternative maintenance
Offer biologic drugs( fail to respond, intolerant, contraindication)
Burden AD, et al. BMJ,2010.
Physical therapy• For patient with BSA >25-30%
• Should be first considered in, chronic plaque type, young age, pregnant patient, guttate lesions, HIV-infected patient, HBV-or HCV-infected patient
1. Narrow band UVB
(object to oral medication, thin lesion, young age, pregnancy,
lactation)
2. Psoralen + UVA (PUVA) + tar bath (Goeckerman)(thick lesion, palms and soles, nail disease, failu re to UVB)
3. Retinoids + PUVA (RePUVA)
4. Laser (excimer) (recalcitrant localized plaque)
Menter A, et al. J Am Acad Dermatol 2010., Pathirana D, et al. JEADV 2009.
Systemic agents
1. Severity of the disease (>10% BSA or PASI)
2. Type of the disease (pustular or erythrodermic)
3. Underlying diseases (liver, kidney, infection, HIV)
4. Contraindication (CHF, Neurological disease)
5. Age
6. Associated symptoms (arthritis)
7. Previous treatment
Systemic agents
Conventional
1. Methotrexate plaque type, arthritis
2. Retinoids pustular psoriasis or chronic plaque type
3. Cyclosporine erythrodermic psoriasis, arthritis
Non-conventional
fumaric acid esters, hydroxyurea, sulfasalazine, mycophenolate, azathioprine, dapsone, tetracycline
Biologics plaque type, arthritis
eg. etanercept, infliximab, ustekinumab
Methotrexate
• Start with a test dose 2.5 mg, average range 10-15 mg/wk, maximum 25-30 mg/wk
• May reduce the severity at least 50% in >75% of patients
• Side effects: hepatoxicity, hepatic fibrosis, myelosuppression, infection, fetal abnormalities
• Monitoring: baseline CBC, LFTs weekly until target dose, then every 4-8 wks, liver biopsy every 1.5 g or 3-4.5 g in selected cases (procollagen type III N-terminal peptide, PIIINP)
• Absolute C/I: pregnancy, lactation• Pregnancy category X
Lebwohl and Ali. J Am Acad Dermatol,2001.
Menter A, et al. J Am Acad Dermatol 2009.
Acitretin
• Dosage: 0.5-1 mg/kg/day• Modestly effective as monotherapy• Side effects: hepatotoxicity, lipid abnormalities,
fetal abnormalities or death, alopecia, sticky skin , mucocutaneous toxicity, hyperostosis
• Monitoring: baseline CBC, LFTs, lipid, pregnancy test every 4 wks, spinal x-rays if symptoms
• Combined with PUVA or NUVB to minimize S/I and to improve therapeutic response
• Absolute C/I: pregnancy during or within 3 yrs afte r termination, lactation
• Pregnancy category X
Lebwohl and Ali. J Am Acad Dermatol,2001.
Menter A, et al. J Am Acad Dermatol 2009.

11/19/2012
7
Cyclosporin A
• High-dose approach : 5 mg/kg/day then tapered• Low-dose approach : 2.5 mg/kg/day, increase every 2-4
wk up to 5 mg/kg/day• Very effective, up to 90% of patients achieve
clearance or marked improvement• Side effects: nephrotoxicity, HT, immunosuppression ,
increase risk of malignancy if before PUVA• Monitoring: BP, CBC, BUN/Cr, Mg, uric acid, every 4 -8
wks• Absolute C/I: uncontrolled HT, abn. renal function,
history/current malignancy• Intermittent short-course safer than chronic long-t erm
use• Pregnancy category C
Lebwohl and Ali. J Am Acad Dermatol,2001.
Menter A, et al. J Am Acad Dermatol 2009.
Fumaric acid esters
• Initiate at low dose and escalate dose weekly, maximum 1.2 g/day
• 80% mean reduction in PASI• Side effects: GI symptoms, diarrhea, flushing,
headache, lymphopenia, acute renal failure• Absolute C/I: chronic disease of GI and kidney,
pregnancy, lactation• Not US FDA approved, widely use in Europe• Pregnancy category C
Lebwohl and Ali. J Am Acad Dermatol,2001.
Hydroxyurea
• 500 mg daily, 1.0-1.5 g daily based on response• 85 patients with chronic plaque, 61% of patients
had satisfactory remission• Side effects: BM suppression, teratogenicity,
mutagenicity, skin rash• Monitoring: CBC, Blood chemistry, LFTs, every 2-
4 wks, hold dosage if severe anemia, WBC<2,500 or platelet< 100,000
• Absolute C/I: prior BM depression, pregnancy, lactation
• Pregnancy category D
Lebwohl and Ali. J Am Acad Dermatol,2001.
Mycophenolate mofetil
• Initiated at 500-750 mg bid, then 1.0-1.5 g bid
• Appears to be only moderately effective• Side effects: GI (constipation, diarrhea,
N/V), myelosuppression, HT, edema• Monitoring: BP, CBC, blood chemistry,
weekly x 6 wk, every 2 wk x 2mo, then monthly
• Absolute C/I: severe infection, malignancy• Pregnancy category C
Lebwohl and Ali. J Am Acad Dermatol,2001.
Sulfasalazine
• Starting dose 500 mg tid, if tolerated after 3 d, 1 g tid, if tolerated after 6 wk, 1 g qid
• Appears to be moderately effective• Side effects: headache, N/V, rash, pruritus,
hemolytic anemia• Monitoring: CBC, blood chemistry, G6PD, CBC +
blood chemistry weekly x 1 mo, every 2 wk x 1 mo, monthly x 3 mo, then every 3 mo
• Absolute C/I: hypersensitivity to sulfasalazine, sulfa drugs, salicylates, porphyria, intestinal urinar obstruction, G-6-PD def.
• Pregnancy category C
Lebwohl and Ali. J Am Acad Dermatol,2001.
Biologics
• Induction of clearance (short-term efficacy):infliximab is the most effective (80% of pts achieving a PASI-75 at wk 10, adalimumab (71-79% at wk16), etanercept (34% 25 mg twice a wk, 49% 50 mg twice a wk at wk 12)
• After wk 12 : initial response rates are maintained by infliximab and adalimumab but tend to increase moderately with etanercept
• Long-term efficacy : etanercept (50 mg twice a wk) peaked at wk 48 with PASI-75 in 63%, decrease to 52% by wk 96, infliximab (every 8 wk) 80% with PASI-75 at wk 24, decrease to 60.5% at wk 50
Menter A, et al. J Am Acad Dermatol 2009., Pathirana D, et al. JEADV 2009.

11/19/2012
8
Biologics
• Intermittent therapy: rebound phenomenon• Approved for chronic plaque type and
arthritis• Combination with oral systemic agents:
methotrexate (FDA-approved for arthritis)• Reactivation of latent infection, induction or
exacerbation of demyelinating disease, worsening cardiac failure, anaphylaxis (infliximab) 10%
• Pregnancy category B (efalizumab C)
Menter A, et al. J Am Acad Dermatol 2009., Pathirana D, et al. JEADV 2009.
New biologics
• Ustekinumab : human IgG monoclonal Ab to p40 subunit of IL-12 and IL-23
• PHOENIX 1 and 2 : 45 and 90 mg SC at wk 0, 4 and every 12 wks
• PASI-75: 67.1% vs 66.4% at wk 12, 76.1% vs 85% at wk 24
• ACCEPT study : ustekinumab and etanercept 50 mg SC 2 times/wk
• PASI-75 : 67.5% (45 mg), 73.8% (90 mg), 56.8% (etanercept)
Menter A, et al. J Am Acad Dermatol 2009., Pathirana D, et al. JEADV 2009.
Biologics
Infliximab Etanercept Ustekinumab
Mechanism Chimeric monoclonal Ab for TNF-alpha
Human recombinant for TNF-alpha receptor
Human monoclonal Ab to IL-12, Il-23
Dosing 5 mg/kg IV infusions at wk 0,2,6, every 8 wk
25-50 mg SC twice weekly
45 and 90 mg SC at wk 0, 4 and every 12 wks
Efficacy PASI-75 wk 10, 82%, wk 26, 50%
PASI-75 wk 12, 34%, wk 24, 44%
PASI-75 wk 12, 67%, wk 24, 76%
Safety Serious infection, TB, MS, malignancy, heart failure
Serious infection, TB, MS, malignancy, heart failure
Serious infection, TB, malignancy
Pregnancy B B -
Pathirana D, et al. JEADV 2009. Week 0 Week 10
Infliximab significantly improves psoriasis
Infliximab significantly improves psoriasis
“Rotational therapy”
“ Combination therapy”
Response
Non response

11/19/2012
9
Combination systemic therapy
Combination Recommendation Comments
Phototherapy + retinoids ++ Increased efficacy
Phototherapy + MTX + Increased phototoxicity
Biologics + MTX + Depending on biologics
Biologics + Cyclosporin + Depending on biologics
Biologics + retinoids + Depending on biologics
Phototherapy + cyclosporin - Increased risk of SCC
Cyclosporin + MTX - Increased immunosuppression but possible
Retinoids + MTX - Increased hepatotoxicity
Retinoids + cyclosporin - No evidence of increased efficacy
Pathirana D, et al. JEADV 2009.
Women of child-bearing potential and during pregnancy
• Avoid MTX (fetotoxic, abortifactant) and retinoids (teratotoxins)
• In selected cases: isotretinoin may be preferred, s hort half-life• Improvement or remission during pregnancy• If needed: emollients or topical treatments• Topical steroids and calcipotriol: pregnancy catego ry C,
caution should be exercised• Several biologics (category B) can be used in pregnancy• Cyclosporin (category C) and nonteratogenic• PUVA and UVB appear to be safe
Menter A, et al. J Am Acad Dermatol 2009.
Children
• First-line: Topical treatments, UVB• PUVA is generally contraindicated
(carcinogenic risk)• Systemic agents: MTX or cyclosporin
or biologics
Menter A, et al. J Am Acad Dermatol 2009., Pathirana D, et al. JEADV 2009.
Patients with HIV infection
• More severe and refractory to traditional treatment s• Many have significant psoriatic arthritis• Many effective drugs for psoriasis are immuno
suppressive • First-line for mild to moderate: Topical treatments• First-line for moderate to severe: phototherapy and
antiretrovirals, second-line : oral retinoids• More refractory, severe: cautious use of
cyclosporin, MTX, hydroxyurea and anti-TNF• Regular monitoring of CD4 counts and HIV viral
loads
Menon K, et al. J Am Acad Dermatol 2009.
Patients with hepatitis C • Exacerbated by interferon therapy• Psoriasis therapies are potentially hepatotoxic,
immunosuppressive• Mild to moderate:
first-line: topical treatments second-line : ultraviolet B phototherapy
• Moderate to severe:first-line: ultraviolet B phototherapy + topical therapies, second-line : oral retinoids, etanercept, infliximab,
adalimumab, PUVAthird-line : cyclosporin, alefacept, efalizumab,
azathioprine• Contraindicated: MTX, MMF
Frankel AJ, et al. J Am Acad Dermatol 2009.
Menter A, et al. J Am Acad Dermatol 2011.

11/19/2012
10
Menter A, et al. J Am Acad Dermatol 2011.
Males Females
Menter A, et al. J Am Acad Dermatol 2011.
THANK YOU







