doppler of carotid artery assessment in evaluation …
TRANSCRIPT

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1877
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
DOPPLER OF CAROTID ARTERY ASSESSMENT IN EVALUATION
OF PATIENTS INDICATED FOR CORONARY ARTERY BYPASS
GRAFT
Dr. Farah Abdul- Khalik Zaki* and Dr. Hana Abdul Ridha Ali AL.Dynori
1,2
M.B.Ch.B, MDRD.
ABSTRACT
Background: Atherosclerosis is a generalized disease, mainly
manifested in all vascular trees. An association between carotid artery
stenosis and coronary artery disease has been well established. Carotid
artery stenosis is an important etiologic factor for cerebrovascular
accidents, is associated with coronary artery disease. Methods: A
prospective study of 86 patients, who were scheduled for CABG, was
done at radiology department, Medical city Baghdad, Gazzi Al-Harirri
hospital from Nov.2016 to July 2017. The majority were males, (73)
and (13) were Females. All patients, after a clinical history was taken
by the cardiac surgery team, they underwent a physical examinations, and investigations;
chest x-ray, ECG, blood was taken for fasting blood suger and cholesterol study, Doppler
ultrasonography for bilateral carotid arteries were performed by aspescailized radiologist for
carotid artery atherosclerosis. Results: The majority of the patients were above 50 years of
age, 73 patients (84.45%) and only 15% were below the age of 50 years. ale affected by
carotid artery atherosclerosis, (76.7%) more than females above the age of 50 years, while
below the age of 50 years females (46.7%) more affected than males (9.58%). Risk factors
were significantly correlated with both carotid and coronary artery stenosis like age, sex,
smoking hypertension, cholesterol and diabetes mellitus. Doppler Ultrasonography was
performed to screen the presence of carotid artery stenosis. Carotid artery atherosclerosis was
present in 66 patients, (76.7%). Ten patients (15.1%) with one coronary artery disease,
17(25.75%) with two coronary artery disease, and 39 patients (59.09%) with three coronary
artery disease. The location of atherosclerosis is mostly in ICA, (53%), of which 15% in the
bulb, in the CCA (32%). Conclusions: Our finding indicated significant associations between
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.632
Volume 10, Issue 6, 1877-1900 Research Article ISSN 2278 – 4357
*Corresponding Author
Dr. Farah Abdul- Khalik
Zaki
M.B.Ch.B, MDRD.
Article Received on
20 April 2021,
Revised on 10 May 2021,
Accepted on 31 May 2021
DOI: 10.20959/wjpps20216-18968

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1878
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
carotid artery atherosclerosis and coronary artery disease. There is strong association between
increase in intma media thickness of carotid arteries and the presence of coronary artery
disease.
INTRODUCTION
Doppler ultrasound is the most common technology used for evaluation and characterization
of blood vessels, the Doppler effect was named after Christian Johann Doppler (1803_1853),
an Austrian mathematician and physicist, who theorized that the sound waves from a moving
source would be closer together as the sound came closer (have a higher pitch), and further
apart as the sound went away (lower pitch).
It’s a real time imaging technique with no risk of radiation.[1]
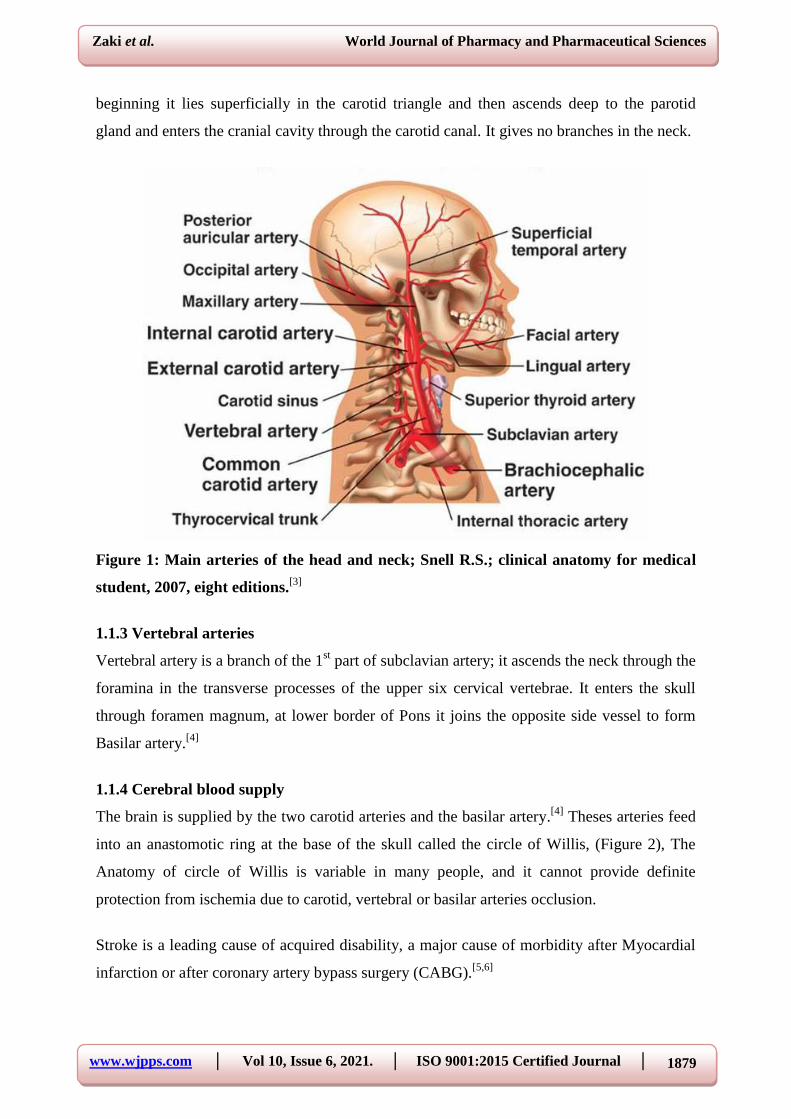
1. 1. Anatomy of the carotid arteries
There are two main arteries, the common carotid arteries on both side of the neck, Figure (1).
The right common carotid artery arises from brachiocephalic artery behind the right
sternoclavicular joint; the left common carotid arises from aortic arch in the superior
mediastinum. Each common carotid artery runs upward through the neck, from the
sternoclavicular joint to the upper border of the thyroid cartilage, where it divides into the
external and internal carotid arteries. At its point of division the common carotid artery shows
a localized dilatation, having thin tunica media but thick tunica adventitia, it is called carotid
sinus.[2]
1.1.1 External carotid artery
It is one of the terminal branches of the common carotid artery, it supplies structures in the
neck face, scalp. And also supplies the tongue and the maxilla. At its origin where its
pulsation can be felt, the artery lies within the carotid triangle, medial to the internal carotid
artery as it Ascends in the neck, it passes backward and laterally.
It gives many branches, to the thyroid gland, lingual, facial, and to the scalp.[3]
1.1.2 Internal carotid artery
It is one of the terminal branches of common carotid artery, the artery begins at level upper
border of the thyroid cartilage and ascends in the neck to the base of the skull, and it enters
the cranial cavity through the cranial canal in the petrous part of temporal bone it lies
embedded in the carotid sheath with the internal jugular vein and vagus nerve. At its
www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1879
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
beginning it lies superficially in the carotid triangle and then ascends deep to the parotid
gland and enters the cranial cavity through the carotid canal. It gives no branches in the neck.
Figure 1: Main arteries of the head and neck; Snell R.S.; clinical anatomy for medical
student, 2007, eight editions.[3]
1.1.3 Vertebral arteries
Vertebral artery is a branch of the 1st part of subclavian artery; it ascends the neck through the
foramina in the transverse processes of the upper six cervical vertebrae. It enters the skull
through foramen magnum, at lower border of Pons it joins the opposite side vessel to form
Basilar artery.[4]
1.1.4 Cerebral blood supply
The brain is supplied by the two carotid arteries and the basilar artery.[4]
Theses arteries feed
into an anastomotic ring at the base of the skull called the circle of Willis, (Figure 2), The
Anatomy of circle of Willis is variable in many people, and it cannot provide definite
protection from ischemia due to carotid, vertebral or basilar arteries occlusion.
Stroke is a leading cause of acquired disability, a major cause of morbidity after Myocardial
infarction or after coronary artery bypass surgery (CABG).[5,6]

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1880
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
The incidence of cerebral infarction after CABG is 2% Cerebral ischemia and infarction, after
CABG, is mostly due to carotid plaque or intra cardiac clot and decrease in perfusion
pressure to below 60 mm Hg, are the possible cases of stroke associated with CABG.[7]
Detecting carotid stenosis due to atherosclerosis in patient undergoing CABG is important,
by using Doppler ultrasonography to diagnose the atherosclerosis preoperatively and
managed at same time of CABG surgery or soon later.[8-10]
Urgent evaluation after stroke is needed because many recurrent events occur, brain imaging,
using MRI, and arterial imaging with the use of carotid ultrasound are mandatory for
diagnosis and management.[11]
1.2 Associations between coronary artery and carotid atherosclerosis
Studies by many authors have found an associations between symptoms and signs of carotid
artery disease and coronary artery atherosclerosis, also have shown an increased risk of
cerebrovascular stroke and statistically significant correlations between atherosclerosis of the
coronary artery and carotid artery have been noted in there study.[5,12,13,14]
1.2.1 Risk factors of carotid atherosclerosis
It is very important to find carotid atherosclerosis by using Doppler ultrasound before CABG
surgery, also it is mandatory to know history of peripheral arterial diseases, a cervical bruit
and age of the patient (50-70) all are strong predictor of carotid artery atherosclerosis. It was
found that carotid stenosis was closely related to the occurrence of stroke post CABG surgery
being both as an independent risk factor for and the cause of significant proportion of
stroke.[11,14,15]
1.2.2 The risk factors
1- Age and sex (old age, male sex is at more risk).
2- Family history (patient with positive family history of coronary artery disease are at more
risk).
3- Smoking.
4- Hypertension.
5- Hyperlipidemia
6- Diabetes mellitus.

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1881
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
7- Obesity and physical activity (obese patient and those with low active life style like bed
ridden is at more risk of developing atherosclerosis).
8- Excessive alcohol.
The risk factors are variable for each patient. However there are, three important risk factors
are appropriate for nearly all the patients; High blood pressure, High cholesterol and long
duration of smoking.[11,15]
Figure 2: circle of Willis; courtesy of Clifford –jones (radiology handbook of clinical
medicine).[4]
1.2.3 Pathophysiology of atherosclerosis
It is a progressive inflammatory process of arterial wall, atherosclerosis begins early in life.
The causes are unknown; the response to injury is the most accepted hypothesis.
At the sites of arterial stress such as bifurcation of the artery, fatty streaks occurs associated
with abnormal endothelial function, the Monocytes bind to receptor and migrate into intimae.
Take up low density lipoprotein (LDL), and become foam Cells or macrophages, when the

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1882
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
foam cells die release their lipid contents and Lipid pool appear in the intimae. The smooth
muscle cells migrate from the media to the intimae in response to cytokines and growth factor
produced by macrophages, the lipid will be covered by smooth muscle and matrix, producing
atherosclerotic plaque.[17]
Due to effect of cytokines such as interleukin-1, interferon and other factors, the plaque
become active and complicated by ulceration and thrombus formation (Figure 3), The plaque
will expose to the mechanical stress, this lead to fissuring or rupture of the plaque, that lead
to aggregation of platelets and thrombosis, this may cause partial or complete occlusion of
arterial lumen, or distal embolization.[18,19,20,21,22]
Figure 3: Pathogenesis of atheroma.[19]
1.3 Carotid Doppler ultrasound overview
Carotid Doppler ultrasound is a useful diagnostic tool for assessing cervical carotid artery
disease.[6]
It is an imaging test that uses ultrasound to examine carotid arteries in the neck, the
test can show narrowing or blockage due to plaque buildup in association with coronary
artery disease, it is highly reliable has no radiation risk, Well tolerated by all patients
including those who are phobic in MRI machine.[11,19,23]
It relies on the properties of longitudinal sound waves, Doppler ultrasound of 2 Steps
procedure, the 2 steps are first is imaging then spectral analysis.[24]
www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1883
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
1.3.1 Physics and hemodynamics[25,26]
A- Pulse echo technique used to image the vessel
1. An initial signal (pulse), is generated in the computer, sent through the transducer on the
patient’s neck, and then bounced off a variety of tissues boundaries.
2. The transducer detects a returning signal (echo).
3. The direction of the pulse and the time elapsed until the signal return, determine the
position of tissues boundary.
4. The echogenicity of an object on the image determines its brightness. Changes in the
plaque echogenicity as measured by the quantitative computer assisted ultrasound index
in some ultrasound machines could be a marker of plaque instability as well as an
indicator of plaque remodeling, thereby providing the means for monitoring anti-
atherosclerosis drugs.
5. An object that rebounds very little of the pulse such as fluid in a cyst is hypoechoic.
6. An object that rebounds much of the signal like heavily calcified plaque, is Hyperechoic.
7. Evaluation of intima media thickness.
8. Flow direction demonstrated in colored modality and in spectral waveform.[24,27]
B-Hemodynamic
1- The velocity changes on spectral analysis reflect the changes in hemodynamics.
2- The greater the degree of stenosis, the higher the velocity.
C- Doppler phenomenon used to assess the velocity of the blood as it moves past the
vessel.[28,30]
1.3.2 Mathematical basics in Doppler ultrasounds
Transducer produces an increase in the reflected ultrasonic frequency of the RBCS that
moves towards the probe, whereas motion a way gives a reduction in the frequency. The
system electronic note whether the detected ultrasound has a higher or lower frequency than
that transmitted and hence extracts information on the direction of motion relative to the
transducer.
When the line of movement of the reflector is at an angle Ө to the transducer beam, then the
Doppler shift, ƒƊ.
The Doppler is shift there for:
ƒḎ=ƒt-ƒʳ =ƒt.2.u.cosӨ/c
www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1884
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
Doppler frequency (fd) =2.F1.V.COSӨ/C
FD= Doppler shift
F1=transmitted beam
C = speed of sound in tissue
V= velocity of blood
Ө=angle of incidence between the ultrasound beam and the direction of the objected RBCs.
The value of (c) differs from medium to medium but always constant in particular medium.
In tissue the value of (c) for ultrasound is 1540 m/s. Because c is constant, the wave length
increases as the frequency decreases; the converse is also true.[30]
Frequency is measured in cycle per second, called hertz (Hz). In ultrasounds the emitted
frequency is millions of cycles per second, therefore, it is measured in megahertz (MHz), the
Doppler shift is 1000 fold less than the emitted frequency therefore, it is measured in
kilohertz (kHz), and it’s with in audible range that’s why we can hear it.
Sometime the term spatial pulse length (SPL) is used; it is equal to the number of cycles in a
pulse multiplied by wave length. It is important in determining Resolution.[28,30]
1.3.3 Tissue attenuation
As ultrasound passes through tissue some of the signal is lost through scattering, reflection,
and absorption in tissue, attention = 0.5 x frequency x path length, decibels (dB). There for
the higher the frequency the greater the attenuation and the less can be imaged at greater
distance from the probe, on other hand, higher frequencies means shorter wavelength and
better resolutions.[31-34]
1.3.4 Artifacts
At least 18 artifacts have been identified in carotid ultrasound.
1- Reverberations result in unreal image on the screen as echogenic layers inside the artery.
2- Refraction, lead to improper position of the object on the screen.
3- Shadowing due to strong reflector like calcified plaque.
4- Enhancing the opposite object shadowing.
5- Aliasing occurs during spectral analysis; spectrum is wrapped around so that the top of
the waveform is seen at bottom of the screen. (This reverse color in color Doppler
mode).[34]

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1885
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
1.3.5 Common uses of Carotid Doppler ultrasound[36,37]
Doppler ultrasounds of the two carotid arteries, which are located on each side of the neck
and carry blood from the heart to the brain, provides detail pictures of these blood vessels and
information about blood flow through them, and gives information about the presence of
carotid atherosclerosis which is a risk factor for patient with transient ischemic attack or
minor stroke.[35]
A Doppler ultrasound study is usually an integral part of carotid artery ultrasound
examination, most frequently performed to detect carotid artery atherosclerosis and intima
media thickness a condition that increases the risk of stroke.
1- The major goal of carotid Doppler ultrasound remains to screen for the narrowing or
blockage of carotid artery, which if present adequate treatment may be initiated.
2- Also Doppler ultrasound performed if the patient having hypertension or diabetes mellitus
or presence of bruits in neck and also in presence any other risk factors.
3- Doppler Ultrasound of carotid artery also is performed in preparation for CABG Surgery.
4- Other uses are
a. Locate a hematoma that may slow or eventually stop blood flow in the artery.
b. Check the state of carotid artery after surgery to restore normal blood flow.
c. Using two dimensional (gray-scale) to measure the thickness of intima and media which a
good marker for atherosclerosis and can aid in plaque characterization, the morphology of
plaque is related to risk of stroke.
1.3.6 Techniques of Doppler ultrasound
A-mode; it is standing for amplitude, gives a 1D trace, it depicats the depth of an interface
and the strength of the reflected signal.
B-mode it is the most common used techniques, it gives brightness and gives 2D sliced
image.
M-mode, it displays a trace of movements of structures within the sound beam line, it used
for imaging the heart valves for example[24]
, Duplex ultrasound; it is useful in arterial and
venous study, it helps to determine flow characteristic of circulation in areal time moving B
mode image.[38]
1.3.7 Performing the ultrasound test;[32,39,40,41]
A. Patient preparation; Wearing comfortable, loose, fitting clots, remove jewels and may
need to remove all clothing in area to be examined. A loose fitting open necked shirt or

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1886
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
blouse is ideal. Doppler ultrasound is very sensitive to motion so patient should be quite.
And other preparation if needed.
B. Equipment: Ultrasound scanners consist of computer, and electronics, a video display
screen and transducer that is used to do the scanning, the transducer is a small hand held
device that resembled a microphone, attached to the scanner by a cord. Some examiners
may use different transducer (with different capabilities), during a single examination.
The principle involved in the sonar is similar to that used by bat, ships, and a fisherman,
when a sound wave strikes an object it bounces back as echoes by measuring these echoes
waves, it is possible to determine how far away the object, as well as its size, shape, and
consistency.
In medicine, ultrasound is used to detect changes in appearance, size, character of organs,
tissues and vessels or to detect abnormal masses (tumor).
In the ultrasound examination, the transducer both, sends the sound wave and receives the
echoing waves. The transducer directs small pulses of inaudible, high frequency waves in to
the body. As the waves become bounce off internal organ, fluids and tissues, the sensitive
microphone in the transducer record the tiny changes.
In the sound pitch direction, that waves are instantly measured and displayed which in turn
reacts a real time picture on the monitor. One or more frame of the moving pictures is
typically captured as still images. Short video loops of the images usually saved.[2,24,40,41]
1.3.8 The procedure performance
The patient is lying face up on the examination table that can be tilted or moved, patient may
be turned to either side to improve the quality of the images. A clear water based gel is
applied to the skin of the neck being studied, to help transducer make secure contact with the
body and eliminate air pocket between the transducer and the skin that can block the sound
waves from passing in to the body.
The sonographer or the radiologist then places the transducer on the skin in various locations
keeping over the area of interest or angling the sound beam from different location to better
see the area of concern.
At the end of examination, the patient dresses and wait while the ultrasound images are
reviewed, the examination will completed within 30-45 minutes. Figure 4.[40]

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1887
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 4: Standard ultrasound probe setting and production of ultrasonographic
images (courtesy of Ryan WD, Komaiko MS, Pressman BD.).[2]
13.9 Advantages and Disadvantage
1- Noninvasive and painless.
2- Available and easy to perform.
3- Safe not use radiation.
4- Give clear picture of soft tissues.
5- If block of the artery found treatment can be done to restore the blood flow.
6- It is free from risk.
Disadvantage
Extreme operator dependent and need expert examination to be performed in the right way to
give confident, dependable, Qualitative, quantitative and statistically standard measures.[40]
1.3.10; Identification of the Carotid arteries
1-Detecting internal and external arteries;[42]
External carotid artery (ECA) has small caliber than, internal carotid artery(ICA) which lies
posterolateral to ECA, the ECA may have superior thyroid artery branch coming off., also
ECA has low diastolic flow, also ECA has positive temporal tap test (Fig 5).[34,42]

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1888
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure.5; ultrasonographic image of CCA, ECA and ICA, normal image, courtesy of
Dr. Shephard, int med. Educ.[41]
2- Identification of Common Carotid Arteries
Having pulsatile wall and its caliper is smaller than internal jugular vein.
3-Determination the degree of stenosis
The commonly used methods are by measuring the peak systolic velocities (PSV) and end
diastolic velocities, also by measuring the ratio between ICA and CCA,(ICA PSV / CCA
PSV) normal<2 and ICA EDV <40cm/sec, the degree of stenosis is determined in term of
exact percentage. A range of 50-69% is more accurate however the measurement vary from
lab to lab, depends on many factors that affect these measurements, these include the
equipment used, the person performing and the sites normal velocity of CCA is 30-40 cm/sec,
increase velocity above the normal level means there is stenosis in which ICA psv is 125-230
cm/sec and plaque is visible sonographically additional criteria include ICA/CCA psv ratio of

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1889
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
2-4 and ICA EDVof 40-100 cm/sec, in ≥70% stenosis of the CCA PSV is more than ≥230
/sec with visible plaque seen at gray scale and colour Doppler ultrasound, additional criteria
include ICA /CCA psv ratio >4 and ICA EDV > 100 cm/sec, in near occlusion of ICA
velocity parameters may not apply,since velocities may be high, low, or undectatable
diagnosis established primarily by demonstrating amarkedly narrowed lumen by gray scale
and coloured Doppler ultrasonography. In presence of < 50% stenosis in ICA the PSV Is 125
cm/sec and presence plaque and intimal thickening (>0.8 mm consider abnormal and highly
associated with atherosclerosis).[30,34]
Also cross sectional area measurement is acurrate and more sensitive than dimensional
measurement in assessment of degree of stenosis, dimensional scale can be used to measure
the intima – media thickness which a good marker for atherosclerosis and can aid in plaques
characterization.[29,42]
Figure 6: Ultrasound images of the intima-media thickness A normal intima media
thickness, and B (showing increase in intma media (0.9cm).

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1890
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 7: Echogenic Atheromatic plaque in CA bulb, a; longutidinal section; B; coronal
section.
1.4. Aim of the study
To evaluate the association between carotid artery atherosclerosis as finding out the presence
of athermanous plaque in the carotid arteries and significant increment in intima-media
thickness and coronary artery atherosclerosis by Carotid Doppler ultrasound.
RESULTS
84.88% of the patients were males while 16% were females, the Majority Were males above
the age of 50 years. Table I, shows the age and sex incidence.
Table 1: Age and sex incidence.
Sex No. % Age < 50 Age > 50
Males 73 84.88 7 66
Females 13 16% 6 7
Total 86 100 13 73
93% of the patients were smoker or ex-smoker, including males and Female (73 males and 7
females). While 75, (87%) having hypercholesterolemia, 63 patients with hypertension
(61%), those with Diabetes mellitus were 26 patients (30%), family history of coronary
cardiac disease was obtained in 18 patients (20.9 %), as shown in Table 2.
Table 2: Risk factors for atherosclerosis.
Risk factor No. % < 50 years > 50 years
Age 86 100 13 73
Smoking 80 93 7 73
Hypercholesterolemia 75 87 5 70
Hypertension 51 61 8 45
Diabetes 26 30 6 20
Family history 18 20.9 12 6

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1891
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
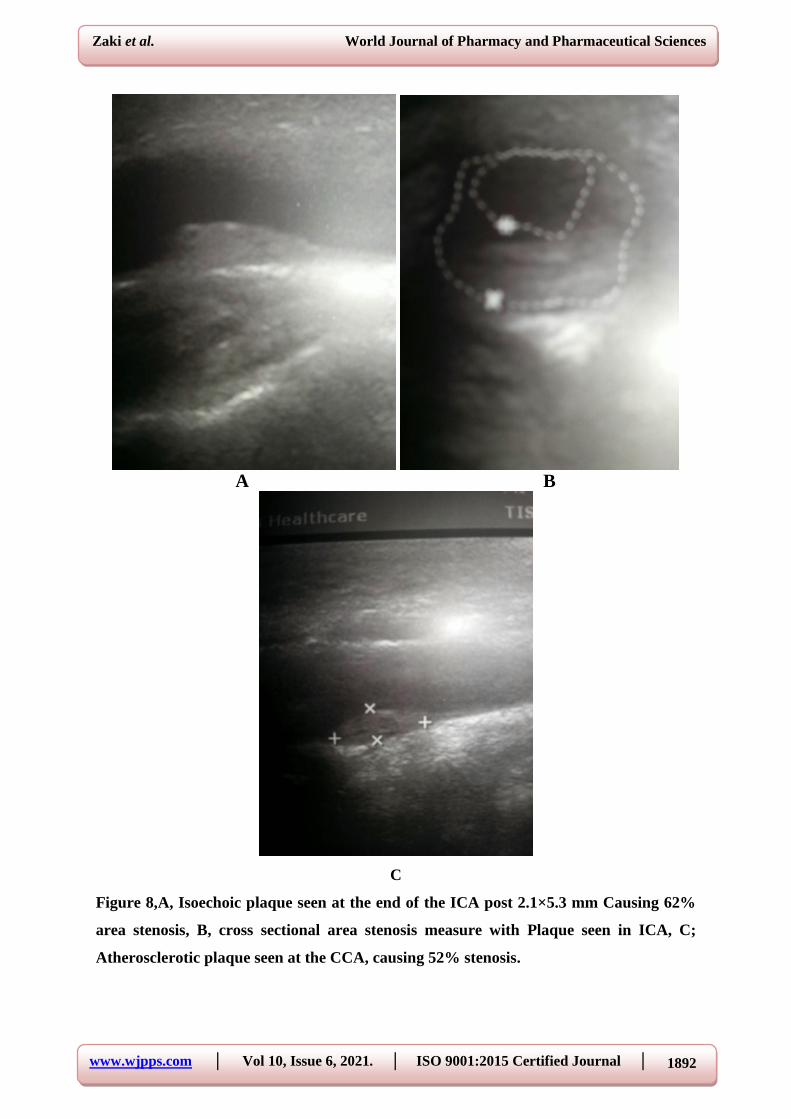
Carotid artery atherosclerosis was found in 66 patients (76.7%), while 20 patients (23.25%),
had normal right and left carotid arteries, as shown in table 3 and Figure(8) a, b,c.
Table 3: Association between risk factors of atherosclerosis and plaque and Intima-
media thickness.
Risk factors Plaque and IMT %
Age>50years 60 69.76%
Age<50 years 6 6.97%
Smoking 66 76.74%
Hypertension 30 34.88%
Diabetes mellitus 20 23.25%
Table IV: Association between plaque and IMTwith age,smooking,hypertension and
diabetes mellitus.
Plaque and IMT Odd's ratio P-value*
Yes% No%
Age ≥50years 60(90.9)% 13(65.0%)
5.38 0.004 <50years 6(9.1)% 7(35.0)%
Smoking +ve 66(100.0)% 14(70.0)%
_ 0.000** -ve 0(0.0)% 6(30.0)5
Hypertension +ve 46(69.7)% 17(85.0)%
0.40 0.175 -ve 20(30.3)% 3(15.0)%
Diabetes mellitus +ve 20(30.3)% 6(30.0)%
1.014 0.97 -ve 46(69.7)% 14(70.0)%
*Chi-square
**Fisher exact
There was significant stastical association between plaqueand IMTwith age,as there was
60(90.9)% patient older than 50with plaque and IMTcompared to 6(9.1)%patients younger
than 50years old and there was 5.38times more riskfor patient equal or older than 50 years to
develop plaque and IMT. There was significant statistical association between plaque and
IMTwith smoking as all 66(100%)smoker had plaque and IMT. niether hypertension nor
diabets mellitus showed astatistically significant association with plaque and IMT.
www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1892
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
A B
C
Figure 8,A, Isoechoic plaque seen at the end of the ICA post 2.1×5.3 mm Causing 62%
area stenosis, B, cross sectional area stenosis measure with Plaque seen in ICA, C;
Atherosclerotic plaque seen at the CCA, causing 52% stenosis.

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1893
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
A B
C
Figure, 9: A: atherosclerotic plaque seen in the CCA Causing 59% stenosis. B:
atherosclerotic plaques Seen in the bulb causing 72% stenosis. C: calcified plaque seen
at the beginning of the ICA.
Regarding the location of atherosclerotic plaques in carotid arteries, the common site was
ICA, with 35 lesions (53%), followed by CCA, 21 lesions (32 %), and the bulb with 10
lesions (15%) as shown in Figure(9), a, b c Majority of the patients had unilateral plaques, 61
patients (92.4%) only 5 patients with bilateral (7.6%).
The severity of carotid atherosclerosis was associated with numbers of coronary arteries
diseases, carotid artery stenosis was present in 15.1% when one coronary vessel was
www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1894
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
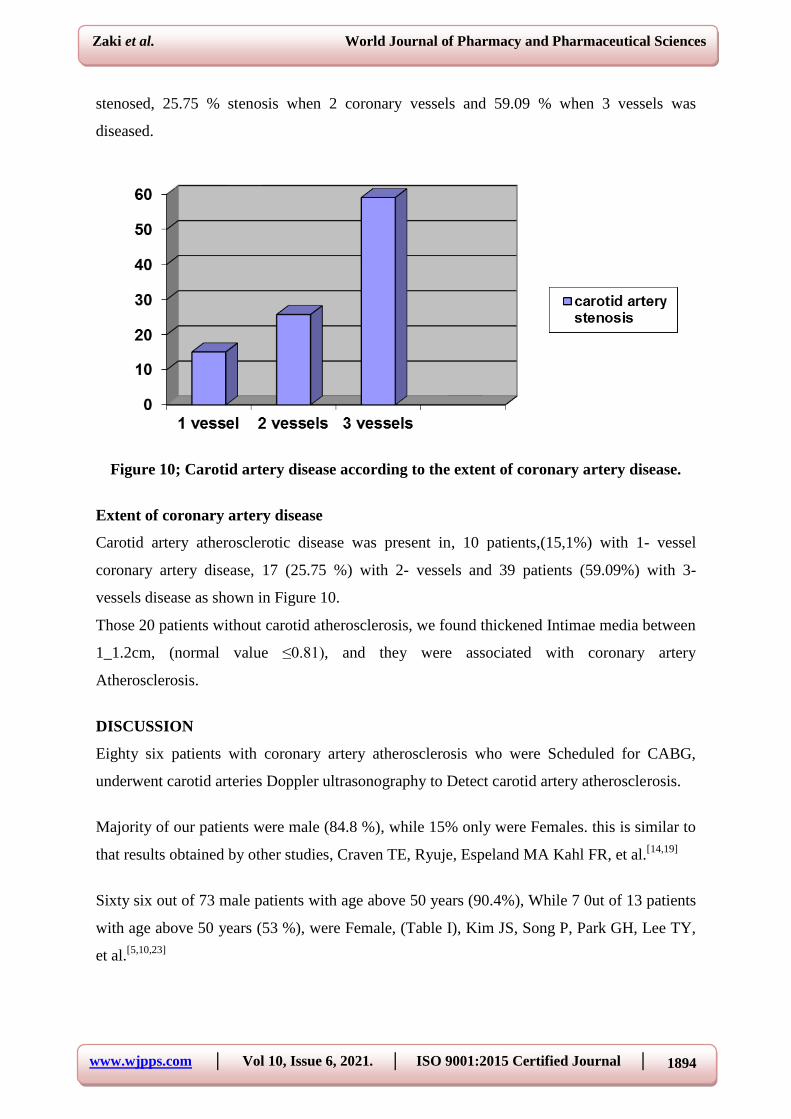
stenosed, 25.75 % stenosis when 2 coronary vessels and 59.09 % when 3 vessels was
diseased.
Figure 10; Carotid artery disease according to the extent of coronary artery disease.
Extent of coronary artery disease
Carotid artery atherosclerotic disease was present in, 10 patients,(15,1%) with 1- vessel
coronary artery disease, 17 (25.75 %) with 2- vessels and 39 patients (59.09%) with 3-
vessels disease as shown in Figure 10.
Those 20 patients without carotid atherosclerosis, we found thickened Intimae media between
1_1.2cm, (normal value ≤0.81), and they were associated with coronary artery
Atherosclerosis.
DISCUSSION
Eighty six patients with coronary artery atherosclerosis who were Scheduled for CABG,
underwent carotid arteries Doppler ultrasonography to Detect carotid artery atherosclerosis.
Majority of our patients were male (84.8 %), while 15% only were Females. this is similar to
that results obtained by other studies, Craven TE, Ryuje, Espeland MA Kahl FR, et al.[14,19]
Sixty six out of 73 male patients with age above 50 years (90.4%), While 7 0ut of 13 patients
with age above 50 years (53 %), were Female, (Table I), Kim JS, Song P, Park GH, Lee TY,
et al.[5,10,23]

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1895
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
In our study, we found that the accepted risk factors of significance in Carotid artery
atherosclerotic changes and coronary artery stenosis are, old age above 50 Years old,
smoking, hypercholesterolemia, diabetes mellitus, hypertension and family history of
previous heart attack, (Table II) this in agreement with other author studies, Kim JS, Song P,
Park GH, Lee TY, et al.[5-6,8,45]
In our study, we found similarities between risk factors for coronary artery disease and
carotid artery disease, Shirani S. Boroumand MA. Abbasi SH. Maghsoodi N, et al, however
we found less difference in the effect of each risk factor, the effect of high cholesterol is less
than hypertension which has profound effect on both carotid and coronary arterial
stenosis.[14,45-47]
We agree with Craven TE et al that because carotid and coronary atherosclerosis share a
certain number of these risk factors.[14]
Ultrasonography of carotid arteries had shown the presence of carotid atherosclerosis in 66
patients, (76.7%), 20 patients had normal carotid arteries, (23.25%). Table II, Davis SM,
Donnan GA, et al.[11,13-14]
Also we found; male with age above 50 years (76.7%) had a significantly more carotid
atherosclerosis than female of same age Female patients with age of less than 50 years having
atherosclerosis six patients out of 13,(46 %), more than male having the same age.
Seven patients (9.58 %) out of the total 73 patient who had carotid atherosclerosis were
females, this is the same finding obtained by other authors, LemoloF. MartinikA.
StienmanDA. Spens JD; et al. This suggesting that differences in sex hormones may affect
remodeling of atherosclerosis.[48,49]
We found the carotid artery intima –media thickness in 20 patients without carotid
atherosclerosis is correlated with extent and severity of coronary artery disease, this is in
agreement with Solonen.[49]
And Solonen finding that stated; the carotid artery intima-media
thickness values in men may associate with higher coronary artery diseases (table III).
Regarding the location of atherosclerotic plaques in carotid artery, it occurs in 61 patients at
one site (unilateral, 93.4%), only 5 patients had bilateral (7.6%), The common site was ICA,
in 51 patients (53%), then the CCA in 21 patients. (5%), the bulb affected in 10 patients (15

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1896
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
%)Fig (7) and Fig (8), this is different than Kallikazaros et al findings, they found bulb is the
commonest site (77.4%) next was the ICA, (53.6%), and the least was the CCA, 48.7%.[13]
We had found a significant correlation between carotid and coronary atherosclerosis, as there
was a stepwise increase in the number of patients with increase severity of those with
coronary artery disease.
As patients with 1, 2, and 3- vessels disease, carotid artery disease was present in 15.1%,
25.75%, 59.09% respectively, (Fig 10). This indicated a strong correlation between carotid
artery disease and severity of coronary artery atherosclerosis, this is similar to result obtained
by other authors, Pozniak MA. Allen PL; et al.[13,51]
Also we agree with those authors, Kallikazaros I, Tsioufs C, Sideris S, Stefandis C,
Toutouzas P; et al; that this classification may not precise but it is very useful and common in
clinical practice.[13]
CONCLUSIONS
There is a significant association between Carotid artery atherosclerotic changes and
coronary artery stenosis. In those patients who scheduled for Coronary artery bypass surgery,
ultrasonography and Doppler are Gold standard for detection carotid artery disease. The
presence of carotid atherosclerosis is strongly related to presence and severity of coronary
artery disease.
The evaluation of intima – media thickness is a useful marker for presence of coronary artery
stenosis.
Recommendations
1- Any patient having a history heart disease should referred for carotid Doppler
ultrasonography to find out the state of his carotid artery
2- Carotid artery Doppler Ultrasonography would be mandatory for all patients who have
coronary artery diseases before cardiac surgery to avoid cerebral vascular complications
like Transient ischemic attack or stroke.
3- Follow the patient post operatively after Coronary artery bypass graft and check for any
brain ischemic insult had occurred with searching for the exact cause of it. Then correlate
the number of brain insulted patient with those who had preoperative carotid artery
atherosclerotic changes to find its significance.

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1897
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
4- Doppler ultrasound should be available in all Hospitals and there should be training
courses in carotid Doppler ultrasound.
5- A join committee between cardiologist, cardiovascular surgeon and radiologist will
increase the detection and diagnosis of associated carotid stenosis and Coronary artery
disease and proper arrangement of management.
REFERENCES
1. Owen Kang, Yurangyweerakkody, etal.
2. Ryan WD, Micell S, Barry DP. editors blue prints in radiology, USMLE step 2 And 3,
Blackweel Publishing, USA, 2003; 4-6.
3. Snell R S. The head and neck, in clinical anatomy for medical student by Snell RS, editor,
8 edition, Lippincott Willams and Wilkins, USA, 2007; 8: 646-649.
4. Cliford-Jones R. cerebral artery territories in oxford hand book of clinical medicine by
Longmore M, Wilkinson I, Turmezei T, Cheung C K. ed 7t editionOxford University
press, London, 2007; 7: 436-441.
5. Kim JS, Song P, Park GH, Lee TY, et al, Biomarker of asymptomatic carotid Stenosis in
patients undergoing coronary artery bypass grafting, Stroke, 2011; 42: 734-739.
6. Naylor AR, Mehta Z, Rothwell PM, Bell PR, Carotid artery disease and stroke During
coronary artery bypass; a critical review of the literature. Eur. J. Vasc Endovasc. Surg.,
2002; 23: 283-294.
7. Schwartz AE, Sandhu AA, Kaplon RJ, Young WL, et al, Cerebral blood flow is
determined by arterial pressure and not cardiopulmonary bypass flow rate. Ann. Thorac.
Surg, 1995; 60; 165-169.
8. Cywinski JB, Koch CG, Krajewski LP. Smedira N, Li L Starr NJ. Increased risk
Associated with combined carotid endarterectomy and coronary artery bypass Graft
surgery; a propensity matched comparison with isolated coronary artery bypass Graft
surgery. J. Cardiothorac Vasc Anesth, 2006; 20: 796-802.
9. Kovacic JC, Roy PR, Baron, DW. Muller DW. Staged carotid artery stenting and
Coronary bypass graft surgery; initial results from a single center. Catheter Cardiovasc
Interv, 2006; 67: 142-148.
10. Kiernan TJ, TaquetiV, Crevensten G, Yan BP, Slovut DP Jaff MR. Correlates of carotid
stenosis in patients undergoing coronary artery bypass grafting – a case control study,
Vasc, Med., 2009; 14: 233-237.

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1898
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
11. Davis SM, Donnan GA. Secondary prevention after Ischemic stroke or Transient
ischemic attack, Modern Medicine, 2013; 10: 28-36.
12. Kannel WB, Wolf PA, Verter J,; Manifestations of coronaray disease predisposing to
stroke; The Framingam study. JAMA; 1983; 35: 2942–2946.
13. Kallikazaros I, Tsioufis C, Sideris S, Stefandis C, Toutouzas P; Carotid Artery disease a
marker for the presence of severe coronary artery disease In patients evaluated for chest
pain, Stroke, 1999; 30: 1002-1007.
14. Craven TE, Ryu JE, Espeland MA, Kahl FR, et al; Evaluation of associations between
carotid artery atherosclerosis and coronary Artery stenosis, A case control study.
STORKE, 1999; 1230- 1242.
15. GotoT, Baba T, Yoshitake Y, Ura M, Sakatar; Cranio cervical and aortic aterosclerosis as
neurologic risk factor in coronary artery surgery. Ann. Thorac. Surg., 2000; 69; 834-840.
16. Lee FJ, Chori KH, Rya JS, Jeon SB, et al; Stroke risk after coronary arterybypass graft
surgery and extent of cerebral artery atherosclerosis J. Am. Coll. Cardiol, 2011; 57(18):
1811-1818.
17. Hotamisligil GS; Endoscopic reticulum stress and atherosclerosis, Nature Medicine,
2010; 16(4): 396-399.
18. Singh RB, Mengi S, Dhalla NS; et al; Pathogenesis of atherosclerosis is multifactorial
process. Exp. Clin. Cardiol. Spring, 2002; 7(1): 40-53.
19. Bloomfield P, Bradbury A, Grubb NR, Newby DF; Cardio vascular disease.
atherosclerosis; in Davidson principle and practice of Medicine 20th
(by Ed; Boon NA,
ColledgeNR, Walker GR, unter JAA), Curcil Livingstone, London, 2006; 20th
: 579-580.
20. Wolf G; The role of oxidized low density lipoprotein (LDL), in the activation of
Peroxisome proliferator – activated receptor gamma; implication for Atherosclerosis.
Nutr. Rev, 1999; 57: 88-91.
21. Shah P K Mechanism of plaque valnerability and rupture. J. Am, Coll Cardiol, 2003;
41(4,5): 15s-22s.
22. Kate GC, DijkA C, Oord SC, et al; Usefulness of contrast – enhanced ultrasound for
detection of carotid plaque ulceration in patient with symptomatic carotid atherosclerosis,
Am. J. Cardiol, 3013; 112: 222-228.
23. Libby B; Multiple mechanisms of thrombosis complicating atherosclortic plaque, Clin
Cardiol, 2000; 23(6): 1-7.
24. Scally P. Ultrasound, Radiology, in Oxford hand book of clinical medicine, ed,
Longmore, Wilkinson I. Turmezei T. et al, 7th
edition, 2009; 722-724.
www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1899
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
25. Martinez S PA. Ultrasonography of carotid plaque for the prevention of stroke. Expert
Rey Cardiovasc. Ther., 2013; 11(10): 1425-1440.
26. Park HP, Evaluation of carotid plaque using ultrasound imaging, J.CardioVas-Ultrasound,
2016; 24(2): 91-95.
27. Grant EG, Benson CB, Moneta GL, et al. Carotid artery stenosis; gray- scale And
Doppler ultrasound diagnosis – Sociaty od radiologestin ultrasound consensus
Conference. Radiology, 2003; 229: 340-346.
28. AbuRahma AF, Srivasta M, Stone PA, et al Clinical apprasial of carotid duplex consensus
criteria in the diagnosis of carotid artery stenosis. J. Vasc. Surg., 2011; 5(1): 53-59.
29. O Lerry DH, Polak JF, Kramal RA, Manolla TA, et al. Carotid artery intima and Media
thickness as a risk factor for myocardial infaraction and stroke in old adult. Cardio
vascular health study. Collaboration Research Group. N. Engl. J. Med., 1999; 340(2): 14-
22.
30. Riles TS, Lee V, Cheever, D, Stable ford J, Rockman CB. Clinical course of
asymptomatic patients with carotid duplex scan end diastolic velocities of 100 to124
centimeters per second. J. Vasc. Surg, 2010; 52(4): 914-919.
31. Shaalan NE, Wahlgren CN, Desai T. Reappraisal of velocity criteria for carotid Bulb
internal carotid artery stenosis utilizing high resolution B- Mode ultrasound Validated
with computed tomography angiography. J. Vasc. Surg, 2008; 48: 104-112.
32. Lee W. General principle of carotid Doppler ultrasonography. Ultrasonograpy, 2014;
33(1): 11-17.
33. Stingele R, Berger J, Alfke K, et al. S P A C E investigators clinical and angiographic risk
factors for stroke and death within 30 days after carotid endarterectomy and stent
protected angioplasty. Lancet Neurol, 2008; 7(3): 216-222.
34. Smith SG, Jr. Greenland P, Grundy SM. Conference proceedings prevention conference
V beyond secondary prevention; identifying the high risk Patient for primary prevention,
Executive summary. Am. Heart. Assoc. Circulation, 2000; 101: 111-116.
35. Gaseki AP, Eliaziw M, Barret HJ. Risk factors for cervical atherosclerosis in patient with
Transient Ischemic Attack or minor ischemic stroke. Stroke, 1994; 25: 226-232.
36. Kaufman JA, Nesbit GM. Carotid and vertebral arteries in; Kaufman JA, Lee MJ eds.
Vascular and interventional radiology; The Requisites 2ed. Philadelphia PA; Elsevier
Saunders, 2014; 5.
37. Daly C, Rodriguez HE. Carotid artery occlusive disease. Surg. Clin. N. Am., 2013; 93(4):
813-832.

www.wjpps.com │ Vol 10, Issue 6, 2021. │ ISO 9001:2015 Certified Journal │
1900
Zaki et al. World Journal of Pharmacy and Pharmaceutical Sciences
38. Huston J 3rd, James EM, Brown RD, et al. Redefined duplex ultrasonography Criteria for
diagnosis of carotid artery stenosis, Mayo Clin Proc, 2000; 75(11): 1133-1140.
39. De la Torre J C, Carotid artery ultrasound and echocardiography testing to lower the
prevalence of alzheimar disease, J. Stroke, cerebrovasc. Dis., 2004; 18(4): 319-128.
40. American heart association. Ultrasound – carotid artery, Sociaty for vascular medicine,
Radiology. info. org., 2016; 21.
41. Filis KA, Johnson, BL, et al. Duplex ultrasound criteria for defining the severity Of
carotid stenosis. Ann. Vasc. Surg., 2002; 16: 413-442.
42. Dr. Shepherd S, Basic Ultrasound Anatomy between ica and eca, mint medical
educations, sanfrnsico, 2015.
43. Park AE, McCarthy WJ, Pearce WW, et al. Carotid plague morphology correlate with
presenting symptomatology. J. Vasc. Surg., 1998; 27: 872-878.
44. Eliasziw M, Strelfler JY, Fox AJ, et al. Significance of plague ulceration in Symptomatic
patient with high risk carotid stenosis. Stroke, 1994; 25: 304 308.
45. Shirani S. Boroumand MA. Abbasi SH. Maghsoodi N. et al, Prospective carotid Artery
screening in patients undergoning coronary artery bypass graft surgery, Arch Med Res.,
2006; 37: 987–990.
46. Gordon T. Kannel WB., Multiple risk functions for predicting coronary heart Disease;
The concept, accuracy, and application. Am Heart J., 1982; 103: 1031-1039.
47. Salonen R. Sepplinen K. Raurramaa Re. Salonen JT; Prevalence of carotid atherosclerosis
and serum cholsterol levels in eastern Finland, Arteriosclerosis, 1988; 8: 788-792.
48. Manson, JE. Hsia J. Johnson KC, Rossouw JE, et al; Estrogen plus progestron and the
risk of coronary heart disease, N. Engl. J. Med., 2003; 349: 523-534.
49. Lemolo F. Martinik A. Stienman DA. Spens JD; Sex differences in carotid plaque and
stenosis. Stroke, 2004; 35: 477- 481.
50. Solonen R, Solonen JT; Determination of carotid intima media Thickness population-
based ultrasonography study in Eastren Finish men, J. Intern. Med., 1991; 229: 225- 231.
51. Pozniak MA. Allen PL, Editor: Clinical Doppler Ultrasond 3rd
edition: Churchil
Livingstone, Elsever Canada, 2014.