donate life louisiana hospital campaign - …c.ymcdn.com/sites/ life louisiana hospital campaign ......
TRANSCRIPT

Donate Life LouisianaHospital CampaignClinical Champion Training
Donate Life Louisiana Hospital Campaign
• Our vision was to create a campaign that every hospital, regardless of size or type, could implement and have an impact on the waiting list.
• Campaign was launched at the 2008 LHA Summer Conference.
• We wanted to increase the registry list while educating our communities.

Original Campaign GoalsTo increase the Donate Life Louisiana Registry by 10% or 160,676 new registrations by the end of 2009.
– Met the first goal in August 2009– Set a second goal to reach 200,000 by
July, 2010 which was achieved in February, 2010

New Goal for Registry Campaign
• Increase the Louisiana Donor Registry by another 50,000 by July 2010 (total of 250,000)– Increase number of hospitals participating in
registry campaign

Campaign Support and Resources:
• Electronic Toolkits • LHA Website – Campaign Section• LOPA/LHA Staff• Donate Life Louisiana Materials• HHS Resources• Champion Network
Hospitals Recognized for Successful Campaigns
• Bunkie General Hospital
• CHRISTUS St. Francis Cabrini
• Lafayette General Medical Center
• Ochsner Medical Center
• Opelousas General Health System
• Our Lady of the Lake
• Our Lady of Lourdes
• Terrebonne General
Indirect Benefits• Referrals from Hospitals that Were
Not Referring• Organ Donors from Previously
“Non-Donor Hospitals”• Increase in Hospital Staff Education• Willingness to Perform Pre-Donor
Management

Taking the Campaign to the Next Level
• New challenge issued by LHA board for 2010
• Increase the conversion rate in all organ donor hospitals in Louisiana to 75% or greater by the end of 2011– This goal is consistent with Joint
Commission and CMS guidelines
Hospital Conversion Rate
• Defined as the number of actual organ donors divided by the number of eligible donors

Clinical Champion
• Provide active leadership and support of organ and tissue donation
• Share best practices with hospital staff members
• Work collaboratively with LOPA Hospital Resource Coordinators to establish a hospital wide commitment to donation

Factors Directly Impacting Conversion Rates
• Timely Notification• Family support and treatment at the hospital• Open communication• Physician support through donation process• Using Effective Requestors• Timeliness and appropriateness of the approach• Maintaining organ function prior to consent and
throughout the donor process

The Need
• As of March 30th there are:– 106,618 waiting in the US– 1,859 waiting in Louisiana
• In 2009 we had 152 organ donors and transplanted 488 organs
• We had a 66% conversion rate; increasing to 75% would result in 20 more donors and approximately 64 more lives saved

Donate Life Month
• Flag Raising Ceremonies• Remembrance Day/Donor Drive• Donor Drive with Blood Bank in Park• Health Network Featuring Donor
Awareness Month• Viral Campaigns

Regulatory Agencies and Partnerships

Agencies• Joint Commission
– Accrediting– Active in promoting organ donation– Standards guided by CMS and best practices
• CMS– Regulatory– Active in promoting performance improvement in organ donation– Conditions guided by best practices, other regulations and desire
to reduce payments

Joint Commission
“Our shared vision must be to narrow (significantly) the organ donation gap and save lives!”

Joint Commission
• Organ donation desired future state:1. No one dies while waiting for a life-saving
organ2. The number of transplants performed each
year exceeds new demand, resulting in a sustained decrease in the Waiting List for Life
3. Organ yield will increase from 3.06 organs per donor to over 3.75 organs per donor

Joint Commission
• Organ donation desired future state:4. Cardiopulmonary criteria for determining
donation potential are well-established in hospitals
5. Hospitals will consistently maintain organ donation conversion rates that exceed 75%
6. The disparity in available organs for racial and ethnic minorities will be eliminated

Joint Commission• Organ donation desired future state:
7. The donation wishes and advance directives of deceased potential donors will be respected and carried out
8. The opportunity for individuals to make a living donation will be facilitated through changes in employment and insurance policies and practice
9. The increase in demand for organ transplantation will slow as a result of more effective health promotion and disease prevention programs

Joint CommissionLatest Updates
• In March 2009, the standards addressing organ and tissue donation moved from the Leadership chapter to Transplant Safety to make it easier to reference.

Overview of Joint Commission Changes
• TS.01.01.01 EP 3 • The hospital has a written agreement
with at least one tissue bank and at least one eye bank to cooperate in retrieving, processing, preserving, storing and distributing tissue and eyes.

Overview of Joint Commission Changes
• Note 1: This process should not interfere with organ procurement.
• Note 2: It is not necessary for a hospital to have a separate agreement with a tissue bank if it has an agreement with its OPO to provide tissue procurement services; nor is it necessary for a hospital to have a separate agreement with an eye bank if its OPO provides eye procurement services. The hospital is not required to use the OPO for tissue or eye procurement, and is free to have an agreement with the tissue bank or eye bank of its choice.

Overview of Joint Commission Changes
• TS.01.01.01 EP 9• The hospital notifies the OPO of patients who have
died or whose death is imminent according to the following:Clinical triggers defined jointly with its medical staff and the designated OPO present.Within the time frames jointly agreed on by the hospital and the designated OPO (ideally, within one hour).Prior to the withdrawal of life-sustaining therapies, including medical or pharmacological support.

Overview of Joint Commission Changes
• TS.01.01.01 EP7• The individual designated by the hospital to
notify the family regarding the option to donate or decline to donate organs, tissues, or eyes is an OPO representative, an organizational representative of a tissue or eye bank, or a designated requestor.

Overview of Joint Commission Changes
• EP 7 cont.• Note: A designated requestor is an
individual who has completed a course offered or approved by the OPO. This course is designed in conjunction with the tissue and eye bank community to provide a methodology for approaching potential donor families and requesting organ and tissue donation.

Joint Commission10 C’s for Success
1. Champion for the cause!2. Commitment of leadership3. Culture of priority for organ donation4. Collaborative effort5. Communicate rapidly (call within 1 hour)6. Clinical trigger for call to OPO7. Conversion rate improvement8. Counsel potential donor families to increase consent9. Clarify procedures10. Consider establishing DCD protocols

CMS• CoP §482.45(a)(3): Ensure, in collaboration with the
designated OPO, that the family of each potential donor is
informed of its options to donate organs, tissues, or eyes, or
to decline to donate.
– Interpretive Guideline:• OPO screens for medical suitability • Family must be informed of the family’s donation options• Ideally, the OPO and the hospital will decide together how
and by whom the family will be approached

CMS
• CoP §482.45(a)(3): The individual designated by the hospital to initiate the request to the family must be an organ procurement representative or a designated requestor.– Interpretive Guideline:
• A designated requestor is a hospital-designated individual who has completed a course offered or approved by the OPO and designed in conjunction with the tissue and eye bank community
CMS• CoP §482.45(a)(5): Maintaining potential donors while
necessary testing and placement of potential donated organs, tissues, and eyes take place.– Interpretive Guideline:
• The hospital must have policies and procedures, developed in cooperation with the OPO, that ensure that potential donors are maintained in a manner that maintains the viability of their organs
• The hospital must have policies in place to ensure that potential donors are identified and declared dead within an acceptable time frame

CMSImportant Changes to OPO CoP
• Definition of an eligible donor– For brain dead patients aged 70 and younger,
everyone is eligible unless and until we can document otherwise
• Declaration in accordance with hospital policy or state law
• Documentation must be of a specific diagnosis• Medical record reviews
– Level I or Level II trauma center or– 150 beds, a ventilator, and an ICU

Transition from end of life care to the gift of life.

Don't think of organ and tissue donation as giving up part of yourself
to keep a total stranger alive. It's really a total stranger giving up
almost all of themselves to keep part of you alive. ~Author Unknown

Family support following a catastrophic brain injury

Circumstances of clinical brain death in organ donors, 1999-2009. MVA = motor vehicle accident. Source: United Network for Organ Sharing (UNOS), 2009.

Mechanism of death in organ donors, 1999-2009. SIDS = sudden infant death syndrome. Source: United Network for Organ Sharing (UNOS), 2009.

Assess the Situation
• What has the family been told about the patients condition?
• What does the family understand about the patients condition?
• Who can best provide them support at this time?

How is the Family Reacting?
• Numbness/Denial/Shock• Depression• Elation• Anger• Guilt• Irritability• Confusion/Bewilderment• Avoidant Behavior and Withdrawal

How to Support the Family
• Respond to emotions with empathy
• Validate family’s feeling and concerns
• Provide clear, consistent, timely communication about the patients condition
• Respond to questions and concerns promptly.
• Remember: a family’s in crisis only hears about 20% of the information provided

Things Not To Say or Do:
• Do not say “It will be alright”• Do not push for details• Do not say “I know how you feel”• Never blame the patient or family for what happened• Avoid telling a survivor “It was not your fault”• Avoid giving advice
The transition from cure to comfort care

Process for healthcare providers
Redirect hope from cure to comfort
Provide information about illness or injury
“Plant seeds” about prognosis
Develop a trusting relationship with the patient’s family
Provide Consistent perspective on patient’s prognosis
Hold meetings with the family
Involve other disciplines (pastoral care, social services)
Continue supportive relationship with the family
Reiterate information as needed
Face the question to forgo life-sustaining therapies
Take on role of surrogate decision maker
Come to terms with what this illness or injury means for the patient:• Suffering• Values• Quality of life• Life story
Understand the critical illness
Recognize futility or probably bleak outcome
Process of family members
The Process for Family Members
1. The families begins to understand the critical illness by seeking information about the irreversible physiological process that are occurring. The family recognizes the futility of the situation or probable bleak outcome.
2. The family comes to terms with the reality of what the illness or injury means for the patient.
3. The family recognizes they are responsible for making decisions and is ready to face the question of forgoing life-sustaining therapies
Thelen, M., (2005). End-of-life decisions making in intensive care.

The Process for Health Care Providers
1. Laying the groundwork:• Develop a trusting relationship with the family• Provide information about the illness or injury• Plant seeds about prognosis
2. Shifting the picture• Provide consistent perspective of patients prognosis• Hold family meetings• Involve other disciplines
3. Accepting a new picture:• Continue supportive relationships with the family• Reiterate information as needed• Redirect hope from cure to comfort
Thelen, M., (2005). End-of-life decisions making in intensive care.

Behaviors That are Helpful:
• Providing timely communication• Providing consistent care providers• Treating the family with compassion and respect• Acting as an arbitrator between family members• Providing spiritual, emotional and grief support• Providing access to the patient
Thelen, M., (2005). End-of-life decisions making in intensive care.

Behaviors That Hinder:
• Avoiding or postponing discussions about a poor prognosis• Being reluctant to use the words “death” or “dying”• Using medical terms• Not knowing the patient• Giving inconsistent messages • Placing full responsibility for decision making on one person• Defining death as a failure• Withdrawing from interactions with the family
Thelen, M., (2005). End-of-life decisions making in intensive care.

Relationship and Communication
• Developing a trusting relationship • This helps families feel safe and supported in the decision-making
process
• Listening • Helps decrease feelings of guilt and burden
• Communication with the family• Must happen early and often • Must be clear, direct and honest
Thelen, M., (2005). End-of-life decisions making in intensive care.

Is it brain death or death?
Recent studies show:• Of 195 physicians and nurses who care for patients with catastrophic brain injury:
– only 35% correctly recognized the legal and medical criteria for determining
brain death
– 58% did not use a coherent concept of death consistently
• Of 164 brain dead patients, the next of kin was queried about their understanding of
brain death:
– 28% stated brain death was the same as coma
– 9% did not know
Sullivan, J., Seem, D. L., & Chabalewski, F., (1999). Determining brain death.

Supportive Language
• “ Despite our best efforts it appears that his condition has
deteriorated. The physician is coming to evaluate your loved
one and we will update you as soon he is here”
• “There has been a change to his neurological condition, It
appears to me that he has lost significant neurological
responses. However, we need the physician to confirm my
assessment”

Steps for a Family Meeting
1. Preparation – review chart, clarify goals and check emotions2. Establish proper setting with seating available for everyone present3. Introductions / Goals / Relationship of all present4. Determine family understanding of condition5. Summarize the situation avoiding jargon and answering questions6. Silence / Respond to reactions7. Present goal-oriented options and stress priority of comfort regardless of goal8. Translate goals into plan of care9. Document and discuss with team caring for patient and check emotions10. Managing Conflict:
– Listen - Use empathetic statements
– Determine source of conflict - Clarify misconceptions– Set time-limited goals with specific benchmarks

Palliative Care
Care that aims to relieve suffering and improve quality
of life for patients with life-threatening illness and their
families

Organ and tissue donation should be a continuation
of end of life care
Organ donation should be integrated into quality end-of-life care. Patients and their families should be offered the opportunity to donate as standard end-of-
life care, and information on organ donation processes should be an integral part of the many
other decisions that are faced at that time.
Institute of Medicine, 2006.

Variables that impede the consent process
• Early mention of donation• Late referral• Trauma vs. non-trauma
– sudden death without underlying history• Infrequent updates to family• Coupling the news of death with the request of
donation• Rigid visitation during the patients end of life

Variables that support the consent process
• Timely referral• LOPA is inclusive in the end of life plan• Collaborative effort to support the family• Donation is introduced at the appropriate time

In all situations we must diligently try to relate to family members on a
human level and meet their informational and emotional needs

The Opportunity
• The opportunity to donate is the family’s right and if donor designated - the patients right
• Donation is proven to be beneficial for families going through the grieving process
• Over 105,000 people are counting on us to get it right

What a difference a word can make
Too often we underestimate the power of a touch, a smile, a kind word, a listening ear, an honest compliment, or the smallest act of caring, all of which have the potential to turn a life around. ~~Leo Buscaglia
Quote From a Donor Family
As I sat there...holding his hand, begging him to wake up,
pleading with God to spare my child... I realized...Justin wasn't
going home with me, his purpose on earth was complete, mine
was yet to be revealed.
Justin Harrison saved the lives of five people in 1997, when he
was 15 years old. He did it without fanfare, through an act of quiet
heroism.

Marilyn Thorn - Justin’s heart recipient
Libby Harrison - donor mom
Justin Harrison-Hero
Marilyn Thorn - heart recipientSue Acaldo – kidney & pancreas recipient

Stephanie
When we were approached by the LOPA people in the hospital my first reaction was "no way", I'm not burying my daughter cut to pieces.
My ex-husband did the listening and when I came to grips that she was not going to make it I realized that this would've been what Stephanie wanted and she probably would’ve said “Oh Mom, I want to do this.”
• It turned out to be a very good thing for us and it saved 5 peoples lives that night.•God bless everyone who makes this decision and the ones that are on the receiving end.

• After Eleven years, Stephanie’s
family(pictured) finally meets her
heart recipient, Elizabeth (far
left). They now consider
themselves to be family and plan
to visit often.

All of us are potential organ recipients as well as potential
organ donors, each of us has a stake in the system.
Institute of Medicine, 2006

References:
• Alexander, D. A., & Klein, S., (2000). Bad news is bad news: Let’s not make it worse. Trauma, 2, 11-18.
• Cooper, A., (2008). Palliative Care and the trauma patient. Journal of Hospice and Palliative Nursing, 10(5), 262-264.
• Coyne, P., Bobb, B. T., & Campbell, M. L., (2009). Role of palliative care nursing in organ and tissue donation: HPNA position paper. Journal of Hospice and Palliative Nursing, 11(2), 127-128.
• Institute of Medicine, (2006). Organ donation: Opportunities for action. Washington, DC: National Academies Press.
• Owens, D. A., (2006). The role of palliative care in organ donation. Journal of Hospice and Palliative Nursing, 8(2), 75-76.
• Shafer, T. J., Wagner, D., Chessare, J., Zampiello, F. A., McBride, V., & Perdue, J., (2006). Organ donation breakthrough collaborative: Increasing organ donation through system redesign. Critical Care Nurse, 26(2) 33-49.
• Sullivan, J., Seem, D. L., & Chabalewski, F., (1999). Determining brain death. Critical Care Nurse, 19(2), 37-46.
• Thelen, M., (2005). End-of-life decisions making in intensive care. Critical Care Nurse, 25(6), 28-37.
• Truog, R. D., Campbell, M. L., Curtis, R., Haas, C. E., Luce, J. M., Rubenfeld, G. D., et al., (2008). Recommendations for end-of-life care in the intensive care unit: A consensus statement by the American Academy of Critical Care Medicine. Critical Care Medicine, 36(3), 953-962.
• Valdes, M., Johnson, G., & Cutler, J. A., (2002). Organ donation after neurologically unsurvivable injury: A case study with ethical implications for physicians. Baylor University Medical Center Proceedings, 15(2),129-132.

Organ Donation:The Clinical Processes

The Organ Referral Process:Identification of a Potential Donor
All patients on a ventilator with a GCS < 5.
Patients that do not meet brain death criteria but have
suffered a non-survivable head injury.
Patient’s life-sustaining support is being withdrawn.

Organ Referrals
Organ Referral
Potential Organ Donor Rule Out
Brain Death Donation after Cardiac Death

Brain Death
Increased intracranial pressure sufficient to impede the flow of blood into the brain causing cellular death of the brain tissue and/or herniation
Donation after Cardiac Death (DCD)
The patient must have suffered a non-survivable brain injury or an anoxic event such that death would be imminent subsequent to the removal of ventilator and vasopressor support

Supporting the Potential Organ Donor
• Avoid DECELERATION in care– Clinical support– Family support
• Understanding the consequences of cerebral herniation
• Preserves the option of donation

Avoiding “Deceleration in Care”
Resuscitationof the patient
Identification of the potential organ donor Continued
resuscitationand declaration ofbrain death Consent
and donormanagementAvoidance of
deceleration in care

Predictable Consequences of Herniation
• Loss of brain stem vasomotor centers – hypotension
• Loss of hypothalamic – pituitary connection – Diabetes Insipidus
• Inflammatory mediators are released causing worsening lung function
• Autonomic storm of herniation can cause impaired heart function
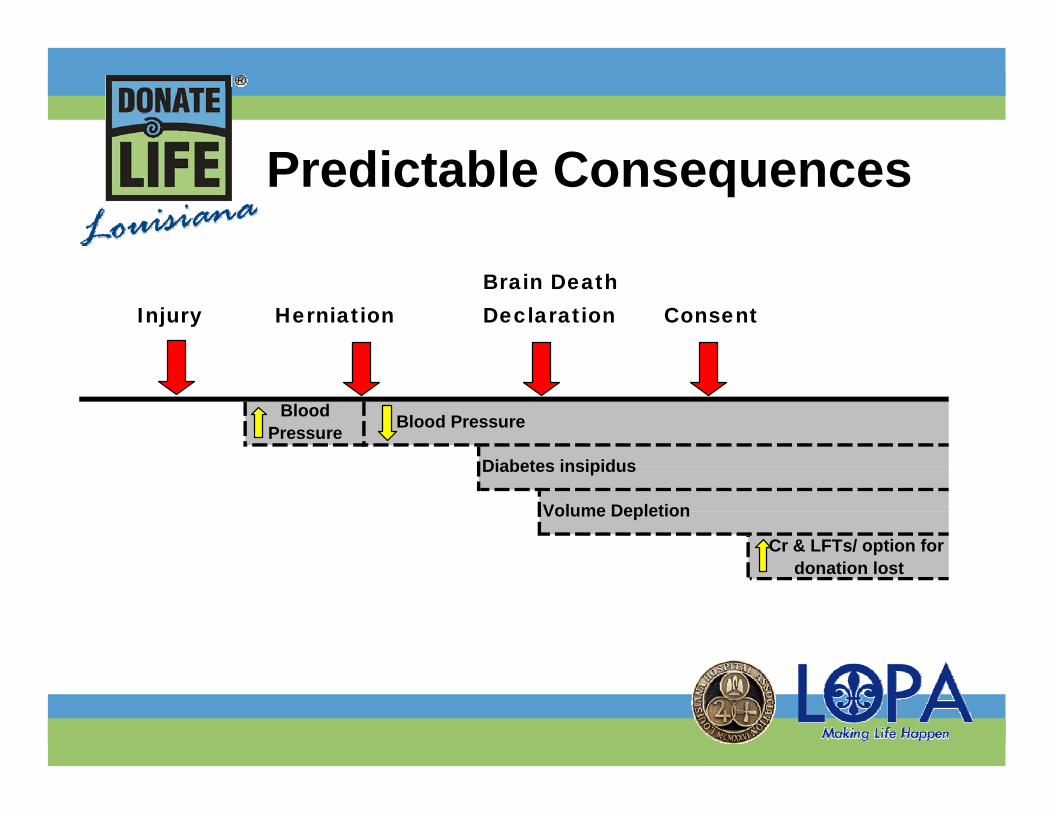
Predictable Consequences
Consent
Cr & LFTs/ option for donation lost
Injury
Volume Depletion
Herniation
Blood Pressure Blood Pressure
Brain Death Declaration
Diabetes insipidus
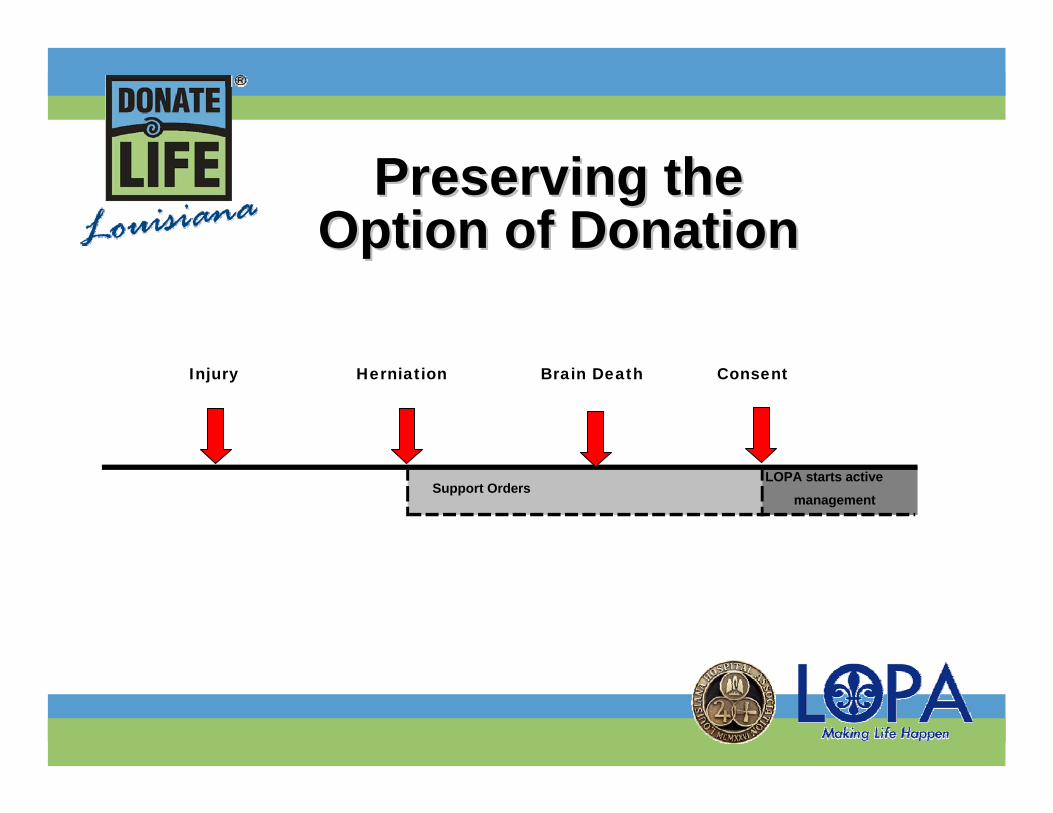
Preserving the Preserving the Option of DonationOption of Donation
Injury Consent
LOPA starts active
managementSupport Orders
Herniation Brain Death

Consequences of Herniation
• Loss vasomotor control + Intravascular Volume Decrease= HYPOTENSIONCauses:– Diuretics– Diabetes Insipudus– Traumatic Blood Loss

Consequences of Herniation• Endocrine
Dysfunction– Caused by pituitary
hypoxia– ↓amount or absence of
antidiuretic hormone (ADH) from post. pituitary
– Diabetes Insipidus– ↓in ACTH (cortisol)

Consequences of Herniation
• Catecholamine Surge– Increase in adrenaline
(epinephrine) which is a potent alpha and beta agonist
– ↑HR and BP– Neurogenic pulmonary edema
• Inflammatory mediator are released causing worsening lung function
– Systemic vasodilation

7 liters5 liters
10 liters10 litersMannitol
Blood loss
DIBrain death
Catecholamine
squeeze
Catecholamine Surge

The Results…• Hypovolemic Shock• Catecholamine Resistance• Hormonal Deficiencies• Hypoxia• Hypothermia• Electrolyte Abnormalities
Resuscitation • Maintain MAP> 65
– SBP-DBP/3 + DBP• CVP 4-12• Rule of 100’s
– U/O – SBP– HR– PaO2– Temp

Resuscitation
• Crystalloids– Maintenaince fluid @ 100 cc/hr with D5W
with KCl (as needed) – ½ NS or ¼ NS CC:CC urine output
replacement q1h
• Colloids and Blood Products– At physician discretion
Vasopressors
• Dopamine• Neosynephrine• Levophed (Norepinephrine)• Dobutamine• Vasopressin• Epinephrine

Hormonal Deficiencies:Antidiuretic Hormone (ADH)
• A.K.A Vasopressin• Secreted from Pituitary• Helps with:
– Hypovolemia– Hypotension– Hypernatremia

Vasopressin• Treatment for Diabetes Insipidus
– If urine output >500 cc/hr for 2 hrs, begin Vasopressin gtt.
– Mix Vasopressin 5 units in D5W 500 cc, and run at 10 cc/hr (0.1 units/hr).
– Titrate to keep urine output 100-300 cc/hr.– May use DDAVP q 12 hours if preferred

Ventilation and Oxygenation
• Maintain adequate O2 delivery to organs• Respiratory Treatments
– CPT, Turn Q2h– Atrovent and Ventolin
• ABG– Correct acid/base imbalances– Optimize oxygentation : +5 PEEP

Thermal Regulation:Hypothermia
• Due to interruption of the temperature-regulating center in the hypothalamus.
• ↓ cardiac function• ↓ amount of O2 supplied to organs
– Maintain Temp of 37°F with warming blanket and/or warm fluids

Electrolyte Abnormalities
Why balance?Fluid and electrolyte imbalances directly effect the hemodynamic stability of the donor and the ultimate viability of the organs for transplant.

Electrolyte Abnormalities:Hypernatremia
• Normal Na+ level 137-150• Treat if Na+ > 157
– Free water to NGT– Hypotonic IV bolus (D5W or ¼ NS)– Vasopressin if U/O is > 500– Lasix/Diuril if U/O is < 200 with absence of
hypovolemia

Electrolyte Abnormalities:Hyper/Hypokalemia
• Hyperkalemia– Lasix IV– Insulin IV (usually accompanied with D50W)– CaCl or Ca gluconate– NaHCO3
Remember to use caution when using one electrolyte to correct another. They often have reciprocal effects on each other.
• Hypokalemia– KCl: 20-40 meq over 1-2 hours– KPhos: 27 mmols = 40 meq K+Use if phosphorous is low
May give K acetate if Cl and Phos highKidneys excrete 20-40 meq K+ in each liter
of urine
Electrolyte Abnormalities:Hyper/Hypokalemia

Electrolyte Abnormalities:Hypocalcemia
–1-2 amps of CaCl or Ca gluconate
–Ca binds with albumin therefore are often given at the same time
Organs Recovered for Transplant:Brain Dead Donor
Kidneys
Lungs Liver
Pancreas
Small Intestine
Heart

Donation after Cardiac Death
• Many families that have loved ones who have suffered non-survivable injuries and wish to discontinue life support.
• DCD gives these families the opportunity to save lives through organ donation

Identification of a Potential DCD Donor
• GCS of 5 or less, on a ventilator• Patient who cannot sustain life without
continued medical intervention(ventilator support, vasopressors etc)
• Poor neurological prognosis, does not meet brain death criteria.
• A discussion regarding “DNR” or withdrawal of support is anticipated

• Medical Suitability
• Life Support Dependence
Identification of a Potential DCD Donor

• Medical Suitability– All patients under 70 with GCS 5 or less are
initially considered for DCD– medical history and labs/diagnostic tests are
utilized to determine first if the patient is medically suitable
Identification of a Potential DCD Donor

• Life Support Dependence– If medically suitable, an evaluation is done
to determine whether or not the patient will cardiac arrest in less than 1 hour
– Ventilatory dependence assessed– Pharmacologic dependence assessed
Identification of a Potential DCD Donor

Organs Recovered for Transplant: DCD
Kidneys
Lungs Liver
Pancreas
Avoiding “Deceleration in Care”:Potential Organ Donor
• Continuous clinical support and management prior to approach for donation– Allows families the opportunity to say “yes”– Donor stability– Increase conversion rate– Increase the number of potential lives saved
through organ donation

Potential Donor Family Support:Avoiding “Deceleration in Care”
• Recognizing the Family’s Needs– Education at the Bedside– Participation in Bedside Care– Personal Items at Bedside
• Supportive Language• Frequent Updates• Spiritual Support• Palliative Care

Avoiding “Deceleration in Care”:Potential Organ Donor Family
• Supporting potential donor families is a process that begins at time of admission
• Supportive language enhances family understanding of brain death
• Supportive communication and education are key elements to a family support plan

Tissue Donor Referral
Every Death is a Potential Tissue Donor
• Report the death to LOPA within 4 hours @ 1.800.833.3666
• Notification of death paperwork must be completed and placed in patient chart
Tissue Donor Referral
Clinical Support Center (CSC) will:– Screen patient for suitability and check the
Donor Registry– Need Legal Next of Kin (LNOK) information
such as name, phone number, and relationship to deceased
– Give hospital a referral number to place on appropriate paperwork

Tissue Donor Referral
LOPA will:– Contact Coroner for clearance– Complete paperwork with family– Set Operating Room Time or arrange for
transport to LOPA Tissue Recovery Suite– Recover Tissue and Post-Recovery Care– Contact Funeral Home and Coroner once
recovery is completed

Tissues Recovered for Transplant
Eyes/corneas - restore sight
Heart Valves – valve replacement surgeries
Fascia – bladder suspension surgeries; dura replacement for craniotomies
Saphenous Veins – cardiovascular/ coronary by-pass surgeries
Tendons & Ligaments –reconstructive joint surgeries
Bones of Upper and Lower Extremities – spinal surgeries; limb salvage; cancer treatment; correction of birth defects
Skin – used for facial reconstruction and surgical repairs

Questions?????