does cannulation technique impact arteriovenous fistula ... cannt does... · does cannulation...
TRANSCRIPT

Does cannulation technique impact arteriovenous fistula
and graft survival?
Maria Teresa Parisotto| CANNT 2017 | Halifax| October 20th, 2017

Preserving the AVF as the patient lifeline: reduced mortality with the AVF compare to Catheter
Polkinghorne et al. J Am Soc Nephrol 15: 477-486, 2004
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 2 CANNT 20.10.2017
0
0.2
0.4
0.6
0.8
1
0 12 24 36
AVF
Catheter
Su
rviv
al
Months
p<0.001
ANZDATA Register

Vascular Access Major Cause of Hospitalisation
Rayner et al. Nephrol Dial Transplant 19: 108-120, 2004
0%
20%
40%
60%
80%
100%
France Germany Italy Spain UK
CV related VA related Infection related Gastrointestinal
DOPPS
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 3 CANNT 20.10.2017

% of VA cannulations
Thrombosis 16,5%
Hemorrage 7,5%
Infection 5,5%
Aneurysm 4,1%
Complications Associated to VA Cannulation
Yürügen and Erdogan, J Vasc Access 2001; 2: 119-124 (Data from Master Thesis at Istanbul University)
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 4 CANNT 20.10.2017

Preserving the Vascular Access is our responsibility
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 5 CANNT 20.10.2017

Phases of Vascular Access Management
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 6 CANNT 20.10.2017
Assessment and
preparation
Cannulation
Monitoring
during treatment
Disconnection
VA creation
Haemostasis
VA surveillance

Phases of Vascular Access Management
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 7 CANNT 20.10.2017
Assessment and
preparation
Cannulation
Monitoring
during treatment
Disconnection
VA creation
Haemostasis
VA surveillance
Fresenius Medical Care
Survey

Vascular Access Cannulation: Study Design
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 8 CANNT 20.10.2017
1. Objective:
Snapshot on the current practice of vascular access cannulation
2. Design:
International, multi-centre, observational, cross-sectional survey
3. Centres:
Dialysis centres of the Fresenius Medical Care network in Europe, Middle East, Africa, participation on voluntary basis
4. Procedures:
Anonymous documentation of vascular access and its cannulation once per patient (Patient Questionnaire) at appointed date (April ‘09)

Vascular Access Cannulation: Inclusion criteria
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 9 CANNT 20.10.2017

Vascular Access Cannulation: Participating Countries and Centres
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 10 CANNT 20.10.2017
33/1,729
5/496 31/1,048
34/
3,394
(Numbers: Centres/Patients by country)
+ South Africa
2/41 44/2,097
4/256
4/766
10/870
4/110
10 countries / 171 centres / 10,807 patients

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 11 CANNT 20.10.2017

Descriptive Statistics
Type of Vascular Access:
AVF: 90.9%
AVG : 9.1%
Location of the VA:
Arm: 98.7%
Leg: 1.3%
Left arm: 72.2%
Right arm: 21.8%
Lower arm 49.6%
Upper arm: 50.4%
Descriptive Statistics
Cannulation technique:
Area: 61.0%
Rope Ladder: 31.0%
Buttonhole: 6.1%
Missing data 1.8%
Survey results (1/2)
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 12 CANNT 20.10.2017

Descriptive Statistics
Needle sizes:
15G: 61.3%
16G : 33.2%
14G: 3.0%
17G: 2.5%
Direction of arterial needle puncture:
Antegrade: 63.0% Retrograde: 37.0%
Direction of bevel:
Upward: 72.3% Downward: 27.7%
Descriptive Statistics
Rotation of needle after cannulation:
Yes: 43.2% No: 54.5%
Nurses 'experience in dialysis
> 5 years: 66.0%
2 – 5 years: 19.0%
1 – 2 years 7.0%
< 1 year 8.0%
Survey results (2/2)
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 13 CANNT 20.10.2017
With the data collected we did three types of evaluations:
1. The variables possibly influencing the probability of reaching an adequate dialysis dose (Kt/V ≥ 1.2)
2. The nursing practices possibly influencing the development of “acute cannulation complications” (multiple-cannulation, infiltration, haematoma, haemorrhage, unknown)
3. The cannulation technique vs vascular access survival (7.058 patients observed for 3 years)
Analysis of the data
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 14 CANNT 20.10.2017

1. Analysis of variables related to the probability of reaching an adequate dialysis dose
Logistic regression on the odds ratio to reach Kt/V > 1.2
Odds ratio 95% confidence interval P-value
Gender (male vs. female) 0.293 0.243 - 0.354 <0.001 Post-dialytic body weight (per kg) 0.938 0.933 - 0.944 <0.001 Treatment time (per min) 1.036 1.032 - 1.041 <0.001 Treatment modality (on-line HDF vs. HD) 1.886 1.603 - 2.219 <0.001 Direction of arterial needle (retrograde vs. antegrade) 1.275 1.088 - 1.494 0.003 Needle size (vs. 17 G) 16 G 2.962 1.786 – 4.913 <0.001 15 G 6.626 3.963 – 11.079 <0.001 14 G 12.145 6.016 – 24.520 <0.001 Fistula type (graft vs. native arterio-venous fistula) 1.930 1.446 – 2.576 <0.001 Blood flow (vs. < 300 ml/min) 300 – 350 2.172 1.755 – 2.687 <0.001 350 – 400 2.651 2.103 – 3.343 <0.001 >400 3.156 2.274 – 4.380 <0.001 Dialyser surface (vs. 1.30 – 1.50 m2) 1.51 – 1.80 1.582 1.279 – 1.957 <0.001 >1.80 1.578 1.222 – 2.037 <0.001
Gauly A, Parisotto MT, et al. “Vascular Access Cannulation in Hemodialysis Patients – A Survey of Current Practice and its Relation to Dialysis Dose”. JVasc Access 2011; 12 (4): 358-364
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 15 CANNT 20.10.2017

1. Analysis of variables related to the probability of reaching an adequate dialysis dose
Logistic regression on the odds ratio to reach Kt/V > 1.2
Odds ratio 95% confidence interval P-value
Gender (male vs. female) 0.293 0.243 - 0.354 <0.001 Post-dialytic body weight (per kg) 0.938 0.933 - 0.944 <0.001 Treatment time (per min) 1.036 1.032 - 1.041 <0.001 Treatment modality (on-line HDF vs. HD) 1.886 1.603 - 2.219 <0.001 Direction of arterial needle (retrograde vs. antegrade) 1.275 1.088 - 1.494 0.003 Needle size (vs. 17 G) 16 G 2.962 1.786 – 4.913 <0.001 15 G 6.626 3.963 – 11.079 <0.001 14 G 12.145 6.016 – 24.520 <0.001 Fistula type (graft vs. native arterio-venous fistula) 1.930 1.446 – 2.576 <0.001 Blood flow (vs. < 300 ml/min) 300 – 350 2.172 1.755 – 2.687 <0.001 350 – 400 2.651 2.103 – 3.343 <0.001 >400 3.156 2.274 – 4.380 <0.001 Dialyser surface (vs. 1.30 – 1.50 m2) 1.51 – 1.80 1.582 1.279 – 1.957 <0.001 >1.80 1.578 1.222 – 2.037 <0.001
Gauly A, Parisotto MT, et al. “Vascular Access Cannulation in Hemodialysis Patients – A Survey of Current Practice and its Relation to Dialysis Dose”. JVasc Access 2011; 12 (4): 358-364
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 16 CANNT 20.10.2017

1. Analysis of variables related to the probability of reaching an adequate dialysis dose
Logistic regression on the odds ratio to reach Kt/V > 1.2
Odds ratio 95% confidence interval P-value
Gender (male vs. female) 0.293 0.243 - 0.354 <0.001 Post-dialytic body weight (per kg) 0.938 0.933 - 0.944 <0.001 Treatment time (per min) 1.036 1.032 - 1.041 <0.001 Treatment modality (on-line HDF vs. HD) 1.886 1.603 - 2.219 <0.001 Direction of arterial needle (retrograde vs. antegrade) 1.275 1.088 - 1.494 0.003 Needle size (vs. 17 G) 16 G 2.962 1.786 – 4.913 <0.001 15 G 6.626 3.963 – 11.079 <0.001 14 G 12.145 6.016 – 24.520 <0.001 Fistula type (graft vs. native arterio-venous fistula) 1.930 1.446 – 2.576 <0.001 Blood flow (vs. < 300 ml/min) 300 – 350 2.172 1.755 – 2.687 <0.001 350 – 400 2.651 2.103 – 3.343 <0.001 >400 3.156 2.274 – 4.380 <0.001 Dialyser surface (vs. 1.30 – 1.50 m2) 1.51 – 1.80 1.582 1.279 – 1.957 <0.001 >1.80 1.578 1.222 – 2.037 <0.001
Gauly A, Parisotto MT, et al. “Vascular Access Cannulation in Hemodialysis Patients – A Survey of Current Practice and its Relation to Dialysis Dose”. JVasc Access 2011; 12 (4): 358-364
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 17 CANNT 20.10.2017

2. Logistic regression model evaluating nursing practice in respect to the event “acute cannulation complication” (multiple-cannulation, infiltration, haematoma, haemorrhage, unknown)
Nursing practice aspect
OR
95% confidence Interval
p-value
Variable Reference Category Lower limit Higher limit
Needle gauge 15
14 0.545 0.199 1.491 NS
16 1.305 1.016 1.676 0.037
17 4.245 2.548 7.072 <0.001
Back-eye needle No Yes 1.879 1.409 2.508 <0.001
Cannulation technique Rope-Ladder Buttonhole 0.559 0.332 0.942 0.029
Area 0.613 0.482 0.780 <0.001
1st needle inserted Arterial Venous 1.677 1.306 2.155 <0.001
Needle axis rotation No Yes 1.522 1.206 1.921 <0.001
Needle fixation Butterfly
Chevron 0.836 0.474 1.475 NS
U-Shape 0.754 0.461 1.232 NS
Others 0.561 0.347 0.905 0.018
Parisotto MT et Al.“Elements of dialysis nursing practice associated with successful cannulation: result of an international survey” J Vasc Access 2017; 18(2): 114 – 119. Open Access DOI: 10.5301/jva.5000617
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 18 CANNT 20.10.2017

Nursing practice aspect
OR
95% confidence Interval
p-value
Variable Reference Category Lower limit Higher limit
Needle gauge 15
14 0.545 0.199 1.491 NS
16 1.305 1.016 1.676 0.037
17 4.245 2.548 7.072 <0.001
Back-eye needle No Yes 1.879 1.409 2.508 <0.001
Cannulation technique Rope-Ladder Buttonhole 0.559 0.332 0.942 0.029
Area 0.613 0.482 0.780 <0.001
1st needle inserted Arterial Venous 1.677 1.306 2.155 <0.001
Needle axis rotation No Yes 1.522 1.206 1.921 <0.001
Needle fixation Butterfly
Chevron 0.836 0.474 1.475 NS
U-Shape 0.754 0.461 1.232 NS
Others 0.561 0.347 0.905 0.018
Parisotto MT et Al.“Elements of dialysis nursing practice associated with successful cannulation: result of an international survey” J Vasc Access 2017; 18(2): 114 – 119. Open Access DOI: 10.5301/jva.5000617
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 19 CANNT 20.10.2017
2. Logistic regression model evaluating nursing practice in respect to the event “acute cannulation complication” (multiple-cannulation, infiltration, haematoma, haemorrhage, unknown)

● Out of the 10,807 patients enrolled for the original survey, access survival data was available for 7,058 (65%)
● Primary outcome was the time of the first surgical access intervention, where survey date serves as baseline.
● The observation period was 3 years (from April 2009 till March 2012).
● To adjust for individual patient differences, the following information was extracted from the clinical
database:
• Patient age and gender, BMI, prevalence of diabetes, use of ACE inhibitors, platelet anti-aggregants, salicylic acid and anticoagulants.
3. Cannulation techniques vs vascular access survival (1/3)
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 20 CANNT 20.10.2017
Mean age was 63.5+15.0 years;
38.5% were female;
27.1% were diabetics;
90.6% had a native fistula;
9.4% had a graft;
51.2% of patients, had a distal access location;
51.1% were treated with anti-aggregants;
2.8% anti-coagulant.
Descriptive Statistics

● Out of the 10,807 patients enrolled for the original survey, access survival data was available for 7,058 (65%)
● Primary outcome was the time of the first surgical access intervention, where survey date serves as baseline.
● The observation period was 3 years (from April 2009 till March 2012).
● To adjust for individual patient differences, the following information was extracted from the clinical
database:
• Patient age and gender, BMI, prevalence of diabetes, use of ACE inhibitors, platelet anti-aggregants, salicylic acid and anticoagulants.
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 21 CANNT 20.10.2017
3. Cannulation techniques vs vascular access survival (1/3)
Needle sizes:
15G: 63.7%
16G : 32.2%
14G: 2,7%
17G: 1.4%
Cannulation technique:
Area: 65.8%
Rope Ladder: 28.2%
Buttonhole: 6%
Descriptive Statistics

● Out of the 10,807 patients enrolled for the original survey, access survival data was available for 7,058 (65%)
● Primary outcome was the time of the first surgical access intervention, where survey date serves as baseline.
● The observation period was 3 years (from April 2009 till March 2012).
● To adjust for individual patient differences, the following information was extracted from the clinical
database:
• Patient age and gender, BMI, prevalence of diabetes, use of ACE inhibitors, platelet anti-aggregants, salicylic acid and anticoagulants.
Direction of arterial puncture:
Antegrade: 57.3% Retrograde: 42.7%
The prevalent combination between arterial needle puncturing and bevel direction:
Antegrade with bevel upward: 43.1% Retrograde with bevel down: 27.1%
Median blood flow:
350 -400 mL / min
Descriptive Statistics
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 22 CANNT 20.10.2017
3. Cannulation techniques vs vascular access survival (1/3)

Parameter Category Reference HR 95% CI p value Marginal
p value
Age 18-50 years 65-76 years >75 years
50-65 years 1.01 1.03 1.45
0.86 0.89 1.26
1.19 1.18 1.67
0.91 0.72 <0.0001
<0.0001
Gender Male Female 0.93 0.84 1.04 0.21
Diabetes Yes No 1.12 1.00 1.26 0.06
Heart failure Yes No 1.39 1.12 1.72 0.003
Vintage 6-24 months ≥24 months Unknown
0-6 months 1.04 0.98 0.55
0.81 0.77 0.26
1.33 1.24 1.18
0.79 0.84 0.13
0.34
Platelet Antiaggregants
Yes No 1.11 1.00 1.24 0.05
Fistula type Graft Fistula 1.74 1.48 2.06 <0.0001
AV-fistula location Right Left 1.13 1.01 1.27 0.03
AV-fistula location Proximal Distal 1.49 1.33 1.67 <0.0001
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 23 CANNT 20.10.2017
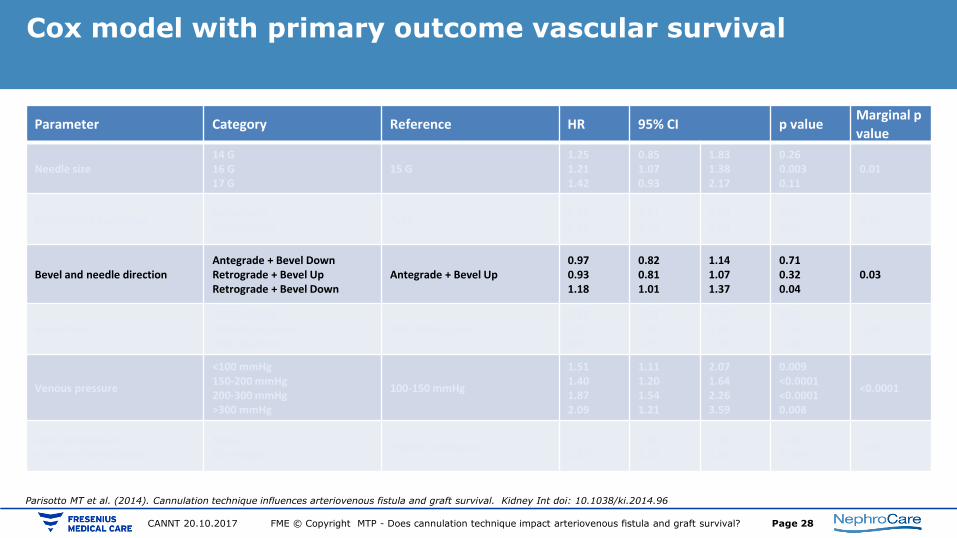
Cox model with primary outcome vascular survival
Parisotto MT et al. (2014). Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int doi: 10.1038/ki.2014.96

Parameter Category Reference HR 95% CI p value Marginal p
value
Needle size 14 G 16 G 17 G
15 G 1.25 1.21 1.42
0.85 1.07 0.93
1.83 1.38 2.17
0.26 0.003 0.11
0.01
Cannulation technique Buttonhole Rope-Ladder
Area 0.78 0.89
0.61 0.79
1.00 1.00
0.05 0.06
0.04
Bevel and needle direction Antegrade + Bevel Down Retrograde + Bevel Up Retrograde + Bevel Down
Antegrade + Bevel Up 0.97 0.93 1.18
0.82 0.81 1.01
1.14 1.07 1.37
0.71 0.32 0.04
0.03
Blood flow <300 mL/min 350-400 mL/min >400 mL/min
300-350 mL/min 1.18 0.91 0.93
1.01 0.80 0.75
1.36 1.04 1.15
0.03 0.16 0.49
0.03
Venous pressure
<100 mmHg 150-200 mmHg 200-300 mmHg >300 mmHg
100-150 mmHg
1.51 1.40 1.87 2.09
1.11 1.20 1.54 1.21
2.07 1.64 2.26 3.59
0.009 <0.0001 <0.0001 0.008
<0.0001
Arm compression at time of cannulation
None Tourniquet
Patient assistance 1.25 1.30
1.04 1.07
1.49 1.58
0.02 0.008
0.02
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 24 CANNT 20.10.2017
Parisotto MT et al. (2014). Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int doi: 10.1038/ki.2014.96
Cox model with primary outcome vascular survival

Parameter Category Reference HR 95% CI p value Marginal p
value
Needle size 14 G 16 G 17 G
15 G 1.25 1.21 1.42
0.85 1.07 0.93
1.83 1.38 2.17
0.26 0.003 0.11
0.01
Cannulation technique Buttonhole Rope-Ladder
Area 0.78 0.89
0.61 0.79
1.00 1.00
0.05 0.06
0.04
Bevel and needle direction Antegrade + Bevel Down Retrograde + Bevel Up Retrograde + Bevel Down
Antegrade + Bevel Up 0.97 0.93 1.18
0.82 0.81 1.01
1.14 1.07 1.37
0.71 0.32 0.04
0.03
Blood flow <300 mL/min 350-400 mL/min >400 mL/min
300-350 mL/min 1.18 0.91 0.93
1.01 0.80 0.75
1.36 1.04 1.15
0.03 0.16 0.49
0.03
Venous pressure
<100 mmHg 150-200 mmHg 200-300 mmHg >300 mmHg
100-150 mmHg
1.51 1.40 1.87 2.09
1.11 1.20 1.54 1.21
2.07 1.64 2.26 3.59
0.009 <0.0001 <0.0001 0.008
<0.0001
Arm compression at time of cannulation
None Tourniquet
Patient assistance 1.25 1.30
1.04 1.07
1.49 1.58
0.02 0.008
0.02
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 25 CANNT 20.10.2017
Parisotto MT et al. (2014). Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int doi: 10.1038/ki.2014.96
Cox model with primary outcome vascular survival

Parameter Category Reference HR 95% CI p value Marginal p
value
Needle size 14 G 16 G 17 G
15 G 1.25 1.21 1.42
0.85 1.07 0.93
1.83 1.38 2.17
0.26 0.003 0.11
0.01
Cannulation technique Buttonhole Rope-Ladder
Area 0.78 0.89
0.61 0.79
1.00 1.00
0.05 0.06
0.04
Bevel and needle direction Antegrade + Bevel Down Retrograde + Bevel Up Retrograde + Bevel Down
Antegrade + Bevel Up 0.97 0.93 1.18
0.82 0.81 1.01
1.14 1.07 1.37
0.71 0.32 0.04
0.03
Blood flow <300 mL/min 350-400 mL/min >400 mL/min
300-350 mL/min 1.18 0.91 0.93
1.01 0.80 0.75
1.36 1.04 1.15
0.03 0.16 0.49
0.03
Venous pressure
<100 mmHg 150-200 mmHg 200-300 mmHg >300 mmHg
100-150 mmHg
1.51 1.40 1.87 2.09
1.11 1.20 1.54 1.21
2.07 1.64 2.26 3.59
0.009 <0.0001 <0.0001 0.008
<0.0001
Arm compression at time of cannulation
None Tourniquet
Patient assistance 1.25 1.30
1.04 1.07
1.49 1.58
0.02 0.008
0.02
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 26 CANNT 20.10.2017
Parisotto MT et al. (2014). Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int doi: 10.1038/ki.2014.96
Cox model with primary outcome vascular survival

Parameter Category Reference HR 95% CI p value Marginal p
value
Needle size 14 G 16 G 17 G
15 G 1.25 1.21 1.42
0.85 1.07 0.93
1.83 1.38 2.17
0.26 0.003 0.11
0.01
Cannulation technique Buttonhole Rope-Ladder
Area 0.78 0.89
0.61 0.79
1.00 1.00
0.05 0.06
0.04
Bevel and needle direction Antegrade + Bevel Down Retrograde + Bevel Up Retrograde + Bevel Down
Antegrade + Bevel Up 0.97 0.93 1.18
0.82 0.81 1.01
1.14 1.07 1.37
0.71 0.32 0.04
0.03
Blood flow <300 mL/min 350-400 mL/min >400 mL/min
300-350 mL/min 1.18 0.91 0.93
1.01 0.80 0.75
1.36 1.04 1.15
0.03 0.16 0.49
0.03
Venous pressure
<100 mmHg 150-200 mmHg 200-300 mmHg >300 mmHg
100-150 mmHg
1.51 1.40 1.87 2.09
1.11 1.20 1.54 1.21
2.07 1.64 2.26 3.59
0.009 <0.0001 <0.0001 0.008
<0.0001
Arm compression at time of cannulation
None Tourniquet
Patient assistance 1.25 1.30
1.04 1.07
1.49 1.58
0.02 0.008
0.02
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 27 CANNT 20.10.2017
Parisotto MT et al. (2014). Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int doi: 10.1038/ki.2014.96
Cox model with primary outcome vascular survival
Parameter Category Reference HR 95% CI p value Marginal p
value
Needle size 14 G 16 G 17 G
15 G 1.25 1.21 1.42
0.85 1.07 0.93
1.83 1.38 2.17
0.26 0.003 0.11
0.01
Cannulation technique Buttonhole Rope-Ladder
Area 0.78 0.89
0.61 0.79
1.00 1.00
0.05 0.06
0.04
Bevel and needle direction Antegrade + Bevel Down Retrograde + Bevel Up Retrograde + Bevel Down
Antegrade + Bevel Up 0.97 0.93 1.18
0.82 0.81 1.01
1.14 1.07 1.37
0.71 0.32 0.04
0.03
Blood flow <300 mL/min 350-400 mL/min >400 mL/min
300-350 mL/min 1.18 0.91 0.93
1.01 0.80 0.75
1.36 1.04 1.15
0.03 0.16 0.49
0.03
Venous pressure
<100 mmHg 150-200 mmHg 200-300 mmHg >300 mmHg
100-150 mmHg
1.51 1.40 1.87 2.09
1.11 1.20 1.54 1.21
2.07 1.64 2.26 3.59
0.009 <0.0001 <0.0001 0.008
<0.0001
Arm compression at time of cannulation
None Tourniquet
Patient assistance 1.25 1.30
1.04 1.07
1.49 1.58
0.02 0.008
0.02
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 28 CANNT 20.10.2017
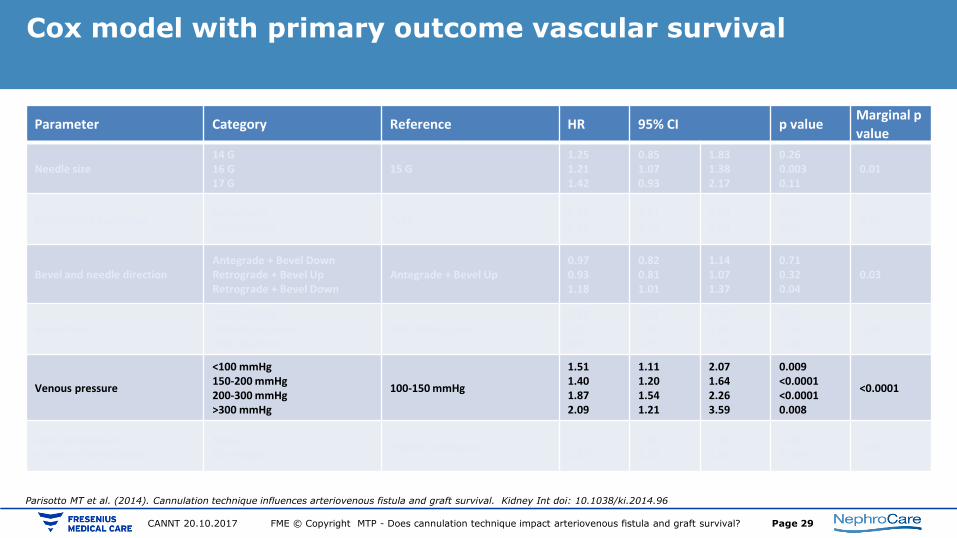
Parisotto MT et al. (2014). Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int doi: 10.1038/ki.2014.96
Cox model with primary outcome vascular survival
Parameter Category Reference HR 95% CI p value Marginal p
value
Needle size 14 G 16 G 17 G
15 G 1.25 1.21 1.42
0.85 1.07 0.93
1.83 1.38 2.17
0.26 0.003 0.11
0.01
Cannulation technique Buttonhole Rope-Ladder
Area 0.78 0.89
0.61 0.79
1.00 1.00
0.05 0.06
0.04
Bevel and needle direction Antegrade + Bevel Down Retrograde + Bevel Up Retrograde + Bevel Down
Antegrade + Bevel Up 0.97 0.93 1.18
0.82 0.81 1.01
1.14 1.07 1.37
0.71 0.32 0.04
0.03
Blood flow <300 mL/min 350-400 mL/min >400 mL/min
300-350 mL/min 1.18 0.91 0.93
1.01 0.80 0.75
1.36 1.04 1.15
0.03 0.16 0.49
0.03
Venous pressure
<100 mmHg 150-200 mmHg 200-300 mmHg >300 mmHg
100-150 mmHg
1.51 1.40 1.87 2.09
1.11 1.20 1.54 1.21
2.07 1.64 2.26 3.59
0.009 <0.0001 <0.0001 0.008
<0.0001
Arm compression at time of cannulation
None Tourniquet
Patient assistance 1.25 1.30
1.04 1.07
1.49 1.58
0.02 0.008
0.02
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 29 CANNT 20.10.2017
Parisotto MT et al. (2014). Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int doi: 10.1038/ki.2014.96
Cox model with primary outcome vascular survival

• In summary, the study revealed that area cannulation technique, despite being the most commonly used, was inferior to both rope-ladder and buttonhole for the maintenance of Vascular Access functionality.
• With regard to the effect of needle and bevel direction, the combination of antegrade position of arterial needle with bevel up or down was significantly associated with better access survival than retrograde positioning with bevel down.
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 30 CANNT 20.10.2017
Cannulation technique vs VA survival: Summary (1/2)

• Results referring to the type and location of access and the technical parameters (i.e. venous pressure) were as follows:
• There was an increased risk of access failure for graft versus fistula, proximal vs distal location, right arm vs left arm, and the presence of a venous pressure greater than 150 mmHg.
• The results on venous pressure are worth considering. A venous pressure of 200-250 mmHg is considered acceptable by the scientific community; the results of this study put these values under discussion. However, further investigations are required to clarify the topic fully.
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 31 CANNT 20.10.2017
Cannulation technique vs VA survival: Summary (2/2)

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 32 CANNT 20.10.2017

• Needle 17G – Ø 1.5 mm • Needle 15G – Ø 1.8 mm
Needle diameter vs blood flow and flow pattern vector
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 33 CANNT 20.10.2017

Effect of needle angle during the treatment Fulker D. et al. The flow field near a venous needle in hemodialysis: a computational study.
Hemodial Int. 2013 Oct;17(4):602-11. doi: 10.1111/hdi.12029. Epub 2013 Mar 1.
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 34 CANNT 20.10.2017

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 35 CANNT 20.10.2017
Effect of needle depth during the treatment Fulker D. et al. The flow field near a venous needle in hemodialysis: a computational study.
Hemodial Int. 2013 Oct;17(4):602-11. doi: 10.1111/hdi.12029. Epub 2013 Mar 1.

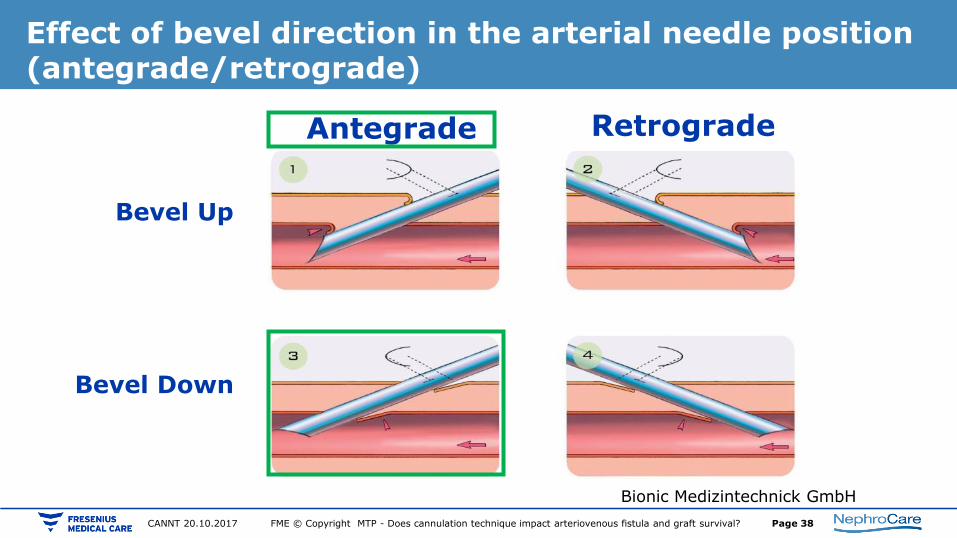
Antegrade puncturing may be fistula protective
• Increased risk of haematoma formation from retrograde filling
• Tract closure through flow force by antegrade puncture
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 36 CANNT 20.10.2017

Effect of bevel direction in the arterial needle position (antegrade/retrograde)
Bevel Up
Bionic Medizintechnick GmbH
Bevel Down
Antegrade Retrograde
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 37 CANNT 20.10.2017
Effect of bevel direction in the arterial needle position (antegrade/retrograde)
Bevel Up
Bionic Medizintechnick GmbH
Bevel Down
Antegrade Retrograde
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 38 CANNT 20.10.2017

Effect of bevel direction in the arterial needle position (antegrade/retrograde)
Bevel Up
Bionic Medizintechnick GmbH
Bevel Down
Antegrade Retrograde
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 39 CANNT 20.10.2017

Arterial needle antegrade: Effect of bevel up direction
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 40 CANNT 20.10.2017

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 41 CANNT 20.10.2017
Arterial needle antegrade: Effect of bevel up direction

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 42 CANNT 20.10.2017
Arterial needle antegrade: Effect of bevel up direction

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 43 CANNT 20.10.2017
Arterial needle antegrade: Effect of bevel up direction

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 44 CANNT 20.10.2017
Arterial needle antegrade: Effect of bevel up direction

FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 45 CANNT 20.10.2017
Arterial needle antegrade: Effect of bevel up direction

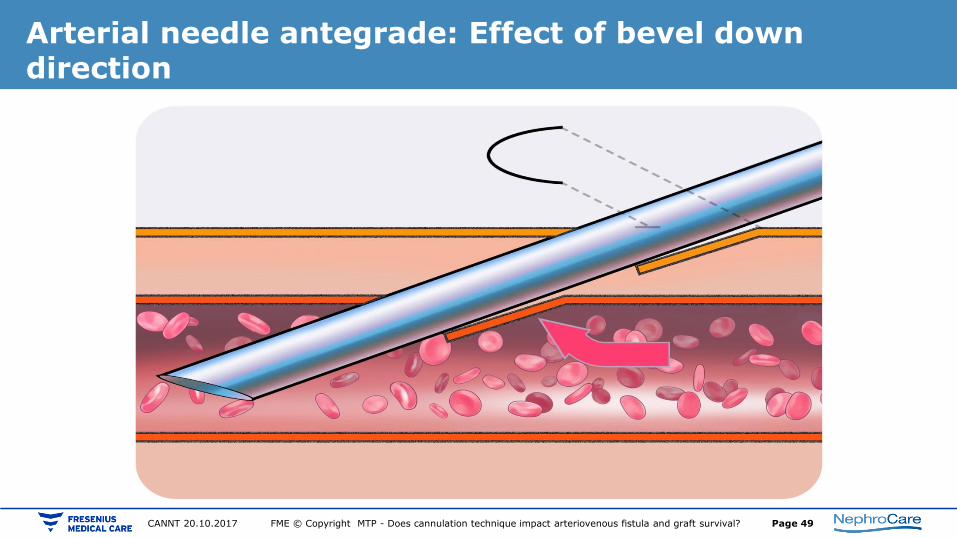
Arterial needle antegrade: Effect of bevel down direction
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 46 CANNT 20.10.2017

Arterial needle antegrade: Effect of bevel down direction
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 47 CANNT 20.10.2017

Arterial needle antegrade: Effect of bevel down direction
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 48 CANNT 20.10.2017
Arterial needle antegrade: Effect of bevel down direction
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 49 CANNT 20.10.2017

Arterial needle antegrade: Effect of bevel down direction
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 50 CANNT 20.10.2017

• “… , taking access blood flow into consideration, no association was found between VA failure and extracorporeal blood flow for the range of extracorporeal blood flows commonly used in routine dialysis practice.
• Low extracorporeal blood flow (<310 mL/min) seems to be a surrogate for poor access blood flow.
• Some caution appears indicated when applying particularly high extracorporeal blood flow (>390 mL/min).”
Ponce P. et al. Hemodialysis International 2014 - Does the extracorporeal blood flow affect survival of the arteriovenous vascular access?
Blood flow and vascular access survival
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 51 CANNT 20.10.2017

• “… , taking access blood flow into consideration, no association was found between VA failure and extracorporeal blood flow for the range of extracorporeal blood flows commonly used in routine dialysis practice.
• Low extracorporeal blood flow (<310 mL/min) seems to be a surrogate for poor access blood flow.
• Some caution appears indicated when applying particularly high extracorporeal blood flow (>390 mL/min).”
Blood flow and vascular access survival
Ponce P. et al. Hemodialysis International 2014 - Does the extracorporeal blood flow affect survival of the arteriovenous vascular access?
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 52 CANNT 20.10.2017
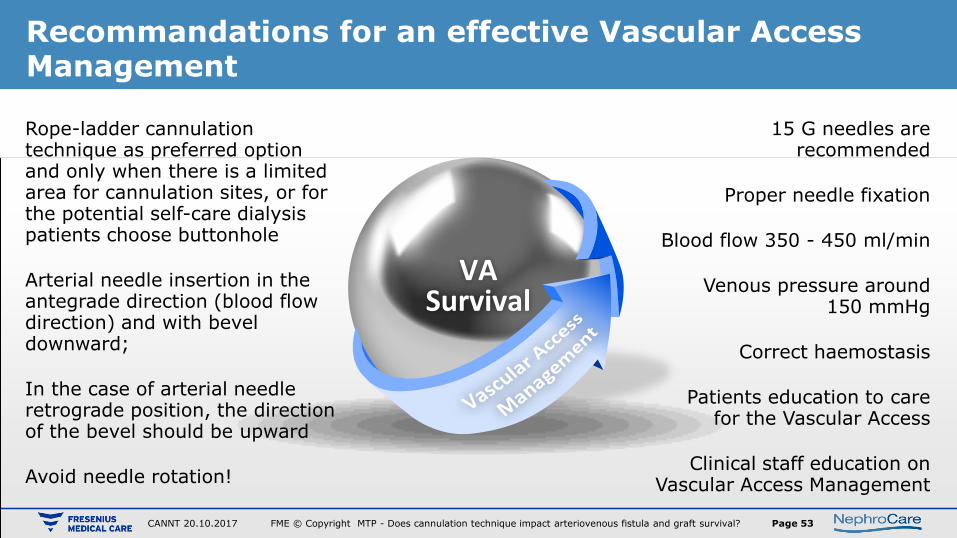
Recommandations for an effective Vascular Access Management
VA Survival
Rope-ladder cannulation technique as preferred option and only when there is a limited area for cannulation sites, or for the potential self-care dialysis patients choose buttonhole
Arterial needle insertion in the antegrade direction (blood flow direction) and with bevel downward;
In the case of arterial needle retrograde position, the direction of the bevel should be upward
Avoid needle rotation!
15 G needles are recommended
Proper needle fixation
Blood flow 350 - 450 ml/min
Venous pressure around 150 mmHg
Correct haemostasis
Patients education to care for the Vascular Access
Clinical staff education on Vascular Access Management
FME © Copyright MTP - Does cannulation technique impact arteriovenous fistula and graft survival? Page 53 CANNT 20.10.2017
