documenting rehab services for a medicare reviewer for referral must be comprehensive and complete...
TRANSCRIPT

Documenting Rehab Services
For a Medicare Reviewer
Jaclyn Warshauer, PT
LeadingAge Missouri 9/27/2012

2
Practice Settings
The basic concept of documenting medical
necessity and skilled services transcends
all therapy disciplines and all practice
settings
This presentation will focus on what a
medical reviewer will look for in
documentation regardless of setting

3
Objectives
Understand the medical review process
Learn the key pieces of documentation
that “sell” the reviewer
Understand the pros and cons of
electronic documentation

The Importance of Good
Medical Records

5
Why Document Well??
Documenting is part of providing care – it’s
not optional
Necessary tool for tracking success and
making treatment modifications when
indicated
Expectation from regulators, payors and
patients in order to get paid
Used to defend our care
6
Why Document Well??
According to the GAO, for fiscal year 2010, HHS reported an estimate of almost $48 billion in Medicare improper payments
Causes cited include inadequate documentation, medically unnecessary services, coding errors
GAO recommendations:
Improve (expand) prepayment reviews
Develop a “robust” process to identify vulnerabilities

7
Why Document Well??
The health care reform law provides $350
million to fight fraud, waste, and abuse
new provisions that provide for enhanced
electronic data collection, screening, and
mining designed to aid in identifying problem
areas and problem providers

The Scoop on Medical
Reviewers

9
Medical Reviewers
Vast majority are nurses
Reviewers have productivity requirements
To PAY a claim is a simple 2-step process
To DENY a claim is a time consuming
multiple step process
Reviewers are audited too

10
Productivity
How you can help
Document payable services
Quality, not Quantity Clear, concise, objective, measurable,
functional and legible
Paint the complexity of the patient’s condition
Describe the complex nature of the treatment
provided
Assessment of the patient/activity and the
treatment adjustments made

Medical Review Selection

12
Medical Review Cannot Look
at Every Record

13
Medical Review (MR) Selection
Providers may be selected for MR when
Atypical billing patterns are identified
Data Mining (looking for Outliers)
A particular kind of problem is identified
Such as errors in billing a specific service
Evaluation of other information, such as OIG
work plan, CERT error rate reports, RAC
vulnerabilities, GAO reports

14
Physical Therapy: Length of Service
Jan - Mar 2011 (example)
18.0
16.0
20.0
36.3
12.8
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
State Avg Provider 1 Provider 2 Provider 3 Provider 4

15
Don’t be an Outlier
Do not to fall into treatment/documentation
patterns of:
ICD-9 Codes
CPT Codes
RUG levels
Frequency
Duration
UNIQUE
PATIENT
INDIVIDUALIZED
PLAN OF CARE

16
If you are an outlier…
Recognize when you might be an outlier
There are valid reasons to be an outlier
Be diligent in your documentation
If identified as an outlier and/or on probe
review:
EXTRA diligent in documentation
All payment decisions are made based on the
documentation, and the documentation alone

Documentation -
Selling the Reviewer
A few quick points…

18
Documentation
Insurance coverage determinations are
made based on the documentation, and
the documentation alone
The reviewer knows nothing else about the
patient or the quality of your facility
The documentation is used to determine if
the patient’s condition and level of function
required the special knowledge and skills
of a therapist

19
Documentation – Paint a Picture
The therapist knows the
patient and any
complications in
physical, cognitive,
emotional,
psychological, and
social situations that
might affect their need
for skilled therapy
services
Documentation should
draw a picture of the
patient complexity for
medical reviewers
Documentation should
also paint a picture of
the sophisticated
nature of the
treatment provided

20
The Reviewer’s Thoughts
“Make it easy for me to pay this.”
Avoid making the reviewer search to
determine if the services are medically
necessary
Risks some important piece of information
being missed
Risks findings of inconsistencies in the
documentation = denials

21
Documentation Points
Today’s training will focus on some of the
key elements in the evaluation and
progress reports that assist the reviewer in
making medical necessity and skilled
services coverage decisions
Not an all inclusive listing of all elements that
should be part of these therapy reports

Initial Evaluation

23
Documentation
It’s all about the Initial Evaluation!
The initial evaluation sets the stage for all subsequent therapy services
Reviewers will begin to anticipate how much therapy might be needed for the condition described
Poor or scant evaluation documentation risks that ALL subsequent therapy services will be denied

24
Initial Evaluation
Descriptive
Must have some sentences/short paragraphs
Makes it a “real” patient for the reviewer
Avoid using check boxes/drop down boxes for
describing the Reason for Referral, Recent
History, and any Assessment Summaries
Narrative description describing the unique patient
history and condition is preferred
Connect the dots for the reviewer

25
Initial Evaluation
Complex
Describe the complex nature of the patient’s
condition
Where not obvious describe the impact the
complexities will have on the plan of treatment
Complexity = Amount of therapy

26
Initial Evaluation
Logical
Must make the reviewer think, “Oh, I can see
why this patient requires therapy now.”
Logical flow from the reason for referral, to the
examination findings/scores, to the selected
treatment interventions, and the subsequent
goals

27
Reason for Referral What Changed and Why
Describe the change in condition
Include the mechanism of injury or cause for the
change in condition
Reason for Referral must be comprehensive and
complete
Paint the picture for “Why Now”
Must be more than one sentence/phrase – should
tell the patient’s story
In many cases the reviewer should only have to read
the Reason for Referral to begin to conclude that
therapy is medically necessary

28
Reason for Referral Examples
Avoid: “Physician Referral.”
Avoid: “Recent hospitalization. Now
requires OT to regain function.”
Avoid: “SLP necessary to regain PLOF.”
Avoid: “Patient with decline in mobility
function. Would benefit from skilled PT.”

29
Reason for Referral Example
(Fracture) Patient is a 66 yo male who suffered a tibial fracture on 5/1/11 as a result of a fall down the stairs. The patient now presents to therapy with chief complaints of pain, stiffness, and weakness, and impaired ability to perform walking without a significant limp or at a normal speed, especially on uneven surfaces, occasionally requiring use of a single crutch. Patient requires a brace during ambulation. Therapy is necessary to regain PLOF of safe ambulation without a brace or crutch, and without significant deviations.

30
Reason for Referral Example
(Positioning) Pt is an 85 yo female resident of the SNF
who presents with increasing tone and contractures in
the right UE as a result of a previous CVA. Patient has
been on a restorative program. Nursing notes
increased positioning and ROM difficulties in the past
month which have resulted in difficulty achieving
adequate ROM in R UE for completing hygiene and an
increased concern for skin breakdown. Nursing
reports increasing frequency of PROM without
success. The patient is now being referred to therapy
to address positioning and ROM necessary for
hygiene and skin integrity.

31
Reason for Referral Example
(Functional Decline) Patient is a 73 year old female who presents with a decline in ability to dress, print and manipulate small items due to increased tremors, contracture of bilateral hands due to RA and poor ROM in left shoulder due to old MVA. The patient started noticing a decline approximately 1 month ago which has since resulted in the patient now requiring significantly more assistance for the completion of writing during bill pay, manipulating coins in hand during purchases and UB dressing. Due to co-morbidities, this patient will require the skilled intervention of a therapist in order to regain the lost function. Patient will also benefit from comprehensive HEP to maintain joint mobility, strength and overall function following D/C.

32
Reason for Referral Example
(Speech) Patient is a 93 year old female who
presents with a recent decline in abilities to
make wants and needs known due to severe
hearing impairment. Six months ago, the patient
was able to communicate wants and needs
effectively, but the patient since has had
difficulty with such things as making
independent choices during ADLs and
conversing with peers. Speech therapy and
aural rehabilitation is necessary to allow for
improved functional communication.

33
Reason for Referral Example
(SAH) 70 yo resident admitted to SNF following hospitalization for Subarachnoid hemorrhage for which she was treated surgically by aneurysm clipping. Post operatively she began to develop left sided weakness and facial droop. Cognitively, pt. is noted to have deficits of organization, recall, expressive language and articulation. Due to oral leakage, stasis, coughing, decreased lingual function and range of motion, pt. is currently NPO because it was felt that she could not get enough nourishment PO. A PEG tube is currently in place. SLP necessary to regain safe swallow and communication abilities to return home with husband.

34
Medical History
List the medical conditions and
complexities that are current and may
potentially have an impact on the therapy
plan of treatment
Listing every medical condition that patient
has ever had risks the reviewer not looking at
any of the conditions

35
Measuring Function
Document a Current Level of Function (LOF) measure for each functional deficit that you will be addressing in therapy Baseline from which to measure progress
Must also document a Prior LOF measure for each functional deficit addressed in therapy Reference for establishing appropriate LTGs
Used to determine the patient’s potential
Also include the overall PLOF such as “lived at home alone, drives, does yardwork…”, “resident of SNF…”, “Lived in ALF with 1 meal a day and once a week cleaning…”

36
Measuring Function
If there is little or no difference between
PLOF and CLOF provide written
justification for why therapy is medically
necessary
(Reviewers love objective measures!)

37
Why can’t I walk/talk/dress like before?
Underlying Impairments
A reviewer wants to know the answer to this question as well
The answer is in the Underlying Impairments
Need to measure every Underlying Impairment impacting the patient’s function that will be addressed in the plan of care Be thorough in your assessment
This is the Therapist’s bread & butter – this is what we get paid to treat
You can’t treat it if you didn’t measure or objectively describe it
(Reviewers love objective measures!)

38
Standardized Measurement Tools
Use standardized measurement tools when
possible
Tinetti, Berg Balance, DASH, Oswestry, Peabody,
NOMS, etc
Be sure to describe the value of the score for
the reviewer
ACL: 4.2 Moderate cognitive impairment
Borg: 5 Severe breathlessness
Berg: 39/56 Medium fall risk

39
What the reviewer is thinking so far…
The diagnoses, the medical history, and the reason
for referral suggest that this patient requires
therapy
Measurable change in function
that likely will not resolve on its own
The amount and type of impairments described are
consistent with the level of functional deficit

40
Plan of Care
Goals
Frequency & duration
Interventions
Logical plan of care based on the evaluation findings
The reviewer already has an idea of what your POC will be based upon your evaluation…there should be no surprises

41
Goals
Goals are part of the medical necessity
picture
All goals must be objective, measurable
and related to function
All goals should have a baseline measure
within the evaluation
Measured functional deficit – Measured
underlying impairment
(Reviewers love objective measures!)

42
Interventions
Can’t treat it if you didn’t measure it
No skilled pain assessment/description ≠ pain
modalities
No skilled cognitive assessment ≠ no
cognitive training
Can’t treat it if it’s WFL or WNL
Strength is WFL ≠ no strengthening ther ex

43
Rehabilitation Prognosis
Provide a prognosis and include a “due to” statement
Prognosis should be written related to the likelihood of achieving the therapy LTGs
“Prognosis for achieving goal is good due to recent PLOF of independent and motivation to regain independence.”
Rarely should prognosis be “poor”
Either the goals are not appropriate or no longer appropriate and should be adjusted, or the patient should be discharged

Progress Notes:
Supporting Coverage for
Ongoing Therapy

45
Coverage
Two factors mainly affect reimbursement
decisions – medical necessity and skilled
services
Inadequate documentation of medical
necessity and/or skilled services risks denial

46
Medical Necessity
WHY NOW?
Complex change in condition that
necessitates your skilled therapy
intervention
Functional Deficits related to Underlying
Impairments that fall within your Scope of
Practice

47
Skilled Services
WHY YOU?
Your skilled assessment, analysis,
adjustments, progressions and special
techniques that are necessary for this
patient to regain function (or to develop a
maintenance program)
The activities that only the therapist has the
knowledge to provide

48
Coverage
Complex Patient
Condition
Sophisticated Therapy
Treatment

Skilled Therapy

50
Skilled Therapy
Alleviating impairments and functional
limitations as determined by the
evaluation through...
designing,
implementing, and
modifying therapeutic interventions
Medicare pays for therapist’s brains,
not just hands!

51
Skilled Therapy
The services must be so inherently
complex that they can only be safely and
effectively performed by a
therapist/assistant
Services that can be performed by or taught
to non-skilled persons or can be completed as
an independent program are NOT skilled
therapy
Non-skilled: the patient, personal trainer, CNA,
spouse, caregiver, aide, tech, etc

52
Skilled Therapy
THERAPIST
Assessment
Analysis
Adjustments
Progressions
Modifications
Special techniques
ASSISTANT
Adjustments
Progressions
Special techniques

53
Skilled Therapy?
Skilled Services Provided:
US
Ther Ex
NMR
Ther Act
Self Care Training

54
Skilled Therapy?
Monday Wednesday Friday
Amb w/ ww 40’
min assist
Amb w/ ww 65’
min assist
Amb w/ ww 70’
CGA

55
Skilled Therapy?
6/15 6/17 6/19
Codmans x 25
Pulley 10 x 2
AROM FL 10 x 2
AROM ABD 10 x2
ER/IR 10 x 2
Codmans x 25
Pulley 15 x 2
AROM FL 10 x 2
AROM ABD 10 x2
ER/IR 15 x 2
Codmans x 25
Pulley 20 x 2
AROM FL 10 x 2
AROM ABD 10 x2
ER/IR 15 x 2

56
The Quick Hit Denial
Repetitive
Services

57
Skilled Services Easy Denial
Reviewers expect to see
documentation of adjustments,
progressions and/or
modifications to your treatment interventions

58
Bottom Line:
Description of your skilled analyses,
adjustments and progressions MUST be
documented
Assistants – except the “analysis piece”
Skilled treatment requires more documentation than just “ther ex” or “therapeutic activities”

Progress Notes
WHY IS THERAPY STILL
TREATING?
60
Why do we do Progress Notes?
Justification for treatment…
1. Provide an update on the patient’s status
1. Function
2. Underlying impairments
3. Goals
2. Describe the skilled services that have been
provided
3. Indentify the areas that will be addressed in the
upcoming week(s) to substantiate the need for
ongoing skilled intervention
61
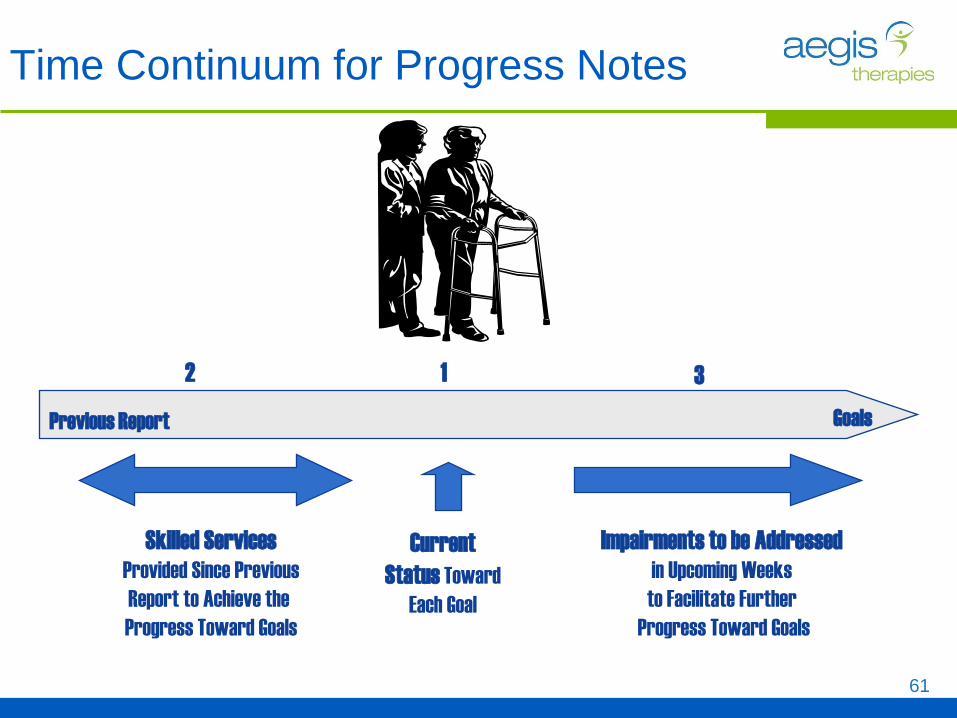
Time Continuum for Progress Notes
Goals
Current
Status Toward
Each Goal
Previous Report
Skilled Services
Provided Since Previous
Report to Achieve the
Progress Toward Goals
Impairments to be Addressed
in Upcoming Weeks
to Facilitate Further
Progress Toward Goals
1 2 3

Goal Status Update

63
Goals
Goal Prior Week
Level
Current Week
Level
Be sure to address all aspects of goals Each function addressed
Any underlying impairments
Don’t change the measurement scale mid-stream
Avoid not measuring a goal If unable to measure, give rationale for deferral
Recognize when a STG is met as stated Indicate GOAL MET
Upgrade, Discontinue, or add new goals as appropriate

64
Medical Necessity: Progress Toward Goals
According to CMS:
There must be an expectation that the patient’s
condition will improve significantly in a
reasonable (and generally predictable) period
of time, or the services must be necessary for
the establishment of a safe and effective
maintenance program required in connection
with a specific disease state
The plan should strive to provide treatment in
the most efficient and effective manner,
balancing the best achievable outcome
with the appropriate resources

65
Progress Toward Goals
Analyze, Modify & Justify Document the reasons for the delay in progress
Document measures taken to improve response
to treatment
Document why a positive response is expected
in the future
slow gains decline lack of gains

Documenting
Skilled Services Provided

67
Avoid the Litany of Services
AVOID: Listing of CPT descriptors
“Ther Ex, Ther Act, NMR, Diathermy”
AVOID: Listing of general treatment interventions
“ADLs, strengthening, balance, endurance, adaptive equipment training”
AVOID: Combination of the two
“Ther Ex for strengthening, Ther Act for transfers, NMR for balance, Diathermy for pain”

68
Skilled Services since Last Report
Provide a summary of ALL adjustments,
progressions, modifications and special
techniques provided since the last report
Need to “prove” to the reviewer that the
services are not repetitive
What did you do different this report period
than the last report period?

69
Skilled Services since Last Report
A statement or summary to justify the skilled nature of each CPT code billed since the last report
Not TASKS…but Adjustments, Progressions and Special Techniques
“Strengthening ex’s progressed to…”
“Balance activities advanced from __ to __...”
“Manual cues necessary during left LE stance to facilitate effective weight shift

70
Skilled Services Note
Therapist or Assistant
Progression of hip/glut strengthening ex’s
to now include weighted resistance;
progression of standing balance activities
from bilat support to unilat support; pre-
gait/balance activities that facilitate
unilateral LE standing, wt shifting,
clearance and step length. Required
manual cues to control movement of RLE
in swing phase of gait.”
97110, 97112, 97116

71
Skilled Services Note Therapist or Assistant
Manual therapy to reduce edema prior to
ther ex. Edema clearing in a shorter
amount of time. Able to increase motion
and stretch duration with prolonged stretch
to thumb flexors and fingers. Fine motor
coordination training advanced to include
smaller objects as pincer grasp improves.
Progressed HEP program to add nerf ball
squeezes for grip strength and ROM.
97140, 97110, 97112

72
Skilled Services
Design of strategies to enhance swallow
endurance over the course of a meal.
Introduced the use of an "effortful" swallow
with the cue to "feel the squeeze!". This
technique is designed to enhance bolus
propulsion and conservation of energy needed
for repetitive swallows over the course of a
meal. Implemented respiration coordination
strategies through the use of an incentive
spirometer to increase breath support.
92526
Patient/Caregiver Training

74
Patient/Caregiver Training
Reviewers like to see that you are involving the patients/caregivers in their care Demonstrates efficiency
Shows that you’re not using therapy time for unskilled activities
Talk about any training done – even if it’s very simple Discussed sitting posture to reduce back pain
Instructed in Ankle Pump exercise when sitting
Transition any ex’s that have become repetitive – no longer need skilled intervention Again, shows that you’re only using therapy time for those
activities that require skill
Document any updates or revisions to any previous instructions

Remaining Functional
Deficits

76
Remaining Functional Deficits/
Underlying Impairments
Be sure to MEASURE the functional
deficits and underlying impairments that
you are currently treating or will be treating
Measures are needed to support the medical
necessity of the specific interventions used
WHAT’S MISSING??
“Patient has the following remaining
impairments impacting function: dec’d
strength to all extremities, dec’d balance
and decreased endurance.”
(Reviewers Love Objective Measures!!)

77
Remaining Functional Deficits/
Underlying Impairments
Document occasionally to answer the
question
“Why can’t this patient continue to improve on
their own or with the help of a
caregiver/restorative aide program?”
What remains so complex about this patient?
Why are YOU still treating????
Medicare Manual Medical
Review: A Few Progress
Note Points…

79
Medicare Manual Medical Review
CMS is implementing an exceptions
process for beneficiaries that exceed
the $3700 therapy threshold
$3700 for OT ; $3700 for PT-SLP Combined
The Medicare FI/MAC will conduct
manual medical review of therapy
documentation to determine if an
exception will be granted

80
Extended Length of Stay
Supporting medical necessity as the patient
progresses through treatment becomes more
challenging
Balance between making progress and still
continuing to be complex
Documentation should demonstrate significant
meaningful and practical progress in a reasonable
period of time
Documentation needs to describe what remains
complex (through objective terms) about the patient
such that their care requires your level of skill

81
Extended Length of Stay
Supporting skilled services as the patient
progresses through treatment also becomes
more challenging
Need to clearly show that the services are not
“repetitive”
Need to show that the techniques remain complex
or the patient requires constant analysis and
adjustments
Reviewers are very focused on skilled services
when auditing the longer episodes of care
Remember that Quick Hit Denial for repetitive services?

Electronic Documentation

83
Electronic Documentation
Cons
The documentation is still only as good as the therapist making the entries Even with controls for “required” fields and
electronic mapping, need to do internal documentation audits
Difficult for the reviewer to obtain a unique picture of the patient (Significant con!) Feels like there’s just a bunch of dots on the page
and nothing is connected
Some documentation programs carry over entries from the previous days Denial risk

84
Electronic Documentation
Pros
LEGIBLE!
You can control the fields that are required
Allows for starter phrases or controlled entries using
language suggestive of medical necessity or skilled
services
Make use of the narrative entry areas! Show the individuality
of the patient’s condition and their plan of care
Reports and alerts for missing or incomplete
documentation
Can be accessed from a distance
