dmards in management of axial ankylosing spondylitis
TRANSCRIPT
DMARDs in Management of Axial Ankylosing Spondylitis
Dr. Homayra Tahseen Hossain
Assistant Professor , Medicine Popular Medical College Hospital
1
Introduction
• Ankylosing spondylitis (AS, from Greek ankylos, crooked; spondylos, vertebra; -itis, inflammation),
• is a chronic inflammatory disease of the axial skeleton, with variable involvement of peripheral joints and nonarticular structures.
2
• AS is one of the sero -ve spondyloarthropathies.
• It has strong genetic predisposition , > 90 % HLA B27 positive.
3
Eppppppppppp
• Prevalence- 0.2-0.9% • Age of onset- onset usually peaks in 2nd &
3rd decades of life. • Gender- occurs more frequently in male (male: female- 3:1)
4
Dpppppppp
• The diagnosis of AS requires fulfilment of the modified New York criteria.
• It requires at least 1 clinical manifestation and at least 1 radiographic parameter.
5
Dppppppppppppppppp
• Clinical manifestations include ≥ 3 months of inflammatory back pain that
improves with exercise and exacerbated by rest, limitation of lumbar motion in both frontal
and sagittal planes, and limitation of chest expansion compared to the
normative population.
6
Dppppppppppppppppp
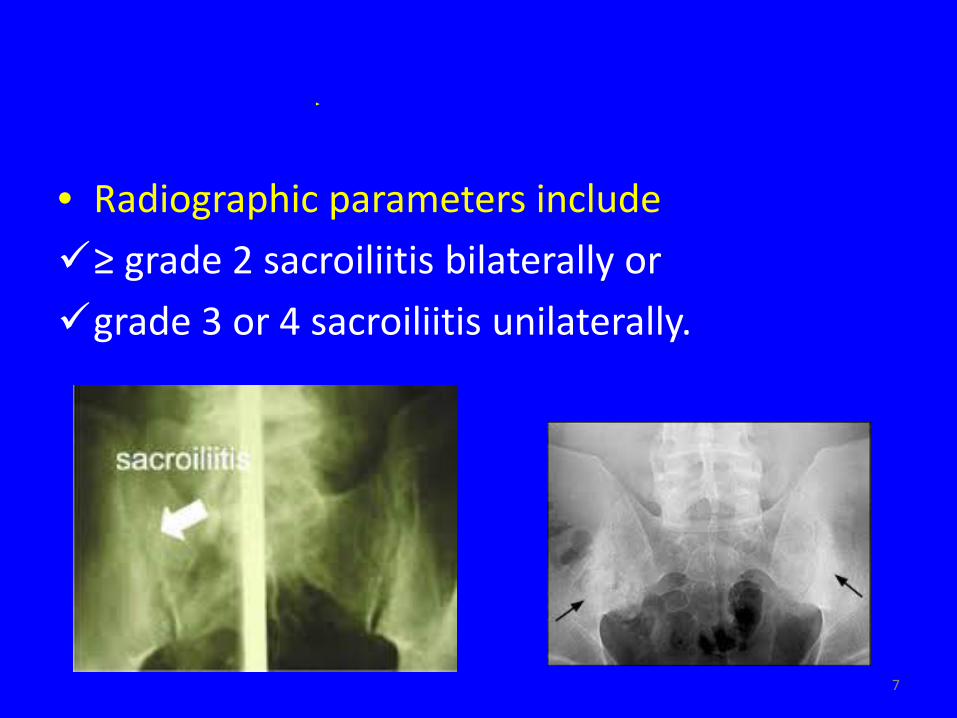
• Radiographic parameters include ≥ grade 2 sacroiliitis bilaterally or grade 3 or 4 sacroiliitis unilaterally.
7
Tpppppppp
• AS is a potentially severe disease with diverse manifestations, usually requiring multidisciplinary treatment coordinated by the rheumatologist.
• There is no cure for AS, although treatments and medications can reduce symptoms & pain.
8
Oppppppppp pp ppppppppp
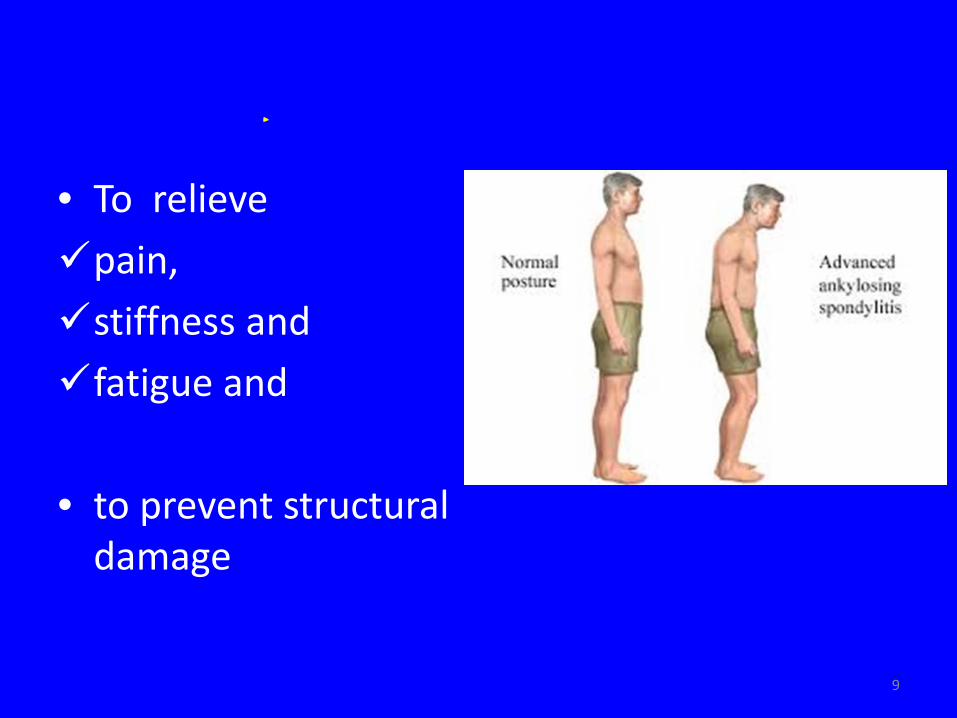
• To relieve pain, stiffness and fatigue and • to prevent structural
damage
9
Tpppppppp pppppppppp
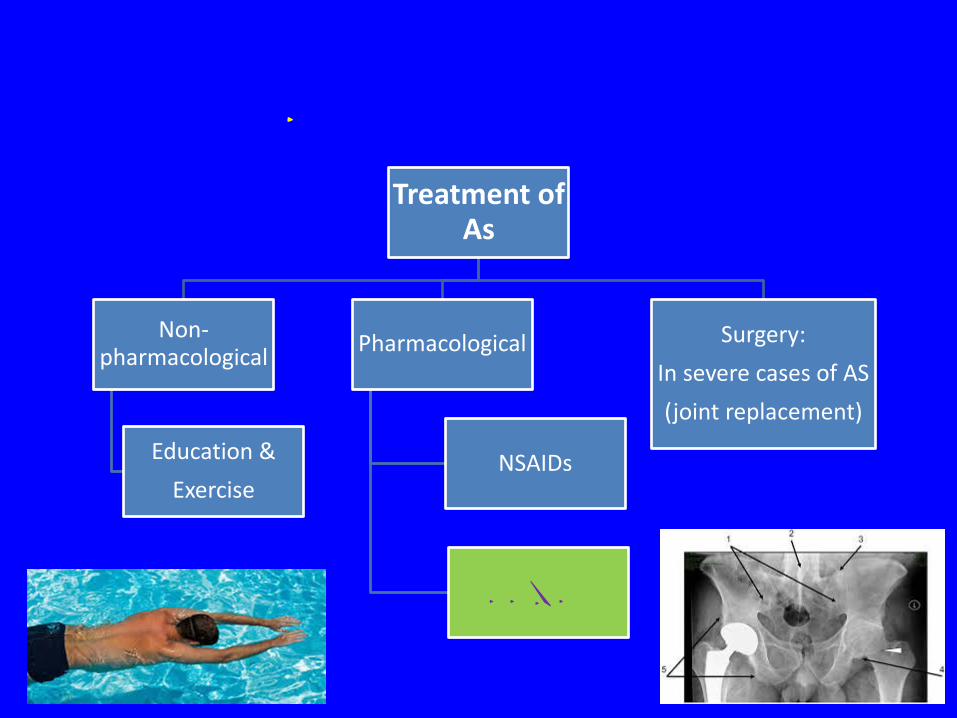
Treatment of As
Non-pharmacological
Education & Exercise
Pharmacological
NSAIDs
DMARDpp
Surgery: In severe cases of AS (joint replacement)
10
DMARDp pp Mppppppppp pp
Apppp AS
• Conventional synthetic DMARD (csDMARD) therapy in patients with axial spondyloarthritis (SpA) is a matter of continuous debate.
• Traditional DMARDs like Sulfasalazine or Methotrexate can be used in peripheral arthritis, but there is NO evidence for their efficacy for the treatment of axial AS.
11
However, newer biologic DMARDs TNF α blockers( Adalimumab, Certolizumab, Etanercept, Golimumab & Infliximab) have definite proven role in axial AS.
12
• British Society of Rheumatology (BSR) guidelines-‘Biologics for the treatment of axial spondyloarthritis(including AS) ‘ -Updated on August’ 2015
• The evidence for these guidelines is based on a systematic literature search of Medline,
EMBASE and the Cochrane library up to 30th June 2014.
13
Eppppppp ppp ppp ppppppppppppp pp ppppppppp pp
ppppp AS
18 eligible RCTs were identified which evaluated the efficacy of the 5 currently available TNF inhibitors (adalimumab, certolizumab, etanercept, golimumab and infliximab) in patients with AS.
14
Eppppppp ppp ppp ppppppppppppp pp ppppppppp pp
ppppp ASppppppp..
10 of the 16 placebo-controlled RCTs, all the used the ASAS20 response rates as primary efficacy outcome, with the time scale varying between 12-24 weeks.
15
Tpp ASAS20 pppppppp pppp ppppppppp
• Improvement in any 3 modalities by 20% or more without deterioration in the 4th modality-
1. Pain 2. Inflammation 3. Well-being 4. Function
16
Eppppppp ppp ppp ppppppppppppp pp ppppppppp pp
ppppp ASppppppppp
All of the placebo-controlled trials achieved the primary efficacy end-point.
17
Opppp pppppppp ppppp pp AS
No other biologic agents have demonstrated efficacy in AS or are licensed for this indication, so cannot be recommended for the treatment of AS.
18
Rppppppppppp ppp ppppp pppppppp pppp ppppp
TNF ppppp
• Evidence for anti-TNF therapy on radiographic disease progression (new bone formation and ankylosis) is currently limited. • Large, controlled, longer term clinical trials are
needed to clarify whether these drugs may be disease modifiers.
19

Treatment guideline
20
Whom to treat?
21
Epppppppppp ppp ppppppppp pppp TNFppppppppp
ppppp
1. The patient’s disease satisfies the modified New York criteria.
2. AS is active. Active disease is defined by a BASDAI and
spinal pain VAS ≥ 4 despite standard therapy. BASDAI should be measured on 2 occasions at
least 4 weeks apart (to avoid overtreatment of patients with a short-lived flare of disease)
22
Standard therapy is defined as 2 NSAIDs at maximal tolerated dose for at least 2 weeks each unless contraindicated.
23
Eppppppppp pppp ppppppppp
1. Women who are pregnant or breast-feeding. 2. Active significant infection. 3. Septic arthritis of a native joint within the last 12
months. 4. Sepsis of a prosthetic joint within the last 12
months or indefinitely if the joint remains in situ.
5. New York Heart Association (NYHA) grade 3 or 4 CCF for infliximab.
6. Clear history of demyelinating disease.
24
Which Anti TNF drug to choose?
25
Cppppp pp pppp
In the absence of head-to-head comparisons, systematic reviews have shown no statistical difference in efficacy between infliximab, golimumab, etanercept, or adalimumab in the treatment of AS.
26
Cppppp pp ppppppppppppp
Choice of drug should be a mutual decision between patient and clinician, taking into account factors such as- • Route, • frequency of administration, and • the presence of co-morbidities.
27
How to assess response?
28
Apppppppp pppppppp ppp pppppppppp ppppppppp
Initial efficacy response should be assessed following 3 to 6 months of therapy and responders should then be reassessed every 6 months.
29
Apppppppp pppppppp ppp pppppppppp
pppppppppppppppppp
Response is defined as reduction of BASDAI and spinal pain VAS by 2 or more units from baseline.
30
When to withdraw treatment?
31
Cppppppp ppp pppppppppp pp ppppppp
• Development of severe adverse effects (as for rheumatoid arthritis).
• In the absence of an initial clinical response by 6 months, or failure to maintain response at 2
consecutive assessments at least 4 weeks apart, withdrawal of that anti-TNF agent should be considered.
32
Wppppppppp pp pppppppppppppppp
• There is no evidence to support the
withdrawal of anti-TNF therapy in treatment responders.
33
Spppppppp ppppp
In the event of anti-TNF failure due to inefficacy or adverse event, an alternative anti-TNF agent should be offered if clinically appropriate.
34
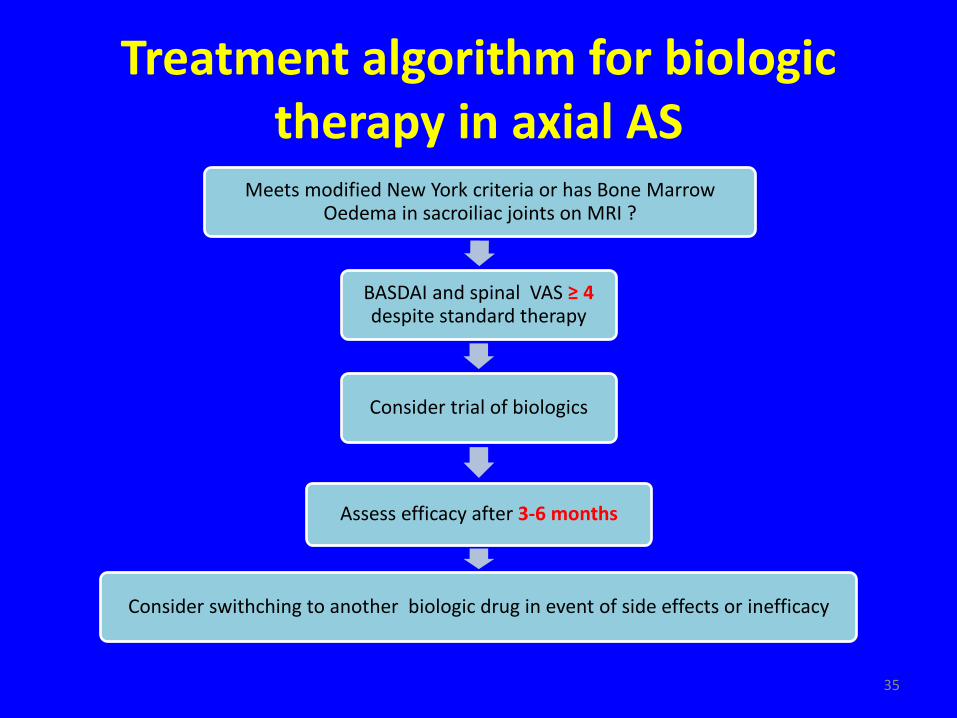
Treatment algorithm for biologic therapy in axial AS
Meets modified New York criteria or has Bone Marrow Oedema in sacroiliac joints on MRI ?
BASDAI and spinal VAS ≥ 4 despite standard therapy
Consider trial of biologics
Assess efficacy after 3-6 months
Consider swithching to another biologic drug in event of side effects or inefficacy
35

Sppppp
The safety of anti-TNF therapies in axial AS is comparable to other inflammatory joint diseases such as RA. There is little evidence to suggest that safety issues differ hugely with different disease groups
36
Lpppppppppp pp AppppTNF ppppppp
• High cost, • Parenteral route of administration • Side effects due to immunosuppression
37
Tppp Hppp Mppppppp
• Whether DMARDs are effective in axial AS is a
debatable issue.
• Traditional DMARDs like Sulfasalazine or Methotrexate can be used in peripheral arthritis, but there is NO evidence for their efficacy for the treatment of axial AS.
38
Tppp Hppp Mpppppppppppppppp
• Newer biologic DMARDs TNF α blockers have definite proven role in axial AS.
• According to BSR guidelines- ‘biologics for the treatment of axial spondyloarthritis (including AS): Anti TNF therapy is effective at reducing disease activity and spinal pain in axial AS.
39
Tppp Hppp Mpppppppppppppppp
• High cost, parenteral route of administration & side effects due to immunosuppression are the main limitations of using these agents.
• So it is the responsibility of the clinician to
assess risk benefit ratio before starting treatment with anti-TNF therapy for axial AS.
40

41
Tpppp Ypp