disorders of the outer and middle ear. disorders of the outer ear auricle/pinna - malformations may...
TRANSCRIPT
Disorders of the Outer and Middle ear

Disorders of the Outer ear
Auricle/Pinna - malformations may be congenital or due to surgery/accident
Does not result in any significant hearing loss Microtia Anotia
Cosmetic surgery - otoplasty or pinnaplasty.
Different Otoscopy images

Disorders of the External Auditory Meatus
Atresia - Lack of canalizationcan be congenital (Ex., Treacher
Collins syndrome) or be due to trauma
Stenosis - Narrowing of the canal
Collapsing External Auditory Canals - seen usually in elderly clients when you place head phones for testing - Caution!

Disorders of the External Auditory Meatus Foreign bodies in the
canal. All of the above
conditions may result in a __________ hearing loss
Maggots in the ear canal!!!

Disorders of the External Auditory Meatus
External Otitis - an infection that occurs in the skin of
the external auditory Meatus If fungal - Otomycosis
Usually caused by overuse of ear drops.
Furunculosis - infection of hair follicles (very painful!).
External otitis of any kind may lead to inflammation of the tympanic membrane
Myringitis
Swimmers ears
Disorders of the External Auditory Meatus
May result in a conductive hearing loss although it is hard to test these patients due to tenderness of the auricle.
Treated with systematic antibiotics and irrigating the ear canal regularly.
Growths in the Ext. Ear includes tumors (benign or malignant) & bony
growths. Ear wax/Cerumen
Treat with cerumenolytic to soften the wax.

Disorders of the External Auditory Meatus Perforations of the
tympanic membrane Could be due to trauma
- usually recovery is good
Middle ear infection - TM usually recovers once the primary infection is treated.
Surgical repair of TM - Myringoplasty Earlier muscle fascia
was used to graft the TM
Disorders of the Middle ear
A) Otitis Media - Any infection of the mucous-membrane lining of the middle ear cleft.Seen in 70% of children before 2 yrs of agePredisposing factors:
Poorly functioning Eustachian tubes Barotrauma (ex., sky diving) Abnormal action of the cilia of the mucous
membranes.

Disorders of the Middle ear
Anatomical deformities of the middle ear Decreased immune functioning (ex, AIDS) Cigarette smoke or other fumes
Infection usually starts at opening of Eustachian tube in nasopharynx.Spreads up the tube. Tube becomes
swollen and shut. Infection spreads to middle ear space.
Results in negative pressure in middle ear which can be recorded in a tympanogram.
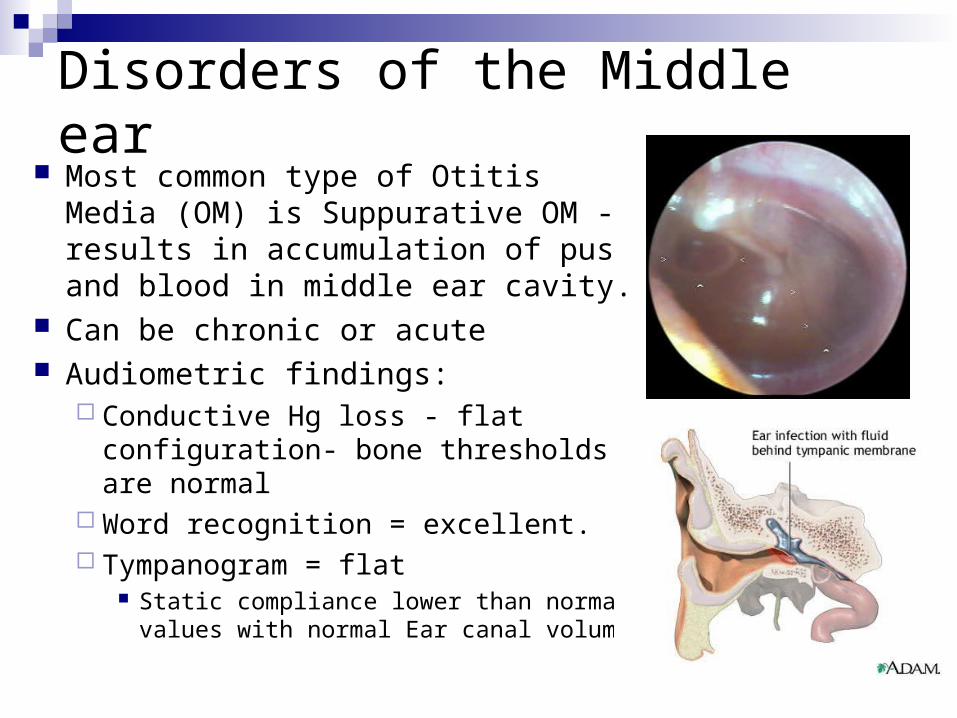
Disorders of the Middle ear Most common type of Otitis Media
(OM) is Suppurative OM - results in accumulation of pus and blood in middle ear cavity.
Can be chronic or acute Audiometric findings:
Conductive Hg loss - flat configuration- bone thresholds are normal
Word recognition = excellent. Tympanogram = flat
Static compliance lower than normal values with normal Ear canal volume
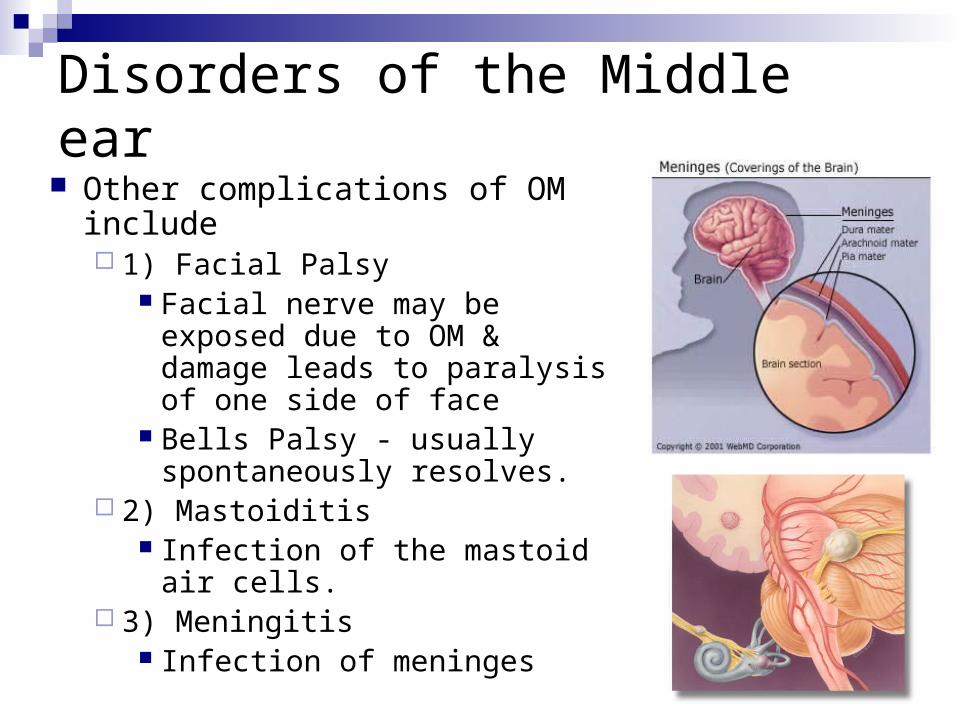
Disorders of the Middle ear Other complications of OM include
1) Facial Palsy Facial nerve may be exposed
due to OM & damage leads to paralysis of one side of face
Bells Palsy - usually spontaneously resolves.
2) Mastoiditis Infection of the mastoid air
cells. 3) Meningitis
Infection of meninges
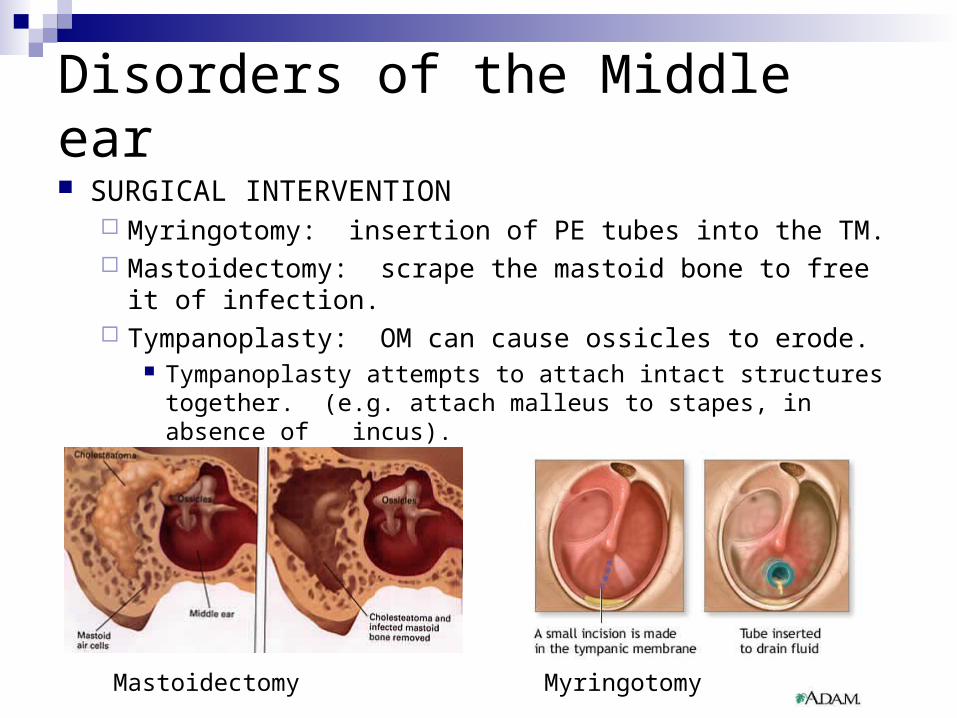
Disorders of the Middle ear SURGICAL INTERVENTION
Myringotomy: insertion of PE tubes into the TM. Mastoidectomy: scrape the mastoid bone to free it of
infection. Tympanoplasty: OM can cause ossicles to erode.
Tympanoplasty attempts to attach intact structures together. (e.g. attach malleus to stapes, in absence of incus).
Mastoidectomy Myringotomy
Disorders of the Middle ear
B) Eustachian tube dysfunctionPatulous Eustachian Tube - chronically open
Eustachian tube Results in autophony - “head in the barrel” May not be identified in normal tympanometry - if
suspected, perform tympanometry when the client is oral/ nasal breathing - you can notice the change in middle pressure for every breathing cycle.

Disorders of the Middle ear C) OTOSCLEROSIS
70% of cases = hereditary. Origin = bony labyrinth of inner ear. Usually not
recognized clinically until it effects the middle ear.
Progressive in nature. Varying age of onset in mid-childhood to late middle adulthood.
Most common in white women (more during pregnancy or menopause).

Disorders of the Middle ear
Growth of spongy bone. Growths occur throughout middle ear, but often are on stapes footplate, which immobilizes it, causing a conductive hearing loss.
As disease progresses, might develop to a mixed hg loss.
Audiometric : Low frequency air bone gap. slightly reduced bone
scores, with a notch at 2000 Hz because of immobility of stapes in the oval window -Carharts notch.
Tympanogram - reduced Static Admittance.

Disorders of the Middle ear
Treatment: Surgical Stapedectomy: removal of the stapes.
Replacement with a prosthetic device. If progressed and leads to a SN hearing loss,
hearing aids may be an option.

Disorders of the Middle ear
Other disorders include - Tumors, disarticulation of ossicles, cancer, trauma.
Disorders of the Inner Ear
Introduction
Constitutes the majority of hearing losses. Mostly due to pathology at the level of the hair
cells. Abnormalities of the cochlea, unlike a
conductive pathology, not only results in a reduced hearing sensitivity but may also result in difficulty understanding speech.

Causes of Inner Ear Disorders
Can be of endogenous (internal factors) or exogenous (external factors) in origin.
Prenatal causesHereditary causes - may be seen isolated or
along with other abnormalities (syndromes)Environmental causes - trauma, viral
infections such as rubella, AIDS and CMV (especially the first trimester)
Causes of Inner Ear Disorders
Perinatal CausesAnoxiaPremature birth (<3.5 pounds) is often
associated with different kinds of abnormalities
Trauma during forced delivery or ‘forceps’ delivery

Causes of Inner Ear Disorders
Postnatal causesComplications of otitis media MeningitisViral infections such as measles, mumps,
chicken pox etcBacterial infections such as syphilis (may
be prenatal or acquired) Infections of the labyrinth - Labyrinthitis
May involve both cochlear & vestibular organs.
Causes of Inner Ear Disorders
Toxic causes Ototoxicity Prolonged use of drugs, especially
antibiotics.May be cochleotoxic (such as kanamycin,
neomycin, viomycin) or vestibulotoxic (streptomycin, gentamycin).
Should be avoided but if absolutely necessary, dosage should be monitored with follow-up audiometry.

Causes of Inner Ear Disorders
Usually the hearing loss starts at the high frequencies.
ASHA (1994) published guidelines for monitoring patients who receive ototoxic drugs Timely identification of at-risk patients. Pretreatment counseling & baseline
audiometric measures. Periodic evaluations to document progression
of hearing loss.

Causes of Inner Ear Disorders
Otosclerosis Progression of the disease may affect the oval
or round window. May be following surgery! (Iatrogenic nature)
Barotrauma Severe, sudden changes in middle ear
pressure may cause a rupture of the round or a tearing of the annulus of the oval window.
Results in a fistula & drainage of the inner ear fluids.
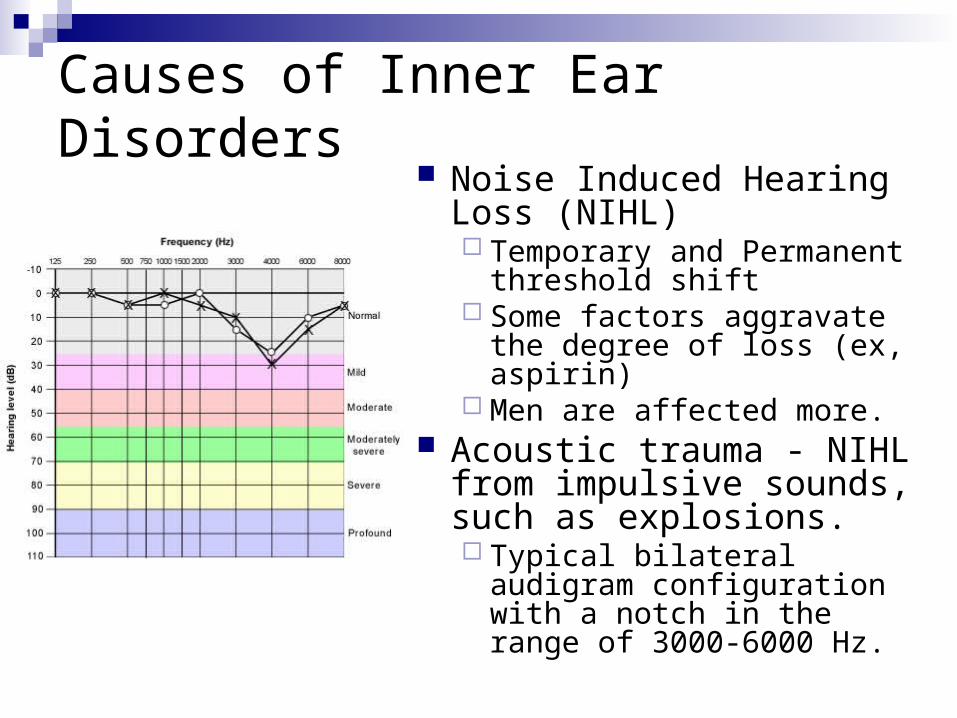
Causes of Inner Ear Disorders Noise Induced Hearing Loss
(NIHL) Temporary and Permanent
threshold shift Some factors aggravate the
degree of loss (ex, aspirin) Men are affected more.
Acoustic trauma - NIHL from impulsive sounds, such as explosions. Typical bilateral audigram
configuration with a notch in the range of 3000-6000 Hz.

Hair cell loss seen in NIHL
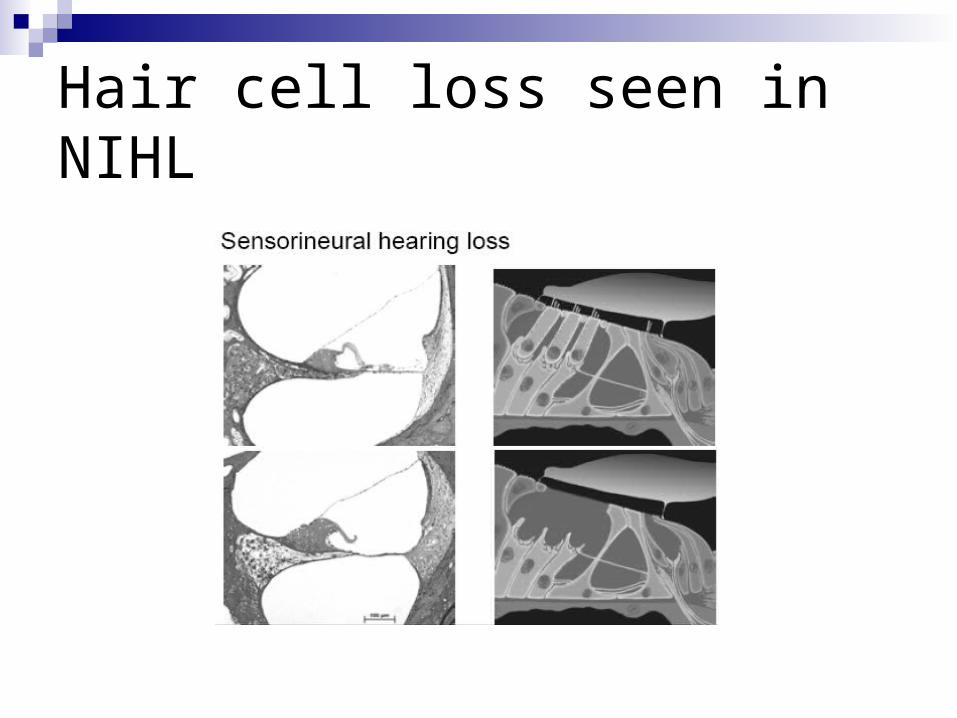
Hair cell loss seen in NIHL
NIHL Occupation noise is a major cause for NIHL Occupational Safety and Health (OSHA) (1983)
has recommended a scale on which the time that worker may be safely exposed to intense sounds is decreased as the intensity of the noise is increased.
Damage risk criteria 85 dBA: 8 hrs 90 dBA: 4 hrs & every five dB increase, half the
permitted time. 105 dBA: 30 mins

NIHL The actual amount of hearing loss due to noise
exposure depends on other factors such as genetics, disease, aging, life style off work etc.
One of the initial symptoms of NIHL (& in fact of many cochlear pathologies) is tinnitus.
Noise has also been shown to other adverse affects such as increased anxiety levels, loss of ability to concentrate, and loss of sleep.

Sudden Idiopathic Sensori-neural hearing loss Refers to a hg loss, usually unilateral, that
may develop over the course of a few days or occur seemingly instantaneously.
The etiology may be either viral or vascular (vasospasm).
A viral origin is suspected if recent respiratory infections were present.
If treated immediately, may be reversible.
Méniére Disease
Another cause of sudden unilateral hg loss. Characterized by sudden attacks of vertigo,
tinnitus, vomiting, and unilateral hearing loss. Onset of symtoms is usually a description of
fullness in one ear, followed by a low frequency roaring tinnitus, difficulty in speech recognition, violent spells of vertigo with vomiting.
The hearing loss is usually fluctuating and progressive in nature.

Méniére Disease Is believed to be caused due to endolymphatic
hydropsThe over secretion or under absorption of
endolymph. Anxiety and allergic factors have been
considered as causes. Is more often seen in males and rarely affects
children. Méniére disease may be extremely
handicapping because of the paroxysmal attacks of vertigo.

Méniére Disease
Normal membranous labyrinth
Dilated membranous labyrinthin Meniere's disease

Méniére Disease
Treatment - limit fluid retention through diuretic drugs and the decrease in sodium intake in the diet.
Surgical approaches often aim at decompressing the endolymphatic sac or draining the excessive endolymph by inserting a shunt into the skull to relieve the pressure.
In extreme cases, the entire labyrinth may be surgically destroyed or auditory nerve sectioned to alleviate the vertigo and tinnitus.

Head Trauma
Due to head injury - The audiogram is quite similar to those due to acoustic trauma with notch in the 3000-6000 Hz range.
Depending upon the magnitude of the injury, the tympanic membrane, middle ear structures, inner ear structures may be affected by varied extents.
The resulting loss may be severe to profound.

Presbycusis Hg loss due to advancing age. The lesions are not restricted to only the
cochlea but produces alteration in nearly all the auditory structures.
Usually begins at the early 60’s for males and late 60’s for females.
It is even believed that the hearing mechanism starts slowly deteriorating from birth!
App 25% in the age range 45-64yrs & 40% above 65 have some degree of hg loss.

Presbycusis

Presbycusis Common audiological symptom - difficulty in
speech recognition. Performance improves with reduced rate of
speech. Management - Hearing aids.