discharge follow-up appointment webinar slide deck
DESCRIPTION
Discharge Follow-Up Appointment Webinar PresentationTRANSCRIPT

Discharge Follow-Up Appointment Challenge
Webinar Presentation
Wednesday, March 7th

On today’s call:
Wil Yu
Special Assistant of Innovations and Research
ONC
JL Neptune
Senior Vice President
Health 2.0
Janhavi Kirtane
Director of Clinical
Transformation
ONC
Amy Berman
Senior Program Officer
John A. Hartford
Foundation
Marybeth Sharpe
Program Director
Gordon and Betty Moore Foundation
Agenda for Today’s Meeting
ONC and the Investing in Innovation (i2) Program
An Introduction to Care Transitions
An Overview of the Discharge Follow-Up Appointment Challenge
Q&A About the Challenge
ONC and i2

5
i2 – Investing in Innovations
Adam Wong
Office of the National Coordinator

6
i2 Goals
• Better Health, Better Care, Better Value through Quality Improvement– Further the mission of the Department of Health and Human Services
– Highlight programs, activities, and issues of concern
• Spur Innovation and Highlight Excellence – Motivate, inspire, and lead
• Community building – Development of ecosystem
• Stimulate private sector investment
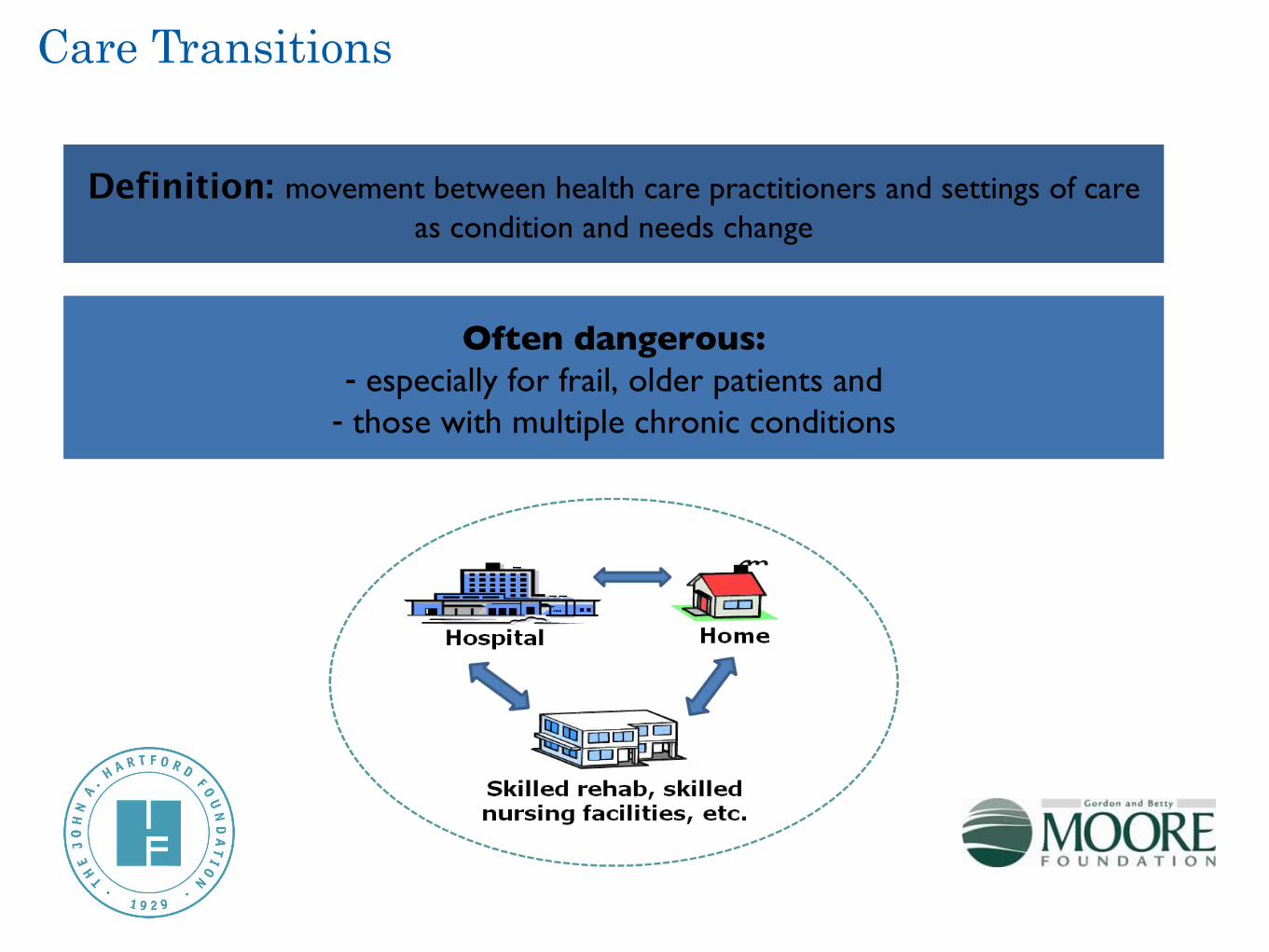
Care Transitions
Definition: movement between health care practitioners and settings of care as condition and needs change
Often dangerous:- especially for frail, older patients and
- those with multiple chronic conditions
Care Transitions: Key Opportunity
Hospital readmissions frequent, and…─ 19.6% of Medicare patients (65 years and older) readmitted to
the hospital within 30 days of discharge; 34% within 90 days
Costly, but…─ At least $17B in Medicare spending; estimated $25B across
all insurance companies annually
Avoidable– Variation between hospitals
– Heart Failure, Pneumonia, Coronary Obstructive Pulmonary Disease, Heart Attack leading conditions
– Proven interventions

Some Elements of a High-Quality Transition• Patient and family education on diagnosis and care during
hospital stay.
• Schedule post-discharge appointments.
• Organize post-discharge services.
• Reconcile medications and confirm medication plan.
• Expedite discharge summary to outpatient providers.
• Teach-back with patients and family.
• Discharge plan to patient.
• Confirmed hand-off to outpatient physicians and others.
• (Telephone call 2-3 days after discharge)

Impact on Patients
Problems– Primary care provider may not know individual has been discharged
– Individual may not have primary care provider– May not set appointment in right time frame
– Even with appointment set, problem may arise– ex. Mary and her medications
The Critical Transitions Challenge Issue– 50% of readmitted patients haven’t had primary care f/u

Impact on Patients
The Challenge:“Create an easy-to-use web-based tool that
will make post-discharge follow-up appointment scheduling a more effective and shared process for care providers, patients
and caregivers.”
•In addition, developers will need to articulate a plan for broader adoption at the community level.
•Submissions can be existing applications, or applications developed specifically for this challenge.
•The technology developed will remain proprietary to the developer and will not become open source.
Part 1: Tool Development
The Ideal application for will include the following components:
4. Easy to navigate user interface
5. Easy to navigate process for downstream accepting providers
6. Information for patient and caregiver convenience and preference
7. Critical background information for downstream provider
8. Messaging capabilities to minimize no-shows and cancellations
9. EHR interface capabilities where applicable
Part 2: Plan for scale and adoption
To assist with pilot plan development, applicants are advised to consider the following examples as potential audiences for the challenge:
•Hospital(s) with a selection of owned or affiliated physician practices•Community collaboratives or payment pilots focused on care transitions improvement, which could include hospitals, physician practices, community-based organizations, skilled nursing homes, etc•Local payers focused on improving transitions at the community level.•Partnership for Patients Hospital Engagement Networks
Part 2: Plan for scale and adoption
To anticipate the needs of a test bed organization or community, successful applicants will also need to submit a brief pilot implementation proposal (250-500 words) that addresses factors including
•timeline, description of pilot environment needs (e.g., types of technical capabilities, •types and number of patients and providers included), and •additional resource needs (e.g., staffing and technical resources).
Judging Criteria
1. Effectively integrate inpatient data and provide structured support for self-care
2. Integrate design and usability concepts to drive patient and provider adoption and engagement
3. Demonstrate creative and innovative uses of mobile technologies
4. Demonstrate potential to improve health status for individuals and the community
5. Leverage NwHIN standards including transport, content, and vocabularies
6. Demonstrate ability to implement the intervention in a pilot setting, and ultimately to scale in a community

Timeline
Submission Period Ends4-30-12
Winner Notified05-23-12