diagnosis and treatment of idiopathic thrombocytopenic purpura€¦ · international journal of...
TRANSCRIPT

international journal of athletic therapy & training march 2012 25
© 2012 Human Kinetics - IJATT 17(2), pp. 25-28
Idiopathic thrombocytopenic purpura (ITP) is a syndrome characterized by a low plate-let count in the peripheral blood that is not related to marrow failure.1 ITP is a relatively common syndrome of unknown origin that is increasingly recognized. Approxi-
mately 66 adults and 50 children per 1,000,000 are diagnosed with ITP annually.2 The popula-tion of athletes with ITP, however, is not cur-rently reported in the literature. The ability to recognize its signs and symptoms and referral for further evaluation is critical for the treatment of patients who are oth-erwise healthy.
Childhood and adult onset of ITB have iden-tical clinical presenta-tions, and treatment is the same but the prog-nosis differs. The major-ity of cases in children
are diagnosed between two and nine years of age, whereas adult-onset ITB can be mani-fested between 20 and 50 years of age. Adult ITP (ITP-A) has a slower onset, no prodromal illness, and appears to be idiopathic.3 Child-
Joe J. Piccininni, EdD, CAT(C), Report Editor
Diagnosis and Treatment of Idiopathic Thrombocytopenic Purpura
CLINICAL EVALUATION & TESTING
Leamor Kahanov, EdD, LAT, ATC; Lindsey E. Eberman, PhD, LAT, ACT; and Shaun Grammer, MSPA, PA-C • Indiana State University
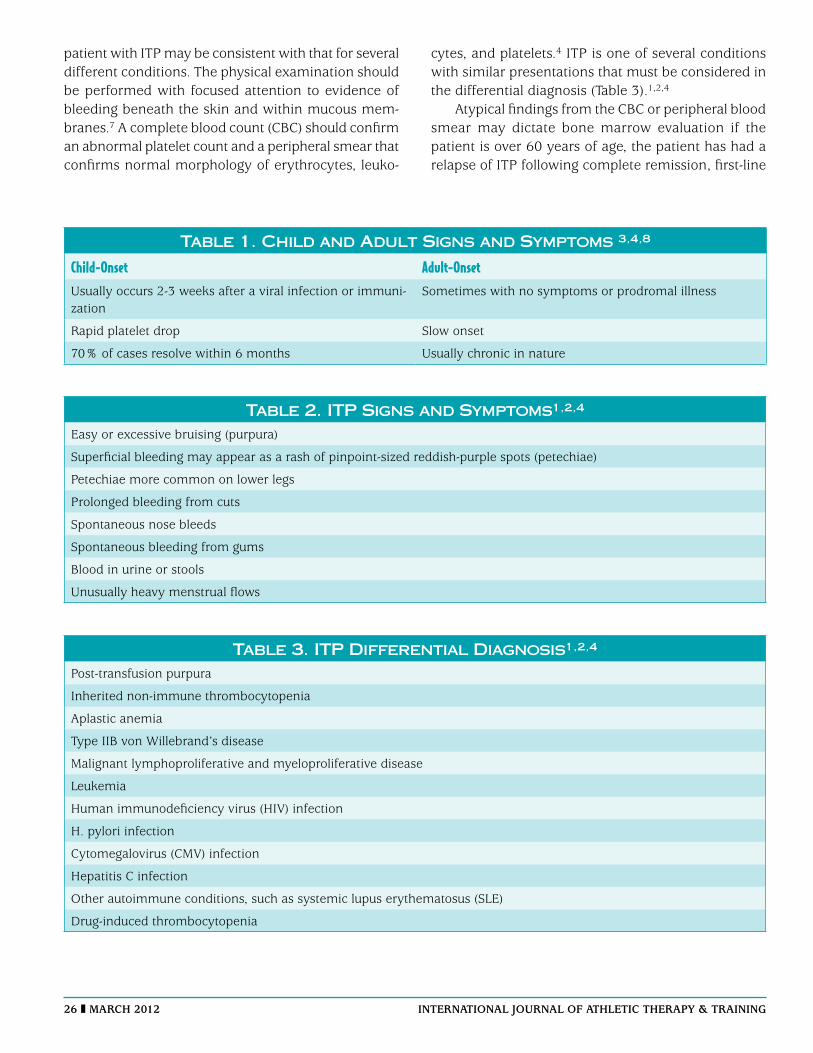
hood ITP (ITP-C) is characterized by a rapid drop in platelet count, with sudden onset of petechiae or purpura (i.e., areas of skin dis-coloration).3 Over 70% of ITP-C cases resolve within 6 months,4 but the ITP-A is a chronic disease that is associated with intermittent remission (Table 1).
Diagnosis of ITP-A and ITP-C are distinct, but an individual in his or her early 20s may exhibit characteristics of both conditions.5 ITP is characterized by antibody response to proteins on platelets that leads to their destruction and diminished platelet produc-tion.6 Signs and symptoms associated with ITP-C and ITP-A vary on the basis of platelet count. Signs may include petechiae, purpura, and ecchymosis of the skin (Table 2). Pete-chiae and purpura are non-palpable and non-blanching. Bleeding may occur within the mucous membranes of the gastrointestinal tract, mouth, nose, and eyes.4 Platelet level is considered normal when it is between 150 to 400 K/mL;1 however, platelet count can be variable over time, and symptoms can develop intermittently (Table 2).1
Diagnosis of ITP is based on exclusion of symptoms associated with other similar conditions. A lack of published evidence con-cerning diagnostic accuracy for a specific set of physical examination findings and labora-tory test results necessitates diagnosis on the basis of clinical expertise. The history of a
Childhood-onset ITP may occur in young adults.
Diagnostic signs of ITP include the presen-tation of purpura, petechiae, and prolonged bleeding.
The criteria for consideration of splenec-tomy include severe thrombocytopenia (< 10 K/mL), a high risk for bleeding (< 30 K/mL), or continuous treatment with corticosteroids necessary to maintain platelet count.
Because remission may occur spontane-ously within 6 months, early splenectomy may not be warranted.
Key PointsKey Points
26 march 2012 international journal of athletic therapy & training
patient with ITP may be consistent with that for several different conditions. The physical examination should be performed with focused attention to evidence of bleeding beneath the skin and within mucous mem-branes.7 A complete blood count (CBC) should confirm an abnormal platelet count and a peripheral smear that confirms normal morphology of erythrocytes, leuko-
cytes, and platelets.4 ITP is one of several conditions with similar presentations that must be considered in the differential diagnosis (Table 3).1,2,4
Atypical findings from the CBC or peripheral blood smear may dictate bone marrow evaluation if the patient is over 60 years of age, the patient has had a relapse of ITP following complete remission, first-line
Table 1. Child and Adult Signs and Symptoms 3,4,8
Child-Onset Adult-OnsetUsually occurs 2-3 weeks after a viral infection or immuni-zation
Sometimes with no symptoms or prodromal illness
Rapid platelet drop Slow onset
70% of cases resolve within 6 months Usually chronic in nature
Table 2. ITP Signs and Symptoms1,2,4
Easy or excessive bruising (purpura)
Superficial bleeding may appear as a rash of pinpoint-sized reddish-purple spots (petechiae)
Petechiae more common on lower legs
Prolonged bleeding from cuts
Spontaneous nose bleeds
Spontaneous bleeding from gums
Blood in urine or stools
Unusually heavy menstrual flows
Table 3. ITP Differential Diagnosis1,2,4
Post-transfusion purpura
Inherited non-immune thrombocytopenia
Aplastic anemia
Type IIB von Willebrand’s disease
Malignant lymphoproliferative and myeloproliferative disease
Leukemia
Human immunodeficiency virus (HIV) infection
H. pylori infection
Cytomegalovirus (CMV) infection
Hepatitis C infection
Other autoimmune conditions, such as systemic lupus erythematosus (SLE)
Drug-induced thrombocytopenia

international journal of athletic therapy & training march 2012 27
ITP therapies have failed, or a splenectomy is under consideration. Other laboratory analyses that may be performed in the process of diagnosing ITP may include an Immunofluorescence test (PIFT), thrombo-poietin (TPO) assay, measurement of platelet RNA by flow cytometry, fluorescent antinuclear antibody test-ing, and serological assays to detect H. pylori; however, these tests are not currently recommended for routine diagnosis of ITP.4
TreatmentThe clinical expertise necessary for proper diagnosis of ITP is also crucial for determination of appropriate treatment, because most options have not yet been supported by research evidence. Symptomatic patients, or patients at risk for bleeding (e.g., contact sport ath-letes), should begin a regime of immunosuppressant medications. To determine risk for bleeding, clinicians should consider age, cormorbidities, and platelet count. A patient with a count greater than 20 K/mL, but who is not symptomatic, should be monitored but should not receive treatment.2
Corticosteroids, such as prednisone or prenisolone at 1 to 2mg/kg per day, are typically prescribed fol-lowing diagnosis of ITP. Almost two-thirds of patients respond favorably to corticosteroids within the first week, which is manifested by clearance of platelets, decreased autoantibody production, and improved cap-illary integrity. Unfortunately, only 10 to 15% exhibit a lasting remission.2 The literature suggests that ITP-A is more likely to resolve permanently in response to early intensive immunosuppressive therapy.
If a patient exhibits bleeding or a platelet level less than 10 K/mL, intravenous immunoglobulin treatment (IVIG) may be effective. IVIG reduces reticuloendothe-lial clearance but also has other immunomodulatory effects: inhibition of complement binding to platelets, interference of immune complex binding to plate-lets, immune activity of anti-idiotype antibodies, and impaired release of pro-inflammatory cytokines from monocytes.2 As a result of the treatment, about 80% of patients exhibit a platelet count above 50 K/mL as quickly as one day after treatment, which peaks at one week, and the response may only last up to 3 to 4 weeks.2
Another treatment option to increase platelet count is anti-D immunoglobulin. Patients must be Rh-positive
and must not have undergone splenectomy for this treatment to be appropriate and effective. Approxi-mately 70% of patients respond positively, with an increased platelet count within 24 to 72 hours and lasting effects for up to 21 days. Anti-D treatment is less costly and has a shorter infusion duration com-pared to IVIG.2
If all conservative treatments have failed, splenec-tomy may be indicated. Indications include severe thrombocytopenia (< 10 K/mL), a high risk for bleed-ing (< 30 K/mL), or continuous treatment with cor-ticosteroids to maintain platelet count.2 Splenectomy may be recommended on the basis of a clinician’s treatment philosophy; however, after 3 months of failed drug treatments and the exhaustion of all nonsurgi-cal options, splenectomy may be the only treatment option that is left.3 In the physically active and athletic populations, splenectomy is not always excluded as a treatment option. The literature indicates that Nplate® and Promacta® are effective new therapies that are tol-erable and not overly toxic.3 Future treatment planning may need to be modified to include new drug therapies. Guidelines for return to sport participation do not cur-rently exist, because management guidelines for the general population have not been clearly established.8,9 Current guidelines suggest that an ITP patient who has been in remission for 4-6 weeks should have a platelet count greater than 300 k/ml.9 The decision to allow an athlete to return to participation should be based on a sustained platelet count greater than 30,000 without bleeding and consideration of the nature of the sport activity.
ConclusionDifferences between ITP-A and ITP-C can complicate the diagnosis of ITP in young adults.5 Conservative treatments, particularly corticosteroids, IVIG, and anti-D treatments are available, but they have limita-tions. Splenectomy should not be considered unless conservative treatments have been ineffective for over three months. Approximately two-thirds of ITP-C cases will improve spontaneously in six months.7 Research evidence should guide the process of establishing a diagnosis, but clinical expertise is often necessary to diagnose ITP. Clinicians should consider conservative treatment options prior to recommending surgical intervention.

28 march 2012 international journal of athletic therapy & training
References 1. British Committee for Standards in Hematology General Haematol-
ogy Task Force. Guidelines for the investigation and management of idiopathic thrombocytopenic purpura in adults, children, and in pregnancy. Br J Haematol. 2003;120(4):574-596.
2. Stasi R, Evangelista ML, Stipa E, Buccisano F, Vendetti A, Amadori S. Idiopathic thrombocytopenic purpura: current concepts in patho-physiology and management. Thromb Haemost. 2008;99(1)4-13.
3. Schoonen WM, Kucera G, Coalson J, Li L, Rutstein M, Mowat F, et al. Epidemiology of immune thrombocytopenic purpura in the General Practice Research Database. Br J Haematol. 2009;145(2):235-244.
4. Grammer S, Kahanov L. Immune (idiopathic) thrombocytopenic pur-pura in a 21-year-old student. J Am Acad Physician Asst. 2011;24(9):E1-3.
5. Berchtold P, McMillan R. Therapy of chronic idiopathic thrombocyto-penic purpura in adults. Blood. 1989;74(7):2309-2317.
6. Provan D. Characteristics of immune thrombocytopenic purpura: a guide for clinical practice. Eur J Haematol. 2009;82(suppl 71):8-12.
7. Cheng Y, Wong RSM, Soo YOY, Chui CH, Lau FY, Chan NPH, et al. Initial treatment of immune thrombocytopenic purpura with high-dose dexamethasone. N Engl J Med. 2003;349(9):831-836.
8. Provan D, Stasi R, Newland AC, Blanchette VS, Bolton-Maggs P, Bussel JB, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010;115(2):168-186.
9. Geroge JN, Woolf SH, Raskob GE, Wasser JS, Aledort LM, et al. Idio-pathic thrombocytopenic purpura: a guideline developed by explicit methods for The American Society of Hematology. Blood.1996(1):3-40.
Leamor Kahanov is the Chair of the Department of Applied Medicine and Rehabilitation at Indiana State University in Terre Haute.
Lindsey E. Eberman is an assistant professor and the Undergraduate ATEP Program Director in the Department of Applied Medicine and Rehabilitation at Indiana State University.
Shaun Grammer is an assistant professor with the Physician Assistant Studies Program in the Department of Applied Medicine and Rehabili-tation at Indiana State University.
A single source for research in all the sport and exercise sciences
Kinesiology Review (KR) provides a forum for discussion and analysis of kinesiology research and its applications.
Although many journals publish reviews on select topics, KR stands alone in its focus on scholarly reviews from any
and all of the kinesiology subdisciplines. This rigorously reviewed online quarterly journal will serve the interests of
those in all areas of study related to health and physical activity, including exercise science, sport management,
sport and exercise psychology, sports medicine, physical education pedagogy, fitness instruction, and physical and
occupational therapy.
The review articles found in KR address important issues and emerging research in all areas of the sport and exercise
sciences. KR also publishes theoretical papers, critical analyses of significant issues and scientific methods, and
position papers pertinent to kinesiology. One issue each year will contain the annual papers of the National Academy
of Kinesiology, which provide commentary on timely issues in the field. Kinesiology Review is the official journal of the
National Academy of Kinesiology and the American Kinesiology Association.
HUMAN KINETICSThe Information Leader in Physical Activity & Health1219 11/11
Kinesiology ReviewJane E. Clark, PhD, EditorFrequency: Quarterly (February, May, August, November)Current volume: 1 (2012)Online format ISBN: 978-1-4504-2388-5
For more information or to order, visit www.KR-Journal.com or call: (800) 747-4457 US • (800) 465-7301 CDN • 44 (0) 113-255-5665 UK
(08) 8372-0999 AUS • 0800 222 062 NZ • (217) 351-5076 International
Call for papersWe are now welcoming submissions to Kinesiology Review. For more information on submitting an article to KR, visit www.KR-Journal.com
Available February 2012