diagnosing lung cancer earlier - london cancer · •incidence of lung cancer in the three years...
TRANSCRIPT
Diagnosing Lung Cancer Earlier
Sam Janes London Lung Cancer Pathway Director
Consultant Respiratory Physician Wellcome Senior Fellow
University College Hospital, London
What cancer is the biggest killer of men in the UK?
a. Bowel and prostate cancer
b. Lung cancer
What cancer is the biggest killer of men in the UK?
a. Bowel and prostate cancer ✗
b. Lung cancer ✔
What cancer is the biggest killer of women in the UK?
a. Breast cancer
b. Lung cancer
What cancer is the biggest killer of women in the UK?
a. Breast cancer ✗
b. Lung cancer ✔
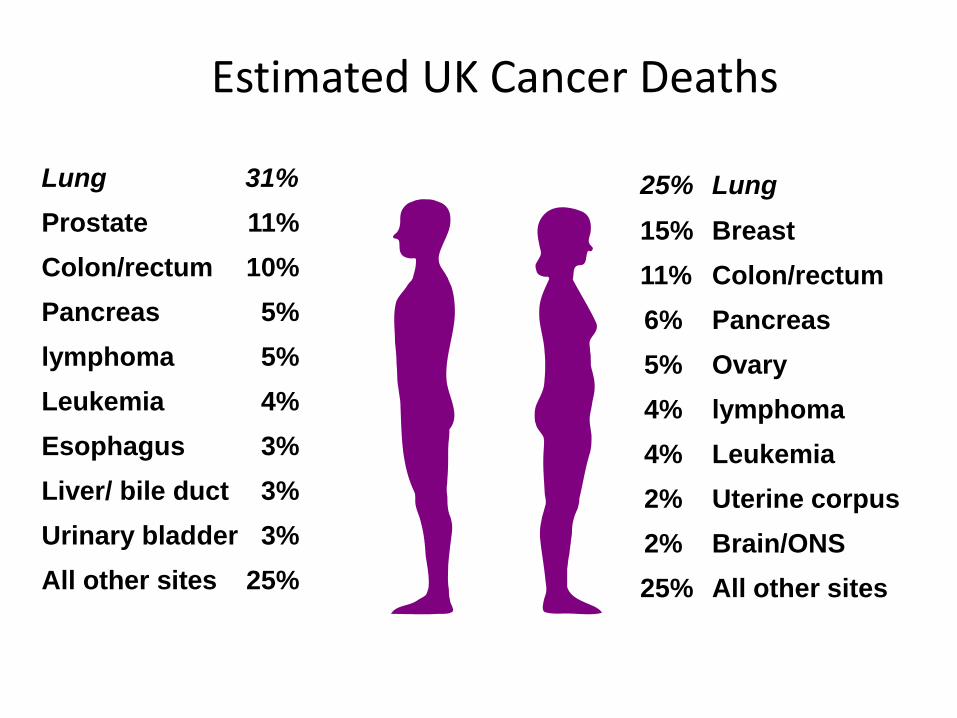
Estimated UK Cancer Deaths Men
Women
25% Lung
15% Breast
11% Colon/rectum
6% Pancreas
5% Ovary
4% lymphoma
4% Leukemia
2% Uterine corpus
2% Brain/ONS
25% All other sites
Lung 31%
Prostate 11%
Colon/rectum 10%
Pancreas 5%
lymphoma 5%
Leukemia 4%
Esophagus 3%
Liver/ bile duct 3%
Urinary bladder 3%
All other sites 25%
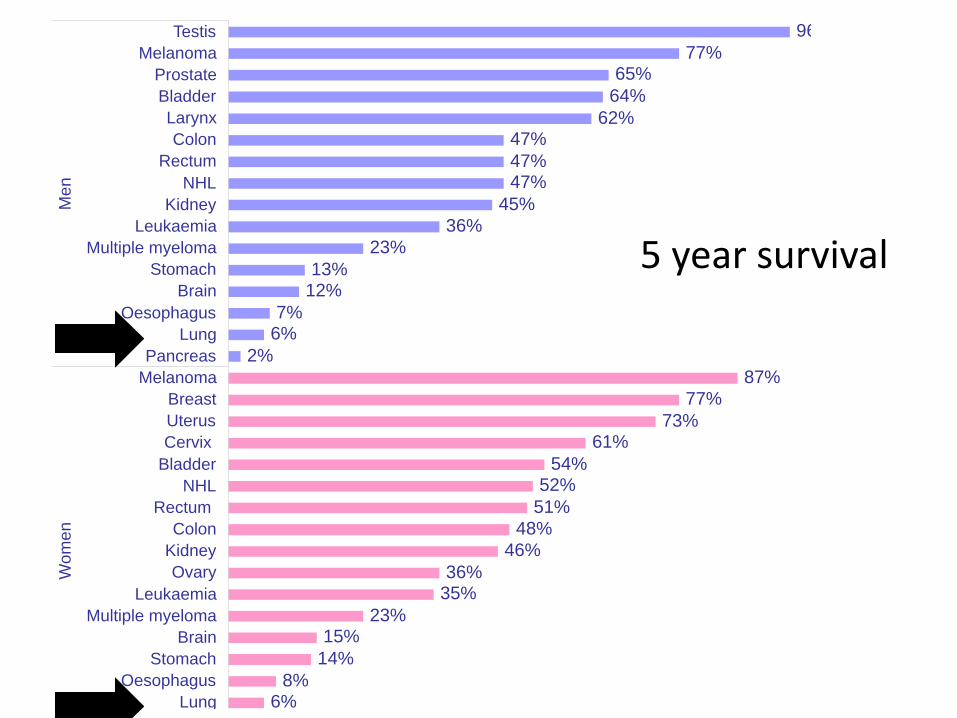
How many people that have had lung cancer are alive 5 years later?
a. 50%
b. 5%
How many people that have had lung cancer are alive 5 years later?
a. 50% ✗
b. 5% ✔
2%
6%8%
14%
15%23%
35%36%
46%
48%
51%
52%54%
61%73%
77%
87%
2%
6%7%
12%13%
23%
36%
45%
47%47%
47%62%
64%
65%77%
96%
Pancreas
Lung
Oesophagus
Stomach
Brain
Multiple myeloma
Leukaemia
Ovary
Kidney
Colon
Rectum
NHL
Bladder
Cervix
Uterus
Breast
Melanoma
Pancreas
Lung
Oesophagus
Brain
Stomach
Multiple myeloma
Leukaemia
Kidney
NHL
Rectum
Colon
Larynx
Bladder
Prostate
Melanoma
Testis
Wo
men
Me
n
5 year survival
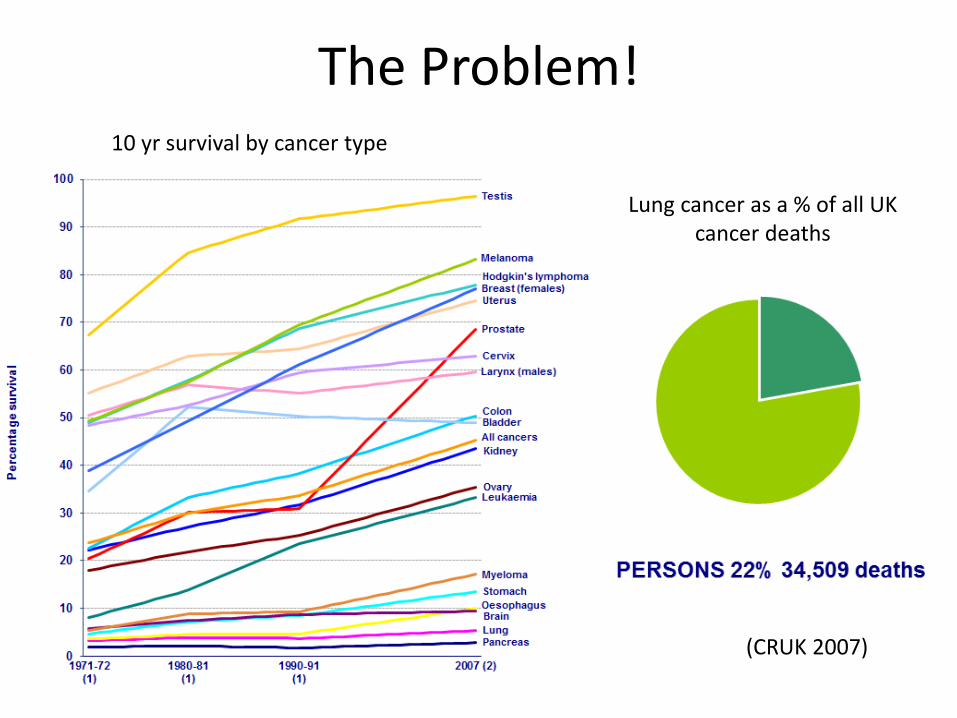
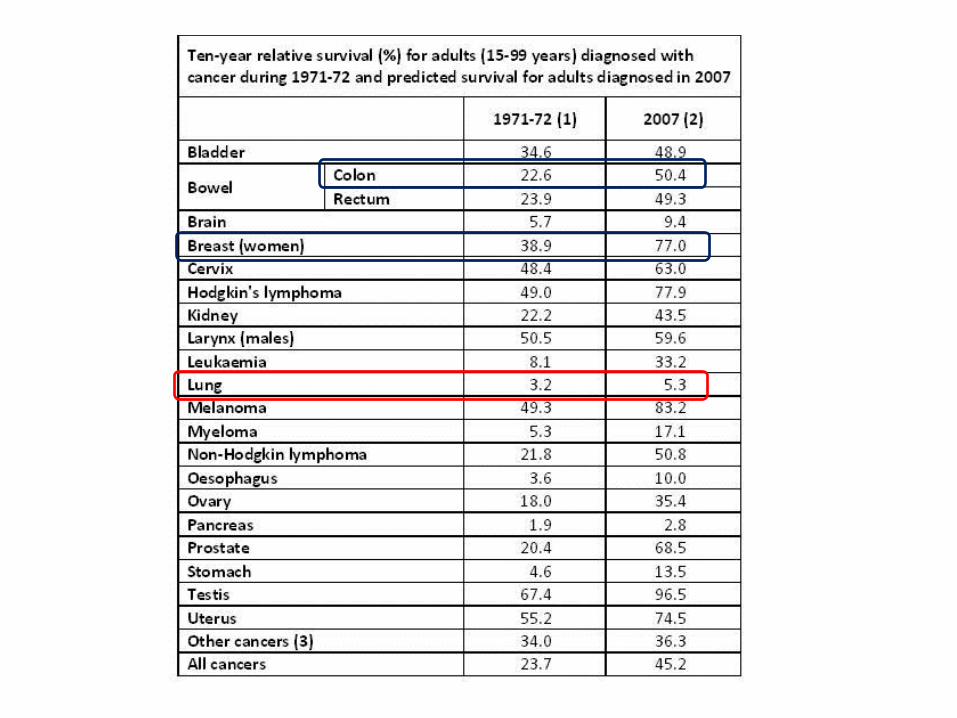
The Problem! 10 yr survival by cancer type
Lung cancer as a % of all UK cancer deaths
(CRUK 2007)
An illustration of why lung cancer survival is so poor despite great
changes between 2007 and 2013
• 67yr male
• Presented Jan 2007
• Cough 2/12
• Blood in sputum
• 4kg wt loss
• 10 pk yrs
Clinical Case
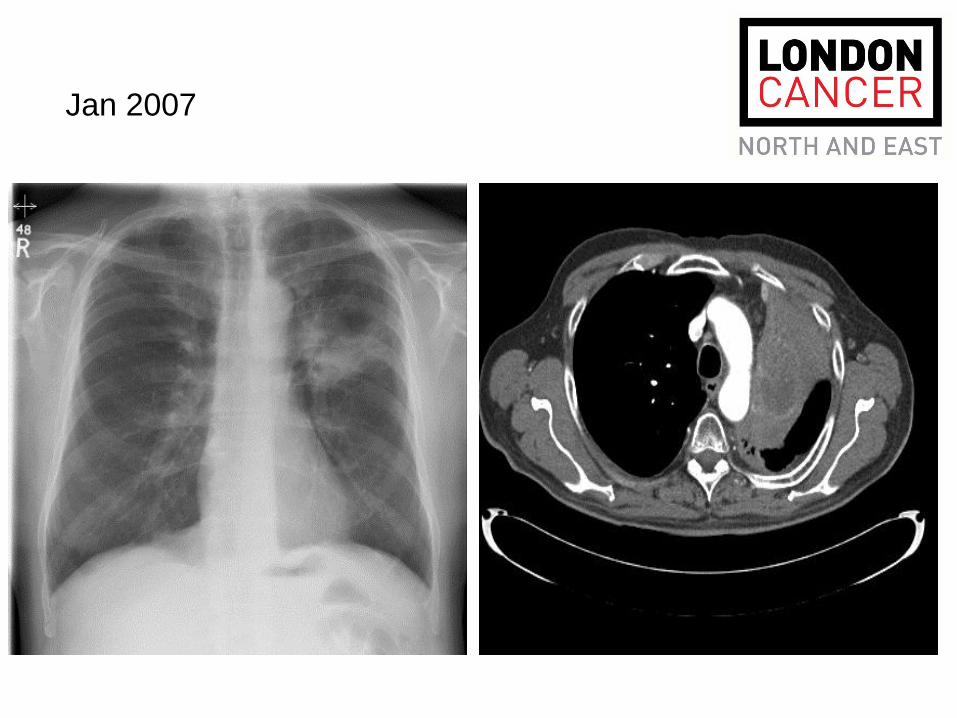
Jan 2007
Clinical Case
•T2N2M1disease (meaning he has metastatic disease) : NSCLC NOS
•(central mediastinal nodes and 2 asymptomatic bone metastases)
•MDT decision: chemotherapy (palliative)
•Started gemcitabine and carboplatin
•4th course assessment
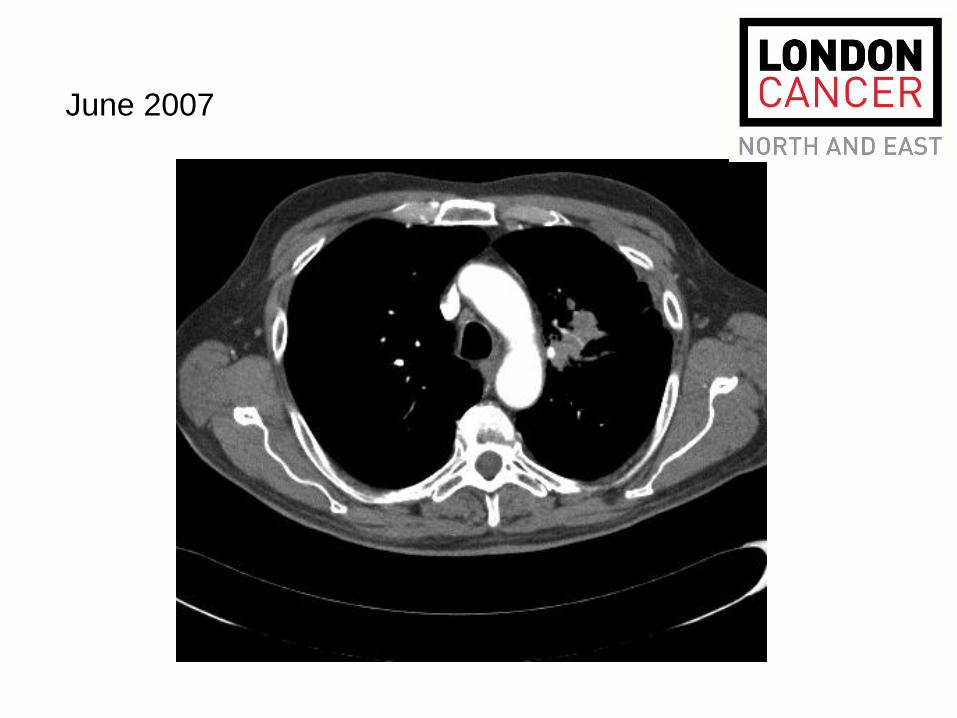
June 2007

Dec 2007
• T2N2M1disease: NSCLC NOS – ADENOCARCINOMA by EBUS
• (central mediastinal nodes and 2 asymptomatic bone metastases)
• EGFR MUTATIONAL ANALYSIS (POSSIBLY ALK)
• MDT decision: chemotherapy
• Started gemcitabine and carboplatin PEMETREXED/CISPLATIN
• 4th course assessment Maintenance?
• IF GOOD PS AND SIGNS OF RELAPSE – ERLOTINIB TKI
What would happen 5 years on in 2013?
Period of rapid change in lung cancer
• New Imaging: PET-CT, newer isotopes, prognosis, whole body MRI
• New Diagnostic tests EBUS/EUS
• New Radiotherapy techniques
• Minimally invasive surgery, sublobar resection
• Personalised systemic treatments (tablets)
So why are we making no inroads to survival? Because we continue to catch lung cancer too late
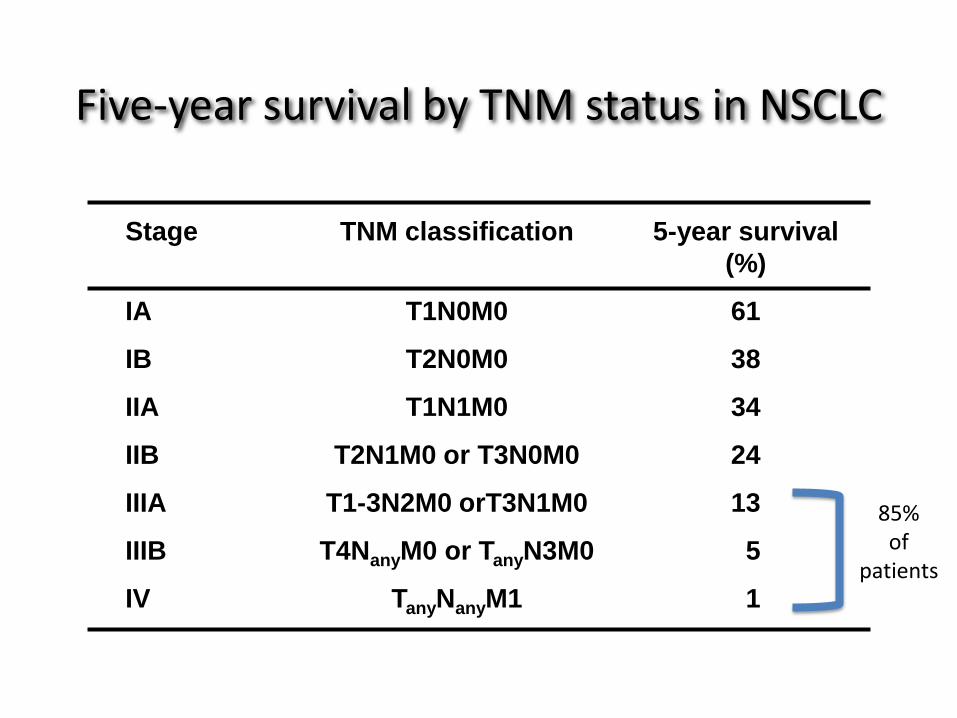
Five-year survival by TNM status in NSCLC
Stage
IA
IB
IIA
IIB
IIIA
IIIB
IV
TNM classification
T1N0M0
T2N0M0
T1N1M0
T2N1M0 or T3N0M0
T1-3N2M0 orT3N1M0
T4NanyM0 or TanyN3M0
TanyNanyM1
5-year survival
(%)
61
38
34
24
13
5
1
Mountain 1997
85% of
patients
• We need to detect lung cancer earlier
• Stage shift towards early- radically curable disease
• Survival benefit
Lung Cancer screening – where are we?
• Symptoms
• Risk scores
• Chest x-ray
• CT
Symptoms
Symptoms of advanced disease
• Change in cough
• New cough lasting >3 weeks
• Breathlessness
• Chest pain
• Haemoptysis
• Unexplained weight loss in a smoker
• Recurrent infection
• (Suddenly stopped smoking)
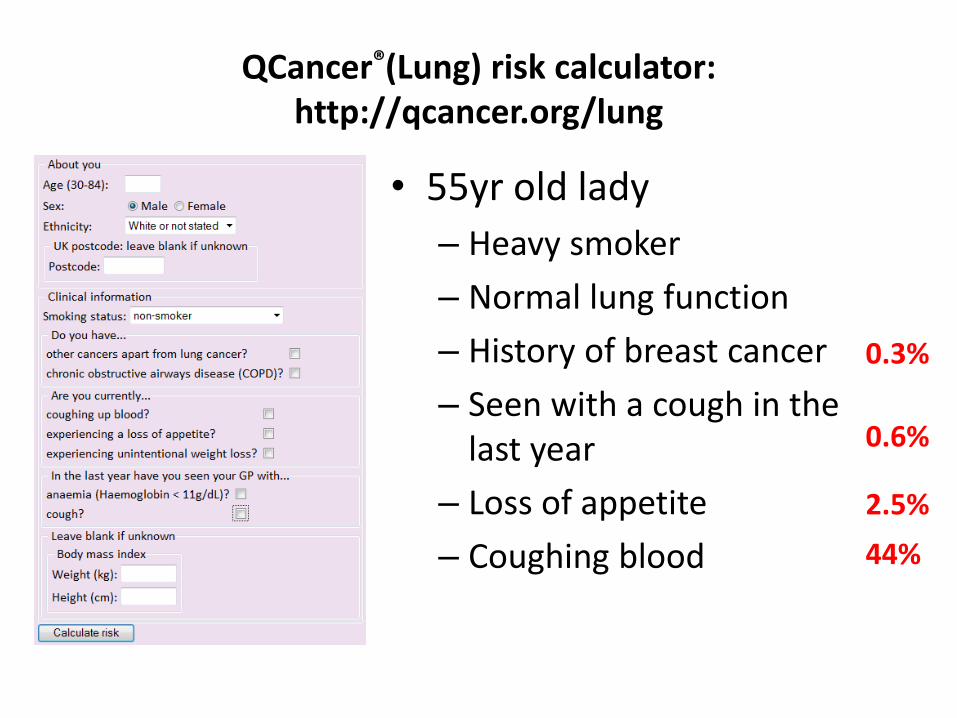
QCancer®(Lung) risk calculator: http://qcancer.org/lung
• 55yr old lady
– Heavy smoker
– Normal lung function
– History of breast cancer
– Seen with a cough in the last year
– Loss of appetite
– Coughing blood
0.3%
0.6%
2.5%
44%
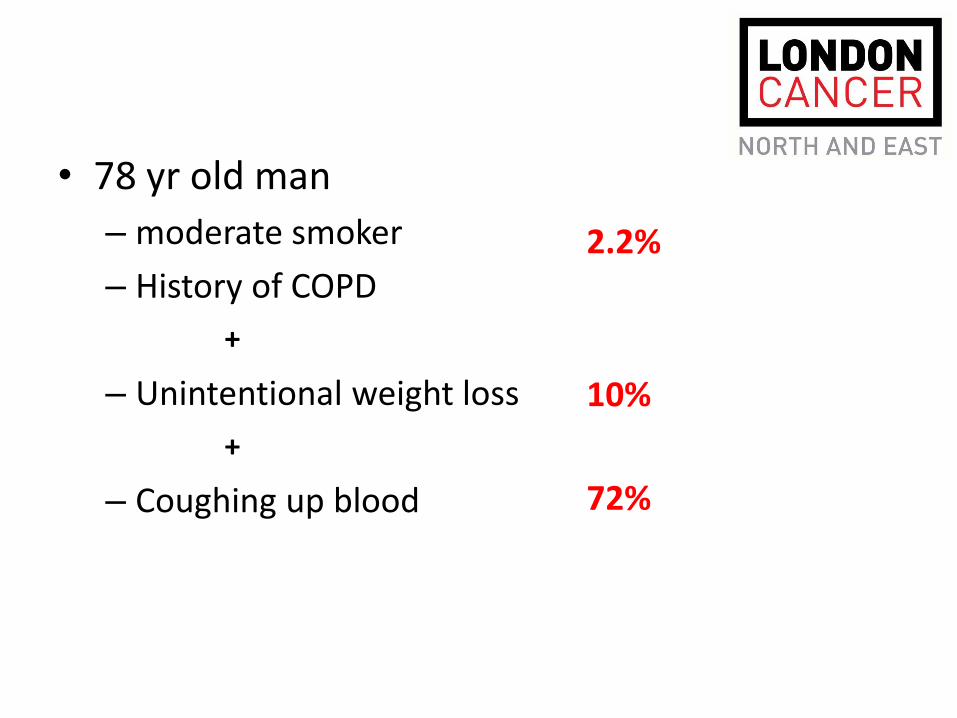
• 78 yr old man
– moderate smoker
– History of COPD
– Unintentional weight loss
– Coughing up blood
2.2%
10%
72%
+
+
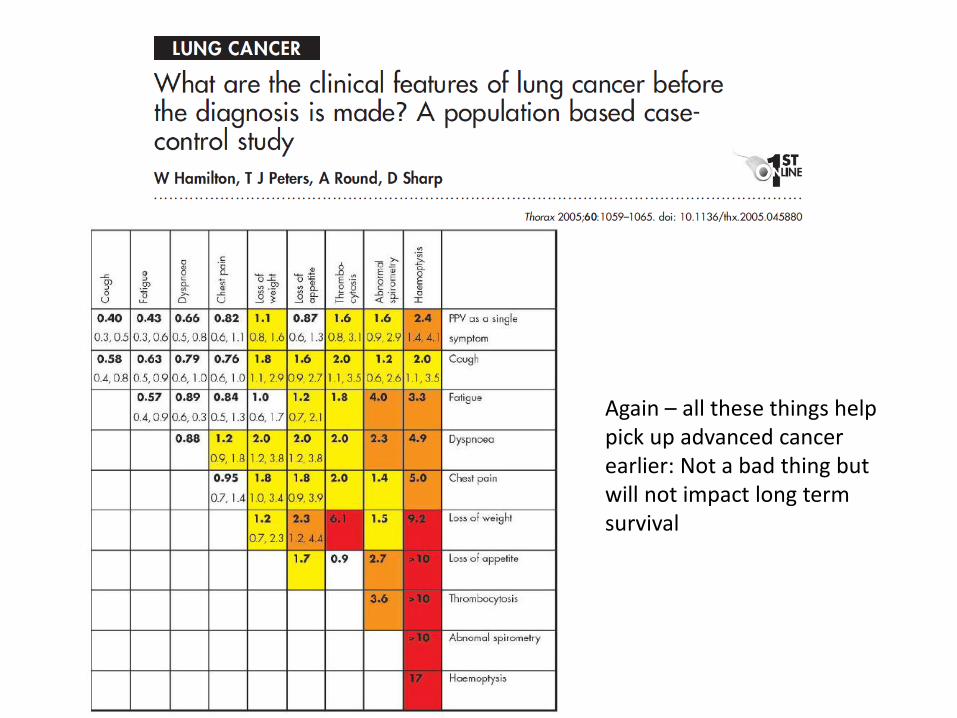
Again – all these things help pick up advanced cancer earlier: Not a bad thing but will not impact long term survival
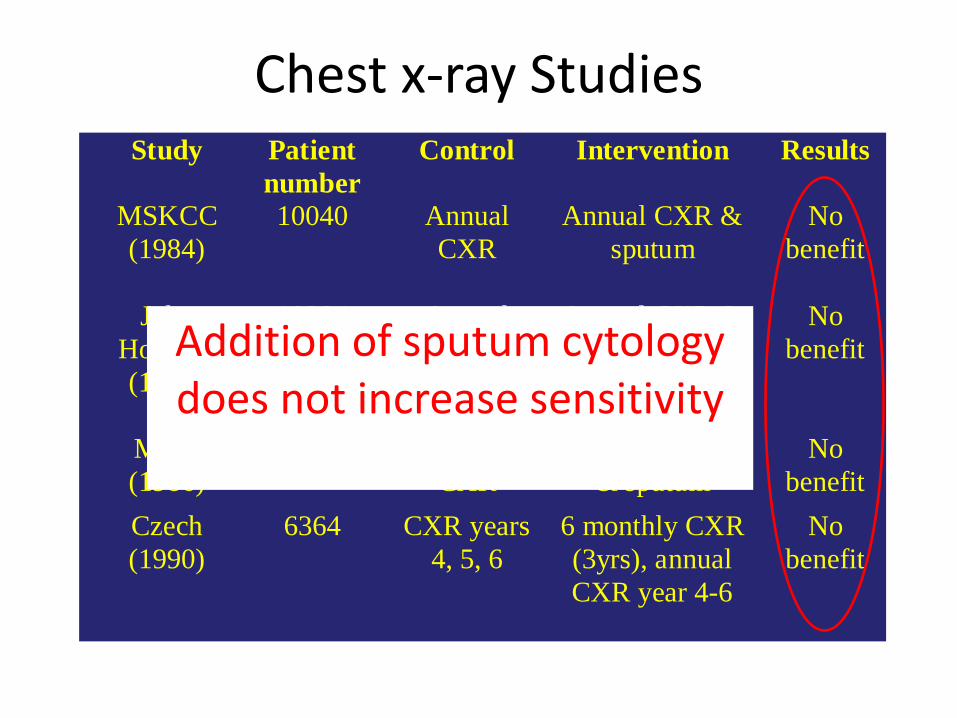
Chest x-ray Studies Study Patient
number
Control Intervention Results
MSKCC
(1984)
10040 Annual
CXR
Annual CXR &
sputum
No
benefit
John
Hopkins
(1986)
10384 Annual
CXR
Annual CXR &
4 monthly
sputum
No
benefit
Mayo
(1986)
9211 Annual
CXR
4 monthly CXR
& sputum
No
benefit
Czech
(1990)
6364 CXR years
4, 5, 6
6 monthly CXR
(3yrs), annual
CXR year 4-6
No
benefit
Addition of sputum cytology does not increase sensitivity
Lung Cancer screening – where are we?
• Symptoms
• Risk scores
• Chest x-ray
• CT
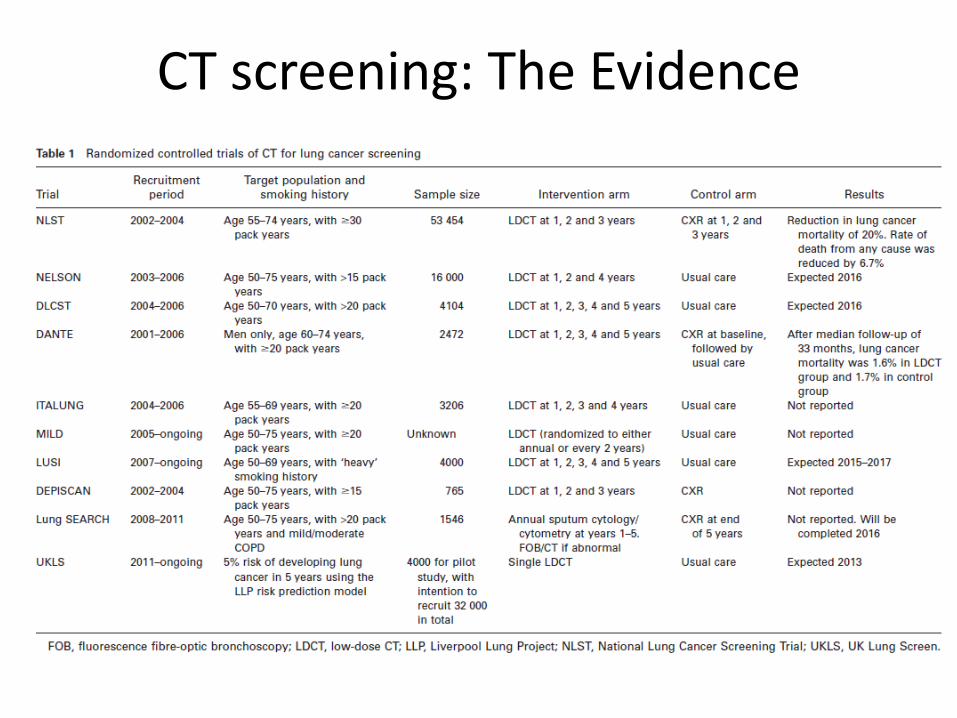
CT screening: The Evidence
Population 55-75 years old Smoker (or Ex) of 30 pack years
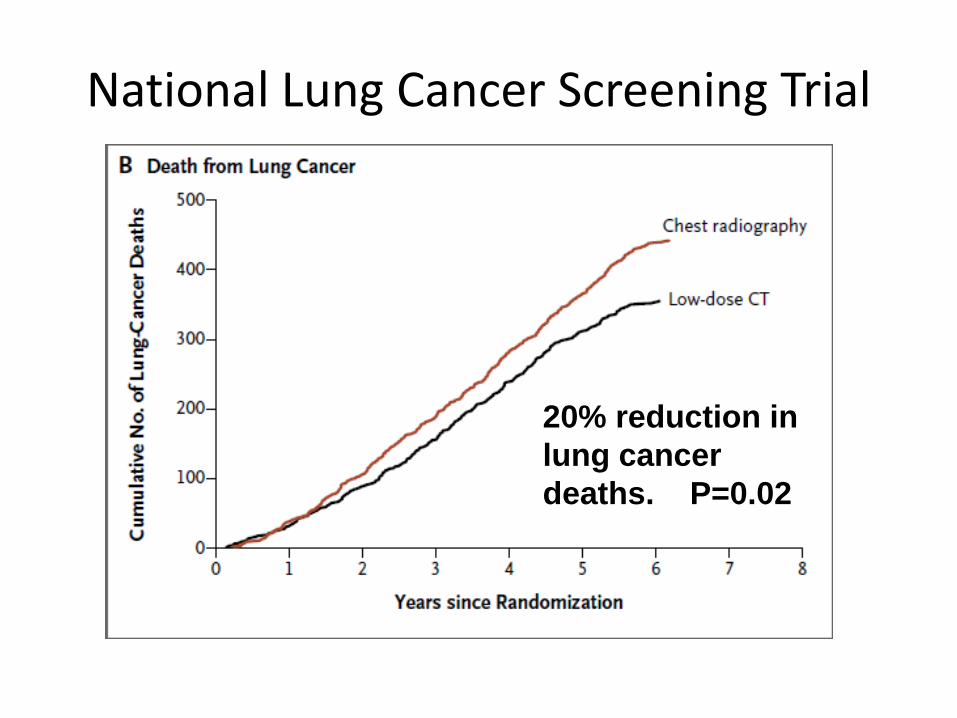
National Lung Cancer Screening Trial
20% reduction in
lung cancer
deaths. P=0.02
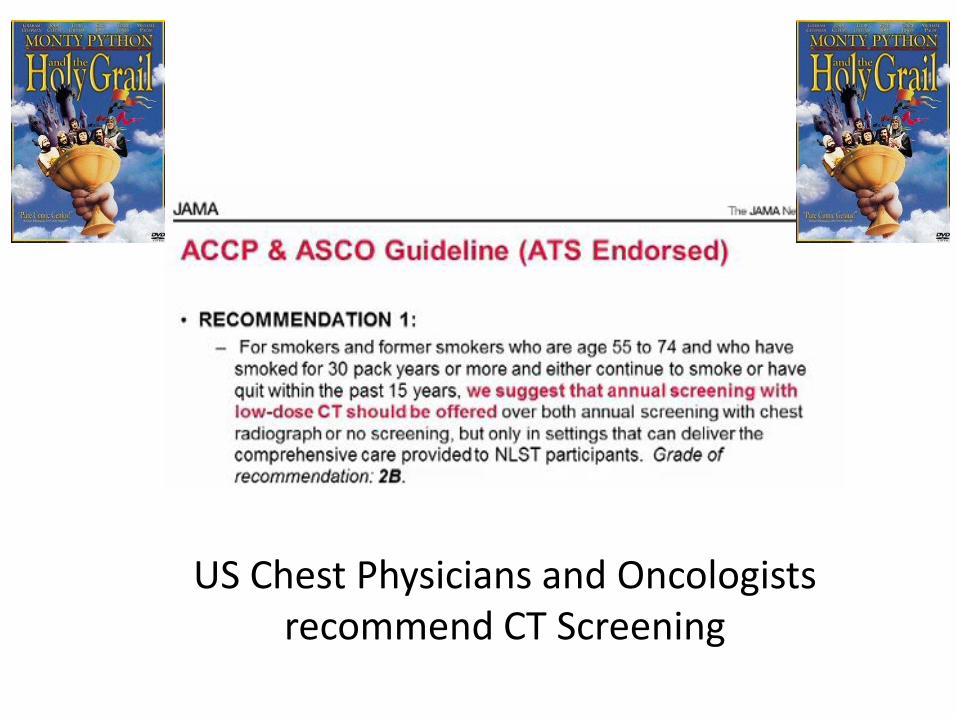
US Chest Physicians and Oncologists recommend CT Screening
• Over diagnosis
• False positive rates
• Patient acceptance/ anxiety/ radiation
• Cost per QALY
Potential Issues
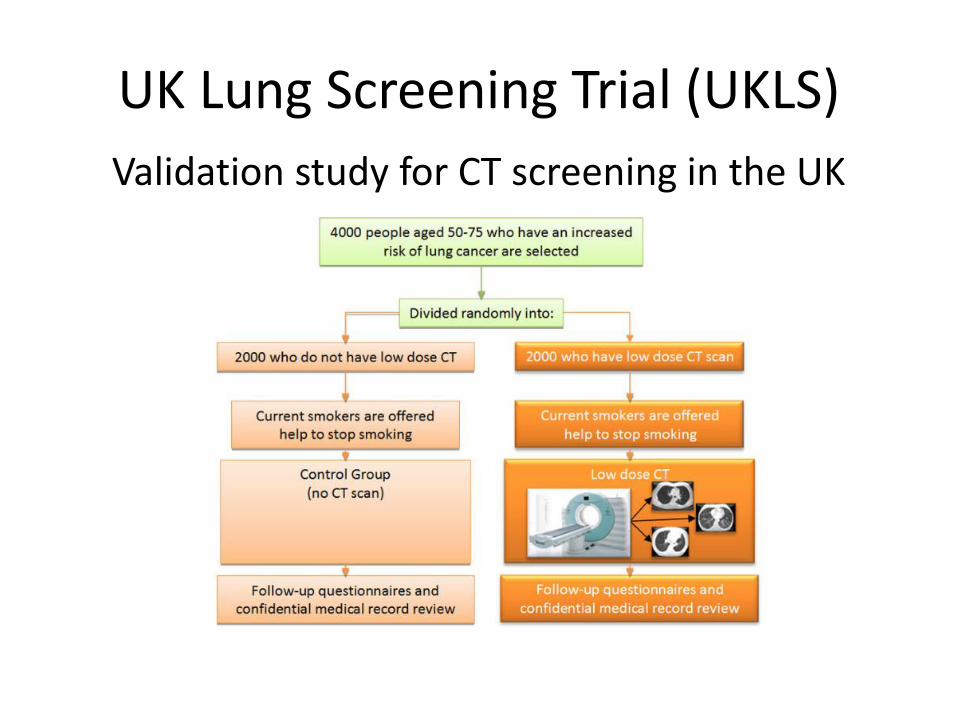
UK Lung Screening Trial (UKLS)
Validation study for CT screening in the UK
UKLS Update
• The investigators have been told their study will not progress beyond the pilot stage
London Cancer and CT Screening: Where do we stand?
• For every 300 scans performed one life will be saved
• We would like London Cancer to be at the forefront of delivering CT screening to the UK population
• We aim to provide the evidence required to decide how CT screening should be delivered to the UK population
The Team
• Lung Physicians
• Radiologists
• Experts in Cancer Screening (Prof Jane Wardle)
• Statisticians (Prof Stephen Duffy)
• The UKLS team (John Field and David Baldwin)
• The US team (NLST) (Dr Christine Berg)
• The Lung Cancer Leaders (Dr Mick Peak)
• The UKLS pilot trial recruited directly via population mailing, sending out 250,000 initial questionnaires to recruit 4000 individuals
Why is this needed?
We propose a demonstration project to:
• Research other models of identification of suitable
subjects for lung cancer screening, such as via primary care
• To build expertise in the screening technique • To investigate the immediate implications of screening
in the UK; (false positive rates etc) • Estimate the human and economic costs of the
screening; and • Investigate the effects of different levels of smoking
cessation support in participants
• We propose comparing invitation techniques in recruiting 2,000 subjects at high risk of lung cancer via primary care
• Subjects would be identified from practice records
• They would be offered a single low-dose CT scan for lung cancer
• In addition, we propose to randomised them to one of two smoking cessation interventions
The Project
The Project: Outcomes
• acceptability to GP’s and patients
• comparison of the recruitment rates and costs
• rates of suspicious findings requiring further workup
• detection rate of lung cancer at screening
• incidence of lung cancer in the three years following screening;
• likely costs of the combined screening and further diagnostic activity generated by the screening
• comparison of smoking cessation rates in the two randomised arms
The Plan: and funding!
• Full design of feasibility of implementation trial
• Understand what this will fund
• Gain funding for the NHS resource that will be used to enable the trial
• Likely scale: 80 practices/2000 patients; two areas in London Cancer
Thank you for listening