st. dominic’s cancer services public …€¦ · of the acr lung cancer screening committee...
TRANSCRIPT
ST. DOMINIC’S CANCER SERVICES
PUBLIC REPORTING OF OUTCOMES
2016
Cancer Services
Please review the following patient and program outcomes from St. Dominic’s Cancer Program. Please feel free to call Cancer Services at 601-200-3300 with any questions.
Lung Cancer Screening Program
Lung cancer is by far the leading cause of cancer death with about 1 out of 4 cancer deaths resulting from lung cancer. Each year, more people die of lung cancer than of colon, breast and prostate cancers combined. According to St. Dominic’s Cancer Community Needs Assessment and American Cancer Society’s “Cancer Facts & Figures 2015,” Mississippi was surpassed by only one state in rates of lung cancer deaths. Therefore the St. Dominic ‘s Cancer Committee chose to monitor outcomes from lung cancer screenings at St. Dominic’s.
The American College of Radiology (ACR)’s Lung Cancer Screening Registry (LCSR) is designed to systematically audit the quality of interpretation of screening lung CT exams. The registry is based on the ACR Lung Imaging Reporting and Data System (Lung-RADS), which is the product of the ACR Lung Cancer Screening Committee subgroup on Lung-RADS. This Lung-RADS system is a quality assurance tool designed to standardize lung cancer screening CT reporting and management recommendations, reduce confusion in lung cancer screening CT interpretations and facilitate outcome monitoring. The ACR LCSR captures Lung-RADS recommendations and monitors and compares the appropriate uses of Lung-RADS.
We received data from the Lung Cancer Screening Registry for 12 patients that were screened at St. Dominic’s. Below are measures calculated from data submitted during January – September 2016 with comparisons of St. Dominic’s with other LSCR facilities.
• Appropriateness of screening by USPSTF criteria: Percent of screening population who are adults aged 55 to 80 years, have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years. o Compared to all LSCR facilities who were 89.53 percent and Community LCSR facilities who were at 90.12 percent, St. Dominic’s was at 100 percent for appropriateness of screening.
• Lung Cancer Detection Rate (CDR) per 1,000: Number per 1,000 screening exams that had both a Lung-RADS assessment category of 3 or 4a, 4b, 4x and a tissue diagnosis of cancer within 12 months. o Compared to all LSCR facilities who were 3.28 percent, St. Dominic’s was at zero percent of lung cancers detected.
• Lung Cancer Screening Abnormal Interpretation Rate (Recall Rate) during annual exam: Percent of annual lung cancer screening exams that have a Lung-RADS assessment of 3, 4a, 4b, or 4x (and lead to additional imaging or biopsy) o Compared to all LSCR facilities who were 19.02 percent, St. Dominic’s was at 8.33 percent of exams with a Lung-RADS assessment of 3, 4a, 4b or 4x leading to additional imaging or biopsy.
Cancer Program Practice Profile Reports (CP3R)
St. Dominic’s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive high quality care that is congruent with nationally accepted measures. To promote comparison and allow for monitoring, the Commission on Cancer (CoC) measures compliance with specific CoC reporting tools including the Cancer Program Practice Profile Reports (CP3R). Below is data from 2014 for one measure followed for breast cancer patients.
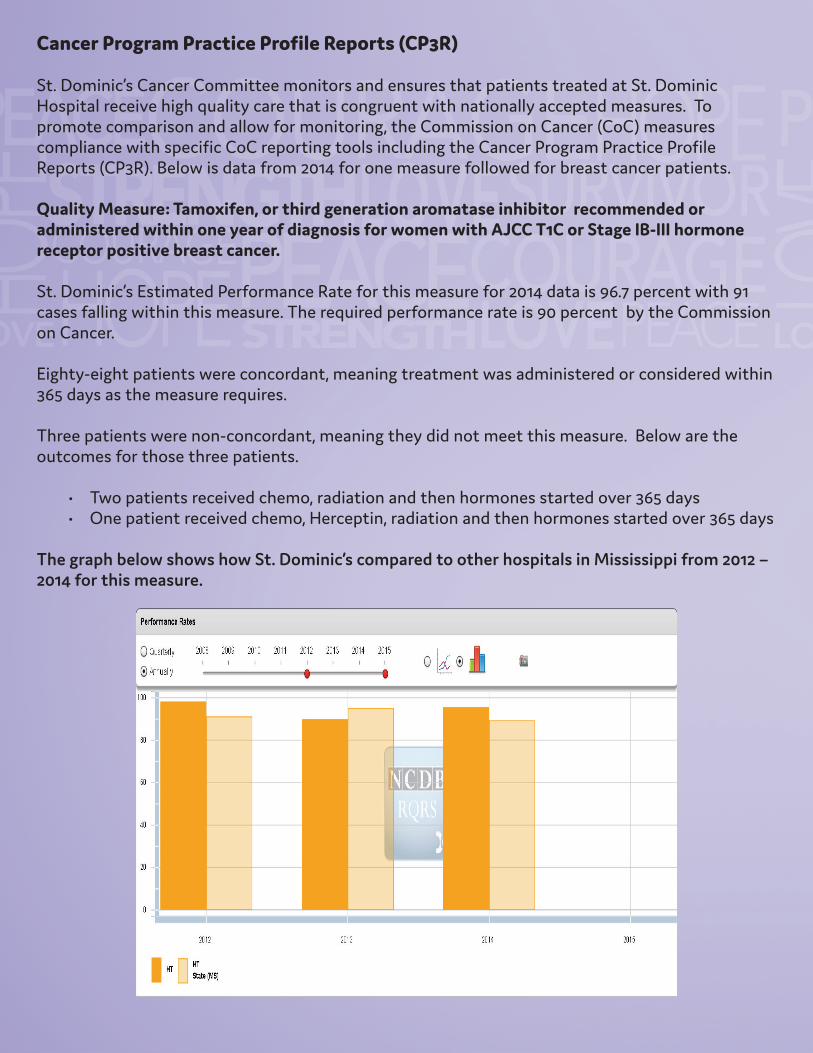
Quality Measure: Tamoxifen, or third generation aromatase inhibitor recommended or administered within one year of diagnosis for women with AJCC T1C or Stage IB-III hormone receptor positive breast cancer.
St. Dominic’s Estimated Performance Rate for this measure for 2014 data is 96.7 percent with 91 cases falling within this measure. The required performance rate is 90 percent by the Commission on Cancer.
Eighty-eight patients were concordant, meaning treatment was administered or considered within 365 days as the measure requires.
Three patients were non-concordant, meaning they did not meet this measure. Below are the outcomes for those three patients.
• Two patients received chemo, radiation and then hormones started over 365 days • One patient received chemo, Herceptin, radiation and then hormones started over 365 days
The graph below shows how St. Dominic’s compared to other hospitals in Mississippi from 2012 – 2014 for this measure.

Monitoring Compliance with Evidence-based Guidelines
Each calendar year, the St. Dominic’s Cancer Committee designates a physician member to complete an in-depth analysis to assess and verify that cancer program patients are evaluated and treated according to evidence-based national treatment guidelines. Dr. Bobby Graham, St. Dominic’s Cancer Committee Chairman, performed an in-depth review of stage IV breast cancer patient with bone metastasis and multiple myeloma patients to determine if appropriate standards for adjunctive treatment were being met. National Comprehensive Cancer Network (NCCN) guidelines state that breast cancer patients with bone metastasis denosumab, zoledronic acid or pamidronate should be given (category 1) in addition to chemotherapy or endocrine therapy (if expected survival is greater than or equal to 3 months, and renal function is adequate). Bisphosphonates (pamidronate and zoledronic acid) are to be used in all myeloma patients receiving primary therapy. Use of bisphosphonates in smoldering or stage I disease should be given preferably in context of a clinical trial. The patients being treated with bisphosphonates should be monitored for renal dysfunction.
Cancer registry and electronic health record data were reviewed from years 2011 to 2015 in July of 2016.
There were 33 cases of stage IV breast cancer with bone metastasis. Of these, seven cases were ineligible: three received palliative care only, two were patients with unobtainable records, and two were patients to whom treatment was provided at an outside facility and not actively treated by a St. Dominic’s affiliated medical oncologist. Of the 26 eligible patients, 16 received denosumab, zoledronic acid or pamidronate.
There were 54 total multiple myeloma cases identified during this time. Fifteen were ineligible: four received palliative care only, seven had renal failure, one patient’s records were not available, and three patients were treated at outside facilities not affiliated with St. Dominic’s Cancer Services. Of the 39 eligible patients, 32 were treated with bisphosphonates.