diabetes mellitus patients in dental management reporter : 吳和泰 modulator: dr. 雷文天
TRANSCRIPT

Diabetes Mellitus patients
in dental management
Reporter : 吳和泰 Modulator: Dr. 雷文天

Introduction Diabetes mellitus is a metabolic disorder charact
erized by relative or absolute insufficiency of insulin, and resultant disturbances of carbonhydrate metabolism.
The major function of insulin is to counter the concerted action of a number of hyperglycemia-generating hormones and to maintain low blood glucose levels.
Epidemiology 6% (16 million persons) of the general population
in the US have diabetes mellitus. Almost 20% of adult older than 65 y/o have DM. A dental practice serving an adult population of
2,000 can expect to encounter 40-80 persons with diabetes, about half of whom will be unaware of their condition.
National Institutes of Health, Aug 2001

國人之糖尿病盛行率
Etiologic classification of DM
There are two types of Diabetes Mellitus:
Type 1, insulin-dependent or, juvenile-onset diabetes (IDDM)
Type 2, non-insulin-dependent, adult-onset diabetes (NIDDM)
Other specific types
JADA, Oct 2001
Type 1 (IDDM)
Autoimmune destruction of the insulin-producing beta cells of pancreas.
5-10% of DM cases. Common occurs in childhood and adolescence, o
r any age. Absolute insulin deficiency. High incidence of severe complications. Prone to autoimmune diseases. (Grave’s, Addiso
n, Hashimoto’s thyroiditis)

Type 2 (NIDDM)
Result from impaired insulin function. (insulin resistance)
Constitutes 90-95% of DM Specific causes of this form are unknown. Risk factors : age, obesity, alcohol, diet, family H
x and lack of physical activity..etc.

ComparisonComparison Type 1 Type 2
Clinical onset <20 years onset >30 years
normal weight obesity
decreased blood insulin normal or increased blood insulin
anti-islet cell antibodies no anti-islet cell antibodies
Genetics ketoacidosis common ketoacidosis rare
human leukocyte antigen (HLA)-D linked
No HLA association
Pathogenesis autoimmunity, immunopathologic mechanisms
insulin resistance
severe insulin deficiency relative insulin deficiency
Islet Cells insulitis early no insulitis
marked atrophy and fibrosis
focal atrophy and amyloid deposits
severe beta-cell depletion mild beta-cell depletion

Other specific types
Genetic defects of beta-cell functions Decrease of exocrine pancreas Endocrinepathothies Drug or chemical usage Infections
………….
Gestational diabetes mellitus (GDM)
Defined as any degree of glucose intolerance with onset or first recognition during pregnancy.
4% of pregnancy in US.

Pathophysiology
Healthy people blood glucose level maintained within 60 to 150 mg/dL.
Insulin synthesized in beta cells of pancreas and secreted rapidly into blood in response to elevations in blood sugar.
Promoting uptake of glucose from blood into cells and its storage as glycogen
Fatty acid and amino acids converted to triglyceride and protein stores.

Pathophysiology
Lack of insulin or insulin resistance, result in inability of insulin-dependent cells to use glucose.
Triglycerides broken down to fatty acids blood ketones↑ diabelic ketoacidosis.
Pathophysiology
As blood sugar levels became elevated (hyperglycemia), glucose is excreted in the urine and excessive of urination occurs due to osmotic diuresis (polyuria).
Increased fluid loss leads to dehydration and excess thirst (polydipsia).
Since cells are starved of glucose, the patient experiences increased hunger (polyphagia).
Paradoxically, the diabetic patient often loss weight, since the cells are unable to take up glucose.

Complications
People with DM have an increased incidence of both microvascular and macrovascular complications.Major organs/systems showing changes Long term complications
Cardiovascular system: heart, brain, blood vessels
myocardial infarct; atherosclerosis; hypertension; microangiopathy; cerebral vascular infarcts; cerebral hemorrhage
Pancreas islet cell loss; insulitis (Type 1); amyloid (Type 2)
Kidneys nephrosclerosis; glomerulosclerosis; arteriosclerosis; pyelonephritis
Eyes retinopathy; cataracts; glaucoma
Nervous system autonomic neuropathy; peripheral neuropathy
Peripherals peripheral vascular atherosclerosis; infections; gangrene
Diagnosis A casual plasma glucose level of 200 mg/dL or g
reater with symptoms presented. Fasting plasma glucose level of 126 or greater.
(Normal <110 mg/dL,IGT,IFG) Oral glucose tolerance test (OGTT) value in bloo
d of 200 mg or greater.
ADA recommend >45 y/o screened every 3 years.
Diabetes Care, 2000National Institutes of Health, Aug 2001
Medical management
Objective : maintain blood glucose levels as close to normal as possible.
Good glycemic control inhibits the onset and delay of type 1 DM, similar in type 2 DM.
Medical management
Glycated hemoglobin assay (HbA1c ) reflects mean glycemia levels over the proceding 2~3 months. (normal < 7%)
HbA1c also a predictor for development of chronic complications.

Medical management Exercise and diet control Insulin : rapid, short, intermediate, long acting. Oral antidiabetic agents

Oral manifestations and complications
No specific oral lesions associated with diabetes. However, th
ere are a number of problems by present of hyperglycemia.
Periodontal disease Microangiopathy altering antigenic challenge. Altered cell-mediated immune response and impaired of neutrop
hil chemotaxis. Increased Ca+ and glucose lead to plaque formation. Increased collagen breakdown.

Oral manifestations and complications Salivary glands
Xerostomia is common, but reason is unclear. Tenderness, pain and burning sensation of tongue. May secondary enlargement of parotid glands with sialosis.
Dental caries Increase caries prevalence in adult with diabetes. (xerostomia, in
crease saliva glucose) Hyperglycemia state shown a positive association with dental ca
ries.

Oral manifestations and complications Increased risk of infection
Reasons unknown, but macrophage metabolism altered with inhibition of phagocytosis.
Peripheral neuropathy and poor peripheral circulation Immunological deficiency High sugar medium Decrease production of Ab
Candical infection are more common and adding effects with xerostomia
Oral manifestations and complications Delayed healing of wounds
Due to microangiopathy and ultilisation of protein for energy, may retard the repair of tissues.
Increase prevalence of dry socket.
Miscellaneous conditions Pulpitis : degeneration of vascular. Neuropathies : may affect cranial nerves. (facial) Drug side-effects : lichenoid reaction may be associated with sul
phonylurea. (chlopropamide) Ulcers
New Zealand Journal, Jan 1985
Dental management considerations
To minimize the risk of an intraoperative emergency, clinicians need to consider some issues before initiating dental tx.
Medical history : take hx and assess glycemic control at initial appt. Glucose levels Frequency of hypoglycemic episodes Medication, dosage and times. Consultation
Dental management considerations Scheduling of visits
Morning appt. (endogeneous cortisol) Do not coincide with peak activity.
Diet Ensure that the patient has eaten normally and taken medications as us
ual. Blood glucose monitoring
Measured before beginning. (<70 mg/dL) Prophylactic antibiotics
Established infection Pre-operation contamination wound Major surgery

Dental management considerations During treatment
The most complication of DM occur is hypoglycemia episode. Hyperglycemia
After treatment Infection control Dietary intake Medications : salicylates increase insulin secretion and sensitivit
y avoid aspirin.
Emergency management
Hypoglycemia Initial signs : mood changes, decreased spont
aneity, hunger and weakness.Followed by sweating, incoherence, tachycard
ia.Consequenced in unconsiousness, hypotenti
on, hypothermia, seidures, coma, even death.
Emergency management
15 grams of fast-acting oral carbonhydrate. Measured blood sugua. Loss of conscious, 25-30ml 50% dextrose soluti
on iv. over 3 min period. Glucagon 1mg. 911, 119
Emergency management
Severe hyperglycemiaA prolonged onsetKetoacidosis may develop with nausea, vomiti
ng, abdominal pain and acetone odor.Difficult to different hypo- or hyper-.
Emergency management
Hyperglycemia need medication intervention and insulin administration.
While emergency, give glucose first ! Small amount is unlikely to cause significant
harm.
JADA, Oct 2001
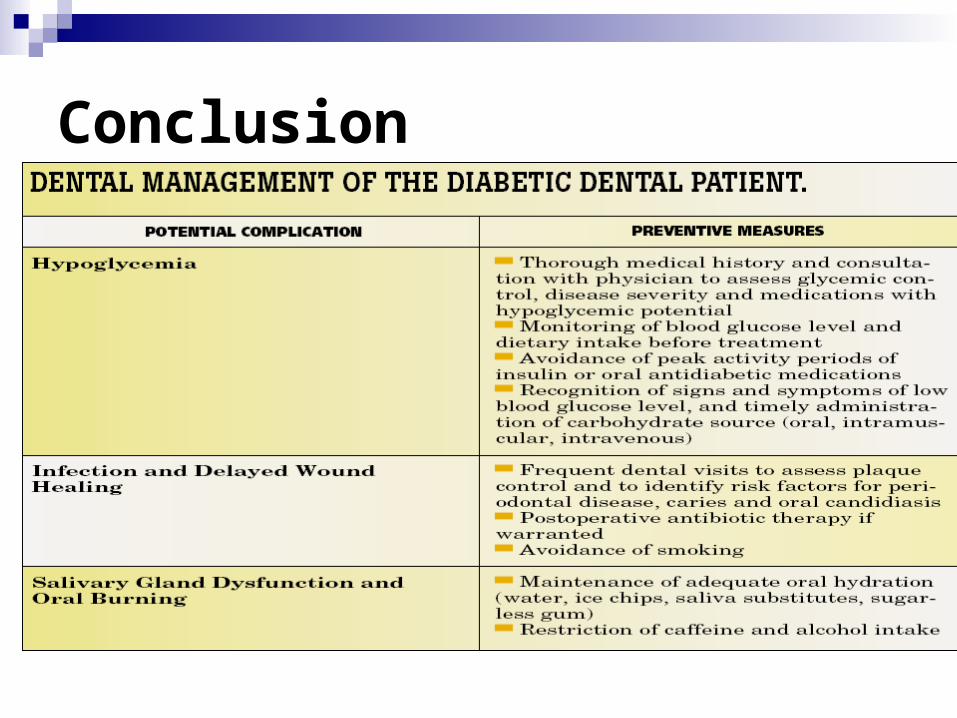
Conclusion
Thanks for ur attention !!

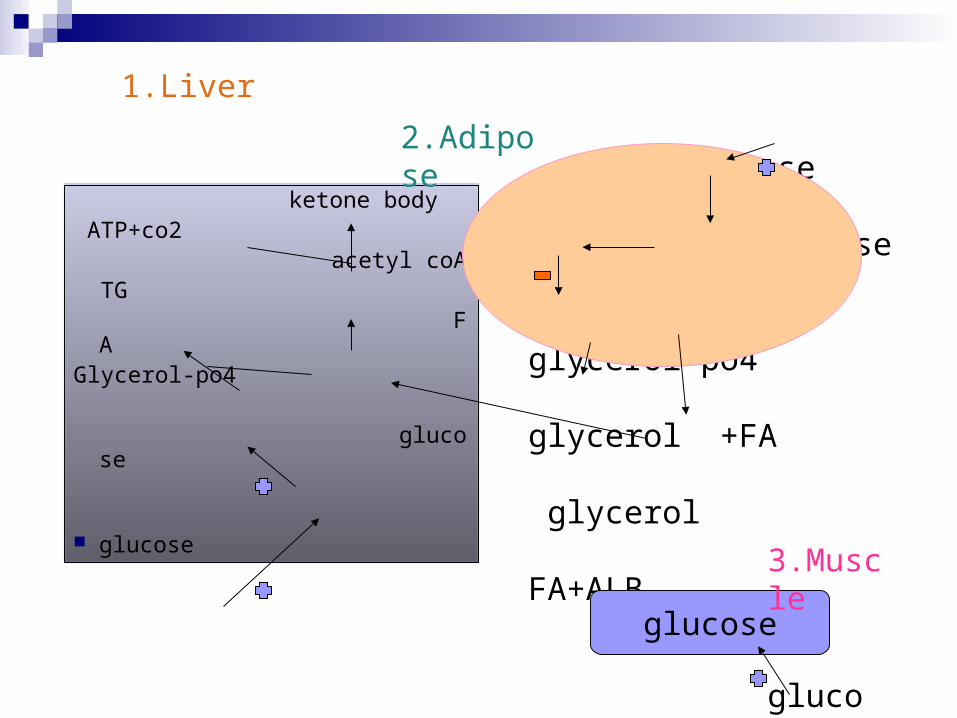
1.Liver
ketone body ATP+co2 acetyl coA TG FAGlycerol-po4 glucose
glucose
glucose glucose
TG glycerol-po4
glycerol +FA
glycerol FA+ALB
2.Adipose
glucose
glucose
3.Muscle