development and evaluation of the oasi care bundle: a …€¦ · induction of labour birthweight...
TRANSCRIPT

Development and evaluation of the OASI Care Bundle: A quality improvement project
to reduce the rates of severe perineal trauma
Posy Bidwell & Alexandra Hellyer

What is an OASI?
An obstetric anal sphincter injury (OASI) is any degree of injury to the anal sphincter muscle sustained during childbirth.
Consequences
• Anal and urinary incontinence, chronic pain, infection
• Multiple attendances for hospital and community treatment
• Caesarean section for subsequent births
• Dyspareunia (painful sexual intercourse)
• Psychosocial disorders (including PTSD)
‘I have permanent
damage to my bowel, pelvic floor and nerve in
my left bum cheek’
‘My experience postnatally has made me terrified when I hear of
others who are about to give birth’
‘I don’t feel as if I’ll ever
be ok’

Why are we doing this?
Rates of OASI in the UK have risen over the last ten years from 1.8% to 5.9%, amounting
to 70,000 women being
affected during this period1
Long-term consequences can be debilitating causing complex
physical and psychosocial burdens which severely impact a
woman’s quality of life, as well a financial burden to the NHS 3
For many women there is no clear reason why they
sustain an OASI. However, underlying problems such as
inconsistencies in practice (e.g. ‘hands on’
or ‘hands poised’) have been identified as
contributing factors
1. GUROL-URGANCI, I. et al. Third- and fourth-degree perineal tears among primiparous women in England between 2000 and 2012: time trends and risk factors BJOG 2013; 120: 1516-25. 2. ABBOTT, D. et al. Obstetric anal sphincter injury. BMJ 2010; 341.
3. PRIDDIS, H. S. Autoethnography and severe perineal trauma—an unexpected journey from disembodiment to embodiment. BMC Women's Health 2015 ; 15: 88
Risk factors for OASI2
Nulliparity
South Asian ethnicity
Induction of labour
Birthweight > 4kg
Persistent occiptio-posterior
position
Prolonged second stage
Instrumental delivery

Evidence of successful interventions
• Norwegian experience that 50% of tears can be prevented through1
• Perineal support
• Women moving freely during birth and pushing in a comfortable position
• Women adopting a position during the last minutes of pushing to allow visualisation of the perineum and perineal support technique
• Mediolateral episiotomy on indication only
• Experiences in the UK • Croydon and Plymouth adopted similar package of interventions to Norway
• Decreased by 23% and 31%, respectively2,3
1Laine K et al. Incidence of obstetric anal sphincter injuries after training to protect the perineum. BMJ Open. 2012. 2Hollands H (personal communication 18 May 2015).
3Naidu M et al. Reducing obstetric anal sphincter injuries using perineal support a preliminary experience. Female Pelvic Medicine & Reconstructive Surgery. 20 (Supplement 1):S1-S40, July/August 2014.

0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
19
68
19
71
19
74
19
77
19
80
19
83
19
86
19
89
19
92
19
95
19
98
20
01
20
04
20
07
20
10
20
13
OASIS (%), all vaginal deliveries
Denmark
Sweden
Norway
Finland
Ullevål
Fredrikstad
Laine K et al. AOGS 2012
Laine K et al. EJOGRB 2009
The Scandinavian success story

Development of the OASI Care
Bundle
May 2014:
Summit held to discuss the increase in OASI. RCM & RCOG write a
joint statement of support for this work.
October 2014:
Working group of experts from RCM,
RCOG & LSHTM formed. Systematic
review of intrapartum interventions to reduce
OASI
November 2014:
OASI Care Bundle group discusses the
evidence and the acceptability and feasibility of each
identified intervention
March 2015:
OASI Care Bundle group participates in a consensus meeting to agree the elements of
the care bundle
January 2016:
Pilot study of the OASI Care Bundle in two
maternity units
May 2016:
Funding obtained from The Health Foundation
to upscale the OASI Care Bundle to sixteen
units as part of a quality improvement programme to reduce
OASI rates
What is a Care Bundle?
A care bundle is a small set of evidence-based interventions for a defined patient segment or population and care setting that, when implemented together, will result in significantly better outcomes than when implemented individually.
Institute for Healthcare Improvement

What does the OASI Care Bundle involve?
Inform the woman about OASI and what can be done
to minimize her risk.
When indicated, episiotomy should be performed
mediolaterally at a 60-degree angle at crowning.
Documented use of manual perineal protection (MPP):
- For spontaneous births, MPP should be used unless the woman objects, or her chosen birth position doesn’t allow for it. - For assisted births MPP should always be used.
Following birth, the perineum should be examined and any tears graded according to the RCOG guidance. The
examination should include a per rectum check even
when the perineum appears intact.
1
2
3
4

Implementation

What does implementation involve?
Multi-disciplinary skills development
module
Awareness Campaign
The Care Bundle
Local Champions attend a Skills Development Day • Training in interventions • Guidance and support in rolling out in their units Training materials provided: • e.g. videos, visual aids
• 4 evidence-based interventions that, when implemented together, will result in significantly better outcomes than when implemented individually.
• A Care Bundle Guide is provided
Such as posters, pens, balloons, memory aids,
newsletter

The intervention will be facilitated by: 1. Local clinical champions (one midwife and one obstetrician from each unit). They will champion the project including: ensuring that staff have completed the multi-disciplinary skills development module, monitoring local compliance with the care bundle, reporting on unit-level OASI rates, and participating in shared learning days with the other units in their block.
2. Leadership and support from professional organisations will be provided by the Royal College of Obstetricians and Gynaecologists (RCOG) and the Royal College of Midwives (RCM) who will actively promote the project and will provide a joint statement endorsing the use of care bundle. In addition, the professional and educational networks of the Colleges will be actively used to support the skills development module.
3. Continuous monitoring and feedback will allow participant units to measure their progress, by reporting their OASI rates, compliance with the care bundle, and uptake of the skills development module. Units will participate in shared learning days with other units to provide a forum to discuss the project as it progresses.

Theory of Change

Project set-up 2016 2017 2018
Region 1 Transition Implementation
Region 2
Region 3
Region 4
Evaluation Implementation outcomes Clinical outcomes
Dissemination
Planning Transition Implementation
Skills development
day
Shared learning day
Overall programme plan St
ages
in e
ach
re
gio
n
Where we are now



Evaluation
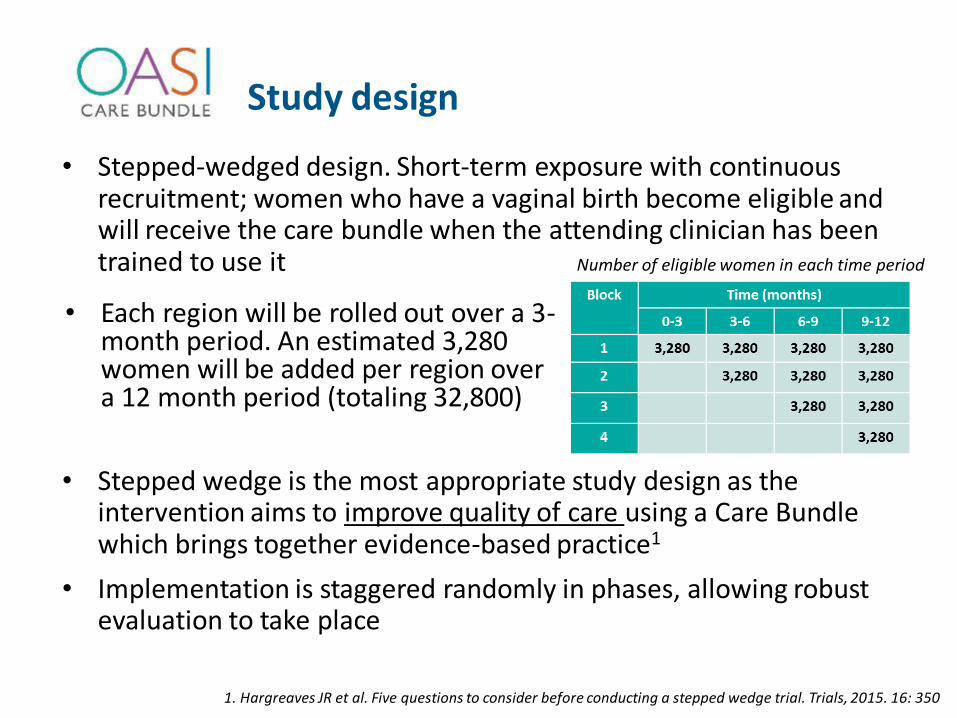
Study design
• Stepped-wedged design. Short-term exposure with continuous recruitment; women who have a vaginal birth become eligible and will receive the care bundle when the attending clinician has been trained to use it
• Stepped wedge is the most appropriate study design as the intervention aims to improve quality of care using a Care Bundle which brings together evidence-based practice1
• Implementation is staggered randomly in phases, allowing robust evaluation to take place
1. Hargreaves JR et al. Five questions to consider before conducting a stepped wedge trial. Trials, 2015. 16: 350
• Each region will be rolled out over a 3-month period. An estimated 3,280 women will be added per region over a 12 month period (totaling 32,800)
Number of eligible women in each time period

Was this a vaginal birth?
Was this birth eligible for use of the care
bundle?
Was this birth compliant with all four elements of the care
bundle?
Yes – eligible
No - not eligible
No – not eligible
A
C
B
Answer question B
Answer question C
Water birth or birthing stool
A caesarean section was performed
Was the clinician trained in using the care bundle?
All 4 elements of the care bundle used, if clinically
appropriate?
Eligibility and compliance
No – not
complaint
Yes – compliant to
the care bundle
Yes – eligible
Primary outcome: • Analysed retrospectively using anonymised patient-level
data (18 months) from local maternity information systems (MIS).
Secondary outcomes: • Quantitative and qualitative data used to provide
information about barriers and enablers with uptake and scaling-up interventions
• Implementation outcomes will be evaluated to assess acceptability, feasibility, coverage and sustainability of the intervention as well as the implementation strategies.

Evaluation of implementation outcomes
Standardised delivery of the evidence based
intervention
Improved knowledge, awareness & skills
Continued uptake & sustainability of the
intervention
Acceptability Satisfaction with
intervention
Feasibility Extent to which
intervention can be applied
Coverage Extent to which population
receive the intervention
Sustainability Extent to which
intervention is maintained
Clinicians at sites (128) • Readiness for change (RfC)
questionnaire prior to focus group
• Focus groups
Women (20) • Interviews
• Routine monitoring of basic data
Champions (64) • Readiness for change (RfC)
questionnaire prior to roll-out • Focus groups at the end of
transition phase • Follow-up interviews

Evaluation timeline
Planning Roll-out Implementation
Skills development
Shared learning day
Stag
es
in
eac
h b
lock
Feedback (champions)
Routine monitoring of basic data
Interviews (champions)
Focus groups & RfC measure
(clinicians)
Focus groups (champions)
Interview & RfC measure (champions)
Interviews with women

The importance of partnership
Women have said ‘oh, it’s really good to know that you
are doing something about it’
‘She [the head of midwifery] is
showing her support’
‘People are keen to share their
successes’
‘Powerful to have the support of the
RCM and the RCOG’
‘It feels nice when we work
together‘ ‘Taking part means
more evidence and I think people want to be part of that’

What have we learned so far?
Importance of
units being receptive to
change
Current
environment of unit, their research
capacity and their staffing
structures
Implementing change takes
time
Good feedback
mechanisms
Importance of engagement
local champions – vital for success
Crucial to have
top level support
‘Change is a big thing’

Acknowledgements
• The OASI Care Bundle Quality Improvement Project is hugely grateful to the champions at each of the 16 units, for their hard work and dedication to improving outcomes for women.
• The OASI Care Bundle Project is fully funded by The Health Foundation, UK
• Any questions, please contact: Dr Posy Bidwell, Research Fellow: [email protected]
Alexandra Hellyer, Project Manager: [email protected]