design-specific analysis of flexor tendon ruptures after volar plating of the distal radius...
TRANSCRIPT

Design-specific analysis of flexor tendon ruptures after volar plating of the distal radius
Maximillian Soong, MD
Gavin Bishop, MD
Lahey Clinic Orthopaedic Surgery

Disclosures
None of the authors have any financial relationship with any of the implant manufacturers mentioned in this presentation.

Background
Flexor tendon rupture from hardware impingement is a potential complication of volar plating of the distal radius.
12% Drobetz, Int Ortho 2003 1% Koval, NEHS 2007
Reported contributing factors:• older-generation non-anatomic plates (pi-plate, T-plate)• distal and/or anterior plate position• plate lift-off from loss of reduction• screwhead prominence
Flexor tendon injuries from specific current-generation anatomic plate designs have been inadequately studied.

Background
The “watershed line”:
“… a transverse ridge located within 2 mm of the joint line on the ulnar side of the radius, and 10-15 mm … on the radial side …”
“Hardware placed distal to the watershed line may come in direct contact with the flexor tendons, resulting in irritation or injury.”
Berglund, JAAOS 2009

Methods
Retrospective review
Inclusion criteria:• all VLP cases from 2005-2008 (n=228)
• three CAQH orthopaedic hand surgeons (n=218)• Acumed Acu-Loc plate (n=208)
Cases involving flexor tendon rupture were identified and analyzed by radiographs and operative notes.

Results
Five cases of flexor tendon rupture among 208 cases (2.4%).
2 – FPL1 – FDP to the index finger1 – FDP to the long finger1 – FDP and FDS to the index finger
All five underwent hardware removal and tendon reconstruction between 4 to 45 months after initial procedure.

Results
Radiographic analysis of five cases with tendon rupture:
1 – plate anterior/distal to volar rim1 – screwheads prominent1 – screwhead prominent, plate anterior to volar rim2 – plate anterior to volar rim
Review of the remaining cases showed that the typical position of this plate is anterior to the volar rim (thus, at the watershed line).

plate distal/anterior to volar rim
screwheads prominent
screwhead prominent, plate anterior to volar rim
plate anterior to volar rim
plate anterior to volar rim
Discussion
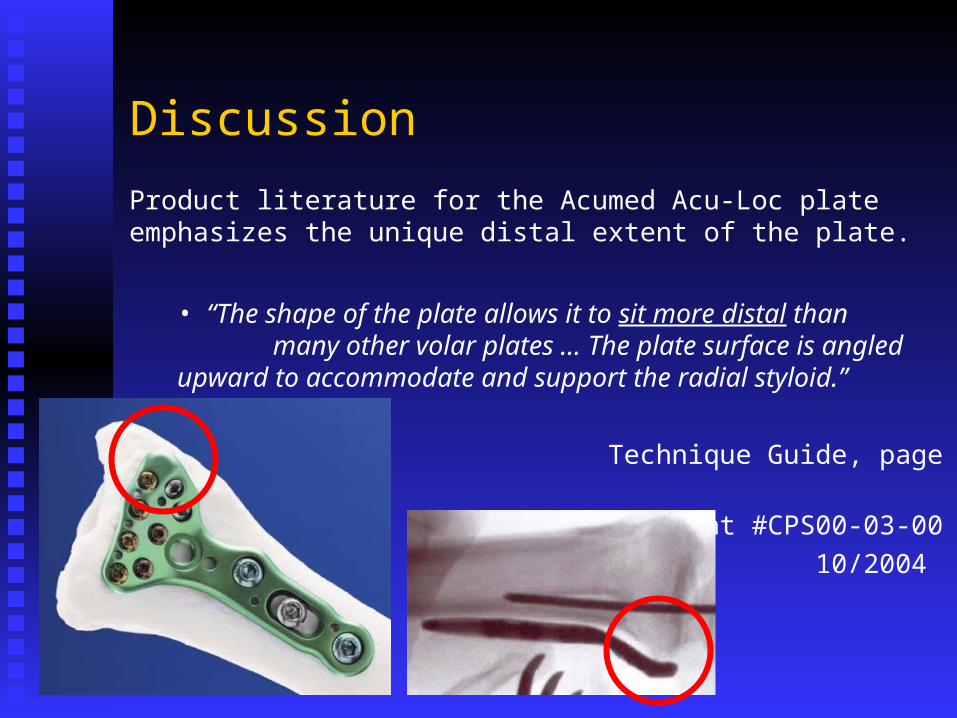
Product literature for the Acumed Acu-Loc plate emphasizes the unique distal extent of the plate.
• “The shape of the plate allows it to sit more distal thanmany other volar plates … The plate
surface is angled upward to accommodate and support the radial styloid.”
Technique Guide, page 6Document #CPS00-03-
00 10/2004

Discussion
A recent cadaver study of several different plate designs has confirmed that the Acumed Acu-Loc plate is uniquely prominent at the watershed line.
• “The Acumed plate fit best [when positioned] at the watershed line, which pushes the theoretical limit set by the surrounding soft tissues.”
Buzzell, JHS 2008

Discussion
A recent clinical study reported five cases of FPL rupture in 201 procedures involving the Acumed Acu-Loc plate (2.5%).
2 – plate distal to volar rim1 – screwheads prominent2 – “not seated properly”
FPL ruptures with other plates in same series:2 of 80 (2.5%) Synthes LCP0 of 40 (0.0%) Hand Innovations (Depuy)
Casaletto, JHS(B) 2009

Discussion
A clinical series using a plate with a low distal profile has shown that flexor tendon rupture can be avoided.
• 87 patients, Hand Innovations (DePuy) plate• no ruptures
Chung, JBJS 2006
DePuyAcumed

Four current volar plate designs (all LEFT radius):the Acumed plate extends beyond the watershed line radially
Acumed Medartis TornierDePuy

Conclusions
Flexor tendon rupture after volar plating of the distal radius is an infrequent complication.
The Acumed Acu-Loc plate may be overly prominent at the watershed line, which may contribute to flexor tendon rupture, and thus future versions of this plate will address this issue.*
Regardless of plate selection, care must be taken to avoid distal and/or anterior position, plate lift-off, and screwhead prominence.