demonstration of intravascular haemo- by means of …
TRANSCRIPT

J. clin. Path. (1958), 11, 206.
THE DEMONSTRATION OF INTRAVASCULAR HAEMO-
LYSIS BY MEANS OF SERUM PAPER ELECTROPHORESISAND A MODIFICATION OF SCHUMM'S REACTION
BY
F. C. NEALE, G. M. ABER, AND B. E. NORTHAMFrom the Departments of Biochemistry and Clinical Pathology, Queen Elizabeth Hospital, Birmingham,
and the Department of Biochemistry, General Hospital, Birmingham
(RECEIVED FOR PUBLICATION OCTOBER 10, 1957)
In studying the pathogenesis of anaemia asso-ciated with many clinical disorders one is oftenconfronted with the problem of whether intra-vascular haemolysis is taking place. Haemolysismay result either from an intrinsic abnormality ofthe red cell, rendering it of shorter life span thannormal, and this may be of an hereditary oracquired nature, or, alternatively, from thepresence of some plasma factor capable ofinducing lysis.Plasma factors producing lysis result from cer-
tain types of poisoning, toxic effects of drugs, andmany generalized infections. Haemolysis mayalso occur as a result of renal or hepatic failureand in other metabolic disorders. The exactmechanism of the haemolysis in these conditions,although unknown, is probably also attributableto plasma factors. Despite the wide range ofknown causative factors many cases of haemolysisremain unclassified, e.g., those which are seen inthe reticuloses and other neoplastic states.
In patients manifesting an extreme degree ofhaemolysis, extracorpuscular haemoglobin can beseen in the serum, which, if in sufficient concen-tration, is excreted into the urine. More com-monly an increased rate of haemolysis is manifestby a raised serum bilirubin level and an increasedexcretion of urobilinogen in the urine and faeces.Reticulocytosis, if present in such circumstances,reflects a compensatory hyperplasia of the bonemarrow, but both these latter diagnostic featuresmay be partially obscured should the rate of bili-rubin production be matched by the ability of theliver to excrete it, or should some complicatingfactor, such as uraemia or chronic infection,simultaneously depress erythropoietic activity.Under these conditions even moderate haemolysismay escape detection by existing routine labor-atory procedures, and in the present work twonew complementary techniques are described
which appear to be more sensitive than othersimple procedures, and can demonstrate thathaemolysis is occurring or has recently taken place.These tests depend on showing an altered patternof haemoglobin attachment to the serum proteins.One technique employs paper electrophoresis ofserum with subsequent differential staining of thestrips to show the position of the protein bandsrelative to the haemoglobin pigments, and theother technique is based on a variation of theSchumm haemochromogen reaction (Schumm,1912), in which the haemoglobin itself is involved.The Schumm reaction, as normally performed,
allows detection of methaemalbumin in muchlower concentration than is possible by directspectroscopic examination (Fairley, 1941). Thepresence of methaemalbumin in serum is indica-tive of intravascular haemolysis, of which theoccasional occurrence in pernicious anaemiaargues for a significant haemolytic component inthat disease. The common finding of raised serumbilirubin levels in patients with the disease pointsto a similar conclusion, and it appeared possiblethat closer examination of such sera and speci-mens from other patients in whom haemolysis wasoccurring or suspected might yield informationconcerning the severity of the haemolytic process,and its response to therapy in relation to thepatients' haematological and clinical progress.
Clinical MaterialCases studied included 10 cases of untreated
pernicious anaemia, five cases of untreatedmegaloblastic anaemia associated with folic aciddeficiency, nine cases of haemolytic anaemia ofvarying aetiology, three patients with evidence ofminor blood transfusion reaction, and three casesof uraemia associated with anaemia in whichhaemolysis was suspected. In addition, tests were
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

INTRAVASCULAR HAEMOLYSIS
performed on 18 patients with various pathologicalconditions, with or without anaemia, but in whomno haemolytic component was suspected. A con-trol group of 30 sera from healthy individuals wasalso similarly investigated. As the underlyingmechanism of the reaction became clearer anattempt was made to characterize further theimplicated proteins. Tests were made involvingurinary proteins from patients with nephrosis anda serum albumin fraction as supplied for trans-fusion purposes by the Lister Institute.
ExperimentalPreparation of Haemoglobin Solution.-A stock
solution of haemoglobin was obtained by lysing aknown volume of washed normal red cells with anequal volume of distilled water followed by freezingand thawing to give an approximate concentration of15 g. haemoglobin/ 100 ml. representing a dilution ofI in 2. This solution may be preserved in the frozenstate for several weeks.
Addition of Haemoglobin Solution to Test Serum.-Haemoglobin concentrations of approximately 0.3,0.6, and 1.2 mg./ml. serum were obtained by the addi-tion of 1 ml. test serum to 0.002, 0.004, and 0.008 ml.of the stock haemoglobin solution. This gives haemo-globin dilutions in serum equivalent to 1 in 1,000, 1 in500. and 1 in 250 of the concentration normallypresent in packed red cells. A further 1 ml. serumwas placed in a fourth tube to which no haemoglobinwas added.Although with practice these volumes were found
to be adequate for spectroscopic examination in aHartridge reversion spectroscope, double quantitiesare more convenient if the specimen permits.
Paper Electrophoresis of Test Serum.-Samples ofeach of the above sera, with and without addedhaemoglobin, after standing for 30 minutes at roomtemperature were subjected to electrophoretic separa-tion on filter paper. Most separations were carriedout on an apparatus of the " hanging-strip " type(Neale, 1955) using 0.05 ml. serum on WhatmanNo. 100 filter paper. The remainder were performedon an E.E.L. horizontal type apparatus using 0.02 ml.serum on Whatman No. 3MM paper. All separa-tions were allowed to run for 16 to 18 hours at roomtemperature. Barbitone buffers of pH 8.6 were em-ployed, as described by Durrum (1950) for thehanging type apparatus, and according to the formulain the manufacturer's handbook for the E.E.L. appar-atus (30 g. sodium barbitone, 19.5 g. CH3COONa.3H20, 205 ml. 0.1 N HCI, made up to 3 litres withdistilled water). After electrophoresis the strips weredried at 100' C. and then cut longitudinally into twoequal parts, one half stained for proteins withbromphenol blue and the other half retained for sub-sequent spraying with benzidine reagent to show thepositions of haemoglobin or haem-containing pig-ments relative to the protein fractions.
Preparation of Haematin Solutions.-Haemin wasprepared from human red cells according to themethod described by Gattermann (1941). A solutionof alkaline haematin was prepared freshly as required,by dissolving 10 mg. of this material in 10 ml. N/10NaOH and diluting to 100 ml. with water as soon assolution was achieved. Portions of this dilute solution(0.1 mg./ml.) were added to 2 ml. portions of serum,giving final concentrations up to 10 jug. haematin/ml.serum. Electrophoresis of these mixtures was carriedout as described above.
Benzidine Reagent.-This was prepared by adding1 ml. of 20 volumes hydrogen peroxide to 30 ml. of asaturated solution of benzidine (extra pure for bloodtesting, B.D.H.) in glacial acetic acid. This ratio ofperoxide to benzidine was found to give optimumsensitivity with minimal background discoloration.The mixed reagent was applied without delay to thehalf-strips by means of an all-glass spray, when anintense blue colour developed within a few seconds inthe presence of haemoglobin or its haem-containingderivatives. This blue colour changes over the next fewminutes to a blue-black, and the background, initiallywhite, becomes light brownish-yellow. If a permanentrecord is desired the strip should be photographedas soon as possible after staining. In place of benzi-dine, which is now becoming difficult to obtain in ahighly purified state because of its reported carcino-genic properties, o-tolidine may be used. The reagentprepared as described by Kohn and O'Kelly (1955),namely equal parts of a 4% ethanolic solution ofo-tolidine, glacial acetic acid, and water, to which isadded a J volume of 20 volumes hydrogen peroxide,gives results similar to the benzidine spray, but thecolour fades rather more quickly.Schumm Reaction.- After samples have been
removed for electrophoresis the four sera werecovered with a layer of ether and 0.1 ml. AnalaRammonium sulphide added to each as recommendedby Fairley (1941). They were then examined in aHartridge reversion spectroscope. In the presence ofmethaemalbumin a positive Schumm test is indicatedby the appearance of a sharp band at 558 in/A; aweaker band at 530 m,u may also be seen. However,when haemoglobin is involved in the production ofthe haemochromogen the 558 ml, band only is seen.
Procedure for Urine.-Haemoglobin dilutions of1 in 4,000, 1 in 2,000, 1 in 1,000, and 1 in 500 in urinewere made and 0.2 ml. samples taken for electro-phoresis; otherwise procedures were as for serum.
ResultsElectrophoretic Behaviour of Haemoglobin and
Haematin in Normal Sera.-In the absence of anyslight haemolysis introduced during the taking ofthe blood or separation from the cells, normalserum is spectroscopically clear and no blue colourappears on spraying the electrophoretic strip withbenzidine reagent. However, such slight haemo-
207
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

F. C. NEALE, G. M. ABER, and B. E. NORTHAM
Pi #z Pr- B z Pr Bz Pt B..
.0*0
Albtumin
No addition 0.3 nag. Hb ml. 0.6 mg. Hb m. .2 mlg. t-i b
FIG. 1.-Electrophoretic results after the addition of haemoglobin to normal serum. Hb is carried by haptoglobinto a concentration of 0.6 mg./ml. Increasing this to 1.2 mg./ml. causes " overflow " into the ,B globulin and thealbumin, and a trail is also left. Pr=protein stain. Bz =benzidine stain.
lysis is not always possible to avoid, even when theutmost care is taken, viz., permitting the blood toflow freely through a large needle (18 s.w.g.) with-out the use of a syringe, and allowing an adequatetime for good clot retraction. When sufficienthaemolysis occurs to permit the alpha band ofoxyhaemoglobin to be just discernible spectro-scopically in a 16 mm. test-tube, then the sprayedstrip develops a diffuse blue band between thea2 and ,B globulins. Occasionally this ratherfaint band is seen directly in line with the a2fraction. On deliberately adding the two lowerhaemoglobin concentrations defined above to mostnormal sera a progressive intensification of thisdiffuse band is seen. When the highest concen-tration, 1 in 250, is reached, however, this benzi-dine-staining band is seen to have two components,one in a position similar to the above, and theother, a slower moving band, corresponds to thefaster moving ,B globulin fraction. At this con-centration, too, a third though much less intenseband may also be seen opposite the albumin anda diffuse trail of haemoglobin becomes apparentbehind the / globulins extending back to theorigin (Fig. 1). This composite pattern appearsto reflect the over-saturation of the haemoglobin-carrying mechanism of normal serum, but incertain of the control sera, where the a2 globulinappeared unusually high, separation into twobands did not occur but a further intensificationof the single band was seen. On the other hand,in a few instances the appearance of a /3 globulinband began at a dilution of 1 in 500, althoughthese were comparatively rare occasions.
Paper electrophoresis of haemoglobin solutionsin saline at similar concentrations exhibited only
a trail, quite dissimilar to the discrete bandsobtained in the presence of serum. Coating thefilter paper with protein by pre-running serum oran albumin transfusion preparation before apply-ing the haemoglobin solutions did not materiallyalter this trail and did not produce the character-istic pattern seen when haemoglobin and serumare mixed before electrophoresis. The absence ofthis trail must indicate a firm combination withprotein fractions which protects the haemoglobinfrom adsorption on to the paper (Fig. 2).The binding of haematin to serum proteins was
similarly studied, and it was found to be carriedalmost equally by the albumin and the leading/3 globulin fractions (Fig. 3). A similar result wasreported by Fiser-Herman and Davorin (1953)with haematin prepared by alkali denaturation ofhaemoglobin, although they found haematin pre-pared from haemin was bound to a2 globulin.Serum to which haematin had been added showedan absorption band at 624 mu when examined inthe spectroscope.Schumm Reaction Applied to Normal Serum.-
Schumm (1912) considered his test to identifyhaematin, but Fairley (1941) interpreted a positiveSchumm reaction as indicative of methaem-albumin in the serum under examination. Innon-haemolysed normal serum no absorptionbands are seen following this reaction, whereasin sera to which small additions of haemoglobinhave been made (dilutions of 1 in 1,000 and 1 in500) the broad but rather faint band of reducedhaemoglobin can be seen. This reverts to thedouble-banded oxyhaemoglobin spectrum on
gently shaking with air, but the reduced spectrumreturns on further standing. At the highest con-
208
I
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

INTRAVASCULAR HAEMOLYSIS
0.3 0.6 1.2mg. Hb'mI.
Untreated Paper
2.4 0.3 0.6 1.2 2.4mg. Hb ml.
Paper Pre-run with "Albumin"
FIG. 2.-Electrophoresis of haemoglobin on albumin-coated and untreated paper. In the concen-trations used Hb is clearly visible only after benzidine spraying and does not form a discreteband but is adsorbed on to filter paper whether or not this has been first " carpeted" with albumin.
Pr Bz Pr Bz Pr Bz Pr Bz
_ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.;....V
3.0
Albumin
No addition 2g. Haematin 4 tLg. Haematin Haematml. ml. ml.
Serum
FIG. 3.-Electrophoresis of normal serum to which haematin has been added. Haematin is taken up by bothalbumin and , globulin. A small quantity of haemoglobin is present in this serum and migrates withthe haptoglobin.
centration (1.2 mg. /ml.) of haemoglobin this bandmay merely be intensified, but in some sera a newsharper and denser band at 558 m,u slowly appearsthrough the centre of the reduced haemoglobin.More occasionally this band has been observed atthe next lower concentration also, viz., 0.6 mg. /ml. Reversion to the oxyhaemoglobin spectrumtakes place on shaking in this case too, but ulti-mately a stage is reached when the 558 m,u bandis permanent and irreversible.Although this band appears at the same wave-
length as in the classical Schumm reaction, it does
not seem to represent the same haemochromogenbecause its reversible replacement by the oxy-haemoglobin spectrum shows clearly that itsorigin is not methaemalbumin, but that it derivesindirectly from haemoglobin. The production ofmethaemalbumin by the incubation of haemo-globin with serum for two days was reportedby Fairley and Bromfield (1937), but the haemo-chromogen now described appears within minutesand under entirely different conditions. Theauthentic Schumm reaction given by serum towhich haematin has been added in vitro differs
209
jil
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

F. C. NEALE, G. Al. AB ER, and B. E. NORTHAM
also by appearing even more promptly and givingtwo absorption bands. These bands can also becaused to fade and reappear for a time byshaking, but no alternative bands take their place.The limiting concentration of haematin in serumthat could be detected by paper electrophoresis,which required only 0.02-0.05 ml. serum, was1 jig. per ml. By Schumm's test when viewed in a16 mm. test-tube, which needs at least 1 ml. serum,it was 2 ug. per ml. Thus, not only has theelectrophoretic technique about twice the ultimatesensitivity of spectroscopy but it will also givereliable results with a very much smaller speci-men.
Electrophoretic Behaviour of Haemoglobin andHaematin in Sera from Patients with Haemo-lysis.-Haemolysis may present as an acute severeepisode or may exist in a milder and chronicform upon which a more severe phase may besuperimposed. Differing electrophoretic patternsreflect these varying degrees of lysis. In patientsexperiencing an acute haemolytic crisis a largequantity of methaemalbumin is usually identifiabledirectly by its absorption band at 624 m,u andthese sera may also contain free haemoglobin invarying amount. The urine may contain haemo-globin and methaemoglobin if the threshold levelis exceeded. Such urines on electrophoresis maybe found to contain other serum protein fractionswhose disappearance coincides with that of thehaemoglobin pigments. Their presence indeedmay be due to competition for reabsorption bythe latter in the tubules (cf. Hardwicke and
Pr Bz Pr Bz
.0_V%0
Albumin
Squire, 1955) rather than the result of any tran-sient kidney damage. In one such case of parox-ysmal cold haemolysis this cycle could be pro-voked at will by immersing the patient's feet andlegs in cold water for a short period. Urines ofthis type show a strongly positive benzidine-staining albumin, but, for reasons discussed later,this alone is not necessarily evidence for thepresence of methaemalbumin although indeed itmay well be present as was claimed by Hensleyand Blackburn (1953). These sera from casesshowing acute haemolysis after electrophoresisand benzidine spraying give an intense bluereaction in the albumin area and there may alsobe a much weaker band on the leading edge of the,B globulins. Behind this latter band a trail ofhaemoglobin may be seen (Fig. 4). If haemno-globin is added in vitro to these sera, the onlyvisible result is that this trail intensifies andspreads forwards as seen when haemoglobin inincreasing concentrations is itself subjected toelectrophoresis (see Fig. 2). In addition to thecase of paroxysmal cold haemoglobinuria men-tioned above, this type of acute phase wasobserved in one patient suffering from acquiredhaemolytic anaemia of the immunological typeand in two patients with pernicious anaemia.
Examination of sera from patients in whomchronic haemolysis of lesser degree has beenoccurring reveals a modification of this pattern, inwhich the benzidine-positive material in thealbumin band is diminished whereas that in the/3 globulin region is increased, and when haemo-
Pr Bz Pr B8
i I
0.3 mg. Hb ml.
Serum0.6 mg. Hb ml.
FIG. 4.-Position, after electrophoresis, of haemoglobin added to serum from a patient with acute haemolysis. In this
case methaemalbumin is found, but neither haptoglobin or Hb-binding globulin is demonstrable, added Hb
combining with the albumin and also leaving a trail.
No addition 1.2 mg, Hb rv-i
210
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

INTRA VASCULAR HAEMOLYSIS
globin is added to these sera this difference isfurther emphasized. Simultaneously the stainingintensity of albumin, f? globulin, and the haemo-globin trail is increased (Fig. 5a). In some cases,where haemolysis introduced during the collectionof the specimen is minimal, the pattern afterelectrophoresis is normal, and it is not until thefirst haemoglobin addition is made that an
abnormal picture appears (Fig. Sb). Examples ofthis type have occurred in cases of familialacholuric jaundice, mild transfusion reaction,acquired haemolytic anaemias of various types,including those associated with the collagen dis-orders and the reticuloses, anaemias associatedwith the uraemic state, as well as in perniciousanaemia and megaloblastic anaemias associated
Pr Bz Pr Bz Pr Bz
-- 0.3 mg. Hb ml. -0.6 mg. Hb ml. -1.2 mg. Hb ml.Serum
FIG. 5 (a).-Mode of attachment of added haemoglobin to sera from patients with chronic haemolysis. No hapto-globin is seen in this serum, haemoglobin being bound only to ,9 globulin and albumin.
Pr Bz Pr Bz Pr Bz Pr Bz
In
.0
0
a2.,
a,
Albumin
No addition 0.3 mg. Hb'ml. -0.6 mg. Hb ml. -1.2 mg. Hb ml.
SerumFIG. 5 (b).-A minimal quantity of haptoglobin is present in this serum: added haemoglobin is attached only
to P globulin and albumin.
x
Pr Bz
7
@_ 9.00
a.,
a1
Albumin
No addition
211
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

F. C. NEALE, G. M. ABER, and B. E. NORTHAM
P B z Pr Bz
.
.0
Al&bu mi n
NoC addition Haematin
Set-rJm pre-treatment
No addition H ae n-a t
Sertum ninth day of treatmen
FIG. 6.-Return of haematin-binding ,B globulin to serum of patient with pernicious anaemia nine days after the
start of vitamin B12 therapy. The serum, taken initially during an acute haemolytic phase, shows a very strong
methaemalbumin band, but will not accept haematin into the S globulins. On the ninth day of treatment
methaemalbumin has disappeared, a little haemoglobin is present, and is seen to be bound to both haptoglobinand , globulin. Added haematin is now accepted by ,B globulins as well as by albumin.
with folic acid deficiency. In many of theseinstances routine laboratory procedures hadfailed to demonstrate any evidence of an activehaemolytic process. In addition to these patho-logical conditions, similar results were seen whencord blood was examined, reflecting the physio-logical haemolysis of the newborn.The acceptance of haematin by sera of these
groups also differs according to the severity of theattack. Its pattern of attachment to the albuminand globulin fractions parallels their ability tobind haemoglobin; thus in the most severe cases,
where both the a!2 and /8 globulin binding fractionhad disappeared, the addition of haematin resultedin uptake by the albumin alone. This points tothe probability of common binding sites in bothalbumin and 8 globulin for haematin and haemo-globin (Fig. 6). By following the progress ofpatients with pernicious anaemia under treatmentwith vitamin B12 the simultaneous return of theability of the globulin to bind both haematinand haemoglobin has been seen.
Schumm Reaction Applied to Sera fromPatients with Haemolysis.-The character of theSchumm reaction in these sera was found to bedependent on the presence of methaemalbuminor quite small amounts of haemoglobin. If theformer were present the haemochromogen spec-trum described by Schumm (1912) and later byFairley (1941) was at once obtained. However, in
many cases where haemolysis was suspected thisreaction was negative, and it was only afterdeliberately adding haemoglobin that a haemo-chromagen band appeared, although rather more
slowly, a band at 558 mju gradually replacingthe reduced haemoglobin spectrum. This reactionhas already been described as occurring in normalserum containing the higher haemoglobin concen-
trations, but in these abnormal sera the lowest con-
centration will invariably bring it about. At a
haemoglobin dilution of 1 in 500 the band inten-sifies, but at 1 in 250, although still darker, itsdemarcation is a little less precise due to the broadabsorption band of reduced haemoglobin withwhich its edges merge.
Influence of Therapy on Haemoglobin Distri-bution in Serum.-In order to follow the returnto normal of the electrophoretic behaviour andSchumm reaction, a study of the influence oftherapy with vitamin B12 in patients sufferingfrom pernicious anaemia was chosen, as in thiscondition a good response to therapy could beconfidently anticipated. For the same reason thzprogress of another group of patients with non-
Addisonian megaloblastic anaemia responding tofolic acid therapy was also followed. Both testshad always been found to be either normal or
abnormal for any given serum, and furtherevidence that both were related to one common
mechanism in haemoglobin carriage arose from
P- Bz Pr BZ.
I; I.,0..
212
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

INTRAVASCULAR HAEMOLYSIS
the simultaneous changes they underwent inresponse to therapy. This sequence of changemay be illustrated by reference to the followingcase.
D. A., a woman aged 56, was admitted to hospitalas a medical emergency. She had a slight icterus,severe anaemia, and was mentally confused. Apartfrom a systolic cardiac murmur, slight ankle oedema,and the spleen being just palpable, there was no othernoteworthy clinical finding.Blood examination showed severe macrocytic
anaemia: Hb 36% (5.3 g.%), R.B.C.s 1.03 m. perc.mm., P.C.V. 12%, M.C.V. 116 c,u, reticulocytes4.8%. Blood films showed features consistent with adiagnosis of pernicious anaemia. The bone marrowwas megaloblastic and there was histamine-fastachlorhydria. The indirect van den Bergh reactionwas positive, serum bilirubin was 2.4 mg./100 ml.,Schumm's test was positive; fasting serum iron182 ,ug./100 ml. and iron-binding capacity 230 ulg./100 ml. Osmotic and mechanical fragility tests onthe red cells were within normal limits and the directCoombs test was negative.Treatment with daily intramuscular injections of
100 jug. vitamin B12 was instituted, and within twodays there was striking clinical improvement. Bio-chemically the first change noted was a sharp fall inserum iron to 20 Mg./100 ml. 48 hours after treatmentwas started (Hawkins, 1955). On the fifth day oftreatment the serum bilirubin had fallen to 0.5 mg./100 ml., reticulocytes had risen to 28.5%. On theseventh day the Schumm test was negative.
Studies of the electrophoretic pattern during therecovery phase revealed a gradual loss of benzidine-
Pr Bz Pr Bz
7
.0
a2
Albumi'n
staining pigments in the albumin region and these hadentirely disappeared by the seventh day, the same dayas the Schumm test became negative. After haemo-globin addition the band in the , globulin regiongradually became more intense, but there was no up-take of haemoglobin in the a2 globulin area until theninth day of treatment, and even then the ability ofthis fraction of the a2 globulin to carry haemoglobinwas far from normal, and remained so until theeleventh day of treatment (Fig. 7).
The absence of any haemoglobin binding in thea2 and the minimal uptake in the /8 globulinregion suggest that in this patient haemolysis hadplayed a major-role in the production of such asevere degree of anaemia. The initially high con-centration of benzidine-staining compound in thealbumin fraction was almost certainly due to thepresence of methaemalbumin, although afterhaemoglobin additions some of this could havebeen accounted for by the haemoglobin. Thesimultaneous return of the Schumm test to normaland the disappearance of this albumin band in theserum after electrophoresis is very much in favourof this hypothesis. The fact that the test withammoniunm sulphide after the addition of haemo-globin in vitro remained positive so long as therewas any acceptance in the /B region is stronglysuggestive that it is the presence of this/8-globulin-haemoglobin compound which isresponsible for the formation of the haemo-chromogen.
Pr Bz Pr Bz Pr Bz
Pre-treatment 3rd day Sth day 7th day 11th dayDuring Treatment
Serum
FIG. 7.-Characteristic changes found on electrophoresis of serum from a patient with pernicious anaemia undergoingtreatment with vitamin B12. Methaemalbumin disappears by the seventh day and haptoglobin reappears by theeleventh day.
213
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

F. C. NEALE, G. M. ABER, and B. E. NORTHAM
A similar sequence of changes was noted in allthe 10 cases of pernicious anaemia successfullytreated with vitamin B12, although with oneexception they showed features of a more chronicrather than an acute haemolytic process.
Identical patterns were also seen in threepatients in whom acute intravascular haemolysishad occurred, but who recovered either spon-taneously or as a result of therapy, and four casesof acholuric jaundice subjected to splenectomyrecovered their normal 'haemoglobin-proteinattachments within seven to 10 days after theoperation. In one patient suffering from a chronichaemolytic anaemia of unknown aetiology, splen-ectomy was undertaken after all other forms oftherapy had failed to influence the anaemia. Oneweek after this operation his serum, after addingto it haemoglobin in vitro, gave normal electro-phoretic and chemical reactions, but after anotherweek, however, he again showed the pre-operativebiochemical abnormalities and a haematologicalrelapse.
In all these patients a constant sequence ofevents was observed. The benzidine-stainingmaterial gradually disappeared from the albumin,and that in the /8 position increased until finallyhaemoglobin attachment to the a2 fraction wasdetected. This then increased at the expense ofthe /3-bound component until eventually only thesera containing the higher concentrations ofhaemoglobin, i.e., 1.2 and 0.6 mg. /ml., showedany staining in the /3 region. The trail of freehaemoglobin gradually diminished as thesechanges in the bound fractions proceeded. Thespeed of return to normal in treated cases ofvitamin B12 and folic acid deficiency anaemiasfavours a central rather than a peripheral haemo-lytic mechanism in these conditions. It appearsthat haemolysis must cease very quickly on institu-tion of therapy, a conclusion supported by the rapidfall in serum iron, certainly sooner than would beanticipated if lysis were to continue till theoriginal peripheral cell population was replacedby normal cells. It seems more probable that thetime required for cessation of haemolysis is of thesame order as that taken for the return to anormoblastic marrow, and this does not seem to becoincidental.
DiscussionAmongst their multiple functions serum pro-
teins have been shown to play a major role in thetransportation of many substances normally foundin human blood. Thus, iron was found to becarried by a 8, globulin (Surgen.or, Koechlin, andStrong, 1949; Holmberg and Laurell, 1947), trans-
port copper is albumin bound (Bearn and Kunkel,1954; Horst, 1954), vitamin B12 was observed tobe combined with a and /8 globulin (Latner andZaki, 1957), and during paper electrophoresis bili-rubin migrates with albumin, to mention but someof the known combinations. It is usually assumedthat these protein carriers merely hand on theirload to the recipient tissues and are then free oncemore for further use; for example, the serumiron-binding capacity is the same before, during,and after an iron absorption test. However, themost likely explanation for the characteristicchanges observed in cases of intravascular haemo-lysis is that liberation of haemoglobin into theplasma in vivo results in a reduction in the quan-tity of those plasma proteins with which it com-bines.
In 1939 Polonowski and Jayle demonstrated thatif a small quantity of haemoglobin were intro-duced intravascularly it appeared to becomeattached to protein(s) in human plasma, theprotein-haemoglobin compound then giving apositive peroxidase reaction. They called this pro-tein haptoglobin and it was later found (Jayle andAbdellatif, 1946) to have a high carbohydrate con-tent. Attention was drawn more recently to theerror that it introduced into analysis of electro-phoretic strips of haemolysed sera because of theretarding effect that haemoglobin has on a2globulin, resulting in an apparent increase in /8globulin at the expense of the a2 globulin (Wieme,1953, 1954; Tuttle, 1955). The former authordescribed how with increasing deliberate additionsof haemoglobin first one then two bands appeared,but these were visible to the eye and were pro-duced by far greater amounts (additions of 4 to 40mg./ml. serum) than have been used here. Thesetwo bands probably represented a2 globulinuptake (the haptoglobin of Jayle) and free-movinghaemoglobin, but the amount added was too greatto have been of value in discriminating betweensera from normal individuals and those under-going haemolysis.
If the primary haemoglobin carrier is thehaptoglobin fraction in the a2 globulins, as sug-gested by Jayle and Boussier (1955), any conditionwhich caused an increase in the a2 globulins mightalso increase the ability of the serum to bindhaemoglobin. Their investigations of sera frompatients suffering from acute and chronic infec-tions, malignancy, and disorders in which severe
tissue damage occurs and which characteristicallyexhibit a rise in a2 globulin, showed that these sera
also accept larger quantities of haemoglobin inthat fraction than do sera from normal persons.
214
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

INTRAVASCULAR HAEMOLYSIS
Pr Bz Pr Hz Pr Bz Pr Bz
No addition --0.3 mg. Hb ml. C.6 mg. Hb ml.
Albumin Preparation-- 1.2 mg. Hb ml.
FIG. 8.-Addition of haemoglobin to albumin transfusion preparation, showing presence of an a2-globulin bindingfraction. Haemoglobin is attachedialso to albumnin, but does not combine with the j8 globulin in this preparation.
From our own results with normal sera it appearsthat in different individuals there is sufficienthaptoglobin to combine with haemoglobin concen-tration ranging from about 0.3 to 1.2 mg./ml. Insome control sera where the a2 globulin concen-tration was unusually high, 2.4 mg./ml. haemo-globin was found insufficient to form more thanone electrophoretic band. The high a2 globulinconcentration which occurs in the nephrotic syn-drome did not saturate till even more haemoglobinhad been added. Conversely when the concentra-tion of a,2 globulin is decreased, acceptance ofsmaller than normal quantities of haemoglobinshould be demonstrable, and in the control groupone individual was found whose haptoglobin wasbarely able to carry a concentration of 0.3 mg./ml.Once the haptoglobin has been saturated,
electrophoresis shows another slightly slower-moving band caused by secondary acceptance bya /B globulin fraction. This can be shown to bea 8,3 globulin by performing the electrophoresis ina buffer containing 20 mg./100 ml. calcium ion,which was shown by Laurell, Laurell, and Skoog(1956) to retard the /3 lipoprotein and resolve the,8 globulins into two bands. The usual E.E.L. bufferwas employed to which calcium chloride had beenadded to a concentration of M /200. In anattempt to characterize this fraction further,experiments were carried out with a sample ofpure iron-free transferrin,* but no attachment ofhaematin to this protein was seen. Likewise analbumin transfusion fraction containing /3 globulin
* Obtained through the kindness of Professor Schultze, of theBehringwerke, Marburg, Germany.
which, by its ability to transport 59Fe was shownto include transferrin, did not contain any /8-haemogloban-combining protein (Fig. 8). Therewas, however, evidence of haemoglobin attach-ment to an ill-defined protein of approximately a2
globulin mobility.Haemoglobin forms a complex with /3, globulin
only after saturating the haptoglobin, but inhaemolytic sera this form of attachment is seenwith even the minimal addition of 0.3 mg. /ml. andthis must, therefore, represent a depletion ofhaptoglobin. In one or two instances of verysevere haemolytic activity it has been possible toshow that both the a2 and /8 globulins are incap-able of binding haemoglobin, and this is furtherevidence of the hypothesis that in disposing ofextracorpuscular haemoglobin the protein attachedto it is compulsorily sacrificed, the /3-binding com-
ponent also having been lost. A similar con-
clusion is reached with regard to haptoglobin lyNyman (1957) and Laurell and Nyman (1957), whorecently found, using a paper electrophoresis tech-nique similar to our own, that it is absent from serain cases of pernicious anaemia and returns on treat-ment with vitamin B12' Their conditions ofelectrophoresis, however, may have caused an
overlap of free-moving haemoglobin and the,8 globulins, which could explain how the haemo-globin complex with this fraction has escapednotice. The same may well hold for the reportby Liang (1957) that human serum containinghaemoglobin exhibits but three bands afterelectrophoresis, namely, albumin-haemoglobin,a2 haemoglobin, and free-moving haemoglobin.
.?,globulin
Albumin
I
215
I
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

F. C. NEALE, G. M. ABER, and B. E. NORTHAM
Although no quantitation was attempted in thisseries, there appeared to be reduced amounts ofa2 and ,B globulins even on qualitative inspectionof the strips, but it was impossible to make anysimilar visual assessment of the albumin. It issignificant that Christenson and Dacie (1957) havereported a diminution in these fractions in sera ofpatients who formed warm auto-antibodies.
In the following way it was possible to demon-strate quite clearly that the effects being seen in
(1)Pt BEz Pr- Bz
A.bui
Albumin l *t
Alone
j2)Pr B
Normal Hb Patient's Hb
Normal Serum
these sera were due to a serum protein deficiencyand not to any peculiarity of the patient's haemo-globin. A constant addition of haemoglobin wasmaintained throughout a series which consistedof: (1) normal serum and normal haemoglobin,(2) normal serum and patient's haemoglobin, (3)patient's serum and normal haemoglobin, and (4)patient's serum and patient's haemoglobin.The normal and patient's sera were also
examined without added haemoglobin. Fig. 9
(3)z P- Bz Pr RB
*JIII I 14~~~~~~~~~~~~~~~~~~~~~~~~~
Alone Normal Hb Psati. P-:;' . HO
Patient's Serurr
FiG. 9 (a).-Result of electrophoresis of mixtures of haemoglobin and sera from normal individuals and subjects showing haemolysis.Normal serum shows haptoglobin-haemoglobin complex with either haemoglobin; patient's serum exhibits a small amount ofhaptoglobin-haemoglobin complex and, globulin binding.
PBI )Pr- Bl-2 P r
(2)Pr B7.
I3) w
Pr Bz Pt- B r J.
I
.00
I.
Albumin
Alonrc. No-mal HbNormal Serum
Patient's Hb Alone
FIG. 9 (b).-Normal serum shows haptoglobin-haemoglobin complex, patient's serum is devoid of haptoglobin, but , globulin and albuminbinding is seen, also a haemoglobin trail.
Patient'sHSberur'Y-,'i "& >
Pati ent 's Se rU rl
216
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

INTRA VASCULAR HAEMOLYSIS
shows the result of electrophoresis. Both (1) and(2) gave a normal result and negative haemo-chromogen reaction, whereas (3) and (4) gave an
abnormal result and positive haemochromogenreaction. Fig. 9 also illustrates typical quanti-tative differences that are found in sera from indi-viduals showing evidence of haemolysis. In Fig.9a (3) and (4) is shown haemoglobin attached to
a small amount of haptoglobin, to ,B globulin, anda slight trail unattached to protein. Fig. 9b (3)and (4) shows complete absence of haptoglobinbinding, but strong globulin and slight albuminuptake. The free-moving haemoglobin is clearlyvisible behind the 83-globulin-haemoglobin com-
plex. Other sera of this type were tested andsimilar results obtained. It was also found that ifto a serum which gave such abnormal results an
equal volume of normal serum was added beforethe haemoglobin addition, then the mixturereacted as normal serum. These experiments showclearly that a factor, initially lacking, was suppliedto the abnormal by the normal serum, and thatthere must have been in the latter a sufficientquantity of haptoglobin to prevent the mixturegiving an abnormal reaction.
Reference has already been made to the appear-
ance of a " haemolytic " pattern in a number ofcord bloods taken from normal full-term infants.Tuttle (1955) showed that the sera from newlyborn babies demonstrated a different haemo-globin-carrying mechanism from that observed inthe adult. He found very little haemoglobinattached to the a2 fraction but a considerableamount was taken up in the globulin, and thatthis pattern gradually changed in the first week oflife to that normally found in older subjects. It isalmost certain that what he was studying was theelectrophoretic pattern of increased haemolysiswhich occurs normally in the early days of life,reflecting the shorter life span of red cells con-
taining foetal haemoglobin. A small number ofcord bloods from " Rhesus babies" were alsoexamined and, not surprisingly, showed markedhaemolytic patterns.The Schumm reaction as conventionally
employed depends on the production of a haemo-chromogen from an albumin-haematin complexunder the influence of ammonium sulphide.Haematin is also accepted by globulin, but sinceapparently equally strong, though not preferential,albumin binding always occurs simultaneously inserum, it is not possible on the present evidence tosay what part this globulin takes in the classicalSchumm reaction. The haemochromogen which isdescribed here appears to derive from the /,3 glo-
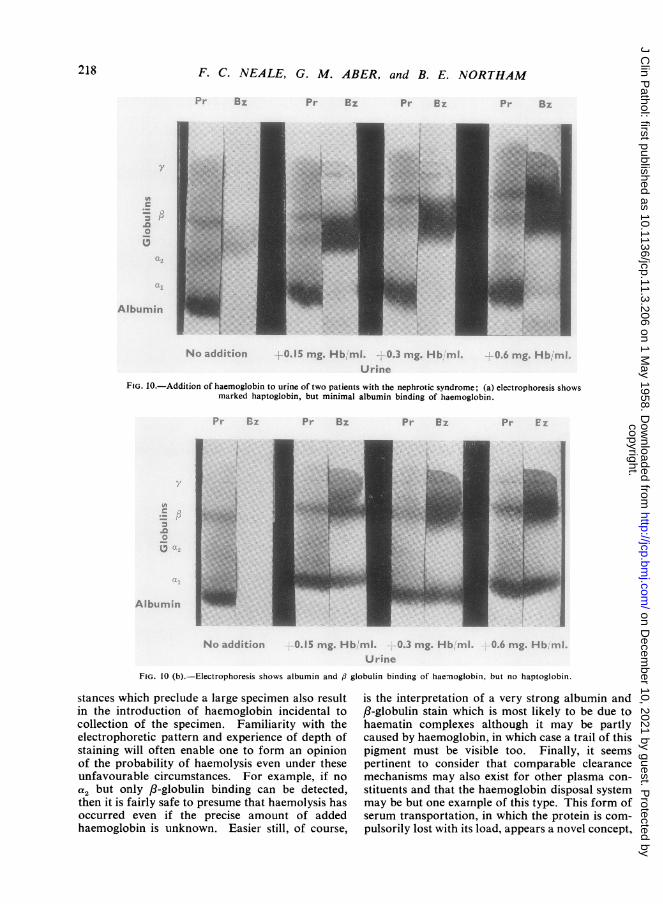
bulin-haemoglobin complex under the samechemical treatment. This becomes apparent oncarrying out both electrophoretic and chemicaltests concurrently on a large number of sera. Thishaemochromogen is produced only when there issufficient haemoglobin to " spill over " into the ,Bglobulins. As long as it is all covered by theprime binding protein, haptoglobin, a spectrum ofreduced haemoglobin only is seen on ammoniumsulphide treatment. Although binding to albuminoccurs to a small degree as the haemoglobin con-centration is increased, this albumin-haemoglobincomplex has probably no part in the haemo-chromogen reaction, for while formation of analbumin complex may be induced in protein-containing urine, no haemochromogen is pro-duced unless there is also a ,B globulin linking pro-tein, and this was found in only two of fournephrotic urines examined (Fig. 10). Jayle andBoussier (1954) found that among 31 nephroticpatients examined only one child excreted a signi-ficant amount of haptoglobin. If large quantitiesof the haptoglobin were lost in this way, falsepositive tests for haemolysis might well complicatethe serum studies on these patients. It appearslikely that many Schumm reactions that have beenreported positive in the past have in fact beencontributed to by the haemochromogen reactionnow described, as most plasmas in acute haemo-lytic crises contain in vivo more than sufficientfree haemoglobin to provoke it. Also a naturallyoccurring mixture of haemoglobin and sulphaemo-globin reacted both electrophoretically and withammonium sulphide exactly as haemoglobin itself.The fate of these various haemoglobin-protein
complexes in the body is not clear, but it appearsreasonable to assume that they are removedcomplete from the blood stream by the reticulo-endothelial system, the haemoglobin broken down,and the associated serum protein lost from thecirculation.The two tests described in this paper are always
found to be complementary, never contradictory.They are positive only if there is insufficient hapto-globin to bind all the haemoglobin present. Inpractice it was found that a concentration of0.3 mg. haemoglobin per ml. serum was critical indifferentiating normal serum from that of patientsexperiencing haemolysis. For routine work whenthere is an adequate sample, the test with ammo-nium sulphide is quicker to carry out than theelectrophoretic technique. When the sample is verysmall it is then often possible to obtain an answerby electrophoresis without further haemoglobinadditions, since it commonly happens that circum-
217
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from
F. C. NEALE, G. M. ABER, and B. E. NORTHAM
B,
N .) -aiddi t ic) r
p*. 8a. Pr 83
0 1S mg- Hb rnl. 0.3 mg. Hb nm' 0.6 rng. HI' r
Urine
FIG. 10.-Addition of haemoglobin to urine of two patients with the nephrotic syndrome; (a) electrophoresis showsmarked haptoglobin, but minimal albumin binding of haemoglobin.
fI Pr- B7 Pr- ez
I
Nc addition 0.15 nig. Hb rmil. 0.3 mg. Hb mj 0 6 mg H ,
Uri ne
FIG. 10 (b).-Electrophoresis shows albumin and ,3 globulin binding of hae-noglobin, but no haptoglobin.
stances which preclude a large specimen also resultin the introduction of haemoglobin incidental tocollection of the specimen. Familiarity with theelectrophoretic pattern and experience of depth ofstaining will often enable one to form an opinionof the probability of haemolysis even under theseunfavourable circumstances. For example, if noa2 but only 8t-globulin binding can be detected,then it is fairly safe to presume that haemolysis hasoccurred even if the precise amount of addedhaemoglobin is unknown. Easier still, of course,
is the interpretation of a very strong albumin andBS-globulin stain which is most likely to be due tohaematin complexes although it may be partlycaused by haemoglobin, in which case a trail of thispigment must be visible too. Finally, it seemspertinent to consider that comparable clearancemechanisms may also exist for other plasma con-
stituents and that the haemoglobin disposal systemmay be but one example of this type. This form ofserum transportation, in which the protein is com-pulsorily lost with its load, appears a novel concept,
Pr 8
U
Albuiminr
I
218
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from

INTRAVASCULAR HAEMOLYSIS
and perhaps applies only where immediate seques-tration of a "foreign " protein is essential, andthere may be a close analogy between this systemand those of the antigen-antibody type. Furtherexamples may be found once the principle is con-ceded, and these will help to decide whether thehaemoglobin interactions are unique or can bebetter classed as a " transport" or as a " defence"system.
SummaryTwo complementary tests are described which
detect intravascular haemolysis and are diagnosticwhen other simple tests are equivocal or evennegative.These two tests, one electrophoretic, the other
purely chemical, are based on a common principle,the mode of haemoglobin attachment to serumprotein. Electrophoretic evidence is presented thathaemoglobin can form complexes not only withhaptoglobin but also with a ,B globulin andalbumin.
Application of the tests to a variety of clinicalconditions involving haemolysis has shown thatdisappearance of haemoglobin from plasma isaccompanied by loss of its carrier proteins. Theimplications of this fact are discussed.
Serial investigation of patients with megalo-blastic anaemia treated with vitamin B12 or folicacid show that haemolysis ceases very soon afterinstitution of therapy and points to a centralrather than a peripheral haemolytic mechanism.
The authors wish to express their gratitude to Dr.J. N. Marshall Chalmers for his interest and en-couragement throughout this work and for hiscriticism of the paper, to Professor J. R. Squire forreading the paper, and to Dr. H. G. Kohler for speci-mens of blood from patients with anaemias ofpregnancy.
AddendumSince submitting this paper for publication,
Allison and ap Rees (1957), using the starch-blockelectrophoretic technique previously employedby Smithies (1955), have described experimentswith serum from normal individuals and frompatients in whom haemolysis had occurred. Theirresults show an acceptance of up to 135 mg.haemoglobin/100 ml. serum in the normal case,but a marked reduction or complete absence ofhaptoglobin in the serum of the patients studied.They concluded, in accord with Laurell andNyman (1957), that both the serum haptoglobinlevel and tubular reabsorption of haemoglobintogether determine the renal threshold for haemo-globin.
REFERENCESAllison, A. C., and Rees, W. ap (1957). Brit. med. J., 2, 1137.Bearn, A. G., and Kunkel, H. G. (1954). Proc. Soc. exp. Biol. (N.Y.),
85,44.Christenson, W. N., and Dacie, J. V. (1957). Brit. J. Haemat., 3, 153.Durrum, E. L. (1950). J. Amer. chem. Soc., 72, 2943.Fairley, N. H. (1941). Quart. J. Med., 34 (n.s. 10), 95.-and Bromfield, R. J. (1937). Trans. roy. Soc. trop. Med. Hyg.,
31, 139.Fiser-Hermai, M., and Davorin, P. (1953). Biochem. Z., 324, 96.Gattermann, L. (1941). Laboratory Methods of Organic Chemistry,
p. 407. Macmillan, London.Ham, T. H. (1939). Arch. intern. Med., 64, 1271.Hardwicke, J., and Squire, J. R. (1955). Clin. Sci., 14, 509.Hawkins, C. F. (1955). Brit. med. J., 1, 383.Hensley, W. J., and Blackburn, C. R. B. (1953). Aust. J. Sci., 16, 64.Holmberg, C. G.,and Laurell, C. B. (1947). Acta chem. scand.,1,944.Horst, W. (1954). Klin. Wschr., 32, 961.Jayle, M. F., and Abdellatif (1946). Bull. Soc. Chim. biol. (Paris),
28, 80.- and Boussier, G. (1954). Ibid., 36, 959.--(1 (1955). Expos. ann. Biochim. med., 16 ser., p. 157.Kohn, J., and O'Kelly, T. (1955). J. clin. Path., 8, 249.Latner, A. L., and Zaki, A. H. (1957). Biochem. J., 66, 54p.Laurell, C. B., and Nyman, M. (1957). Blood, 12, 493.- Laurell, S., and Skoog, N. (1956). Clin. Chem., 2, 99.Liang, C. C. (1957). Biochem. J., 66, 552.Neale, F. C. (1955). J. clin. Path., 8, 334.Nyman, M. (1957). Scand. J. clin. Lab. Invest., 9, 168.Polonowski, M., and Jayle, M. F. (1939). Bull. Soc. Chim. biol.
(Paris), 21, 66.Schumm, 0. (1912). Hoppe-Seyl. Z. physiol. Chem., 80, 1.Smithies, 0. (1955). Biochem. J., 61, 629.Surgenor, D. M., Koechlin, B. A., and Strong, L. E. (1949). J. clin.
Invest., 28, 73.Tuttle, A. H. (1955). Science, 121, 701.Wieme, R. J. (1953). Experientia (Baie!), 9, 380.- (1954). Rev. belge. Path., 23, 321.
219
copyright. on D
ecember 10, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.11.3.206 on 1 May 1958. D
ownloaded from