defining and diagnosing severe asthma-bateman and... · 2015-10-02 · defining and diagnosing...
TRANSCRIPT
Defining and diagnosingsevere asthma
SY9
WAO – WISC2010Dubai December 2010
Eric D. BatemanEric D. BatemanMD, MBChB, FRCP, DCHMD, MBChB, FRCP, DCHProfessor of Respiratory Medicine, University of Cape TownProfessor of Respiratory Medicine, University of Cape TownDirector of University of Cape Town Lung InstituteDirector of University of Cape Town Lung InstituteHead, Division of Head, Division of PulmonologyPulmonology, , Cape TownCape Town

Presenter DisclosuresPresenter DisclosuresEric D Bateman
Lecture Fees: AstraZeneca, Alk Abello, BoehringerIngelheim, Chiesi, GlaxoSmithKline, Nycomed, Pfizer, TEVA
Consultancy or Advisory Boards: Almirall, AlkAbello, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Forest, Hoffmann la Roche, GlaxoSmithKline, Merck, MorriaBiopharmaceuticals, Novartis, Nycomed, Pfizer, ScheringPlough
Industry-sponsored grants (Institution): Aeras, Almirall, Altana, AstraZeneca, Boehringer Ingelheim, Chiesi, Hoffmann la Roche, GlaxoSmithKline, Merck, MorriaBiopharmaceuticals, Novartis, Nycomed, Pfizer.
Learning objectivesLearning objectives
Defining and diagnosing severe asthmaDefining and diagnosing severe asthma
� To review new definitions of severe asthma� WHO� ATS/ERS Task Force on Severity and Control� ATS/ERS Task Force on Severe Asthma
� Consider the clinical implications of these definitions
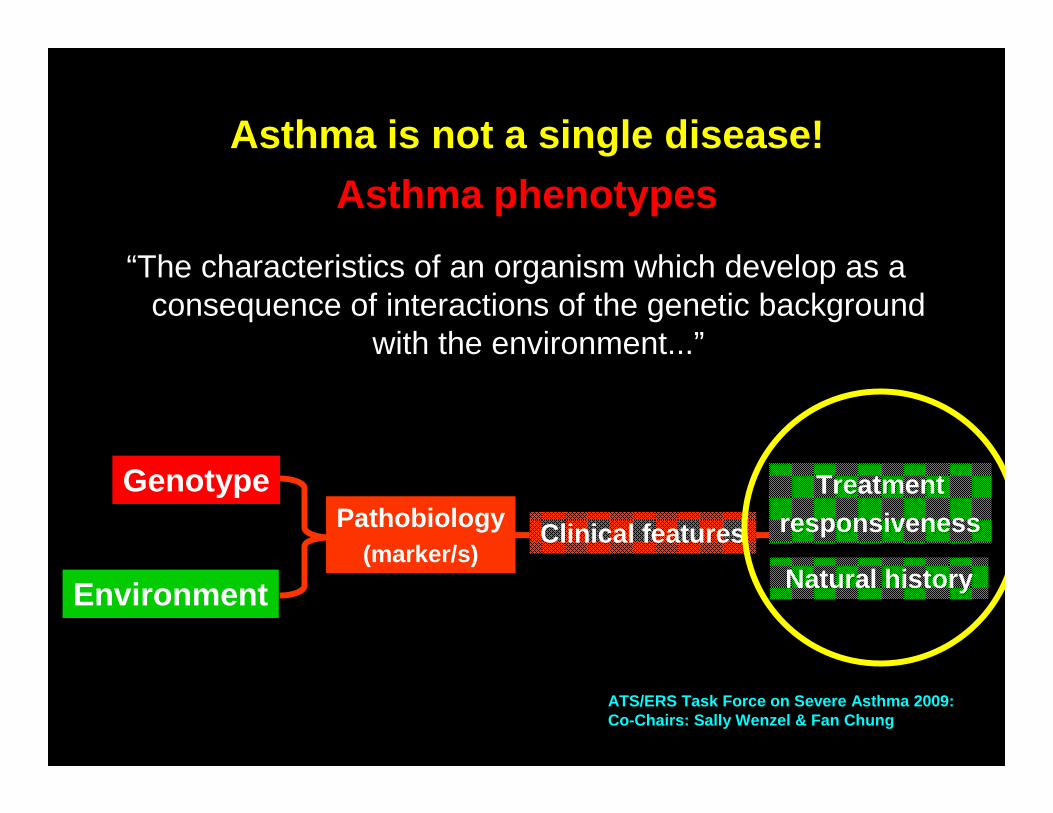
ATS/ERS Task Force on Severe Asthma 2009:Co-Chairs: Sally Wenzel & Fan Chung
Asthma is not a single disease!
Asthma phenotypes
“The characteristics of an organism which develop as a consequence of interactions of the genetic background
with the environment...”
Genotype
Environment
Pathobiology(marker/s)
Clinical features
Treatmentresponsiveness
Natural history
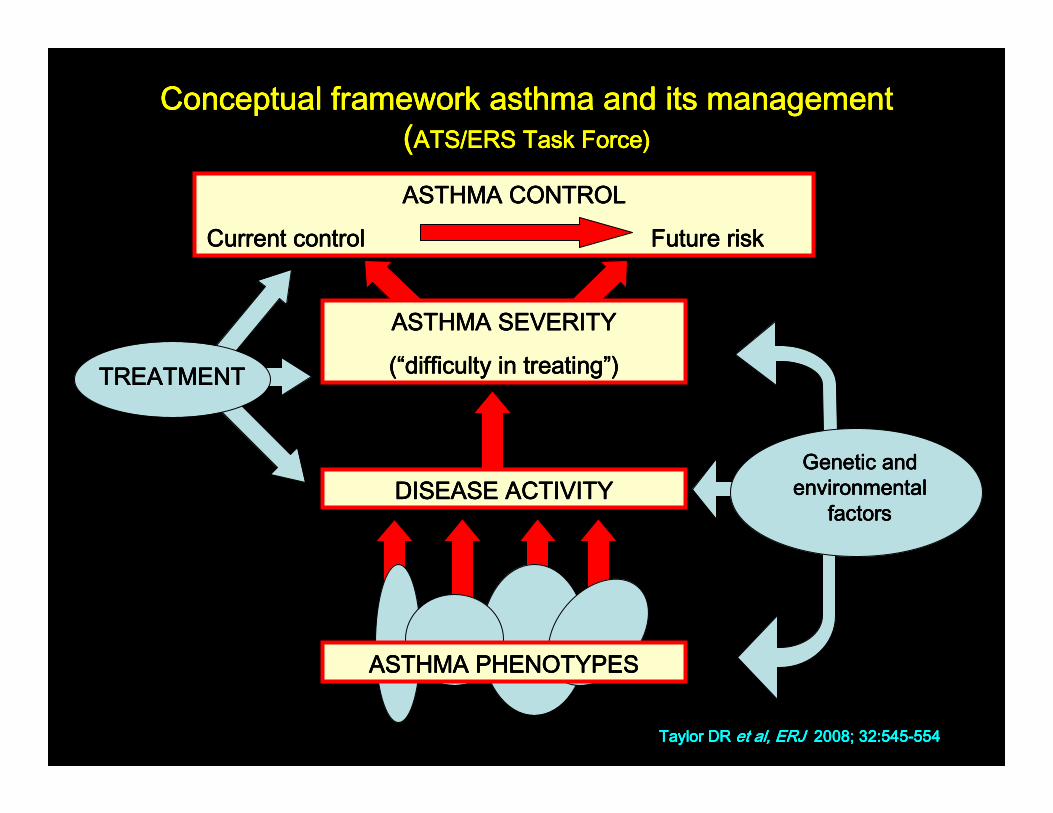
ASTHMA CONTROLASTHMA CONTROLASTHMA CONTROLASTHMA CONTROL
Current controlCurrent controlCurrent controlCurrent control Future riskFuture riskFuture riskFuture risk
ASTHMA SEVERITYASTHMA SEVERITYASTHMA SEVERITYASTHMA SEVERITY
((((““““difficulty in treatingdifficulty in treatingdifficulty in treatingdifficulty in treating””””))))
Genetic and Genetic and Genetic and Genetic and environmental environmental environmental environmental
factorsfactorsfactorsfactors
Conceptual framework asthma and its managementConceptual framework asthma and its managementConceptual framework asthma and its managementConceptual framework asthma and its management((((ATS/ERS Task Force)ATS/ERS Task Force)ATS/ERS Task Force)ATS/ERS Task Force)
TREATMENTTREATMENTTREATMENTTREATMENT
DISEASE ACTIVITYDISEASE ACTIVITYDISEASE ACTIVITYDISEASE ACTIVITY
ASTHMA PHENOTYPESASTHMA PHENOTYPESASTHMA PHENOTYPESASTHMA PHENOTYPES
Taylor DR Taylor DR Taylor DR Taylor DR et al, ERJ et al, ERJ et al, ERJ et al, ERJ 2008; 32:5452008; 32:5452008; 32:5452008; 32:545----554554554554
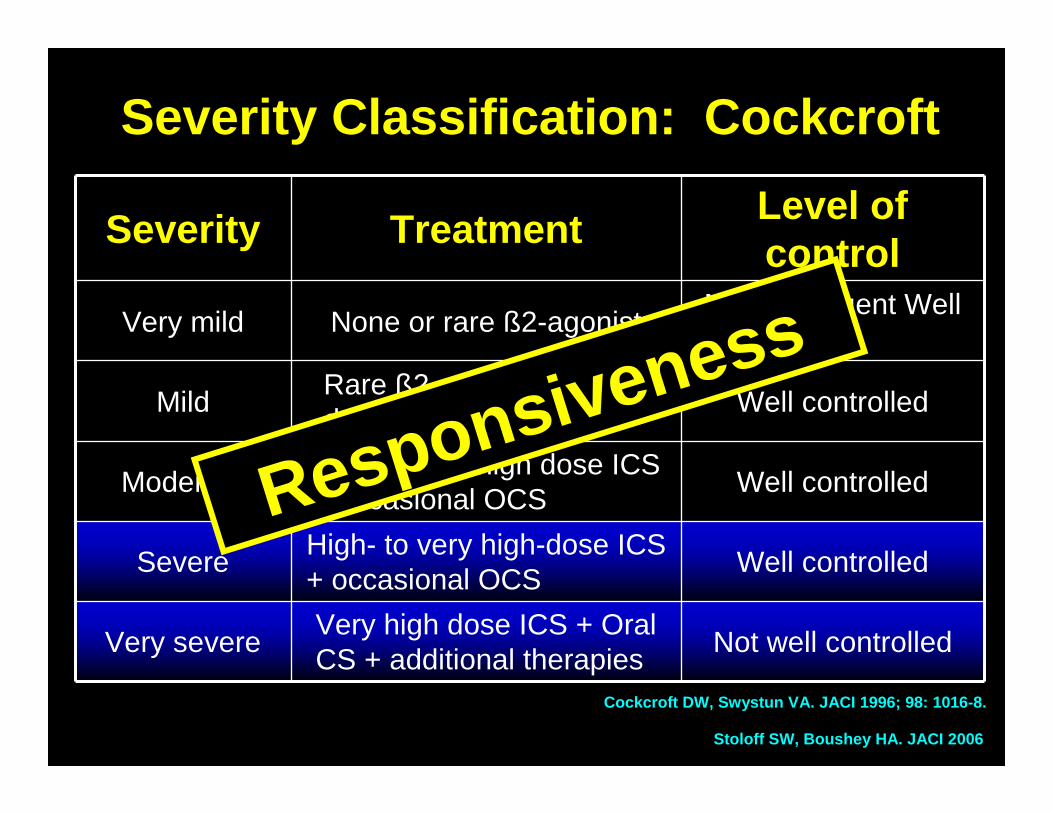
Severity Classification: Cockcroft
Severity TreatmentLevel of control
Very mild None or rare ß2-agonistMild infrequent Well controlled
MildRare ß2-agonist +/- Low-dose ICS
Well controlled
ModerateModerate to high dose ICS + occasional OCS
Well controlled
SevereHigh- to very high-dose ICS + occasional OCS
Well controlled
Very severeVery high dose ICS + Oral CS + additional therapies
Not well controlled
Cockcroft DW, Swystun VA. JACI 1996; 98: 1016-8.
Stoloff SW, Boushey HA. JACI 2006
Responsiveness
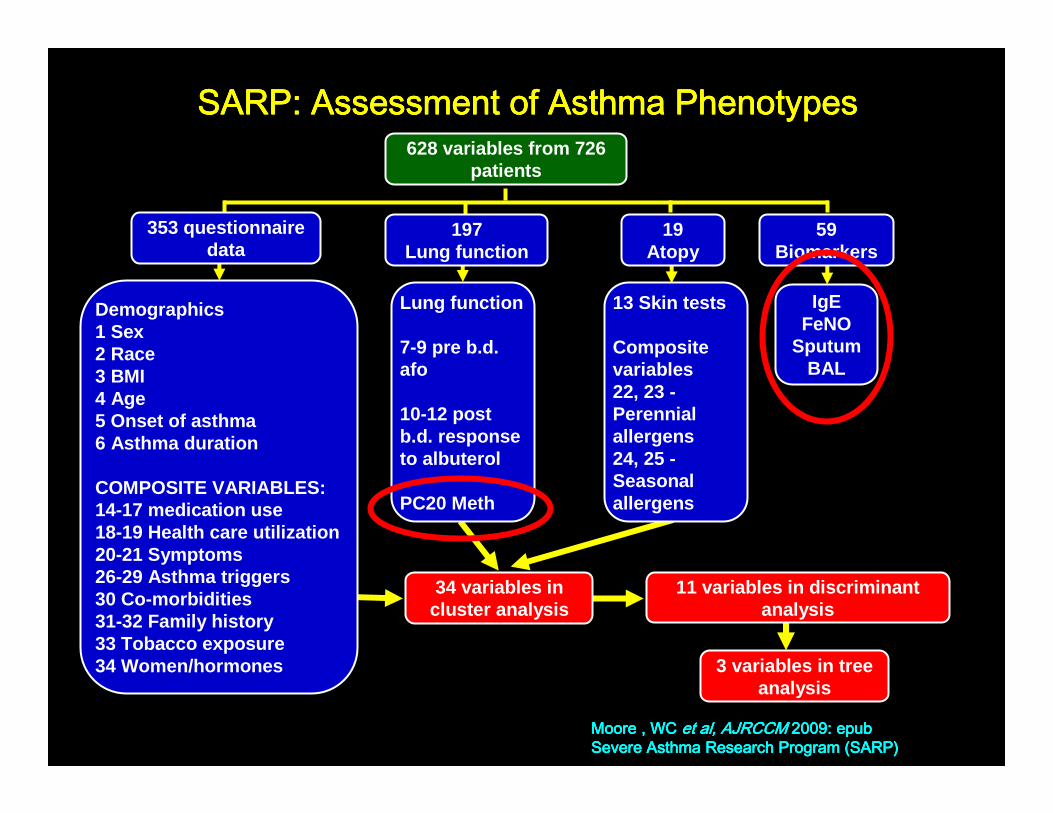
SARP: Assessment of Asthma PhenotypesSARP: Assessment of Asthma PhenotypesSARP: Assessment of Asthma PhenotypesSARP: Assessment of Asthma Phenotypes
Moore , WC Moore , WC Moore , WC Moore , WC et al,et al,et al,et al, AJRCCM AJRCCM AJRCCM AJRCCM 2009: epub2009: epub2009: epub2009: epubSevere Asthma Research Program (SARP)Severe Asthma Research Program (SARP)Severe Asthma Research Program (SARP)Severe Asthma Research Program (SARP)
628 variables from 726 patients
IgEFeNO
SputumBAL
Lung function
7-9 pre b.d. afo
10-12 post b.d. response to albuterol
PC20 Meth
Demographics1 Sex2 Race3 BMI4 Age5 Onset of asthma6 Asthma duration
COMPOSITE VARIABLES:14-17 medication use18-19 Health care utilization20-21 Symptoms26-29 Asthma triggers30 Co-morbidities31-32 Family history33 Tobacco exposure34 Women/hormones
34 variables in cluster analysis
11 variables in discriminantanalysis
3 variables in tree analysis
353 questionnaire data
197Lung function
59Biomarkers
19Atopy
13 Skin tests
Composite variables22, 23 -Perennial allergens24, 25 -Seasonal allergens
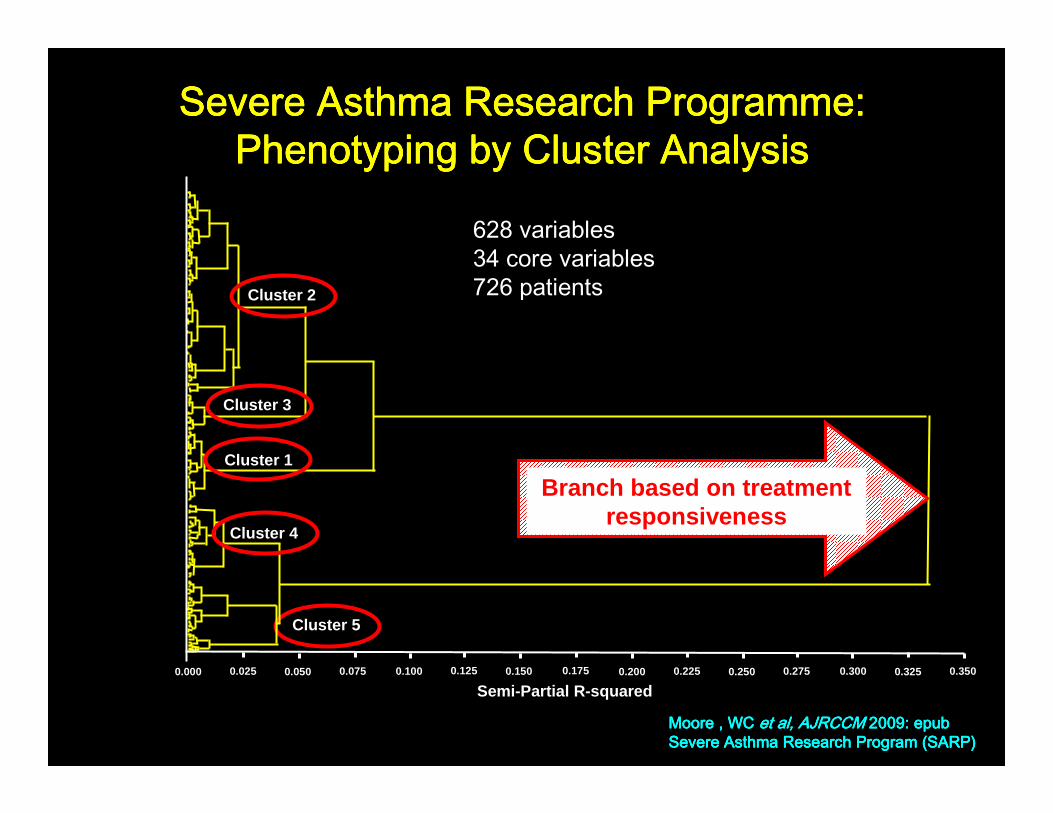
Severe Asthma Research Programme: Severe Asthma Research Programme: Severe Asthma Research Programme: Severe Asthma Research Programme: PhenotypingPhenotypingPhenotypingPhenotyping by Cluster Analysisby Cluster Analysisby Cluster Analysisby Cluster Analysis
Moore , WC Moore , WC Moore , WC Moore , WC et al,et al,et al,et al, AJRCCM AJRCCM AJRCCM AJRCCM 2009: epub2009: epub2009: epub2009: epubSevere Asthma Research Program (SARP)Severe Asthma Research Program (SARP)Severe Asthma Research Program (SARP)Severe Asthma Research Program (SARP)
628 variables34 core variables726 patients
0.000 0.025 0.050 0.075 0.100 0.125 0.150 0.175 0.200 0.225 0.250 0.275 0.300 0.325 0.350
Cluster 1
Semi-Partial R-squared
Cluster 4
Cluster 3
Cluster 5
Cluster 2
Branch based on treatment responsiveness
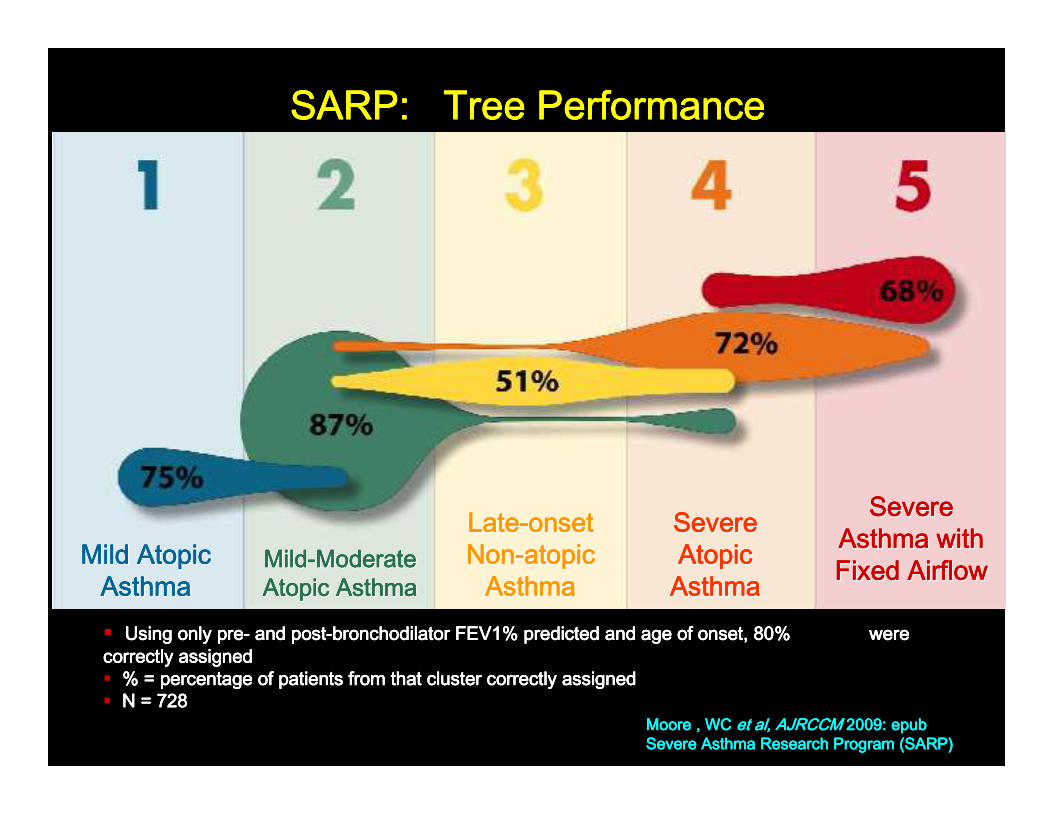
SARP: Tree PerformanceSARP: Tree PerformanceSARP: Tree PerformanceSARP: Tree Performance
Moore , WC Moore , WC Moore , WC Moore , WC et al,et al,et al,et al, AJRCCM AJRCCM AJRCCM AJRCCM 2009: epub2009: epub2009: epub2009: epubSevere Asthma Research Program (SARP)Severe Asthma Research Program (SARP)Severe Asthma Research Program (SARP)Severe Asthma Research Program (SARP)
Mild Atopic Mild Atopic Mild Atopic Mild Atopic Mild Atopic Mild Atopic Mild Atopic Mild Atopic AsthmaAsthmaAsthmaAsthmaAsthmaAsthmaAsthmaAsthma
MildMildMildMildMildMildMildMild--------Moderate Moderate Moderate Moderate Moderate Moderate Moderate Moderate Atopic AsthmaAtopic AsthmaAtopic AsthmaAtopic AsthmaAtopic AsthmaAtopic AsthmaAtopic AsthmaAtopic Asthma
LateLateLateLateLateLateLateLate--------onset onset onset onset onset onset onset onset NonNonNonNonNonNonNonNon--------atopic atopic atopic atopic atopic atopic atopic atopic
AsthmaAsthmaAsthmaAsthmaAsthmaAsthmaAsthmaAsthma
Severe Severe Severe Severe Severe Severe Severe Severe Atopic Atopic Atopic Atopic Atopic Atopic Atopic Atopic
AsthmaAsthmaAsthmaAsthmaAsthmaAsthmaAsthmaAsthma
Severe Severe Severe Severe Severe Severe Severe Severe Asthma with Asthma with Asthma with Asthma with Asthma with Asthma with Asthma with Asthma with Fixed AirflowFixed AirflowFixed AirflowFixed AirflowFixed AirflowFixed AirflowFixed AirflowFixed Airflow
� Using only preUsing only preUsing only preUsing only pre---- and postand postand postand post----bronchodilator FEV1% predicted and age of onset, 80% bronchodilator FEV1% predicted and age of onset, 80% bronchodilator FEV1% predicted and age of onset, 80% bronchodilator FEV1% predicted and age of onset, 80% were were were were correctly assignedcorrectly assignedcorrectly assignedcorrectly assigned� % = percentage of patients from that cluster correctly assigne% = percentage of patients from that cluster correctly assigne% = percentage of patients from that cluster correctly assigne% = percentage of patients from that cluster correctly assignedddd� N = 728N = 728N = 728N = 728

Severe asthma requiring high intensity treatmentATS / ERS Task Force Asthma Control and Exacerbatio ns
Standardizing Endpoints for Clinical Asthma Trials and Clinical Practice
Good control on high Good control on high intensity treatmentintensity treatment
Poor control despite high intensity treatment
Poor control Poor control despite despite high high intensity treatmentintensity treatment
Treatment responsive, but with persistent
problems e.g. poor adherence,
smoking
Treatment Treatment responsive, but responsive, but with persistent with persistent
problems e.g. poor problems e.g. poor adherence, adherence,
smokingsmoking
Persistent coPersistent co --morbidities e.g. morbidities e.g.
GE reflux, obesityGE reflux, obesity
Treatment Treatment resistant/ resistant/
refractory asthmarefractory asthma
“Severe asthma is defined as the requirement for high intensity treatment after modifiable factors and comorbidites have been
appropriately managed”
Reddel H , et al, Amer J Resp Crit Care Med 2009;180:59-99
• All severe asthma requires confirmed diagnosis of asthma, compliance/adherence and co-morbidities addressed
• All severe asthma requires treatment with “gold standard medication” (for that age group) for 3 months by asthma specialist* to prevent patient from becoming uncontrolled or which remains uncontrolled.
• *Asthma specialist can vary from country to country and from children to adults. In adults, this is traditionally an allergist or pulmonologist/respirologist with advanced training and experience in asthma. In pediatric populations this may also include pediatricians with additional training and experience in severe asthma
WHO: Definition of Severe or Difficult to Manage Asthma
Bousquet J et al, JACI 2010

High dose inhaled CS and LABA (or LT modifier) and / High dose inhaled CS and LABA (or LT modifier) and / or systemic CS for or systemic CS for >>50% of the previous year. 50% of the previous year.
High dose ICS is fluticasone High dose ICS is fluticasone >>1000 mcg/day 1000 mcg/day (or equivalent)(or equivalent)
Definition of Severe or Difficult to Manage Asthma:
Gold Standard TherapyGold Standard Therapy
Bousquet J et al, JACI 2010
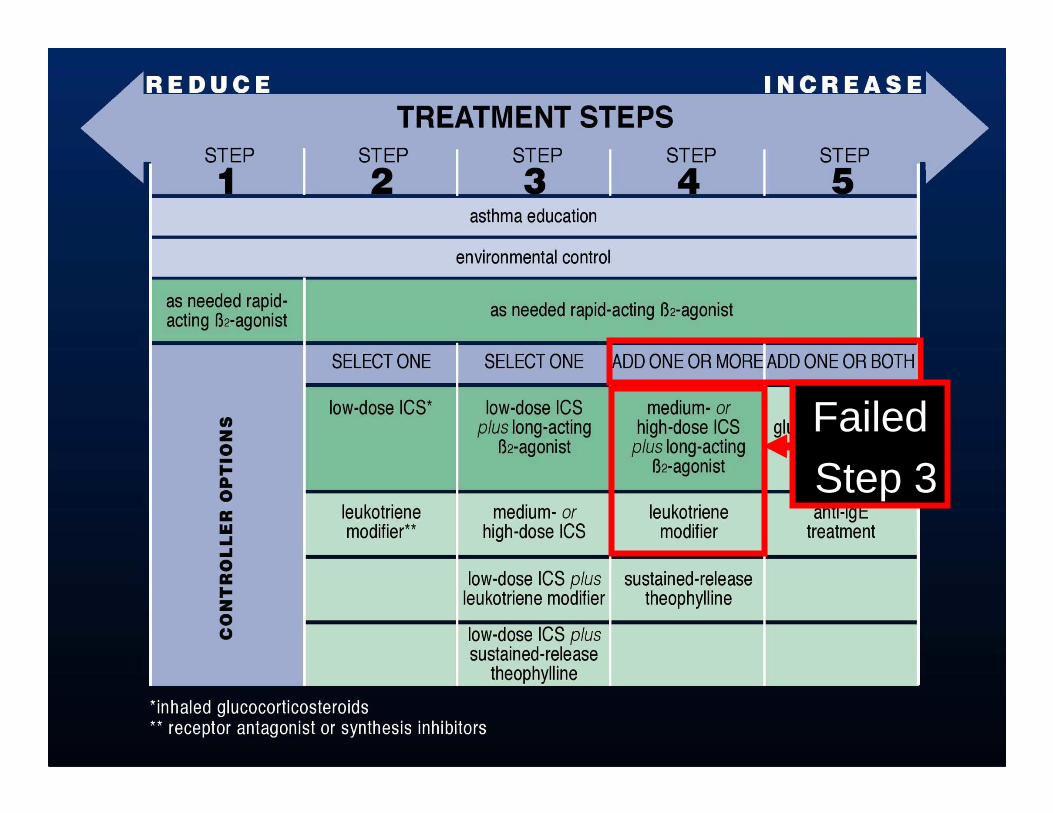
FailedStep 3
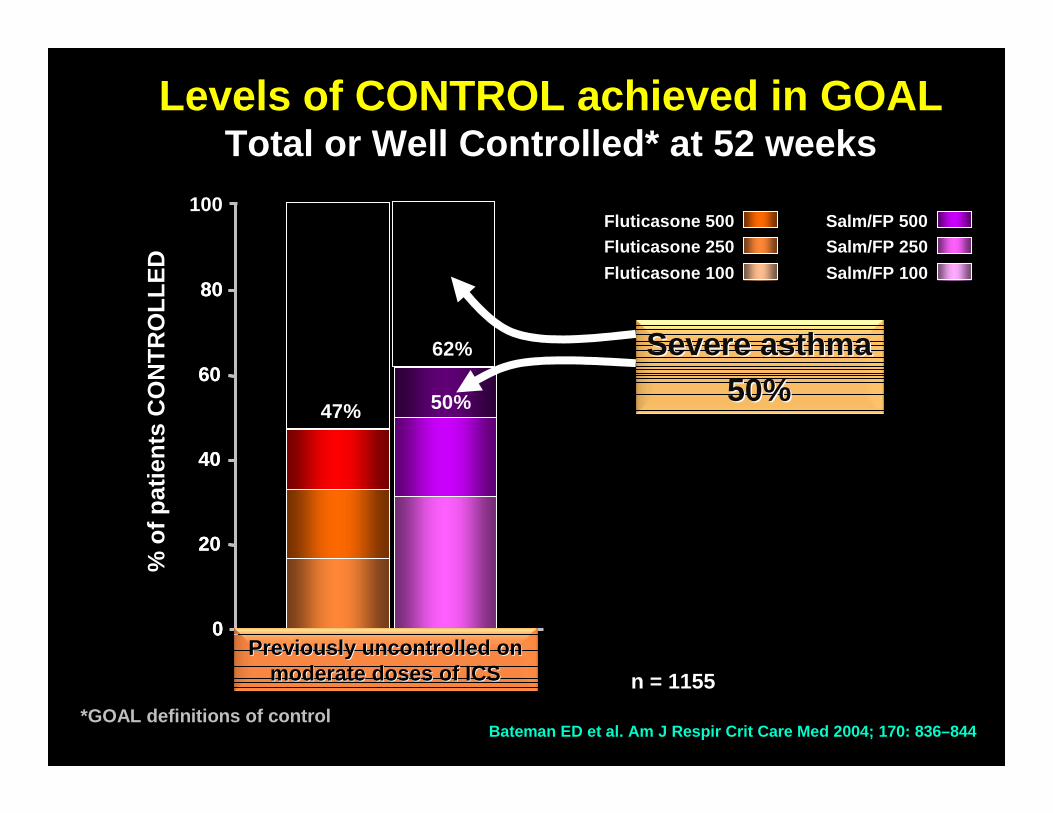
Levels of CONTROL achieved in GOALTotal or Well Controlled* at 52 weeks
Salm/FP 500Fluticasone 500Salm/FP 250Fluticasone 250
Salm/FP 100Fluticasone 100
0
n = 1155
20
80
40
60
% o
f pat
ient
s C
ON
TR
OLL
ED
0
20
80
40
60
100
62%
47%
Bateman ED et al. Am J Respir Crit Care Med 2004; 170: 836–844*GOAL definitions of control
Previously uncontrolled on Previously uncontrolled on moderate doses of ICSmoderate doses of ICS
Severe asthmaSevere asthma50%50%50%

Week
Con
trol
led
and
Par
tly
Con
trol
led
(%)
0 4 8 12 16 20 24 28 32 36 40 44 48 52
10
0
20
30
40
50
56
60
1. O’Byrne PM, et al. Am J Respir Crit Care Med 2005;171:129–1362. Scicchitano R, et al. Curr Med Res Opin 2004;20:1403–141
3. Rabe KF, et al. Lancet 2006;368:744–7534. Kuna P, et al. Int J Clin Pract 2007;61:725–736
5. Bousquet J, et al. Respir Med 2007;101:2437–2446
Patients (% per week) achieving GINA Controlled or Partly Controlled weeks during Bud/Form M&R studies
Bud/Form M&R Bud/Form M&R vsvsHighHigh --dose dose ICS/LABA ICS/LABA + SABA+ SABA 4,54,5
Week
0 4 8 12 16 20 24 28
10
0
20
30
40
50
60
Con
trol
led
and
Par
tly
Con
trol
led
(%)
Week
0 4 8 12 16 20 24 28 32 36 40 44 48 52
10
0
20
30
40
50
56
60
Con
trol
led
and
Par
tly
Con
trol
led
(%)
Bud/Form M&R Bud/Form M&R vsvsSameSame--dose dose ICS/LABA ICS/LABA + SABA+ SABA 1,31,3
Bud/Form M&R Bud/Form M&R vsvsHighHigh --dose ICS dose ICS
+ SABA+ SABA 1,21,2
Bateman ED Bateman ED Bateman ED Bateman ED et alet alet alet al, , , , JACIJACIJACIJACI 2010 2010 2010 2010
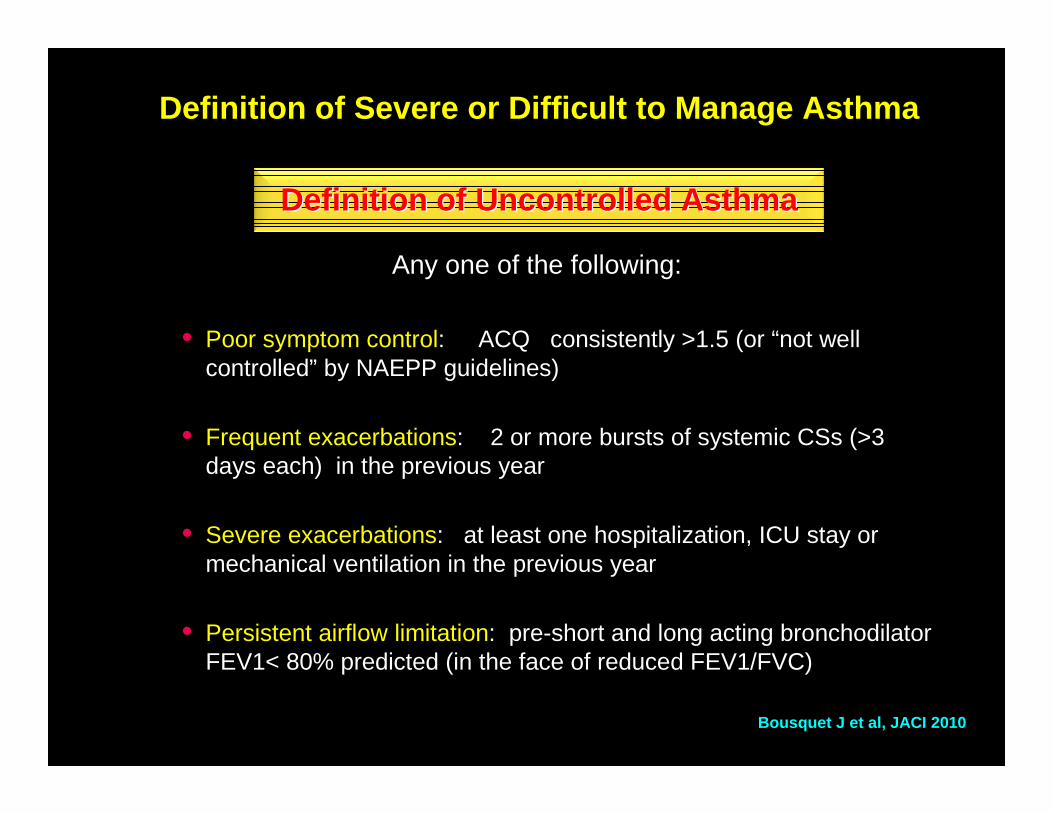
Any one of the following:
• Poor symptom control: ACQ consistently >1.5 (or “not well controlled” by NAEPP guidelines)
• Frequent exacerbations: 2 or more bursts of systemic CSs (>3 days each) in the previous year
• Severe exacerbations: at least one hospitalization, ICU stay or mechanical ventilation in the previous year
• Persistent airflow limitation: pre-short and long acting bronchodilator FEV1< 80% predicted (in the face of reduced FEV1/FVC)
Definition of Severe or Difficult to Manage Asthma
Definition of Uncontrolled AsthmaDefinition of Uncontrolled Asthma
Bousquet J et al, JACI 2010
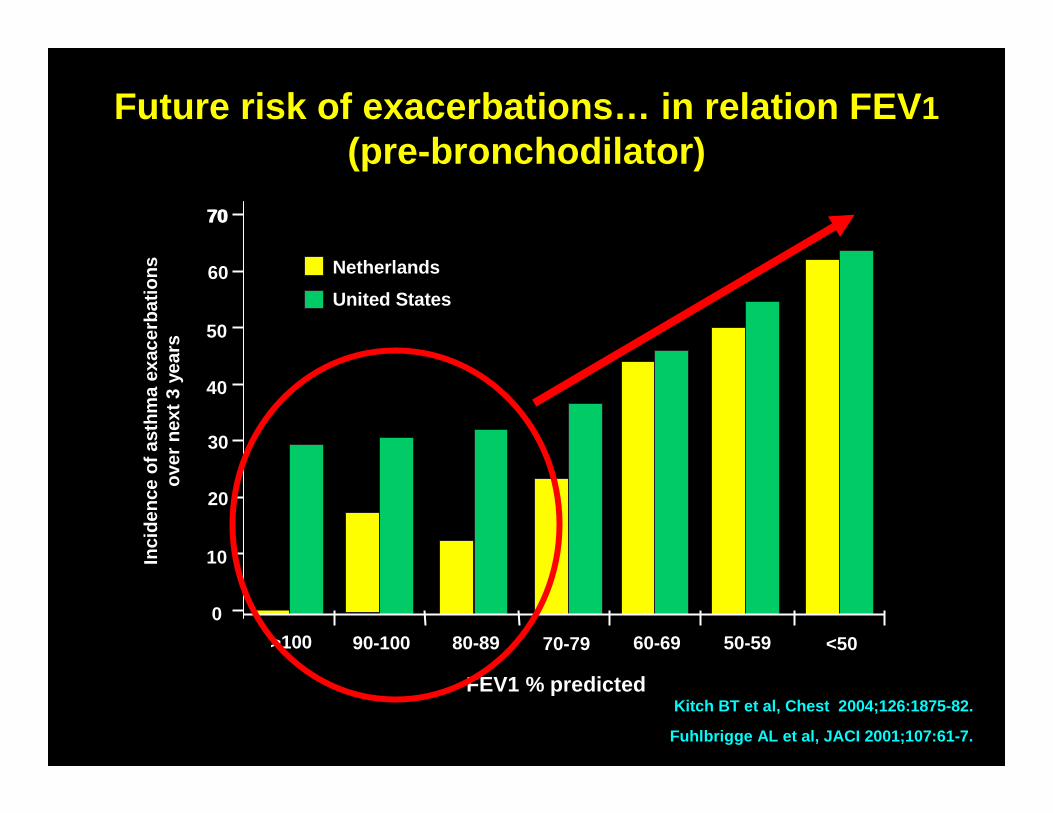
Future risk of exacerbations… in relation FEV 1(pre-bronchodilator)
Fuhlbrigge AL et al, JACI 2001;107:61-7.
7070
60
50
40
30
20
10
0
United States
Inci
denc
e of
ast
hma
exac
erba
tions
ov
er n
ext 3
yea
rs
>100 90-100 80-89 70-79 60-69 50-59 <50
FEV1 % predicted
Netherlands
Kitch BT et al, Chest 2004;126:1875-82.
• Controlled asthma on these high doses of inhaled corticosteroids or systemic CS (or additional biologics) places a patient at high future risk for side effects from medications
Definition of Severe or Difficult to Manage Asthma
Bousquet J et al, JACI 2010
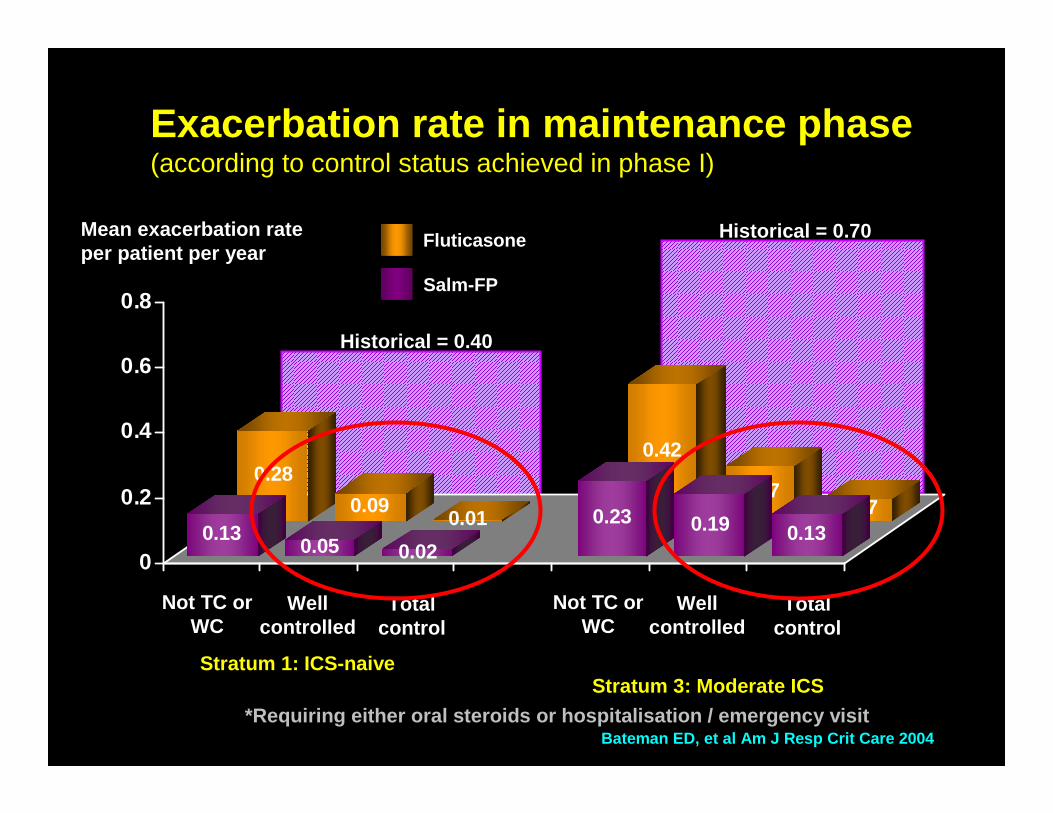
Historical = 0.40
Historical = 0.70
0.28
0.090.01
0.42
0.170.07
0.130.05 0.02
0.23 0.19 0.130
0.2
0.4
0.6
0.8
Stratum 1: ICS-naiveStratum 3: Moderate ICS
*Requiring either oral steroids or hospitalisation / emergency visitBateman ED, et al Am J Resp Crit Care 2004
Exacerbation rate in maintenance phase(according to control status achieved in phase I)
Not TC or WC
Well controlled
Total control
Not TC or WC
Well controlled
Total control
Mean exacerbation rate per patient per year
Fluticasone
Salm-FP
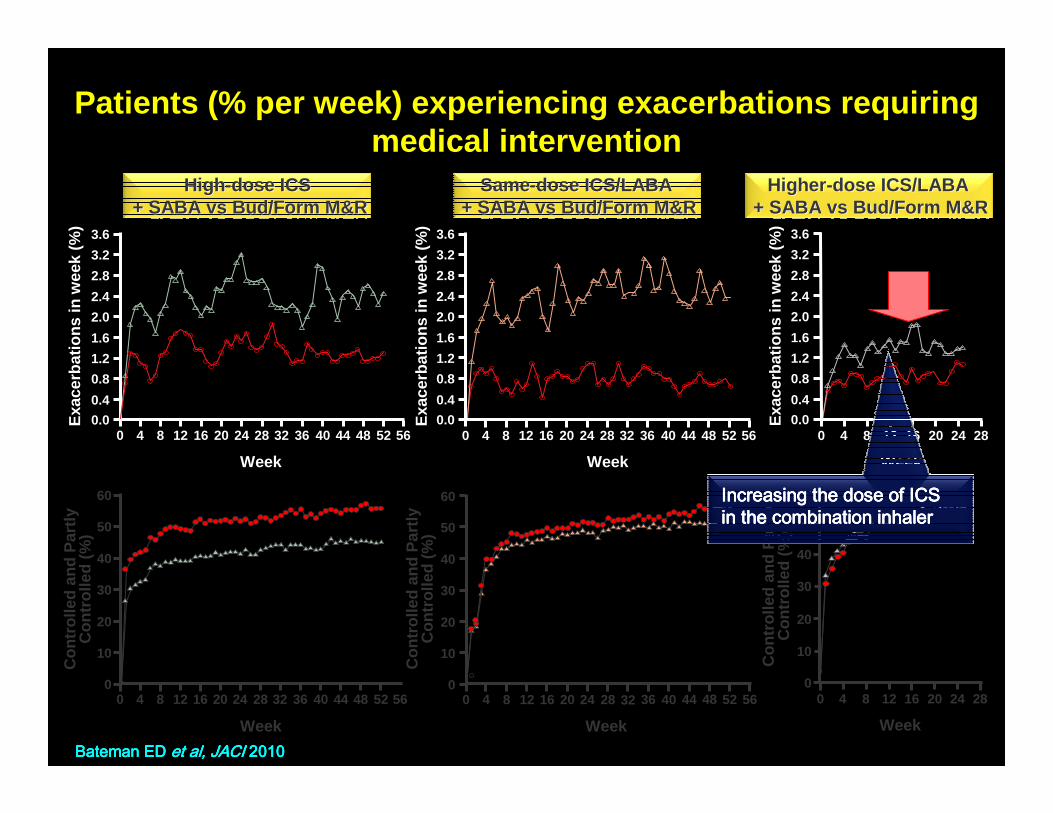
HighHigh --dose ICS dose ICS + SABA + SABA vsvs Bud/Form M&RBud/Form M&R
Exa
cerb
atio
ns in
wee
k (%
)
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56
1.6
0.0
2.0
2.4
2.8
3.2
3.6
1.2
0.8
0.4
Week
SameSame--dose ICS/LABA dose ICS/LABA + SABA + SABA vsvs Bud/Form M&RBud/Form M&R
1.6
0.0
2.0
2.4
2.8
3.2
3.6
1.2
0.8
0.4
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56E
xace
rbat
ions
in w
eek
(%)
Week
HigherHigher --dose ICS/LABA dose ICS/LABA + SABA + SABA vs vs Bud/Form M&RBud/Form M&R
0 4 8 12 16 20 24 28
Week
1.6
0.0
2.0
2.4
2.8
3.2
3.6
1.2
0.8
0.4
Exa
cerb
atio
ns in
wee
k (%
)
Patients (% per week) experiencing exacerbations re quiring medical intervention
Week
0 4 8 12 16 20 24 28 32 36 40 44 48 52
10
0
20
30
40
50
56
60
Con
trol
led
and
Par
tly
Con
trol
led
(%)
Week
Con
trol
led
and
Par
tly
Con
trol
led
(%)
0 4 8 12 16 20 24 28 32 36 40 44 48 52
10
0
20
30
40
50
56
60
Week
0 4 8 12 16 20 24 28
10
0
20
30
40
50
60
Con
trol
led
and
Par
tly
Con
trol
led
(%)
Increasing the dose of ICSIncreasing the dose of ICSIncreasing the dose of ICSIncreasing the dose of ICSin the combination inhalerin the combination inhalerin the combination inhalerin the combination inhaler
Bateman ED Bateman ED Bateman ED Bateman ED et al, JACI et al, JACI et al, JACI et al, JACI 2010201020102010
Disease factors:� Wrong diagnosis: Functional upper airway problems,
heart disease� Unrecognised trigger factors: drugs, occupational
agents�Associated disease: GORD, sinusitis, thyrotoxicosis�Corticosteroid refractoriness or resistance
Health system factors:� Inadequate or inappropropriate treatment�Failed patient / physician partnership
Patient factors:�Poor adherence �Psychological / personality �Socio-behavioural
Severe and difficult to manage asthma

‘normal’
Mild asthmasteroid-responsive
Severe asthma‘steroid-dependent’
Steroid resistant
Corticosteroid refractoriness is not absolute
Dose of corticosteroidDose of corticosteroid
Improved Improved Improved Improved Improved Improved Improved Improved asthma asthma asthma asthma asthma asthma asthma asthma controlcontrolcontrolcontrolcontrolcontrolcontrolcontrol
Reduced Reduced Reduced Reduced Reduced Reduced Reduced Reduced airway airway airway airway airway airway airway airway
inflammation inflammation inflammation inflammation inflammation inflammation inflammation inflammation (%)(%)(%)(%)(%)(%)(%)(%)
Disease factors:� Wrong diagnosis: Functional upper airway problems,
heart disease� Unrecognised trigger factors: drugs, occupational
agents�Associated disease: GORD, sinusitis, thyrotoxicosis�Corticosteroid refractoriness or resistance
Health system factors:� Inadequate or inappropropriate treatment�Failed patient / physician partnership
Patient factors:�Poor adherence �Psychological / personality �Socio-behavioural / economic considerations
Severe and difficult to manage asthma

Severe /Difficult to manage asthma
Patients are not all the same !Patients are not all the same !
Revised NEO Personality InventoryRevised NEO Personality InventoryCosta PT & McCrae RR, 1992Costa PT & McCrae RR, 1992
Asthma Management and Prevention Programme
Component 1: Develop a doctor / patient partnership
DoctorDoctor --directed patient selfdirected patient self --managementmanagement
Written self-management plans are associated with improved asthma outcomes
Alexithymia
Alexithymia
= difficulty in perceiving and expressing
emotions and body sensations
� Prevalence: 8 - 19% of males in general population� Toronto Alexithymia Score� Correlates with neuroticism� Negative correlation with Extraversion and Openness
Bagby RM et al, J Pschosom Res 1994; 38: 23 Luminet O Bagby RM et al, J Pschosom Res 1994; 38: 23 Luminet O Bagby RM et al, J Pschosom Res 1994; 38: 23 Luminet O Bagby RM et al, J Pschosom Res 1994; 38: 23 Luminet O et alet alet alet al, J Pers Assess 1999; 73:345, J Pers Assess 1999; 73:345, J Pers Assess 1999; 73:345, J Pers Assess 1999; 73:345Serrano J Serrano J Serrano J Serrano J et alet alet alet al, ERJ 2006; 28: 296 Plaza V , ERJ 2006; 28: 296 Plaza V , ERJ 2006; 28: 296 Plaza V , ERJ 2006; 28: 296 Plaza V et alet alet alet al, J Asthma 2006; 43: 639, J Asthma 2006; 43: 639, J Asthma 2006; 43: 639, J Asthma 2006; 43: 639
Alexithymia more common in patients with near-fatal asthma episodes (36 versus 13%)
More severe asthma, and very severe near-fatal episodes
Severe and Difficult to Manage Asthma
� Severe asthma is common !
� Definition is clinical
� Consider domains to establish cause
� In real life practice, patient factors are most common
� Resistance to treatment is relative and seldom complete
� New second/third line (targeted) controllers are needed
Take home messages