december 2, 2017 - nhpharmacists.net presentations/last chance 2017... · renal fxn, thyroid panel,...
TRANSCRIPT

1
Devon Anne Sherwood, PharmD, BCPPAssistant Professor, UNE College of PharmacyClinical Psychopharmacology Specialist, Spring Harbor Hospital
December 2, 2017

Identify the pathophysiologic mechanisms underlying bipolar disorder relating to the various presentations involved.
Describe the medication profile of mood stabilizers and recommend appropriate acute and chronic treatments
Analyze the pharmacology and side-effect profile of FDA approved treatments
Explain a general approach to treatment for special populations (ie. elderly, pediatric, pregnant patients)
2
A lifelong disorder of periods of elevated mood, high energy, irritability, decreased need for sleep, grandiosity and euphoria◦ 1st episode is usually depressed ( or ) More men than women present as
manic first
80% experience multiple episodes
3

Caused likely due to:◦Genetics, environmental triggers, and dysregulation of neurotransmitters, neurohormones, and second messenger systems in the brain
Epidemiology:◦ ~3-7% lifetime prevalence◦ Recent study = 4.5% BPD I = 1%, BPD II = 1.1% Average onset 15 – 30 years old
Kaplan & Saddock Comprehensive Textbook of Psychiatry, 9th edDrugs. 2009;69:2063–2101.
Up to Date 2017 Dipiro 10th Ed.4
5

Chromosomal regions reported to be linked to bipolar and unipolar disorders
Kaplan & Saddock - Comprehensive Textbook of Psychiatry 9th ed. Volume 1 - Table 13.3-5
Pathophysiology: Genetic influence80% concordance in identical twin80-90% have a biological relative with a mood disorder• Family, twin and adoption studies report lifetime prevalence
risk among 1st degree relatives

Neurotransmitter alterations in the CNS:◦ Monoamine hypothesis
Functional deficit of NE, DA, and/or 5-HT in depression and excess of NE and DA in mania
◦ Permissive hypothesis
CNS 5-HT is low in mania & depression, and superimposed low NE = depression & high NE = mania
◦ Dysregulation hypothesis
Mood disorders may be caused by a dysregulation between NT systems
7
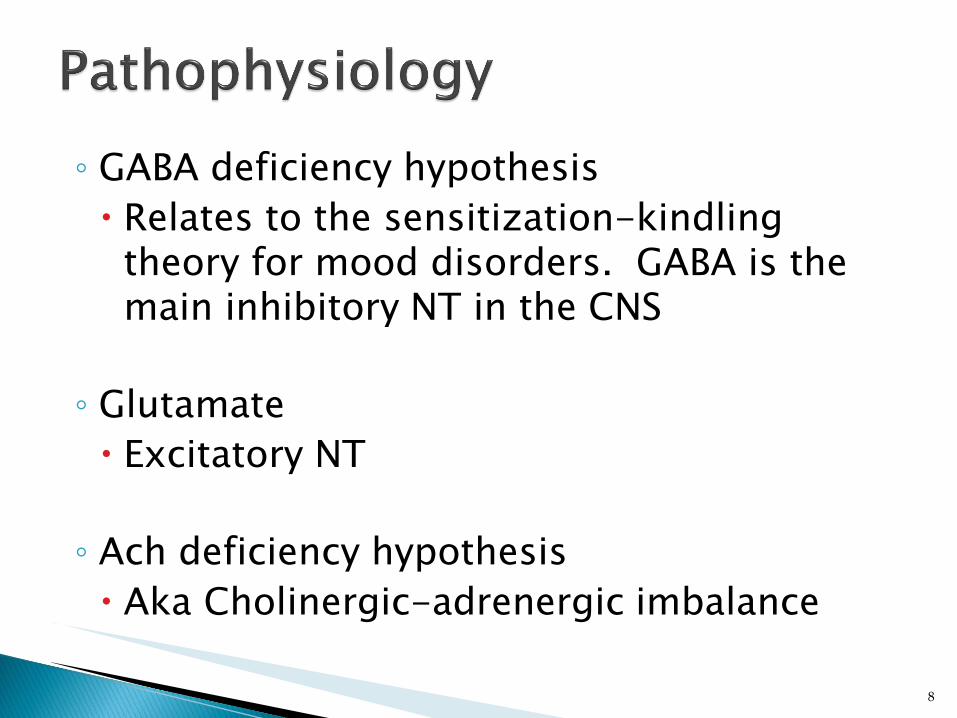
◦ GABA deficiency hypothesis
Relates to the sensitization-kindling theory for mood disorders. GABA is the main inhibitory NT in the CNS
◦ Glutamate
Excitatory NT
◦ Ach deficiency hypothesis
Aka Cholinergic-adrenergic imbalance
8

Neuroimaging studies:◦ Shown abnormalities in neurochemical, anatomical
and functional abnormalities
9
http://www.bipolar-lives.com/bipolar-brain-imaging.html

Environmental & Psychosocial stressors
Others:◦ Second messenger theories◦ Infections◦ Immunological reactions◦ Nutritional deficiencies◦ Sleep deprivation◦ Disruption of circadian rhythms◦ Endocrine abnormalities (ie, hormonal disturbances, thyroid)◦ Hypocalcemia / hypercalcemia
10
DS
M 5, 2013
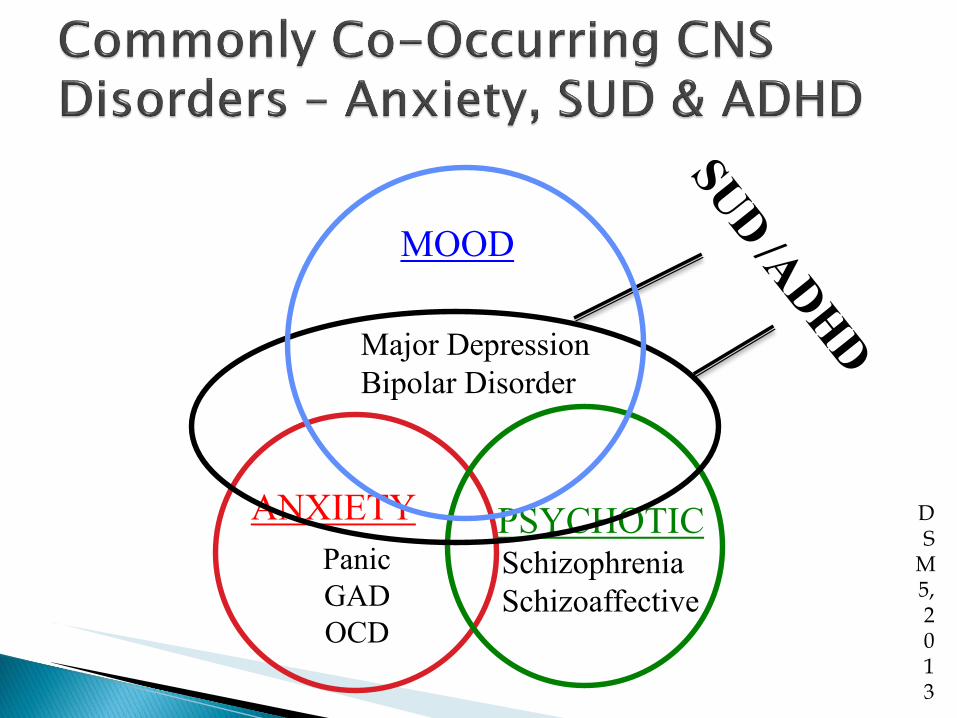
ANXIETY
Panic
GAD
OCD
PSYCHOTICSchizophrenia
Schizoaffective
MOOD
Major Depression
Bipolar Disorder

12
Am J Psychiatry 2002;159(4):iv,1-50.Mahli GS et al. CNS Drugs 2003;17:9-25Kaplan & Saddock Comprehensive Textbook ofPsychiatry, 9th edDSM-5
46% of patients abuse EtOH◦ Attempt to self-medicate
41% of patients use other drugs◦ Illicit and prescription
25 - 50% attempt suicide◦ 10-15% succeed
◦ 30 times greater when depressed

Primary mania without treatment◦ 50% remission in 20 weeks
◦ 100% remission in 40 weeks
Overall◦ 50% relapse rate if
untreated in 1 year
Mixed mania or depressive phase◦ 45% remission in 1 year
13
Bipolar I Disorder
Bipolar II Disorder
Cyclothymic Disorder
Substance/Medication-Induced Bipolar and Related Disorder
http://dsm.psychiatryonline.org.une.idm.oclc.org/doi/full/10.1176/appi.books.9780890425596.dsm03
14

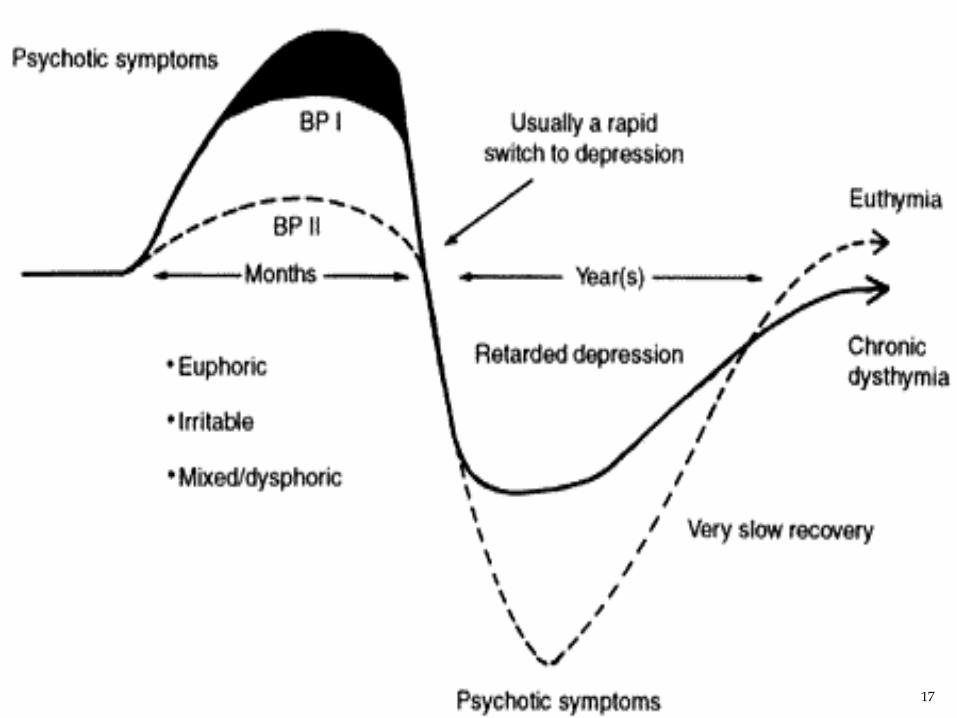
Bipolar I Disorder :
◦ “requires at least one Manic or Mixed episode, but there may be episodes of Hypomania, MajorDepression, or mixed features. (This diagnosis conforms to the classic concept of manic depressive illness.)”
15

Bipolar II Disorder:
◦ “requires neither a Manic nor a Mixed Episode, but does require at least one episode of hypomania in addition to an episode of Major Depression”
16
17

Complete history ◦ PMHx/PSurgHx
◦ Past Psych Hx
◦ Family
◦ Social
◦ Medication
Physical & neurologic exam◦ Include vitals & ECG in initial workup
Labs ◦ CBC, CMP (Chem7, LFT’s), fasting glucose, lipids,
renal fxn, thyroid panel, Utox, UA, pregnancy
Mental Status Examination
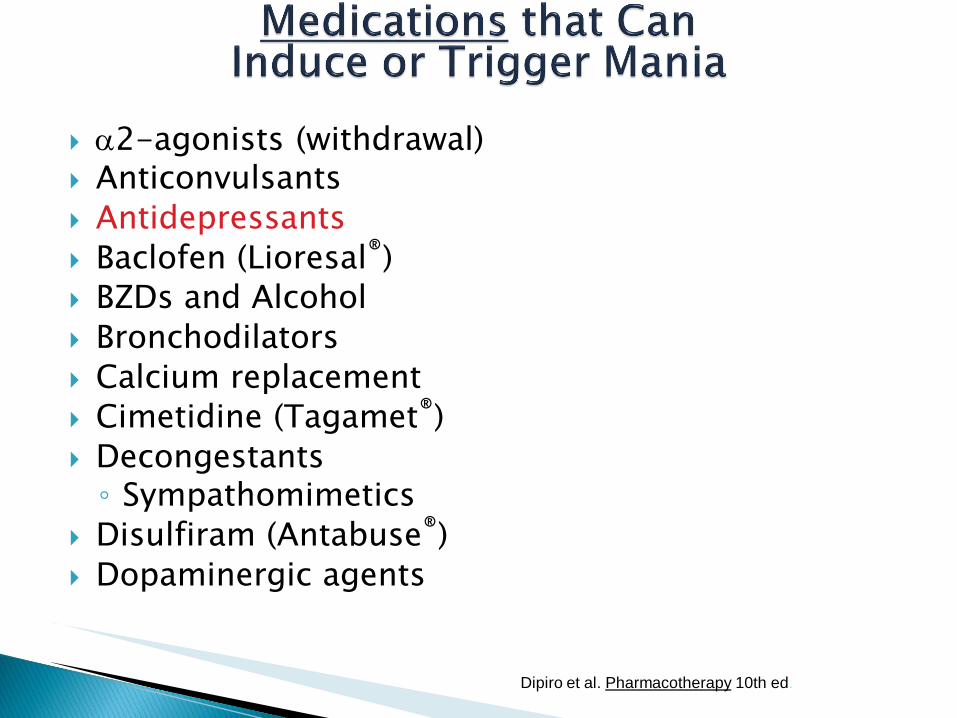
2-agonists (withdrawal) Anticonvulsants
Antidepressants
Baclofen (Lioresal®)
BZDs and Alcohol
Bronchodilators
Calcium replacement
Cimetidine (Tagamet®)
Decongestants ◦ Sympathomimetics
Disulfiram (Antabuse®)
Dopaminergic agents
19Dipiro et al. Pharmacotherapy 10th ed.

Hallucinogens: LSD, phencyclidine
Interferon (withdrawal)
Isoniazid
NSAIDs (ie. Motrin®, Aleve® )
Procainamide
Quinacrine
Steroids
◦ Anabolic, corticosteroids, ACTH
Stimulants
Xanthines
Yohimbine
20Dipiro et al. Pharmacotherapy 10th ed.

Mood◦ Euphoric◦ Elated/happy◦ Irritable
Cognitive◦Grandiose◦ Flight of ideas/racing thoughts◦Hallucinations and delusions◦ Ideas of reference
21

Activity and behavior◦ Aggressiveness/
violence/outbursts◦ Insomnia/
constant motion◦ Impulsiveness◦ Pressured speech◦ Increased sexual activity◦ Increased artistic abilities
22
Bipolar I:◦ Lifelong mood stabilizer therapy is recommended for patients
with 2 manic episodes, 1 severe manic episode, a strong family BPD hx, more than1 manic episode per year, or rapid onset of manic episodes.
Bipolar II:◦ Long-term prophylaxis for patients is recommended after three
hypomanic episodes or if the patient required an antidepressant but became hypomanic.
Breakthrough episodes ◦ Short-term BZD’s or AP’s for mania
◦ Short-term Antidepressants for depression??? – controversial!!
23

Hypomanic episodes may not require treatment unless there is a hx of mania
Acute manic episodes can be treated with a mood stabilizer (Lithium, CBZ or VPA) with adjunctive BZD for anxiety/insomnia. ◦ Severe episodes with psychosis and agitation require
antipsychotics + BZD’s along with the mood stabilizer.
24
If no response w/in 2-4weeks, a second mood stabilizer can be added. If patient is still nonresponsive, the mood stabilizer should be switched to another agent, or ECT may be used.
After remission, adjunctive agents are tapered and discontinued over 2-6 months
After response, patients with only one manic episode should continue on a mood stabilizer for 12 months
25
Largest BPD trial to date– NIMH study offering several findings since 2003
Standard Care Pathway◦ Mood Stabilizers:
Anticonvulsants
Antipsychotics
Role of Antidepressants?
26
Sachs G, et al. Acta Psychiatrica Scandinavica 2004;110(suppl. 422):7-17).Sachs G, et al. Effectiveness of Adjunctive Antidepressant Treatment for Bipolar Depression: A Double-blind Placebo-controlled Study . New England Journal of Medicine. online 28 Mar 2007.
Concomitant antidepressant therapy (not monotherapy!)
◦ 35% of rapid cyclers will switch
◦ 26% have rate of cycling (incl. depression)
◦ SSRIs reported to cause up to 27% mania
◦ Lithium can reduce switching
◦ Bupropion may cause less switching vs. other antidepressants
Many patients require polypharmacy
Rapid medication discontinuation
◦ ’s relapses by 250%
◦ Meds should be tapered over 2-4 week
Prim Care Companion CNS Disord. 2014; 16(5) 10
NICE Guidelines
Arch Gen Psychiatry 2000;57:490-2
.27
28

MANIA MAINTENANCE DEPRESSION
Lithium 1970 1974
Thorazine 1973
Depakote 1995
Zyprexa 2000 2003
Lamictal 2003
Risperdal 2003
Seroquel 2004 2008 2006
Abilify 2004 2005 2007
Geodon 2004
Symbyax 2009 2004
Equetro 2004
Tegretol XR 2004
Saphris 2009 2010
Latuda 2013
Vraylar 2015

Pregnancy◦ Use lowest effective dose (ie. try to dose reduce if
possible) for any medication used treating bipolar disorder in pregnancy
◦ Haldol often still preferred for acutely manic symptoms or as mood stabilizer – most commonly used in this population
◦ SGA’s = limited studies, watch for gestational diabetes
◦ Benefit vs. Risk??? Lithium Lamotrigine Carbamazepine Valproic acid/Divalproex Sodium
30
Pediatrics◦ Lithium, carbamazepine & valproic acid all used
◦ Lithium FDA approved over 12yo
◦ Aripiprazole & risperidone approved in 13-17yo, mania
◦ Quetiapine approved in 10-17yo, monotherapy or adjunct to lithium or valproic acid
◦ Olanzapine is approved in 13-17yo, mania or mixed
Elderly◦ Lithium elimination T½ increase as renal clearance
decreases (can double)
◦ Valproic acid T½ increases with aging
◦ Elderly may be more sensitive to side effects of mood stabilizers and antipsychotics, especially with dementia
31
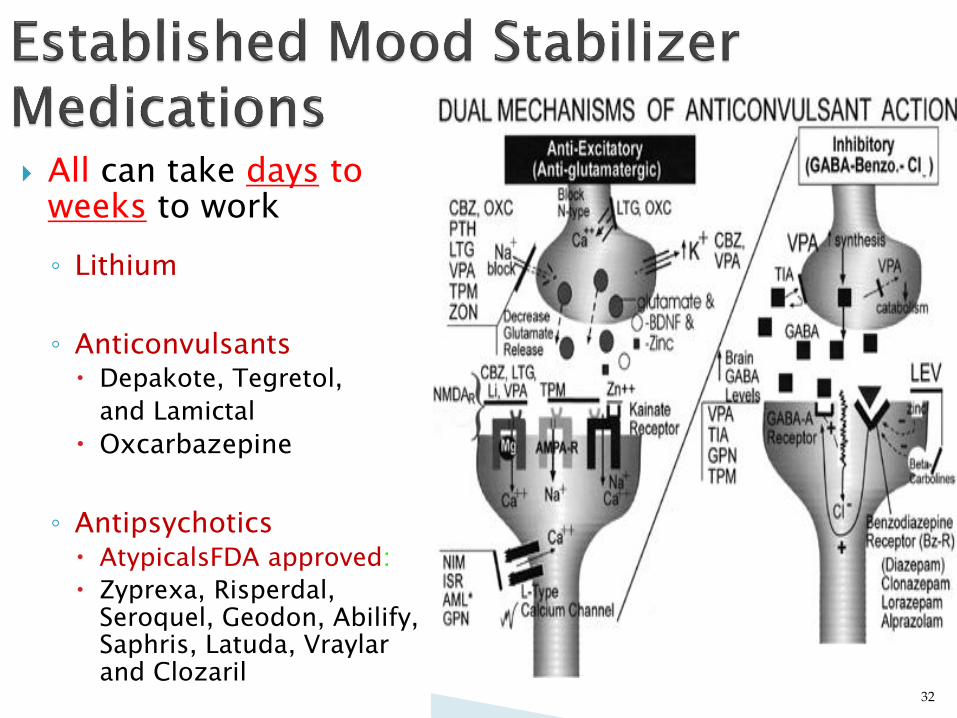
All can take days toweeks to work
◦ Lithium
◦ Anticonvulsants Depakote, Tegretol,
and Lamictal
Oxcarbazepine
◦ Antipsychotics AtypicalsFDA approved:
Zyprexa, Risperdal, Seroquel, Geodon, Abilify, Saphris, Latuda, Vraylarand Clozaril
32

A. Risperidone
B. Lithium
C. Valproic Acid
D. Carbamazepine
E. Lamotrigine
33
Equally effective in preventing both manic and depressive episodes 20 - 30% patients do NOT respond or can’t tolerate
~70% effective for acute manic episode 80-90% effective for prophylaxis◦ Less effective in rapid cycling and mixed BPD ◦ 20-50% relapse rate over 2 years
Half-life ranges from 18 to 36 hours◦ Dependent on renal function, disease state and concomitant
drug use
Caution in pregnancy and breast-feeding◦ Can cause Epstein’s Anomaly
Toxicity can be fatal
34
Absorption◦ Readily absorbed from GI tract
◦ Peak serum levels occur in 2-4 hours
◦ Complete within 8 hours
◦ Slow release formulation have a slower and more variable absorption rate
Elimination◦ >95% renally excreted
◦ 80% reabsorbed at proximal tubule
◦ 20% is excreted in urine
35
Dosage◦ 300mg BID up to 900mg TID
◦ Dose according to blood levels
Acute phase = 0.8 - 1.2 mEq/L (up to 1.4 severe)
Maintenance phase = 0.4 - 1.0 mEq/L
Initiation◦ Start low and titrate up slowly (Usually 300mg bid)◦ Observe for clinical improvement while monitoring level range
(acute vs maintenance phase)
Steady State serum level determination◦ Steady state should be reached after 4-5 days of dose change◦ Draw levels 12 hours post dose◦ Once maintenance therapy achieved, monitor every 2-3 months
36

Fine hand tremor (50%)
◦ Tx. with -blockers!
Polyuria
Polydipsia
Weight gain (20%)
Goiter / hypothyroidism
◦ 5-15% of patients
◦ May develop after years
◦10 X more likely in women
◦ Mostly irreversible
Leukocytosis
EKG changes
Neurologic
Dermatologic
libido
Metallic taste
Urinary incontinence
37
(>70%)

Side Effects
◦ Early GI disturbances
Muscle weakness, lethargy
Sedation
HA, confusion, ↓ memory, ↓ concentration
Tremor
Dry mouth
Leukocytosis
Late◦ Nephrogenic diabetes insipidus◦ Hypothyroidism
38

Toxicity - Related to plasma levels◦ Diarrhea◦ Severe nausea and vomiting◦ Coarse hand tremor◦ Hyperreflexia◦ Drowsiness, lethargy◦ Muscular weakness, lack of coordination, ataxia◦ Blurred vision, dry mouth◦ Large output of dilute urine◦ Confusion, CNS irritability◦ Slurred speech◦ Cardiovascular (arrhythmias, hypotension)◦ Seizures, coma, death Intermittently dialyze if blood levels > 3.5mEq/L
39

Lavage (for acute ingestion)
Correct / Maintain fluid and electrolyte balance
Maintain adequate fluid and salt intake, especially in situations of dehydration.◦ BEST TREATMENT: NaCl 0.9% IV
Monitor cardiac and respiratory fxn
Seizure precaution
Monitor Li+ conc. (Q 3-4 hours)
Dialysis ◦ Li+ is the only psychotropic that is dialyzable!
40

NSAIDs ( Li+)◦ Decrease renal function
Diuretics ( Li+)◦ K-Sparing, Thiazides
Antipsychotics / Antidepressants
Xanthines (i.e. Theophylline, Caffeine) ( Li+)
Cardiovasculars ( Li+)◦ i.e. ACE inhibitors
Sodium Chloride ( Li+)◦ Inversely related to lithium concentrations
41
65-70% response in mania
Less toxicity with this agent than lithium◦ Much wider therapeutic window
Highly protein bound
42
Mixed / dysphoricbipolar
Rapid cycling
Migraine headaches
Neurological findings
Organic mania
Lithium treatment failures
Co-morbid substance abuse
Co-morbid psychiatric illnesses◦ Anxiety, Panic disorder
Irritability, aggression, and impulsive behavior
43
◦ Dose range is 500 to 3000 mg/day, divided
Start at 250 - 500 mg BID to TID
Max. = 60mg/kg/d
Give with food to minimize GI symptoms
Fast crisis stabilization regimen◦ Add a “0” to patient’s weight (lbs)
Plasma concentration monitoring ◦ 50-125mcg/ml for acute bipolar treatment
Up to 150mcg/ml have been used if needed NOTE: For epilepsy, range is 50-100mcg/ml
Toxicity is seen at levels above 100!
44

Neurologic◦ Ataxia, dizziness, drowsiness, tremor
Gastrointestinal◦ Nausea and vomiting◦ Give with food to minimize GI SEs
Hematologic◦ Prolonged bleeding times◦ Thrombocytopenia
Hepatologic◦ Transient s in LFTs◦ Liver failure reported
Dermatologic◦ Rash, alopecia, hair changes
45
Weight gain
Caution with pregnancy and breast-feeding◦ Formerly Category D - all trimesters
◦ Causes congenital malformations (neural tube defects)
In first trimester associated withspina bifida
Lower IQ well documented in in-utero exposed children
46

Enzyme inhibitor of metabolism
◦ MAJOR interaction with Lamictal®!
Lithium may increase VPA concentrations
Oral anticoagulants / Aspirin◦ Can cause bleeding times
Highly protein bound drugs
CNS depressants◦ Additive drowsiness
47

>60% effective for acute mania◦ Better efficacy in rapid cycling, mixed episodes,
and severe mania (with Lithium)
60-75% effective for prophylaxis
Time to response may be up to 1-3 weeks
48

Dosing◦ Initiate at 200-400mg/day◦ Increase by 200mg every 3-5 days up to 600-
1200mg/day in divided doses
Plasma concentration range is 4-12mcg/ml◦ Steady state is in 5 to 7 days◦ Draw levels 12 hours post-dose◦ Check biweekly for 2 months, then q 2-4 months if necessary Auto-induction takes about 4-5 weeks
May need to adjust dose upward to compensate
49
Neurologic (60% of patients)◦ Drowsiness, dizziness, diplopia
Gastrointestinal (15% of patients) Dermatologic◦ Rash, photosensitivity
Hematologic (25% of patients)◦ Rare risk of agranulocytosis and aplastic anemia
8 patients per 1 million patients per year exposure◦ Transient in WBC’s
Hyponatremia (Rare SIADH) Hepatologic (Transient s in LFTs) Caution in pregnancy and breast-feeding◦ Formerly classified Category D
Neural tube (folate antagonist), cardiovascular, and urinary tract defects
50

Enzyme inducer of CYP 1A2 & 3A4enzymes
◦Will metabolism of other drugs & itself Result is a in other drugs’ blood levels
Caution with critical drugs
ie. birth control pills, antibiotics, anticonvulsants, anticoagulants, etc.
51
FDA approved for maintenance of Bipolar I◦ “The effectiveness of LAMICTAL in the acute treatment
of mood episodes has not been established”
May be best used in bipolar depression and maintenance prophylaxis◦ If acutely manic – may be used as an adjunct
Maintenance efficacy proven in 2 – 18 month studies after acute stabilization◦ Time until depression or manic relapse prolonged
52

◦ Concerns: RASH in 0.08 – 10% of adults, up to 14% pediatrics
◦ Higher incidence in children; MUST discontinue drug at first sign of rash
◦ Dosing properly is critical to reduce risk of rash
◦ STEVEN’S JOHNSON’S SYNDROME!!

Common – GI: N/V/D, Abdominal pain
Neuro: Asthenia, Ataxia, Coordination problems, Dizziness, Headache, Insomnia, Somnolence, Tremor, Vertigo, Pain
Ophthalmic: Blurred vision , Diplopia
Psychiatric: Anxiety, Depression
Reproductive: Dysmenorrhea
Serious - Erythema multiforme , Stevens-Johnson Syndrome, Toxic
Epidermal Necrolysis, Anemia, Disseminated Intravascular Coagulation, Eosinophilia, Leukopenia . Thrombocytopenia, Liver failure, Aseptic Meningitis, Angioedema
Formerly Pregnancy Category C (D1 AUS): Increased cleft lip noted, decreased folate in rat pups 1st trimester
Respiratory: Rhinitis

55
As
monotherapy
With Valproic
acid
With an
EIAED*
Weeks 1&2 25mg QD 25mg QOD 50mg QD
Weeks 3&4 25mg BID 25mg QD 50mg BID
Weekly dose
↑ thereafter25 or 50mg 25mg 100mg
Average
maintenance
dose
200mg QD100-200mg QD
(or BID)
300-500mg
( BID)
If a patient misses a few days of medication, a careful titrationback to the maintenance dosage is recommended
* carbamazepine, phenytoin, phenobarbital, and primidone

A. Lithium
B. Lamotrigine
C. Valproic Acid
D. Quetiapine
57
FDA approved as monotherapy or adjunct to other mood stabilizers◦ Adjunctive therapy results in faster and better
remission rates
Significant symptom improvements can be seen in 3 to 7 days
Expert Consensus Guidelines changed from 1999 to 2004 to include atypicals as first-lineagents
Bipolar Depression: Seroquel, Abilify, Latuda(and Symbiax) are FDA approved
58
A. Ziprasidone
B. Paliperidone
C. Quetiapine
D. Iloperidone
59

Drug Weight
Gain
Sedation EPS Cardio GI
Olanzapine +++ ++ + 0 +
Risperidone ++ + ++ 0 +
Ziprasidone + + + + +
Quetiapine ++ ++ 0 0 +
Aripiprazole + + + 0 ++
Clozapine +++ ++ 0 + +
60
0= none known (placebo rate); +=minimal; ++=moderate or occasional; +++= severe or
common; Strakowski SM, et al. CNS Drugs. 2001;15:701-708; Strakowski SM, et al. Expert Opin

Dosage: ◦ Initial 2-3mg po daily (still can give BID to minimize
ADR)
◦ Avg dose 4-6mg/day; doses above 6mg/day not evaluated in BPD
◦ Risperdal Consta - dosing same as for schizophrenia
(25mg – 50mg IM q2weeks)
Common Side Effects◦ Drowsiness / Somnolence
Titration necessary to minimize orthostatic hypotension
◦ Orthostatic hypotension / Dizziness
◦ Little EPS at low doses / s at hi doses
◦ Medium weight gain (mostly in adolescents)
61
Dosing range: 5-20mg QD at bedtime◦ Zyprexa Zydis® (orally disintegrating tablet) & Zyprexa
IM (injection) available for agitation Agitation – Bipolar I Disorder: 10mg ODT/IM q2-4hrs
(range 2.5 – 10mg; up to 10mg IM x 3 doses q2-4hrs max in 24hrs)
Common Side Effects◦ Drowsiness
◦ Dizziness
◦ Akathisia
◦ Weight gain (avg. > 10 lb.)
Occurs early in tx. and continues avg. 9 months
◦ Hyperglycemia / Diabetes
62

63
FDA approved for bipolar depression Dosing◦ Begin with 6mg/25mg QHS◦ Adjust dose every 2 to 4 weeks as needed
How supplied:
6mg/
25mg
6mg/
50mg
12mg/
25mg
12mg/
50mg
olanzapine
equivalent 6 6 12 12
fluoxetine
equivalent 25 50 25 50
Clozapine analog◦ Half-life =
Immediate release: T1/2 = 6 hours (longer in some elderly pts.)
Extended release: T1/2 = 7 hours
N-desalkyl quetiapine (extended release): T1/2 = 9-12hrs
◦ Metabolized partially by CYP3A4
Phenytoin increases clearance up to 500% May need to dose of quetiapine
Medium weight gain observed◦ Dizziness and somnolence seen
◦ No EPS or prolactin at any dose studied Believed due to transient binding at D2 receptors
Usual doses are 400-800mg/d divided◦ Higher doses well tolerated
64

Average half-life is 7 hrs.
5HT/NE reuptake inhibition
Metabolized by CYP 3A4◦ Carbamazepine – Can ziprasidone by 36%
(need more Geodon®)
◦ Ketoconazole – Can ziprasidone by 33% (need less Geodon®)
Side effects◦ Rare QTc prolongation (EKG recommended); avoid
concomitant QTc prolonging medications or patients with EKG abnormality
◦ Drowsiness / insomnia, akathisia
Little weight gain or hyperglycemia observed
Dosing: 20mg-80mg BID with food◦ Up to 240mg/d clinically has demonstrated benefit in BPD
Rapid I.M. injection available (10-20mg)
65
Doses range from 10 to 30mg a day
◦ Bipolar studies used 30mg/d
◦ Once daily dose appropriate (T½=75hrs)
Also Approved for atypical depression◦ Suggests for those in the depressed phase, may be especially
useful if fear of switching to mania with an
antidepressant
ADR:◦ Less risk of metabolic side effects than other 2nd
generation/atypical antipsychotics – weight increased noted more in pediatrics (~7%, rates 2.5-21.5%)
◦ May cause akathisia (2-25%), other EPS reported
◦ Headache, insomnia, GI upset (N/V) usually transient
66
Maintenance dose from 5 – 10mg SL BID◦ Monotherapy start & max = 10mg SL BID
◦ Adjunctive therapy start 5mg SL BID Dosed BID due to sedation
(T½=24hrs)
Watch for drug interactionswith strong CYP 1A2 inhibitors
Adverse Effects◦ Somnolence, dizzness,
EPS, weight increase
67

Approved for Bipolar Depression only
Doses range from 20 – 120mg/day◦ 80-120mg/d no additional benefit in studies
◦ Take with food (at least 350 calories)
◦ Side effects: akathesia, EPS, somnolence
◦ PK: 3A4 Substrate
68

Newest approved agent for Bipolar I manic & mixed type, schizophrenia (Fall 2015)
Long T½ -◦ Parent 2-4 days, but active metabolite didesmethyl
cariprazine (DDCAR) 1-3 weeks
Severe hepatic or renal impairment - Do not use!◦ Mild or moderate, no adjustment necessary
Strong inhibitors of CYP 3A4 – Decrease dose 50%!
CYP 3A4 inducers = Do not use!
Most common ADR = EPS (including akathesia)
Starting dose = higher than schizophrenia◦ Bipolar Mania (maintenance) = 3-6mg
(schizophrenia maintenance= 1.5 – 6mg)
Indicated for treatment resistant schizophrenia AND bipolar disorder◦ Used for resistant bipolar disorder only
Many unpleasant side effects◦ Drooling, weight gain, seizures,
cardiovascular effects, diabetes, orthostasis, agranulocytosis, etc.
◦ Requires monitoring in REMS program
Costly lab monitoring
Dose titration (same as for schizophrenia)& national registry paperwork required
Arch Gen Psychiatry 2003;60:82-91
70

71
72
Lithium
VPA, CBZ, LTG
(Note: both answers are drugs, not classes. There may be more than one correct answer!)

Benzodiazepines◦ Can help with insomnia and anxiety
◦ Clonazepam and lorazepam studied
◦ Only to be used short-term
◦ Can be combined with an antipsychotic
◦ NOT CONSIDERED MOOD STABILIZERS
73

All antipsychotics can be used
Calcium Channel Blockers◦ Verapamil (Calan®, Isoptin®)
◦ Nifedipine (Procardia®, Adalat®)
◦ Nimodipine (Nimotop®) Has anticonvulsant effects
May be safer in pregnancy
74

Antihypertensives◦ Clonidine◦ Propranolol
Other Anticonvulsants –◦ Oxcarbazepine (Trileptal®)◦ Gabapentin (Neurontin®)◦ Topiramate (Topamax®)◦ Tiagabine (Gabitril®)◦ Many others in study
Electroconvulsive therapy (ECT)
75
Studies have shown lack of efficacy!!!!
No perfect mood stabilizer exists yet
Some may need 3 or 4 medsto “stabilize” their mood
Must consider benefits & risks, side effects, and outcomes◦ Patient must make an informed
decision with their medication
76