david amor - victorian clinical genetics services - pre-pregnancy genetic screening
TRANSCRIPT

Pre-pregnancy genetic screening
7th Annual Obstetric Malpractice Conference David Amor 22nd June 2015 VCGS is a not for profit subsidiary of Murdoch Childrens Research Institute and the main provider of clinical and pathology genetics services in Victoria

All couples hope for a healthy baby; however human reproduction is hazardous
• 4% of all babies are born with a congenital abnormality or genetic disorder that is evident at birth
• Most people have at least one recognised genetic disease
• All people are born with a genetic predisposition to various medical problems
• Every person’s genome contains 50-100 variants that are expected to cause genetic disease
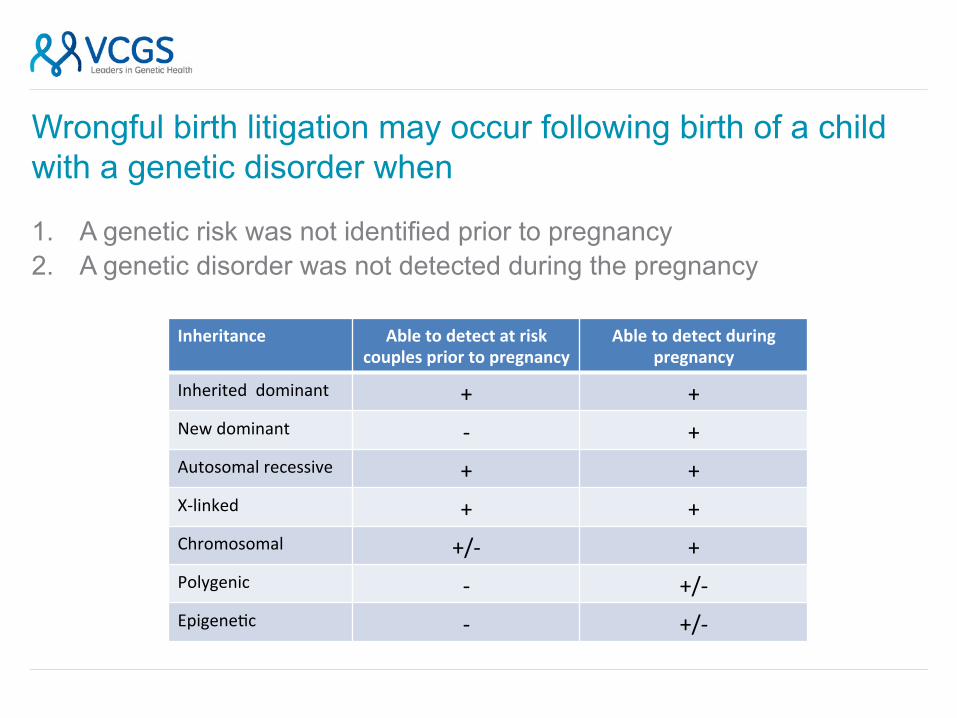
Wrongful birth litigation may occur following birth of a child with a genetic disorder when
1. A genetic risk was not identified prior to pregnancy 2. A genetic disorder was not detected during the pregnancy
Inheritance Able to detect at risk couples prior to pregnancy
Able to detect during pregnancy
Inherited dominant + + New dominant -‐ + Autosomal recessive + + X-‐linked + + Chromosomal +/-‐ + Polygenic -‐ +/-‐ Epigene@c -‐ +/-‐

Your baby has been diagnosed
with a rare gene@c disease
Circa 1998

Unfortunately we do not understand this fully. Gene@c tes@ng is not possible, and it
could not have been prevented
Circa 1998

OK, thanks.
Circa 1998

Testing technologies and practices relatively stable (and limited) from 1998-2013 • Taking a family history • Down syndrome screening • CVS and amniocentesis • Ultrasound
Allowing various reproductive options to be exercised: • TOP • PGD • Not have children • Accept risk

Your baby has been diagnosed with rare gene@c
disease
Circa 2015

We’ve iden@fied the faulty gene and both of you are carriers
Circa 2015

Couldn’t this have been picked up
during pregnancy?
Circa 2015

Nobody warned us this might happen.
Circa 2015

…and I told our doctor we wanted ALL the tests….
Circa 2015

Is there someone we can sue?
Circa 2015

New genetic technologies are currently transforming reproductive genetics
1. Pre-pregnancy genetic carrier screening using next generation sequencing
(NGS) This technology is transformative because it offers the ability to simultaneously test for large numbers of genes in a cost effective manner. Availability of preimplantation genetic diagnosis (PGD) depends on identification of risk prior to pregnancy
2. Non-invasive prenatal diagnosis (NIPD)
This technology is transformative because it enables examination of fetal DNA without any risk to the fetus

We all carry multiple recessive genes

The ‘long tail’ of recessive genetic disease
0
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
Carrier frequ
ency
Disease frequency

History of genetic screening in Australia Until now, the single gene conditions for which pre-pregnancy genetic carrier screening is undertaken are: • Haemoglobinopathies
(thalassaemia)
• Autosomal recessive diseases more common in the Ashkenazi Jewish community including Tay-Sachs disease
• Cystic fibrosis

Population carrier screening for CF • Cystic fibrosis (CF) is the most common inherited life shortening
condition affecting Australian children, with a carrier frequency of 1 in 25.
• Most children with CF (94%) have no family history of the condition.
• The Human Genetics Society of Australasia (2010) recommends that couples planning or in the early stages of pregnancy be made aware of the availability of CF carrier screening

Program Development 2005
2006
2007
Working group
Pre-‐pilot
Pilot: private pracDce
State-‐wide: shared care
General pracDce
Expanded program: -‐ more mutaDons -‐ more condiDons
2013

How the CF screening program worked • Pre-pregnancy or prenatal
screening offered by obstetrician or GP
• Pre-test information • Obstetrician/GP • Brochure in test pack • Website
• Testing by cheek brush • Self-administered • 12 CFTR mutations
• Posted to laboratory • Cost: $200 per test

The first 7 years experience • Number screened: 10,489
• Approx 90% females • Number carriers: 320 (3.05%; 1 in 33)
• 83% deltaF508 mutation • Number carrier couples: 15
• 11 pregnant at time of screening • 9 chose prenatal diagnosis • 3 affected pregnancies • All carrier couples chose prenatal diagnosis or preimplantation
genetic diagnosis in subsequent pregnancies • 1 false negative result (missed case)
• parents screened as low risk – child with CF due to paternal uniparental disomy of chromosome 7
(Archibald et al., Medical Journal of Australia 2014)

VCGS expanded approach VCGS Reproductive screen
• CF • SMA • Fragile X
These disorders are • Common • Severe • Tests relatively sensitive and
specific • Mature technology
Cost to patient AU$385
Diseases screened Cystic fibrosis
CF is an inherited condition affecting breathing and digestion. CF causes thick mucus which traps bacteria, resulting in recurrent infections that damage the lungs. Until recently, many children with CF died in early childhood
but now many live to be 30, 40 or more. There is no cure for CF but better treatments are under research and development.
Fragile X syndrome
FXS is the most common cause of inherited intellectual disability. People with FXS can have developmental delay,
learning difficulties, anxiety, autism and epilepsy. The features of FXS vary from mild to severe with males more likely to be severely affected than females. There is no cure for FXS although some interventions can improve outcomes for people with FXS. Some females who are carriers of FXS may have early menopause.
Spinal muscular atrophy
SMA is a condition that affects nerves in the spinal cord and causes muscles to get weaker. There are four types of
SMA. SMA type 1 is the most severe. Babies with SMA type 1 have weak muscles from birth and usually do not live past 2 years of age. SMA types 2 and 3 progress more slowly than type 1. There is no cure for SMA, however
there are treatments and interventions available aimed at managing symptoms and improving quality of life.


The future - expanded carrier testing • We are all carriers of 5-10 autosomal
recessive mutations • Theoretically it should be possible to
screen all couples prior to pregnancy to identify these mutations
• Offer prenatal diagnosis or PGD to couples who both carry a mutation in the same gene
• Current obstacles = • Cost • Interpretation

Target Enrichment (e.g. Exome, gene panels)
Whole genome




Counsyl test (Srinivasan et al., 2010; Lazarin et al. 2013) • 108 genetic diseases, 417 causal disease variants
• Includes many ethnic specific mutations • For ¼ of diseases, sensitivity is <10% of all mutations • For ½ of diseases, sensitivity is <50% • High specificity (>99.6%) – if something is detected, it is likely to be
real • Can either test one partner first (two-step) or both simultaneously
(one-step) • 1 in 4 patients receive abnormal result
• Test cost AU$849 (with Fragile X) through Healthscope

Counsyl test in practice (Lazarin et al. 2014) • 23,453 patient screened • 417 mutations associated with 108 conditions • 5,633 (24%) received were carriers for at least one condition (1 in 4.2) • 127 carrier couples
• 47 alpha-1 antitrypsin deficiency • 27 CF • 15 SMA • 10 sickle cell disease • 3 Ashkenazi • = 102 would have been detected using existing testing including
VCGS RGCS
Compared to VCGS RGCS, need to screen about 1000 people to detect one extra carrier couple!



723 variants in 147 genes All of 147 genes
Emory

…..or the “Rolls-Royce”

Choosing the right test
Single gene e.g. CF $150
VCGS 3 disorder screen $385
Counsyl, Emory targeted
muta@on panel 100-‐150 genes $900-‐$1700
Emory sequencing
panel 150 genes
$2000-‐$4000
Whole genome • 22,000 genes and all in between
• $14k-‐$28k

Criticisms of extended carrier screening • Marketing direct to patients • Lack of supportive clinical guidelines • Do not meet generally accepted criteria for population screening
• (many conditions rare, not severe, natural history not understood) • Depending on approach, there will always be:
• False negatives (low sensitivity) or • False positives (low specificity)
• Follow up testing and counselling likely to be expensive • Psychological impact significant • Inclusion of some common mild disorders inflates data • Lack of public funding
Stoll and Resta, Genetics in Medicine 2013
