cyclophosphamide: a comprehensive review as an …
TRANSCRIPT

www.wjpps.com Vol 7, Issue 6, 2018.
322
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
CYCLOPHOSPHAMIDE: A COMPREHENSIVE REVIEW AS AN
ANTICANCER
*Rashmi Wani, Shivaji Sumbhe, Akanksha Singh and Bhagyashree
Assistant Professor, Ideal College of Pharmacy and Research, Kalyan,
Maharashtra, India.
ABSTRACT
Cyclophosphamide (CP), also known as Cytophosphane among other,
is a medication used as chemotherapy and to suppress the immune
system. Cyclophosphamide is classified as Alkylating agent are most
active in the resting phase of the cell. These drugs are cell-cycle non
specific. Cyclophosphamide is used to treat several forms of cancer
including leukemias, lymphomas and breast cancer. and autoimmune
diseases. Due to its toxicity, it is replaced as soon as possible by less
toxic drugs. It is used to treat a certain type of kidney disease in children
after other treatments have not worked. Cyclophosphamide therapy is
associated with minor transient serum enzyme elevations and has been
linked to rare cases of acute liver injury. In addition, when given in high doses as a part of a
myeloablative therapy, Cyclophosphamide can cause acute sinusoidal obstruction syndrome.
Cyclophosphamide is used alone or in combination with other medications to treat Hodgkin's
lymphoma and non-Hodgkin's lymphoma, cutaneous T-cell lymphoma, Multiple myeloma
and certain types of leukemia including chronic lymphocytic leukemia (CLL), chronic
myelogenous leukemia (CML), acute myeloid leukemia (AML, ANLL), and acute
lymphoblastic leukemia (ALL). It is also used to treat retinoblastoma (cancer in the eye),
neuroblastoma (a cancer that begins in nerve cells and occurs mainly in children), ovarian
cancer (cancer that begins in the female reproductive organs where eggs are formed), and
breast cancer. Cyclophosphamide is also used to treat nephrotic syndrome.
INTRODUCTION[1-4]
Cancer is the uncontrolled growth of abnormal cells anywhere in a body. There are over 200
types of cancer. Anything that may cause a normal body cell to develop abnormally
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.421
Volume 7, Issue 6, 322-340 Review Article ISSN 2278 – 4357
*Corresponding Author
Rashmi Wani
Assistant Professor, Ideal
College of Pharmacy and
Research, Kalyan,
Maharashtra, India.
Article Received on
26 March 2018,
Revised on 16 April 2018,
Accepted on 06 May 2018,
DOI: 10.20959/wjpps20186-11685

www.wjpps.com Vol 7, Issue 6, 2018.
323
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
potentially can cause cancer; general categories of cancer-related or causative agents are as
follows: chemical or toxic compound exposures, ionizing radiation, some pathogens, and
human genetics. Cancer symptoms and signs depend on the specific type and grade of cancer;
although general signs and symptoms are not very specific the following can be found in
patients with different cancers: fatigue, weight loss, pain, skin changes, change in bowel or
bladder function, unusual bleeding, persistent cough or voice change, fever, lumps, or tissue
masses. Although there are many tests to screen and presumptively diagnose cancer, the
definite diagnosis is made by examination of a biopsy sample of suspected cancer tissue.
Cancer staging is often determined by biopsy results and helps determine the cancer type and
the extent of cancer spread; staging also helps caregivers determine treatment protocols.
In general, in most staging methods, the higher the number assigned, the more aggressive the
cancer type or more widespread is the cancer in the body. Staging methods differ from cancer
to cancer and need to be individually discussed with your health care provider. Treatment
protocols vary according to the type and stage of the cancer. Most treatment protocols are
designed to fit the individual patient's disease. However, most treatments include at least one
of the following and may include all: surgery, chemotherapy, and radiation therapy.
In the most basic terms, cancer refers to cells that grow out-of-control and invade other
tissues. Cells become cancerous due to the accumulation of defects, or mutations, in their
DNA.
Certain
Inherited genetic defects (for example, BRCA1 and BRCA2 mutations),
Infections,
Environmental factors (for example, air pollution), and
Poor lifestyle choices -- such as smoking and heavy alcohol use -- can also damage DNA
and lead to cancer.
Most of the time, cells are able to detect and repair DNA damage. If a cell is severely
damaged and cannot repair itself it undergoes so-called programmed cell death or apoptosis.
Cancer occurs when damaged cells grow, divide, and spread abnormally instead of self-
destructing as they should.
a. Change in bowel or bladder habits
b. A sore throat that does not heal
www.wjpps.com Vol 7, Issue 6, 2018.
324
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
c. Unusual bleeding or discharge (for example, nipple secretions or a "sore" that will not
heal that oozes material)
d. Thickening or lump in the breast, testicles, or elsewhere
e. Indigestion (usually chronic) or difficulty swallowing
f. Obvious change in the size, color, shape, or thickness of a wart or mole
g. Nagging cough or hoarseness
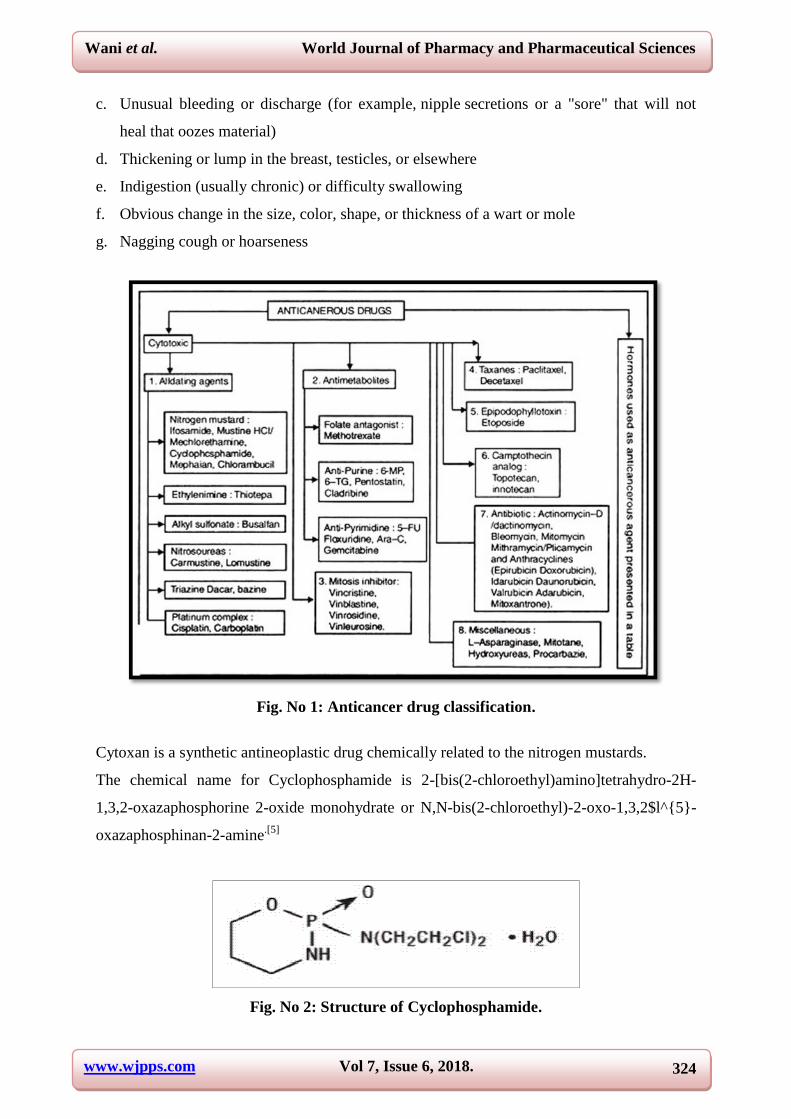
Fig. No 1: Anticancer drug classification.
Cytoxan is a synthetic antineoplastic drug chemically related to the nitrogen mustards.
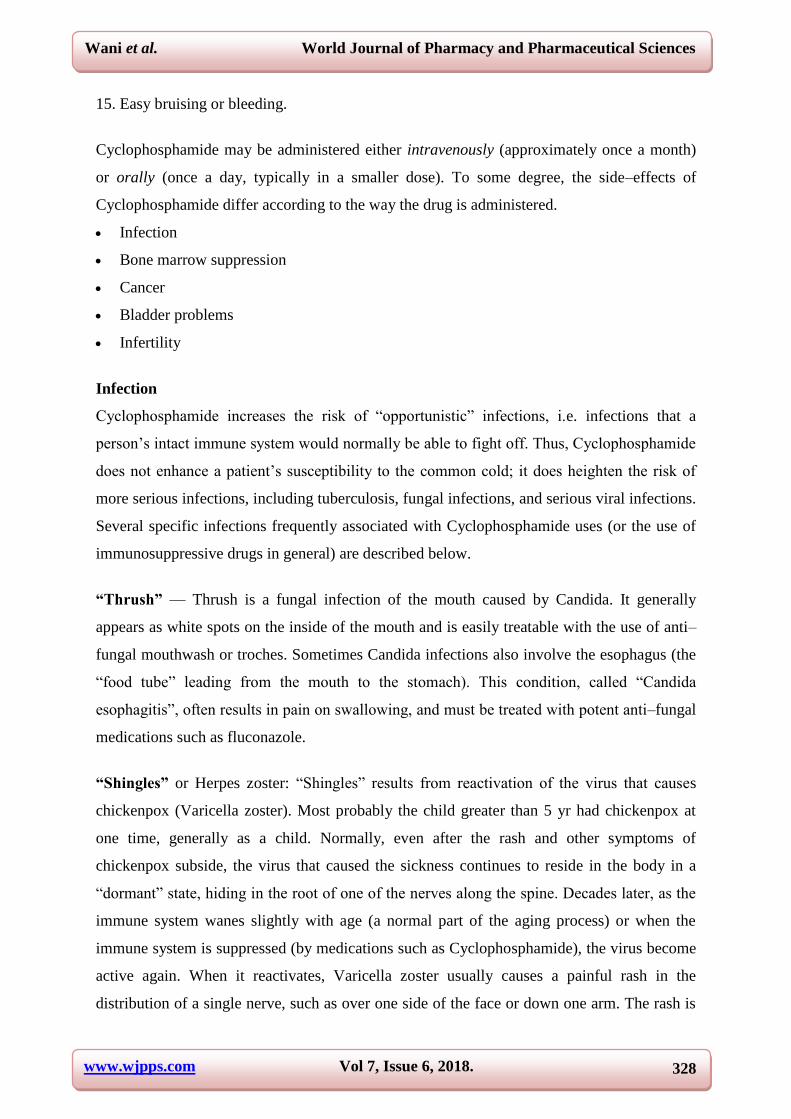
The chemical name for Cyclophosphamide is 2-[bis(2-chloroethyl)amino]tetrahydro-2H-
1,3,2-oxazaphosphorine 2-oxide monohydrate or N,N-bis(2-chloroethyl)-2-oxo-1,3,2$l^{5}-
oxazaphosphinan-2-amine.[5]
Fig. No 2: Structure of Cyclophosphamide.

www.wjpps.com Vol 7, Issue 6, 2018.
325
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
Cyclophosphamide has a molecular formula of (C7H15Cl2N2O2P•H2O) and a molecular
weight of 279.1.Physiochemical property:-Cyclophosphamide is soluble in water, saline, or
ethanol.
Pharmacokinetics[6-7]
Absorption: The Cyclophosphamide has Bioavailability of 75% and Onset of action 2-3
hours. The Peak plasma time for Cyclophosphamide is 1 hour and for metabolites 2-3 hours.
Distribution: Protein bound of Cyclophosphamide is low and metabolites are >60% protein
bound. Volume of Distribution: 0.48-0.71 L/kg.
Metabolism: The Cyclophosphamide is metabolized by liver and metabolites are 4-
hydroperoxycyclophosphamide, 4-aldophosphamide.
Elimination: The Cyclophosphamide has Half-life of 3-12 hour and excreted via Urine.
MECHANISM OF ACTION[7-10]
Cyclophosphamide is a chiral prodrug antineoplastic agent requiring activation by metabolic
and non-metabolic processes. It is activated by cytochrome P-450 (CYP450) enzyme in the
liver followed by the release of activated phosphoramide mustard and acrolein. The initial
metabolic step is mediated primarily by CYP2B6 and involves regioselective hydroxylation
at C4 of the Oxazaphosphorine ring to generate a Carbinolamine. This hydroxylation reaction
must occur before the molecule will be transported into cells and approximately 90% of drugs
get converted. CYP3A4 and CYP2B6 stereospecifically catalyze an inactivating N-
dechloroethylation reaction on the R ans S isomers yields highly nephrotoxic and neurotoxic
chloracetaldehyde. The CYP generated Carbinolamine undergoes non-enzymatic hydrolysis
to provide the Aldophophamide either in the blood stream or inside the cells. If this
hydrolysis occurs extracellularly, the aldophosphamide is still able to penetrate cell
membranes to reach the intracellular space. Once inside the cell, Acrolein is cleaved via
spontaneous β-elimination generating Phosphoramide mustard with pKa 4.75.
Phosphoramide mustard is the final alkylating agent responsible for cross-linking the
interstranded DNA at guanine N-7 position. Acrolein is highly cytotoxic to cultured tumor
cells but is not responsible for the cytotoxicity of Cyclophosphamide. It is in fact responsible
for hemorrhagic cystitis which is a life threatening side effect associated with
Cyclophosphamide.

www.wjpps.com Vol 7, Issue 6, 2018.
326
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. No 3: Mechanism of Action of Cyclophosphamide.
Fig. No 4: Sulfhydral Alkylation of Acrolein.

www.wjpps.com Vol 7, Issue 6, 2018.
327
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. No 5: Metabolites of of Cyclophosphamide.
SIDE EFFECTS:[10-13]
Cyclophosphamide is a cancer medication used to treat several types
of cancer. Cytoxan is also used to treat certain cases of nephrotic syndrome (kidney disease)
in children. Common side effects of Cytoxan include.
1. Nausea or vomiting (may be severe),
2. Loss of appetite,
3. Stomach pain or upset,
4. Diarrhea,
5. Temporary hair loss,
6. A wound that will not heal,
7. Missed menstrual periods,
8. Changes in skin color (darkening), or
9. Changes in nails.
10. Pink/bloody urine,
11. Unusual decrease in the amount of urine,
12. Mouth sores,
13. Unusual tiredness or weakness,
14. Joint pain, or
www.wjpps.com Vol 7, Issue 6, 2018.
328
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
15. Easy bruising or bleeding.
Cyclophosphamide may be administered either intravenously (approximately once a month)
or orally (once a day, typically in a smaller dose). To some degree, the side–effects of
Cyclophosphamide differ according to the way the drug is administered.
Infection
Bone marrow suppression
Cancer
Bladder problems
Infertility
Infection
Cyclophosphamide increases the risk of ―opportunistic‖ infections, i.e. infections that a
person’s intact immune system would normally be able to fight off. Thus, Cyclophosphamide
does not enhance a patient’s susceptibility to the common cold; it does heighten the risk of
more serious infections, including tuberculosis, fungal infections, and serious viral infections.
Several specific infections frequently associated with Cyclophosphamide uses (or the use of
immunosuppressive drugs in general) are described below.
“Thrush” — Thrush is a fungal infection of the mouth caused by Candida. It generally
appears as white spots on the inside of the mouth and is easily treatable with the use of anti–
fungal mouthwash or troches. Sometimes Candida infections also involve the esophagus (the
―food tube‖ leading from the mouth to the stomach). This condition, called ―Candida
esophagitis‖, often results in pain on swallowing, and must be treated with potent anti–fungal
medications such as fluconazole.
“Shingles” or Herpes zoster: ―Shingles‖ results from reactivation of the virus that causes
chickenpox (Varicella zoster). Most probably the child greater than 5 yr had chickenpox at
one time, generally as a child. Normally, even after the rash and other symptoms of
chickenpox subside, the virus that caused the sickness continues to reside in the body in a
―dormant‖ state, hiding in the root of one of the nerves along the spine. Decades later, as the
immune system wanes slightly with age (a normal part of the aging process) or when the
immune system is suppressed (by medications such as Cyclophosphamide), the virus become
active again. When it reactivates, Varicella zoster usually causes a painful rash in the
distribution of a single nerve, such as over one side of the face or down one arm. The rash is

www.wjpps.com Vol 7, Issue 6, 2018.
329
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
characterized by groups of small vesicles (blisters) sitting on a base of reddened skin, and
may be extremely painful. ―Shingles‖ is treatable with anti–viral medicines such as acyclovir
or famcyclovir. These should be instituted as soon as possible. Narcotic pain medicines may
also be necessary for several weeks. In a small minority of cases, ―shingles‖ results in pain
that can last for months. This condition is called ―post–herpetic neuralgia‖.
Pneumocystis carinii pneumonia (“PCP”) — Pneumocystis carinii is a fungus that resides
within the lungs of most people. People with intact immune systems have no trouble keeping
the organism at bay. In patients who are immunosuppressed, the organism can cause a serious
type of pneumonia: PCP. A few years ago, PCP was the most common cause of serious lung
infections in patients with AIDS. Because of advances in the treatment and prevention of this
condition, PCP is now a much rarer problem in AIDS. Similarly, PCP may also be prevented
in patients with vasculitis by having patients take certain types of antibiotics daily or every
other day. The antibiotics most commonly used for this purpose are Trimethoprim–
Sulfamethoxazole (Bactrim, Septra) or, in patients who are allergic to sulfa medications,
dapsone.
Bone Marrow Suppression
The bone marrow is the organ of the body that makes red blood cells (which carry oxygen),
white blood cells (which fight infection), and platelets (which help the blood clot). Nearly all
patients treated with Cyclophosphamide experience some suppression of the bone marrow’s
ability to produce these vital blood elements. Thus, careful monitoring of blood counts is
essential during Cyclophosphamide therapy. Suppression of the bone marrow by
Cyclophosphamide is usually transient — i.e. responsive to a decrease in dose or
discontinuation of the medicine — but dangerously low levels of any of these three cell lines
(or even permanent bone marrow failure) may occur.
The white blood cells are the cell line that is usually most sensitive to the effects of
Cyclophosphamide. When Cyclophosphamide is given intravenously, the white blood cell
count tends to reach its low point (―nadir‖) between 7 and 14 days after administration.
Therefore, blood cell counts should be measured approximately 10 days after the
administration of Cyclophosphamide, and repeated as often as needed to insure that the
counts do not go too low. This normally means checking blood counts every 2–4 weeks.
When Cyclophosphamide is given orally, blood counts should be checked about 7 days after
starting treatment and once every 3 weeks. At some centers experienced in the care of

www.wjpps.com Vol 7, Issue 6, 2018.
330
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
patients with Vasculitis and the use of Cyclophosphamide, blood counts are checked every 2
weeks.
Cancer
Many of the side–effects of Cyclophosphamide are most likely to occur while the patient is
taking the medication. With those side–effects, the risk of their occurrence diminishes greatly
after discontinuation of the drug. In contrast, the risk of cancer associated with
Cyclophosphamide use may continue for many years, even after patients stop the medication.
The risk of cancer appears to be dependent upon the length of time patients have taken the
medication and the cumulative dosage of the drug. Patients who have taken
Cyclophosphamide have an increased risk for at least two primary types of malignancy:
leukemia/lymphoma and bladder cancer. There may also be increased risks for other kinds of
cancer, but the risks are less high.
Leukemia/lymphoma — One of the long–term side–effects of Cyclophosphamide use is a
significant increase in the risk of bone marrow and lymph node cancers (known as leukemia
and lymphoma, respectively). Physicians are currently unable to predict which patients will
be at risk for these complications. The best means of avoiding these types of cancer is to use
Cyclophosphamide judiciously: the lowest possible dose of the medicine for the shortest
length of time necessary to control the disease.
Bladder cancer — Cyclophosphamide has a tendency to damage the bladder (see Bladder
problems, below). This damage predisposes patients to the development of bladder cancer.
The risk of bladder cancer (and of other bladder complications) is greater when
Cyclophosphamide is administered in the oral daily form. Among patients with Wegener’s
granulomatosis treated with oral daily Cyclophosphamide at the National Institutes of Health,
the risk of bladder cancer was 6%. Among patients followed for up to 15 years, the projected
incidence of bladder cancer was as high as 16%. Therefore, patients who have been treated
with Cyclophosphamide need to be followed indefinitely for the possibility of bladder
complications of the treatment. The best method of screening for this complication is to
check for red blood cells in the urine by performing a urinalysis, followed by cystoscopy if
red blood cells are present. Patients shown to have bladder damage by Cyclophoshamide, i.e.
to have drug-induced cystitis, should undergo surveillance cystoscopies at regualar intervals
determined by their urologists.

www.wjpps.com Vol 7, Issue 6, 2018.
331
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
When cyclophosphamide is administered intravenously, a bladder-protective medicine called
MESNA may be given at the same time. MESNA appears to neutralize the toxic metabolite
of Cyclophosphamide (acrolein) that is thought to be responsible for the bladder
complications. Additional strategies for decreasing the bladder toxicity of Cyclophosphamide
include: 1) giving intravenous hydration prior to cyclophosphamide; 2) taking all of the
medicine in a single morning dose and washing it down with a large amount of fluid; and 3)
drinking ample quantities of fluid throughout the day (eight 8–ounce glasses of water) to
maintain a brisk urine output.
Bladder Problems
In addition to cancer, Cyclophosphamide may cause a variable amount of bleeding from the
bladder, a complication known as ―hemorrhagic cystitis‖. This bleeding may range from a
few red blood cells in the urine (invisible to the naked eye; only detectable by examining the
urine under the microscope) to life–threatening hemorrhage from the bladder. If any bleeding
from the bladder is discovered while a patient is taking Cyclophosphamide, the medicine
should be stopped until the bladder can be evaluated by cystoscopy.
Infertility
Cyclophosphamide may cause infertility in both men and women who are treated with the
medication. As with many of Cyclophosphamide’s side–effects, the risk of infertility appears
to be related to the length of time a patient receives the drug (and probably the cumulative
dose, as well). A woman’s age may also affect her risk of infertility, with the occurrence of
early menopause higher in women over the age of 30 at the time treatment is begun.
In a long-term study of the effectiveness of Cyclophosphamide in treating lupus, the risk of
infertility among women of childbearing potential was 57%.
DRUG-DRUG INTERACTION[15-17]
Adenovirus types 4 and 7 live, oral Cyclophosphamide decreases effects of adenovirus
types 4 and 7 live, oral by pharmacodynamic antagonism. Avoid or Use Alternate Drug.
Immunosuppressive may diminish therapeutic effects of vaccines and increase risk of
adverse effects (increased risk of infection). Live-attenuated vaccines should be avoided
for at least 3mo after cessation of immunosuppressive therapy.
www.wjpps.com Vol 7, Issue 6, 2018.
332
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
Hydrochlorothiazide: Hydrochlorothiazide increases toxicity of Cyclophosphamide by
decreasing renal clearance. Avoid or Use Alternate Drug. Increased myelo-suppressive
effects can be seen.
Argatroban: Cyclophosphamide increases effects of Argatroban by unknown mechanism.
Use Caution/Monitor. Additive risk of bleeding may be seen in thrombocytopenic
patients receiving antineoplastic agents in combination with Argatroban because these
agents can decrease platelet counts.
Bivalirudin: Cyclophosphamide increases effects of Bivalirudin by unknown mechanism.
Additive risk of bleeding may be seen in thrombocytopenic patients receiving
antineoplastic agents in combination with anticoagulants such as bivalirudin.
Cholera Vaccine: Cyclophosphamide decreases effects of cholera vaccine by
immunosuppressive effects; risk of infection. Modify Therapy/Monitor Closely.
Immunosuppressive therapies, including irradiation, antimetabolites, alkylating agents,
cytotoxic drugs and corticosteroids (used in greater than physiologic doses), may reduce
the immune response to cholera vaccine.
Digoxin: Cyclophosphamide decreases levels of digoxin by inhibition of GI absorption.
Doxorubicin: Doxorubicin increases toxicity of Cyclophosphamide by unspecified
interaction mechanism. Increased risk of hemorrhagic cystitis is associated with this.
Heparin: Cyclophosphamide increases effects of heparin by unknown mechanism. Use
Caution/Monitor. Due to potential thrombocytopenic effects of Cyclophosphamide, an
additive risk of bleeding may be seen in patients receiving concomitant anticoagulants.
Hydroxyurea: Cyclophosphamide, hydroxyurea Combination may increase risk of
myelosuppression
Pentobarbital & Phenobarbital: Pentobarbital will decrease the level or effect of
Cyclophosphamide by affecting hepatic enzyme CYP2B6 metabolism.
Warfarin: Cyclophosphamide increases effects of Warfarin by unknown mechanism.
Anticoagulant effect is increased. Monitor coagulation parameters during and after
Cyclophosphamide therapy. Adjust the Warfarin dose as needed.
Dosage Forms & Strengths:[18-20]
Powder for injection: 500mg, 1g, 2g Tablet: 25mg,
50mg.

www.wjpps.com Vol 7, Issue 6, 2018.
333
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. No 6: Cyclophosphamide for Injection 1gm.
Fig. No 7: Cyclophosphamide for Injection 2 gm.
Fig. No 8: Cyclophosphamide for Injection 500 mg.
www.wjpps.com Vol 7, Issue 6, 2018.
334
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. No 9: Cyclophosphamide Capsule 25 mg.
1. Malignant Diseases
IV (intermittent therapy): 40-50 mg/kg (400-1800 mg/m²) divided over 2-5 days; may be
repeated at intervals of 2-4 weeks
IV (continuous daily therapy): 60-120 mg/m²/day (1-2.5 mg/kg/day)
PO (intermittent therapy): 400-1000 mg/m² divided over 4-5 days
PO (continuous daily therapy): 50-100 mg/m²/day or 1-5 mg/kg/day
2. Nephrotic Syndrome
2-3 mg/kg/day for up to 12 weeks when corticosteroids unsuccessful.
3. Non-Hodgkin Lymphoma
600-1500 mg/m² IV with other antineoplastics (part of CHOP regimen).
4. Breast Cancer
600 mg/m² IV with other antineoplastics; dose intensification possible.
5. Burkitt’s Lymphoma
High doses of IV (1-4 gm per square body surface area) in combination with other
chemotherapeutic agents as Vincristine, Methotrexate, Doxorubicin and Cytarabine
6. Chronic Lymphocytic Leukemia
IV with 250 mg per square body surface area on days 2-4 on cycle 1 and on days 1-3 in
subsequent cycles.

www.wjpps.com Vol 7, Issue 6, 2018.
335
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
7. Breast Cancer
Tablet 100 mg per square body surface area on days 1-14 given every 28 days, or IV 600 mg
per square body surface area given every 21 days as a part of CMF (Cyclophosphamide,
Methotrexate and Fluorouracil) regimen.
8. Systemic Lupus Erythematosus
IV dose is 7-25 mg per square body weight every month for 6 cycles. Oral dose is 1.5-3 mg
per square body weight per day.
9. Multiple Scelrosis
IV dose is 700 mg per square body surface area monthly.
10. Mononeuritis Muyltiplex
Oral dose 2 mg per kg body weight per day.
11. Pemphigus Vulgaris
Tablet 1-2 mg per kg body weight per day.
12. Bullous Pemphigoid
Tablet 1-2 mg per kg body weight per day.
13. Wegener’s Granulomatosis, Churg-Strauss Syndrome and Microscopic Polyangiitis:
Cyclophosphamide is an effective therapy for the treatment of this vasculitis. It is given in
doses of 2 mg per kg body weight per day orally together with glucocorticoid. After the
induction of complete remission (complete disappearance of detectable disease), patients are
maintained on Cyclophosphamide therapy for upto a year to minimize the risk of relapse and
gradually tapered and discontinued thereafter.
14. Goodpasture’s Syndrome
Usual dose is oral Cyclophosphamide 2 mg per kg body weight per day together with
Prednisolone for 2 weeks.
15. Bone Marrow Transplantation
Usual dose is 60 mg per kg body weight IV for 2 days.
www.wjpps.com Vol 7, Issue 6, 2018.
336
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
16. Autoimmune Hemolytic Anemia
Usually Prednisolone is used to prevent Hemolysis (breakdown of red blood cells) in
autoimmune hemolytic anemia. If the hemolysis fais to respond to Prednisolone, repeated
cycles of Cyclophosphamide at a dose of 50 mg per kg body weight per day for 4 days may
be considered.
17. Ovarian Cancer
Usual Adult Dose for For use in the treatment of epithelial ovarian cancer:
600 mg/m2 intravenously on day one in combination with Carboplatin or Cisplatin
Repeat cycle every 28 days.
Usual Adult Dose for Multiple Myeloma: In combination with other chemotherapeutic
agents as a part of the M2 protocol 10 mg/kg IV on day 1.
Administration[21-22]
1. Give dose early in day
2. Patients should drink plenty of fluids with PO doses
3. Patients should empty bladder frequently to prevent hemorrhagic cystitis
4. Sometimes, mesna is used concomitantly as prophylaxis against hemorrhagic cystitis
5. Monitor blood counts during therapy (WBC count may decrease to 2000-3000/μL without
serious risk of infection)
6. May be administered IM, intraperitoneally, intrapleurally, by IV piggy-back, or by
continuous IV infusion
7. IV Incompatibilities
8. Y-site: Amphotericin B cholesteryl sulfate
9. Cisplatin/etoposide, fluorouracil, hydroxyzine, methotrexate, methotrexate/fluorouracil,
mitoxantrone, ondansetron
10. Syringe: Bleomycin, cisplatin, doxapram, doxorubicin, droperidol, furosemide, heparin,
leucovorin, methotrexate, metoclopramide, mitomycin, vinblastine, vincristine
11. Y-site (partial list): Allopurinol, amifostine, bleomycin, most cephalosporins, cisplatin,
diphenhydramine, doxorubicin, doxorubicin liposomal, filgrastim, fluorouracil,
furosemide, gemcitabine, linezolid, lorazepam, mitomycin, morphine, paclitaxel,
prochlorperazine, propofol, sodium bicarbonate, trimethoprim/sulfamethoxazole,
vancomycin, vinblastine, vincristine
www.wjpps.com Vol 7, Issue 6, 2018.
337
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
IV Preparation[23]
Maximum concentration of Cyclophosphamide is limited to 20 mg/mL because of solubility
IV push: Reconstitute with NS (do not use SWI, because it is hypotonic).
Infusion: Reconstitute with SWI to concentration of 20 mg/Ml.
It may be diluted further with D5W, NS, lactated Ringer solution or other compatible fluids.
Combination Therapy[24-25]
Ewing’s sarcoma: It is one type of malignant bone tumor. Intravenous Cyclophosphamide
500 -1200 mg per square body surface area is used as chemotherapy in Ewing’s sarcoma in
combination with other chemotherapeutic agents such as doxorubicin, etoposide, vincristine
and dactinomycin.
Wegener’s granulomatosis: All are small vessel vasculitis. Cyclophosphamide is an
effective therapy for the treatment of this vasculitis. It is given in doses of 2 mg per kg body
weight per day orally together with glucocorticoids.
Chronic lymphocytic leukemia (CLL): Usual dose is intravenous Cyclophosphamide 250
mg per square body surface area on days 2-4 on cycle 1 and on days 1-3 in subsequent cycles,
as part of Cyclophosphamide, rituximab and fludarabine regimen.
Burkitt’s lymphoma: Usually higher doses of intravenous Cyclophosphamide (1 to 4 gm per
square body surface area) are used in Burkitt’s lymphoma in combination with other
chemotherapeutic agents such as Vincristine, Methotrexate, Doxorubicin and Cytarabine.
CONTRAINDICATIONS
Hypersensitivity Reaction:[26]
Cyclophosphamide is contraindicated in patients who have a history of severe
hypersensitivity reactions to it, any of its metabolites, or to other components of the product.
Anaphylactic reactions including death have been reported with Cyclophosphamide. Possible
cross-sensitivity with other alkylating agents can occur.
Urinary Outflow Obstruction
Cyclophosphamide is contraindicated in patients with urinary outflow obstruction.
Hemorrhagic cystitis, pyelitis, ureteritis, and hematuria have been reported with
Cyclophosphamide.

www.wjpps.com Vol 7, Issue 6, 2018.
338
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
Cardiotoxicity:[27]
The risk of cardiotoxicity may be increased with high doses of Cyclophosphamide, in patients
with advanced age, and in patients with previous radiation treatment to the cardiac region
and/or previous or concomitant treatment with other cardiotoxic agents.
Pulmonary Toxicity:[28]
Pneumonitis, pulmonary fibrosis, pulmonary veno-occlusive disease and other forms of
pulmonary toxicity leading to respiratory failure have been reported during and following
treatment with Cyclophosphamide.
Infertility:[29]
Male and female reproductive function and fertility may be impaired in patients being treated
with Cyclophosphamide. Cyclophosphamide interferes with oogenesis and spermatogenesis.
It may cause sterility in both sexes. Development of sterility appears to depend on the dose of
Cyclophosphamide, duration of therapy, and the state of gonadal function at the time of
treatment.
Herbal Preparation[30-33]
Amla
Cyclophosphamide (CP) is one of the most popular alkylating anticancer drugs in spite of its
toxic side effects including immunotoxicity, hematotoxicity, mutagenicity and a host of
others. The present study was undertaken to assess the protective effects of total aqueous
extract of a medicinal plant, Indian gooseberry (Emblica officinalis Gaertn.) in mice treated
with CP. These protective effects were studied on immunological parameters and kidney and
liver antioxidants. Plant extract treatment at a dose of 100 mg/kg body weight per os (p.o.)
for 10 days resulted in the modulation of these parameters in normal as well as CP (50
mg/kg)-treated animals. Plant extract in particular was very effective in reducing CP-induced
suppression of humoral immunity. Plant extract treatment in normal animals modulated
certain antioxidants of kidney and liver. In CP-exposed animals, plant pretreatment provided
protection to antioxidants of kidney. Not only were the reduced glutathione levels
significantly (p<0.001) increased but plant extract treatment resulted in restoration of
antioxidant enzymes in CP-treated animals. It is suggested that E. officinalis or its medicinal
preparations may prove to be useful as a component of combination therapy in cancer
patients under CP treatment regime Protective effects of Emblica Officinalis Gaertn In
cyclophosphamide-treated mice.

www.wjpps.com Vol 7, Issue 6, 2018.
339
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
CONCLUSION
Cyclophosphamide is used alone to treat Hodgkin's lymphoma, non-Hodgkin's lymphoma,
Burkitt’s Lymphoma, Goodpasture’s Syndrome, Wegener’s Granulomatosis and Multipple
Sclerosis. Cyclophosphamide-related hepatotoxicity is rare but can occur. Cyclophosphamide
can be used in combination with other medicaments to treat Ewing’s sarcoma, chronic
lymphocytic leukemia and Burkitt’s lymphoma like disorders and diseases.
Cyclophosphamide also can be used with herbal drug Amla to reduce Cyclophosphamide
iduced suppression of immunity. Cyclophosphamide is used to treat variety of Cancer hence
we can say that it has proves as a magical drug due to its multidirectional efficacy.
REFERENCES
1. Johan H. Block & Johan H. Beale, Wilson & Gisvolds Textbook Of Organic Medicinal &
Pharmaceutical Chemistry, 7th
Edition, Lippincott William & Wilkins Publishing, USA,
1977; 400.
2. Thomas L. Lemke, David A. Williams, Victoria F. Roche & S. William Zito, Foyes
Principles of Medicinal Chemistry, 7th
Edition, Wolters Kluwer Publishing, Delhi, 2013,
1211.
3. Grahaml Patrick, An Introduction To Medicinal Chemistry, 3rd
Edition, Oxford
Publishing, USA, 2005; 240, 508, 687.
4. Harkrishan Singh, Medicinal & Pharmaceutical Chemistry, 2nd
Edition, Vallabh
Prakashan Publishing, Delhi, 2005; 451, 594, 595, 625, 205.
5. Dr. Anees Ahmand Siddiqui, Seemi Siddiqui & Dr. R. Rajesh, Medicinal Chemistry, 1st
Edition, Vol. 1, Birla Publication Pvt. Ltd. Publishing, Delhi, 2008-2009, 47.
6. Alex Gringauz, Introduction To Medicinal Chemistry (How Drug Act & Why), 1st
Edition, Wiley India Pvt. Ltd. Publishing, Delhi, 2011; 112: 108.
7. Dr. Sriram & P. Yogeeswari, Medicinal Chemistry, 2nd
Edition, Pearson Publishing,
Delhi/Chennai/ Chandighar, 2010; Page No-562 & 563.
8. Ashutosh Khar, Medicinal Chemistry, 5th
Revised & Expanded Edition, New Age
International Publishing, Delhi, 2010; 801-806.
9. Dr. SS. Kadam, Dr. KR. Mahadik& Dr. KA. Bothara, Principles of Medicinal Chemistry,
16th
Edition, Vol-1, NiraliPrakashan Publishing, Pune, 2007; 154.
10. Thomas Nogrady& Donald F. Weaver, Medicinal Chemistry (A Molecular &
Biochemical Approch), 3rd
Edition, Oxford University Press Publishing, USA, 2005; 393:
448 & 456.

www.wjpps.com Vol 7, Issue 6, 2018.
340
Wani et al. World Journal of Pharmacy and Pharmaceutical Sciences
11. Alex Kleemann, Jurgen Engel, Bernhand Kutscher & Dietmar Reichert, Pharmaceutical
Substances( Synthesis, Patents & Application Of Most Relevant APIS), 5th
Edition
completely Revised, Thieme Stuttgart Publishing, New York, 2009; 567.
12. Prof. surendranath Pandeya, Medicinal Chemistry & Drug Design, 1st Edition, S. G.
Publishing, Varanashi, 2009; 201.
13. http://chemocare.com/chemotherapy/drug-info/cyclophosphamide.aspx.
14. https://www.webmd.com/drugs/2/drug-6093/cyclophosphamide-oral/details.
15. https://medlineplus.gov/druginfo/meds/a611044.html.
16. https://reference.medscape.com/drug/cytoxan-cyclophosphamide-342214.
17. https://www.medicinenet.com/cyclophosphamide/article.htm.
18. https://pubchem.ncbi.nlm.nih.gov/compound/cyclophosphamide#section=Top.
19. https://www.macmillan.org.uk/information-and-support/treating/chemotherapy/drugs-
and-combination-regimens/individual-drugs/cyclophosphamide.html.
20. http://www.cancerresearchuk.org/about-cancer/cancer-in-general/treatment/cancer-
drugs/drugs/cyclophosphamide.
21. https://www.drugbank.ca/drugs/DB00531.
22. http://www.bccancer.bc.ca/drug-database-
site/Drug%20Index/Cyclophosphamide_monograph_1June2013_formatted.pdf.
23. https://www.rxlist.com/cytoxan-drug.htm.
24. https://www.drugs.com/pro/cyclophosphamide.html.
25. http://step1.medbullets.com/oncology/111043/alkylating-agents.
26. https://www.pharmgkb.org/pathway/PA2035
https://www.ncbi.nlm.nih.gov/pubmed/12406916.
27. https://link.springer.com/chapter/10.1007/978-1-4615-1965-2_15.
28. https://www.webmd.com/drugs/2/drug-19924/cyclophosphamide-intravenous/details/list-
contraindications.
29. https://www.infomed.ch/100drugs/cyccont.html.
30. https://online.epocrates.com/u/1032009/cyclophosphamide/Contraindications+Cautions.
31. http://www.druglib.com/druginfo/cyclophosphamide/interactions_overdosage_contraindi
cations/.
32. https://www.pediatriconcall.com/drugs/cyclophosphamide/242.
33. https://www.researchgate.net/publication/11428538_Protective_effects_of_Emblica_Offi
cinalis_GaertnIn_cyclophosphamide-treated_mice [accessed Dec 20 2017].